This course will be updated or discontinued on or before Monday, June 28, 2027
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will know how to provide accurate assessment, education, and recommendations to lactating patients to promote and protect breastfeeding.
Objectives
After completing this continuing education course, the participant will be able to:
Explain the benefits of breastfeeding regarding infant health and development, maternal health, and broader global benefits.
Identify the goals, initiatives, and laws that aim to preserve and promote breastfeeding.
Describe the components of Baby-Friendly status.
Characterize the potential barriers to breastfeeding.
Categorize patients who are most at risk of experiencing barriers to breastfeeding.
Analyze the considerations that exist for mothers who are pumping versus feeding at the breast.
Describe the guidelines for breastmilk storage.
Summarize the physiology behind lactation at various stages of infant feeding.
Outline how to assess infant positioning, latch, and signs of effective milk transfer.
Formulate potential solutions for common problems encountered by breastfeeding mother-infant dyads.
CEUFast Inc. and the course planners for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Among the many approaches and beliefs regarding how to raise healthy and happy children, there is one constant that rings true in nearly all paradigms; choosing to breastfeed is often a very beneficial choice. The reasons to breastfeed are many, and the benefits can stretch well beyond a child's early years, with increased breastfeeding rates having the potential to impact global health on a profound scale.
The most current data regarding breastfeeding rates in the United States, from 2019, indicates that 83.2% of infants are breastfed at some point after birth, but only 55.8% of those infants are still breastfeeding at six months (Centers for Disease Control and Prevention [CDC], 2024c).
The Healthy People 2030 objectives for breastfeeding are meant to increase those rates and the public health benefits that come with them. To help to increase the rate of breastfeeding initiation and continuation, women must have adequate information and resources available, including knowledgeable and readily accessible healthcare professionals through every stage of pregnancy, birth, and lactation. With a mid-century decline in breastfeeding rates in the 1900s, when the popularity and availability of infant formula increased, there are now several generations of women who have little to no breastfeeding experience. The proverbial " village" of motherhood is often lacking quality breastfeeding advice for modern mothers. Because of this, much of the responsibility to help educate and support lactating women falls on healthcare professionals. The need for practical, accurate, and consistent breastfeeding advice is a necessity for anyone working with pregnant women, new mothers, or infants and children.
It is important to note here that although the default descriptive terms that will be utilized throughout this course are “breastfeeding, “breastmilk", "woman”, and “mother”, they are not meant to exclude any individual or any term someone prefers or identifies with. All birthing individuals, gestational carriers, surrogates, parents, and caregivers are meant to be included.
This course aims to present current and applicable information about breastfeeding and its challenges. It is vital that professionals who work with pregnant and postpartum mothers have all the tools they need to make a positive and lasting impact on promoting and protecting breastfeeding in a modern world.
It is common knowledge that breast milk is good for babies, but what exactly is beneficial about this liquid gold? Breastfeeding is a biological norm; breast milk is custom-made for exactly what each mother-baby dyad needs. While formula may be used for adequate caloric intake, no substitutes can provide the same biological and psychological advantage of breastfeeding.
Perhaps one of the most beneficial aspects of breastmilk is its immunological properties. During pregnancy, antibodies are passed from mother to infant through the placenta. These antibodies continue to circulate in the infant's body for several weeks following birth. For breastfed infants, the protection from viruses and bacteria does not stop there. In fact, new antibodies are received each time the infant consumes breastmilk.
The antibodies found in breastmilk can change daily based on microorganisms a lactating mother encounters throughout her day, including those that the baby has been exposed to and passes to the mother during feeding. Small amounts of the baby's saliva received through the skin of the nipple are scanned by the mother's immune system and, if any pathogens are found, appropriate antibodies may be included in the breastmilk by the next feeding (La Leche League, n.d.-c). This exchange and interaction of saliva and breastmilk also serves to regulate the infant’s microbiome and boost immunity this way as well. As a result of these immune properties, breastfed infants experience fewer illnesses and visits to the doctor's office, urgent care centers, and hospitals. In fact, breastfeeding reduces the rate of common childhood conditions such as (CDC, 2024a):
Children are usually several years old before their immune systems are fully developed. Still, with breastmilk support, any illnesses they do experience are generally less severe and have a shorter duration (CDC, 2024a).
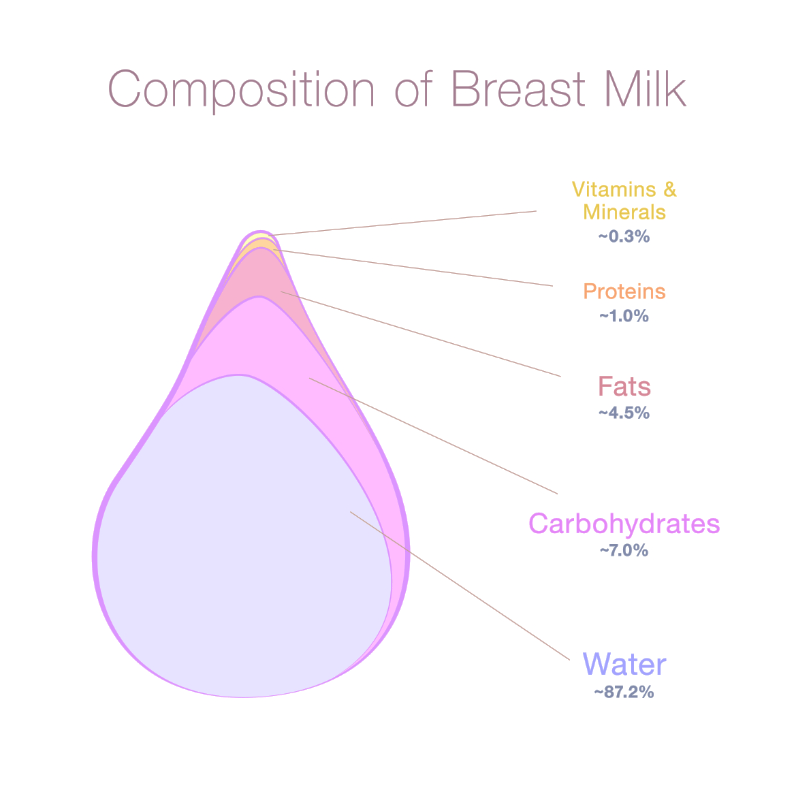
Breastmilk also has many nutritional benefits and is customized for each baby's particular needs. All breastmilk comprises some combination of proteins (whey and casein), fat, vitamins, carbohydrates, and water.
Image 1: Composition of Breast Milk
The exact composition changes as the baby grows and even changes throughout the day or within the same feeding, depending on the baby's needs. During the first few days of life, babies receive colostrum which is dense in calories and antibodies. Only small amounts of colostrum are needed to fill a newborn's small stomach and meet their nutritional needs with each feeding. It is easily digested and acts as a laxative to help clear meconium from the baby's intestines (La Leche League, 2018b). Over the first few days to weeks of life, breastmilk transitions to be thinner and primarily carbohydrate-based.
Babies born prematurely can benefit greatly from breastmilk. Preemie milk has been found to have a different combination of protein, minerals, and fat than term milk and is calorically dense, easier to digest, and promotes brain function, neurological tissue, and eyesight development, all of which are beneficial to premature infants. It is also packed with antibodies that reduce the occurrence of serious conditions common with prematurity, like necrotizing enterocolitis (NEC) (American Academy of Pediatrics [AAP], 2024.). In fact, a 2023 study reports that the rate of NEC in exclusively formula fed premature infants is 8.0%, while the rate in exclusively breastfed infants is only 1.9% (Xiong et al., 2023). This has an immense impact on the overall health, growth, need for surgery or other intervention, and cost of care for premature infants in the neonatal intensive care unit (NICU). Therefore breastmilk, either from the infant’s mother or donor milk, is strongly encouraged for all infants in the NICU to maximize health outcomes, reduce mortality, and reduce costs.
The health benefits of breastfeeding extend far beyond infancy as well. Children, teens, and even adults who were breastfed as infants experience lower rates of (CDC, 2024a):
Obesity
Dental caries
Cancer
Diabetes
Asthma
Allergies
Cardiovascular disease
Autoimmune diseases
Higher IQ levels, better speech development, and school performance are also noted in breastfed children (La Leche League, n.d.-c). Infants and children receiving breast milk are also found to have better social and emotional development and improved attachment security to their mothers than formula-fed peers (Krol & Grossman, 2018). However, these types of benefits may be heavily influenced by social factors like socioeconomic status, education level, and support systems in addition to just infant feeding methods and the exact relationship of breastmilk and social and intellectual development is unclear. In recent years, there is more and more emphasis being placed on social determinants of health and their role in impacting health in a way largely out of control of people themselves. It would make sense then, that the ability to successfully breastfeed is closely linked to similar characteristics of a person’s social circumstances and life.
Additionally, breastfeeding does not just benefit babies. It also has many protective factors for mothers as well. Women who have breastfed experience lower rates of cancers of the reproductive tract and breasts and have a decreased risk of diabetes and cardiovascular disease (CDC, 2024a). Studies show higher rates of mother-infant bonding, lower maternal stress, and reduced rates of postpartum depression in mothers who breastfeed as well (Krol & Grossman, 2018).
In addition to all of the health benefits that breastfeeding affords to individual babies and their mothers, there is also a broader impact to consider. In 2019, a child and maternal health initiative called “Alive and Thrive” developed a data analysis tool, The Cost of Not Breastfeeding Tool, to synthesize data regarding human and economic costs in relation to current breastfeeding rates (Walters et al., 2019). This tool can be utilized by breastfeeding legislators and advocates when considering health initiatives and how breastfeeding can affect regional, global health, and economics (Walters et al., 2019).
The tool's recent analysis indicates that, globally, nearly 600,000 childhood deaths from diarrheal illnesses or pneumonia could be prevented each year by breastfeeding (Walters et al., 2019). Additionally, a staggering 974,956 cases of childhood obesity and 98,238 maternal deaths from breast and ovarian cancers are attributed to a lack of breastfeeding each year (Walters et al., 2019).
Globally, this is equivalent to $1.1 billion in healthcare treatment costs and $53.7 billion in future earnings lost from children and women who died unnecessarily (Walters et al., 2019). Using data that suggests non-breastfed children grow up to earn less money than their breastfed peers due to cognitive differences or chronic health conditions, the tool also calculates a $285.4 billion loss in earnings each year. Combined, this all comes out to a whopping $341.3 billion economic loss each year, all from unmet breastfeeding goals (Walters et al., 2019).
Breastfeeding is also an excellent way to protect the ecosystem and is a low-cost, sustainable, and reduced-waste feeding method. The use of infant formulas creates greenhouse gases, pollution, and waste throughout every stage of manufacturing, packaging, marketing, and transporting. It requires energy and creates waste to mix formula, refrigerate or heat it, and sterilize bottles. A significant amount of plastic waste from bottles, nipples, and formula packaging winds up in landfills and oceans. Conversely, feeding at the breast requires none of those things and has a nearly undetectable carbon footprint, mostly from increased food and water consumption needed by lactating women (Burbidge & Williams, 2020). Pumping and milk storage supplies means exclusive pumping is not entirely waste free, but there is no pollution or waste from breastmilk production and the immune benefits help reduce healthcare costs for infants fed expressed breast milk, making pumping still more environmentally friendly than formula feeding.
The effects of breastfeeding on a woman's reproductive system are also eco-friendly. Breastfeeding, particularly when done exclusively and at least every 4-6 hours, can often effectively suppress ovulation. This helps with pregnancy spacing and smaller family sizes, if desired. Population control is especially important in areas where resources may be scarce. Lactating women often do not restart their period cycles for an average of 14 months while breastfeeding, which can greatly reduce the amount of waste from sanitary products used during menstruation (Burbidge & Williams, 2020).
Breastfed infants have been shown to require, on average, around 15% fewer visits to a healthcare provider each year, freeing up valuable and limited healthcare resources. The reduction in rates of obesity, cancers, and diabetes for the lactating mother has a similar effect, using up fewer resources and producing less strain on the healthcare system (Burbidge & Williams, 2020). The caregivers of healthier infants also require less time off work, resulting in fewer lost wages. In the long run, these children also often grow into healthier adults with fewer chronic health conditions who are then able to contribute more readily to the workforce and further benefit the economy (Burbidge & Williams, 2020).
With all of these potential life and money-saving benefits, it only makes sense that protecting and promoting the biological norm of breastfeeding would be a huge public health initiative and the focus of national and global health goals.
While the reasons for less-than-ideal breastfeeding rates vary by global region, some of the biggest contributing factors over the years in the United States include:
Lack of breastfeeding knowledge for patient before, during, and after pregnancy
Lack of appropriate and timely breastfeeding resources and assistance
Lack of protection for breastfeeding mothers at work or in public
Decades of unregulated lobbying and marketing practices from the formula industry
Thankfully, in recent years, much of this has been identified as problematic, and slow but measurable steps are being taken in the right direction for breastfeeding advocacy.
On a global scale, the World Health Organization (WHO) and United Nations Children's Fund (UNICEF) have developed guidelines for the Baby-Friendly Hospital Initiative (BFHI). BFHI aims to increase breastfeeding rates by ensuring healthcare facilities have the evidence-based knowledge and tools in place to provide the information and help women need to breastfeed successfully. Since many women begin their breastfeeding journeys at hospitals and birthing centers, it seems these are the best places to reach them and best promote breastfeeding.
The BFHI comprises ten steps, and the WHO calls upon participating countries to create their organizations, policies, and standards to implement the program. Since its launch in 1991, the program has been adopted by 152 countries and is being implemented at more than 20,000 facilities worldwide (World Health Organization [WHO], n.d.-a). Multiple studies since the program began support its success in increasing breastfeeding initiation and exclusivity rates. Studies also support that the closer a facility adheres to the program, the better the success and longevity of the mother's experience on their breastfeeding journey (Munn et al., 2016).
The first step of the BFHI is to have a written policy on infant feeding and routinely communicate these standards to staff and patients. This step is multifaceted and includes certain factors to ensure its success.
It is not enough for the policy to exist and the staff to be informed. In order to ensure it is successful, the policy should be well-integrated into facility and staff culture. In order to assess this, it is recommended that 80% of staff be able to identify at least two components of the initiative if randomly questioned.
The details of the policies also need to be evidence-based and in alignment with the current recommendations of WHO and UNICEF. Additionally, the policy should comply with the International Code of Marketing of Breast-Milk Substitutes (discussed later in more depth).
Finally, the policy must include a plan for collecting data and tracking progress of the program on facility outcomes. There must be a plan for how adjustments will be made to work towards goals. Specifically, WHO requires that facilities track breastfeeding initiation and exclusivity rates during a patient’s time at the facility, among other data.
The second step is to ensure that all staff have proper training, and the skills related to breastfeeding and can provide competent breastfeeding-centered care.
As with any intervention in a healthcare setting, the proposed program is only able to be successful with active engagement and proper training of staff. Mothers who have struggled with breastfeeding in the past will often cite mixed information or inconsistent knowledge among clinicians that they encounter. As such, consistent and streamlined patient experiences, even with shift changes and differences in staff members is paramount. The members of the healthcare team should function as one well-trained and knowledgeable unit on all things breastfeeding, including:
Therapeutic communication techniques
Understanding of lactation and breast milk
Proper ways to assess a latch and feeding effectiveness
Identify potential or actual problems in a timely manner
How to make adjustments or suggest changes during a feeding
Troubleshoot common issues or concerns with breastfeeding
The third step is to provide pregnant women and their families with information about the importance of breastfeeding.
Studies indicate that the decision of whether or not to breastfeed begins long before the baby is born. Because of this, pregnant women should be among the target audience for breastfeeding education. Patients should be given plenty of time to ask questions, explore options, and consider their choices prior to giving birth. The first trimester is the ideal time to first introduce the topic of breastfeeding.
Many birthing facilities also have clinics that manage prenatal care, putting them in the perfect position to provide information about breastfeeding early on. For facilities that do not provide antenatal care, networking with clinics, primary care, and community resources to get this information to patients is a necessity.
The counseling and information provided should be culturally and socially sensitive and tailored to each patient and family’s unique needs and circumstances, being mindful of barriers that may exist.
Information for pregnant patients should include a verbal discussion, written information or pamphlets, and options for additional classes and support groups. Information should include the benefits of breastmilk for both the baby and the mother and information that may be important for mothers to include in their birth plan, such as skin-to-skin contact and initiating the first feeding within the first hour of birth. After the initial discussion, the topic can be revisited and additional questions answered throughout the duration of the pregnancy.
The fourth step is to prioritize skin-to-skin contact immediately after birth (whenever safely possible) and encourage mothers to initiate breastfeeding for the first time within the first hour of life (known as the Golden Hour).
Whenever the health of the mother and baby allows, babies should be immediately placed prone on the mother’s chest after delivery. This contact should continue uninterrupted for the first hour of life, delaying interventions such as bathing and weighing for the more important task of bonding and the first feeding.
Image 2: Skin-to-Skin
Skin-to-skin contact, which is also known as “kangaroo care”, provides temperature, heart rate, and breathing regulation for the baby and provides both the mother and the baby with oxytocin release and bonding (Cleveland Clinic, 2023b).
For infants born via cesarean section, the current standard is usually to place the infant under a warmer until the surgery is finished and the mother has been moved to recovery, however more and more evidence is emerging that supports skin to skin immediately after delivery, in the operating room, as long as the mother and baby are medically stable. The benefits of this practice should take priority over existing habits, routines, or ease for the operating room staff. This practice also provides increased birth experience satisfaction for mothers who deliver via cesarean section.
For preterm or low birth weight infants, this practice can be especially beneficial, as these infants are at risk for poor temperature regulation due to less brown fat (Cleveland Clinic, 2023b). For these infants who could very well be admitted to the NICU based on weight and level of prematurity, the act of skin-to-skin will look different for the health and well-being of the baby. Depending on the medical stability of the infant, additional components and medical supports such as ventilators, chest tubes, intravenous lines, nasogastric (NG) tubes, or nasal cannulas, might need to be worked around to safely engage in skin-to-skin. While they provide a unique challenge, NICU staff should be well equipped in assisting a mother in therapeutic skin-to-skin with her child when possible. While it might not always be possible soon after birth, NICU staff and providers should work closely with the mother to decide when the best times would be to provide skin-to-skin care for the first and subsequent times. These skin-to-skin sessions are best when they are carefully coordinated with the NICU parent, NICU nurse, and NICU respiratory therapist, as needed, to ensure all wires and tubes are moved gently and secured in place while mom has her special time with her infant. A NICU nurse should carefully monitor the dyad to ensure mom and baby are comfortable and that the baby remains stable. While many NICUs will maintain the infant on an external monitor for vitals including heart rate and respiratory rate to be able to be read without even being in the patient’s room, it is important that the NICU nurse monitor the infant’s temperature closely to ensure they do not get too cold or too warm. If at any point the infant is not tolerating skin-to-skin as evidenced by bradycardia and/or desaturation episodes, after a period of time when minor adjustments are attempted to allow the session to continue, it might become appropriate to end the session early to allow the infant to restabilize safely and unstimulated in their isolette.
In addition to the bodily regulation and bonding for mother and baby after the monumental task of birth, immediate skin-to-skin helps to facilitate early initiation of breastfeeding. In turn, early initiation of breastfeeding also increases the secretion of oxytocin needed for milk production and successful breastfeeding. Therefore, skin-to-skin has many benefits for both the baby’s health and the mother’s milk supply.
After that initial hour of life, babies typically are more sleepy and less alert and delayed first feeding attempts may be less successful, so offering it as early as possible, again prioritizing medical stability, is most beneficial.
The fifth step of BFHI is to show mothers how to breastfeed and navigate everyday challenges.
Despite being said to be a natural process, breastfeeding does not occur automatically, and mothers and infants need to get to know each other and learn how to do this act together. Mothers often need reassurance and practical support including information, demonstrations, and encouragement during the early days of breastfeeding. Frequent topics that need to be covered are what exactly feeding cues are, positioning of baby for a proper latch, hand expression of milk, nipple care, and how to assess that a feeding has been successful.
The sixth step is concerning the action of supplementation of nutrients in addition to breastmilk. According to BFHI, it is important to not give newborns any additional food or drink other than breastmilk unless it is medically necessary.
Each time a newborn baby is at the breast, nipple stimulation triggers a hormone response in the mother’s body and positively impacts milk production. During the early days when milk supply is being established, any time a baby is fed not at the breast, an opportunity to stimulate milk supply is missed. If other caregivers would like to feed the baby via a bottle or if mom is unable to breastfeed for some reason, the mother can still pump to signal to the body that another feeding is taking place and continue with milk production accordingly.
There are definitely some medically indicated circumstances when formula or supplementation may be recommended for the baby’s health, but these situations need to be determined by a pediatrician or pediatric nurse practitioner (PNP) in collaboration with the child’s family. Examples of situations that may require supplementation can include:
Hyperbilirubinemia
Liver problems that affect the baby’s ability to absorb nutrients from breast milk
Truly inadequate milk supply due to a medication mom is taking
Inadequate milk supply due to medical conditions
An allergy or intolerance to breast milk that is not resolved with changes to the maternal diet (such as galactosemia)
Insufficient weight gain with exclusive breastfeeding and/or pumped expressed milk
The supplementation that is recommended might just be mom’s pumped breast milk rather than latching at the breast. If the infant is struggling with mom’s milk for some reason or if there are supply issues, donor milk or formula might be recommended.
While breastfeeding at the breast is generally preferred, in the case of supplementation, there is the option of supplementing but doing so without introducing a bottle. Because it can sometimes be difficult for infants to learn how to breastfeed while also feeding using a bottle nipple, it can be an option to utilize a cup, finger, or tube/syringe to provide milk instead. See the image below showing a newborn infant being fed via cup.
Image 3: Cup Feeding
Limited staff time or knowledge, or limited resources are not appropriate reasons to recommend formula or supplementation. It is important that a lactation professional work with mom in these special cases to help determine why an infant might not be gaining weight appropriately or how mom can try to increase her supply before resorting to other options. Supplementation in many cases can be temporary to mitigate short-term problems that can be resolved quickly if treated in the right way (San Diego Breastfeeding Center, 2019).
The seventh step is what is known as “rooming-in”. It is important to allow the mother and her baby to remain together for 24 hours a day unless separation is medically necessary.
Rooming-in facilitates bonding between a mother and her infant and also helps mothers learn feeding cues and how to respond quickly when the infant starts to indicate hunger. Evidence suggests mothers have an increased milk supply and longer duration of breastfeeding and exclusivity when they room-in with their infants after delivery.
Rooming-in is also empowering to women and provides them with more positive feelings about their ability to breastfeed and care for their infants upon discharge.
In situations where infants do need to be separated, the separation should not exceed an hour whenever possible. If the infant or mother are unstable or ill following delivery, rooming-in may not be possible and the appropriate resources such as NICU admission, should be utilized. In general, however, separating mom and baby by taking infants to the nursery for assessment or vitals, or on a routine schedule to allow mothers to rest, should not be part of routine postpartum unit protocol.
In the event the infant is admitted to NICU, many NICUs have the ability to provide rooming-in prior to the infant being discharged home. It is extremely valuable for NICU parents to have the opportunity to room-in with their child who has had a NICU stay, especially for those who have been NICU patients for weeks or months. During this time, mom is given the opportunity to learn more about her child by herself or with her partner, in addition to learning to manage breastfeeding and/or her pumping schedule and mastering her use of medical equipment or medications that might be components of discharge learning for a NICU graduate.
The eighth step of BFHI is to teach mothers about hunger cues and encourage feeding on demand.
One of the reasons mothers may struggle to effectively latch an infant is that they are waiting too long to put the baby to the breast, resulting in a fussy and uncooperative infant. This might occur for several reasons, including attempting to adhere to a strict schedule or inadequate knowledge of early feeding cues. Breastfed babies should be fed on demand as they cannot be overfed and frequent nipple stimulation, especially early on, is beneficial for milk supply. Babies who are in the early stages of hunger latch more easily and are less likely to be frustrated or resist positioning as they are not yet distressed.
Mothers should be taught to look for hunger cues. Early hunger cues can include (Engelbrecht, 2025; CDC, 2024e):
Rooting/rooting reflex (head turning to side to look for breast when cheek or mouth touched)
Sucking on hands
Moving fists to their mouth
Licking their lips
Lip smacking
Opening and closing mouth
Becoming more alert and active
Clenching their hands
Fidgeting
Image 4: Rooting
Late hunger cues can include(Engelbrecht, 2025; CDC, 2024e):
Fussing
Crying
Agitated
Hungry babies show they are hungry before they start to cry. The goal is to intervene and feed while the infant is demonstrating early signs of hunger to increase the chances of a good latch at the breast and a more organized feeding session.
The ninth step is discussing with mom the risks of using pacifiers or bottles while initially trying to establish breastfeeding.
Pacifier and bottle use have been said to lead to reduced nipple stimulation at the breast and can result in a decreased milk supply in the mother. Therefore, the use of artificial nipples is overall discouraged in the early weeks, before good habits and efficient breastfeeding are established. Additionally, artificial nipple use has been associated with confusion for the baby regarding proper sucking methods to receive milk or may hold off or “mask” hunger cues.
It is important to also note that once breastfeeding is well established, there is no contraindication for pacifier or bottle use.
The tenth and final step is to coordinate access to breastfeeding support resources for once mom and baby are discharged from the facility.
Continued support upon discharge is necessary to continue a healthy breastfeeding relationship. As the baby grows and matures, the breastfeeding relationship will change, new problems or issues may occur, or mothers may lose confidence. Regardless of how good the support and care in the hospital was, it is not enough to solve the new issues in the coming weeks and months, and a solid and knowledgeable support system is needed.
Many mothers do not personally know anyone who has breastfed or is knowledgeable in breastfeeding, so they should be given information about support groups or meeting spaces with other lactating mothers. Many women find these relationships immensely useful for boosting confidence and feeling validated by others with similar experiences.
They should also be given information for how to contact professional resources like lactation services. Facilities are encouraged to make follow-up calls or schedule appointments within the first week of discharge.
This program is adopted and implemented via Baby-Friendly USA in the United States. CDC tracking of breastfeeding rates over the last several years indicates that BFHI has, at least in part, contributed to improving breastfeeding initiation, exclusivity, and longevity (Baby-Friendly USA, 2024). Take a brief look at table 1 below.
Table 1: Percentage of U.S. Children Who Were Breastfed, by Birth Year, National Immunization Survey, United States (Percentage ± half 95% Confidence Interval)
Birth Year
2013
2014
2015
2016
2017
2018
2019
2020
2021
Ever Breastfed
81.1 ± 1.1
82.5 ± 1.1
83.2 ± 1.0
83.8 ± 1.2
84.1 ± 1.0
83.9 ± 0.9
83.2 ± 1.0
83.1 ± 1.0
84.1 ± 0.9
At 6 months
51.8 ± 1.4
55.3 ± 1.4
57.6 ± 1.4
57.3 ± 1.6
58.3 ± 1.4
56.7 ± 1.2
55.8 ± 1.3
58.2 ± 1.2
59.8 ± 1.1
At 12 months
30.7 ± 1.3
33.7 ± 1.3
35.9 ± 1.3
36.2 ± 1.5
35.3 ± 1.4
35.0 ± 1.1
35.9 ± 1.2
37.6 ± 1.2
39.5 ± 1.1
Exclusively through 3 months
44.4 ± 1.4
46.6 ± 1.4
46.9 ± 1.4
47.5 ± 1.6
46.9 ± 1.4
46.3 ± 1.2
45.3 ± 1.3
45.3 ± 1.2
46.5 ± 1.2
Exclusively through 6 months
22.3 ± 1.1
24.9 ± 1.3
24.9 ± 1.2
25.4 ± 1.3
25.6 ± 1.2
25.8 ± 1.0
24.9 ± 1.1
25.4 ± 1.1
27.2 ± 1.0
Data from 2013 to 2015 births were based on landline and cellular telephone sampling, and data for 2016 births and onwards were based on cellular telephone sampling only. See Survey Methods for details and data before 2010 at Data, Trends, and Maps.
The Healthy People 2030 objectives for breastfeeding include (Office of Disease Prevention and Health Promotion, n.d.):
Increasing the exclusivity rate at six months to 42.4%
Increasing the percentages of infants breastfed in any capacity at 12 months to 54.1%
The CDC works to achieve these goals in several ways, including (CDC, 2024a):
Tracking breastfeeding data
Tracking data for how well states and birthing facilities support breastfeeding mothers
Supporting the 10-step hospital initiative we have just discussed in great detail
Implementing a call to action from the Surgeon General for nurses and doctors to support breastfeeding
Partnering with states to help employers meet standards for pumping breaks and appropriate spaces for pumping and milk storage
Recognizing the mothers who are less likely to have appropriate breastfeeding support (such as Black mothers) and promote the development of and access to community resources for breastfeeding
Promoting access to support systems like counseling and peer support groups in the community
Supporting policy in childcare and early education settings that support continued breastfeeding
How can nurses and doctors best support breastfeeding? They can do this by:
Utilizing opportunities for learning about breastfeeding and staying up to date on best practices for supporting lactating women
Talking with mothers early in pregnancy, throughout pregnancy, and after birth about the benefits of breastfeeding
Making breastfeeding support a part of standard care in the hospital setting and clinic setting after birth
Creating breastfeeding support teams within the hospital or clinic setting and include certified lactation specialists (International Board Certified Lactation Consultant [IBCLC] or Certified Lactation Counselors [CLC]) for the highest quality resources
Knowing and utilizing community resources for lactation support once mothers leave the hospital
Following the International Code for Marketing of Breastmilk Substitutes and avoiding advertising for a formula of giving out free samples
The U.S Preventive Services Task Force (USPSTF) is a task force that is tasked to improve the health of the people in the United States by making evidence-based recommendations for effective ways to lengthen life and avoid disease (U.S. Preventive Services Task Force [USPSTF], 2025). The USPSTF recently issued a formal recommendation in an effort to further its’ support for breastfeeding. Much like the Healthy People 2030 objectives, USPSTF knows that the association between breastfeeding and the health benefits have been well established and aimed to focus their in-depth review over a couple of years to evaluate the evidence of the health benefits of breastfeeding for both the mother and the baby as well as any harm that would be contributed with the use of behavioral counseling interventions (USPSTF, 2025). The USPSTF found adequate evidence that counseling interventions provided a moderate benefit in improving not only the initiation and duration, but also the exclusivity of breastfeeding (USPSTF, 2025). This recommendation states that it is encouraged that primary care providers provide interventions, referrals, and adequate counseling, both during pregnancy and after birth, to support a woman in their success with breastfeeding (USPSTF, 2025). The recommendation is made to apply to all pregnant and postpartum adults as well as those who are adolescents (USPSTF, 2025). USPSTF also believes that evidence-based interventions should be readily available and accessible for all pregnant and postpartum patients (USPSTF, 2025). The counseling that they are referring to may be offered in a manner that is most helpful and most accessible for each patient, in a variety of settings, either via in-person/in-home, video, telephone, or text access and can include the following (USPSTF, 2025):
Formalized breastfeeding knowledge program
Practical breastfeeding skills to include proper latch
Management of breastfeeding complications as they arise
Advice and support for the family members of the breastfeeding woman so that they can provide support for her (direct support, psychological support, etc.)
In recent years, state and federal legislatures have also changed to support breastfeeding women in public and the workforce. Under the Affordable Care Act (ACA) in 2010, the Fair Labor Standards Law of 1938 was amended to require all employers to provide reasonable break time for employees to express milk whenever needed. The law also requires employers to provide a clean and private space that is not a bathroom for milk expression. Additionally, under the ACA, insurance plans must cover supplies and services related to breastfeeding, such as breast pumps and lactation consultation appointments.
In 2019, the Fairness for Breastfeeding Mothers Act was passed, requiring certain public spaces to have clean and private "lactation rooms" for the public to use for breastfeeding or pumping needs. At the state level, all 50 states and the District of Columbia, Puerto Rico, and the Virgin Islands protect the right of women to breastfeed in any public or private space. This legislation aims to promote and protect breastfeeding and helps avoid barriers for women successfully meeting their breastfeeding goals (National Conference of State Legislatures [NCSL], 2021).
Entrenched in some controversy in the United States is the International Code of Marketing of Breastmilk Substitutes. This list of rules was developed by the WHO in 1981 and is intended to regulate the marketing of breastmilk substitutes, primarily formula so that marketing ploys for baby-food companies do not undermine breastfeeding. Included in the Code are provisions such as (WHO, 1981):
Product advertising, free samples, discounts, and promotions targeted towards pregnant or new mothers are prohibited
Product representatives may not contact mothers
Warning labels that products are not comparable to breastfeeding must be included on products
Healthcare workers should encourage and protect breastfeeding and should only factually discuss substitutes and not promote the use of such products
Formula manufacturers may not provide gifts or monetary compensation to healthcare workers who might, in turn, promote their products
Product advertisements may not be displayed at healthcare facilities
Product labeling cannot contain words such as "humanized," which implies the product is equivalent to breastfeeding
Product labels must contain a written warning about the potential risk of contamination with microorganisms
The Code was developed for international use, and 84 countries signed it when it was originally written. Still, due to heavy lobbying by formula companies, it was not adopted by the United States until 2010, and even then, no legislation was enacted to enforce it. The present date serves as guidance for facilities that utilize the Baby-Friendly Hospital Initiative but are not enforceable by law. Unfortunately, there are widespread violations by the baby-food industry who continue to lobby against any regulations or legislation to their marketing (Walls, 2018).
Despite overwhelming evidence to support the benefits of breastfeeding and the somewhat renewed energy being put into supporting it, many women in this country still struggle with a series of barriers to successfully breastfeed their infants. Healthcare providers must be aware of these and work to minimize their impact on mothers attempting to breastfeed. ACOG has categorized these barriers into several groups (2021).
Healthcare providers not appropriately educated to assist breastfeeding families also represent a barrier to breastfeeding. During pregnancy, mothers may not receive adequate information about feeding choices to make a truly informed decision if their healthcare providers are ill-equipped to answer questions about breastfeeding (American College of Obstetricians and Gynecologists [ACOG], 2021). Once the baby has arrived, mothers may struggle with breastfeeding if healthcare providers cannot properly address any difficulties or questions or if each nurse or provider gives varying advice. Additionally, failure to understand the physiology of lactation can lead providers to provide a parent with the wrong advice and potentially damage the mother's ability to breastfeed (ACOG, 2021). For example, in the event a nurse offers to keep the baby in the nursery for the night and give the baby a bottle so that the mother can sleep (ACOG, 2021).
Problems with access to donor milk:
Sometimes breastfeeding may not be possible or supply is inadequate for the infant’s needs during hospitalization, or a NICU stay and donor milk may be recommended. Variations in supply, cost, and distribution of donor milk may cause difficulty with using this method (ACOG, 2021). Formula is often more readily available or covered by insurance in hospital settings and may be recommended over donor milk (ACOG, 2021).
While "breast is best" is often touted by healthcare professionals and most women are aware that breastfeeding benefits infants, many women do not understand the extent of breastfeeding benefits and may even feel that modern infant formula is equivalent to human milk (ACOG, 2021).
Additionally, many women do not realize that successful breastfeeding is a skill that must be learned by both mother and baby and takes some time to establish (ACOG, 2021). Early feeding struggles may discourage mothers who feel that not immediately "getting it" means something is wrong or that they will never adjust, so they give up. Current evidence suggests higher levels of formal education are positively associated with increased breastfeeding rates (ACOG, 2021).
Social norms:
The popularity of formula in the mid to late 20th century means several generations of women have never breastfed, making bottle feeding and formula the norm for many households (ACOG, 2021). A woman who decides to breastfeed may be met with a line of relatives who have no advice or support for her, having never breastfed themselves. Poor adherence to The Code also means that formula advertisements and samples are readily available to pregnant women and may influence their opinions early on about what is "popular,” “normal," or what "most" women are doing to feed their babies (ACOG, 2021).
Low income or social support:
Women of lower socioeconomic status are less likely to breastfeed and may have diminished access to support systems (ACOG, 2021). Women with breastfeeding friends and family in their circle are much more likely to breastfeed their children. A family's lack of support may be because family members did not breastfeed themselves or attempted to but stopped before meeting their original goals. Family members may not value breastfeeding because they do not understand the health benefits or want a role in feeding and bonding with the baby (ACOG, 2021).
Embarrassment:
While the last few years have seen an increase in acceptance of public breastfeeding and support in legislation for mothers to feed their infants anywhere they choose, the damage of decades of shaming women for “public indecency” and society's view of breasts as sexual objects has created a sense of embarrassment for many women who might need to feed their infants in a public place (ACOG, 2021). The increased available spaces for breastfeeding and the normalization of breastfeeding through social media and pop culture are steps in the right direction. However, for many women, the stigma is still difficult to overcome (ACOG, 2021).
Employment issues:
Maternity leave in the United States is notoriously short, if present at all, compared to other countries (ACOG, 2021). The lack of quality time at home with a new infant can greatly impact a woman's ability to establish breastfeeding and build an adequate supply. Even for those women who are successful in breastfeeding while on leave, returning to work means that she must find the time to express milk and keep up with her infant's feeding demands while separated from her child. Even with a law mandating dedicated lactation breaks and spaces at work, women may feel pressured to skip pumping breaks instead to prioritize job performance. States like California and New Jersey with paid family leave policies demonstrate increased breastfeeding rates (ACOG, 2021).
Cultural/Racial disparities:
It is also important to note the need for racially sensitive practices to help mothers breastfeed successfully. Black women are disproportionately affected by poor breastfeeding initiation and continuation rates due to a myriad of factors, including (ACOG, 2021):
Generational trauma from enslaved women being used as wet nurses
Lack of quality education about the benefits of breastfeeding
Lack of social support and healthcare support when Black women do attempt to breastfeed
In 2019, data indicated that 73.6% of Black women initiated breastfeeding in the hospital compared to 85.5% of white women (Chiang et al., 2021). Awareness of these disparities is important for all healthcare professionals working with lactating women, particularly those working in areas with large populations of Black women. Efforts for Baby-Friendly policy implementation, community support, and healthcare worker education and sensitivity should be at the forefront of maternal and child health efforts in these communities (Beauregard et al., 2019).
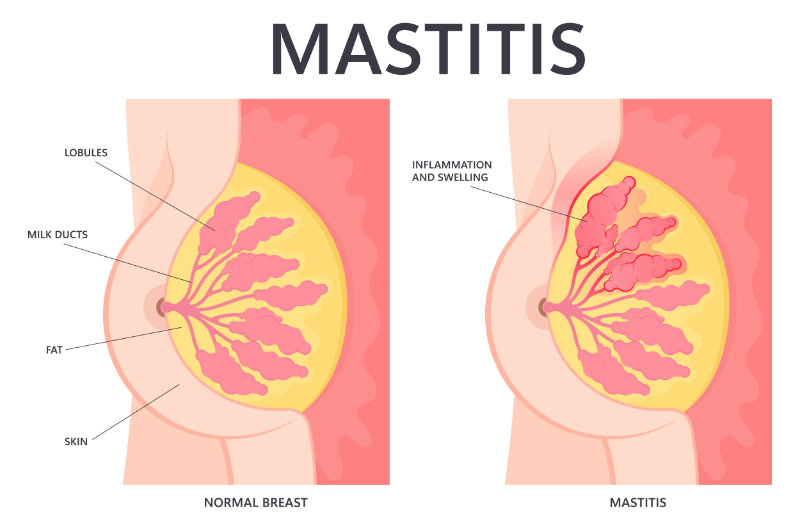
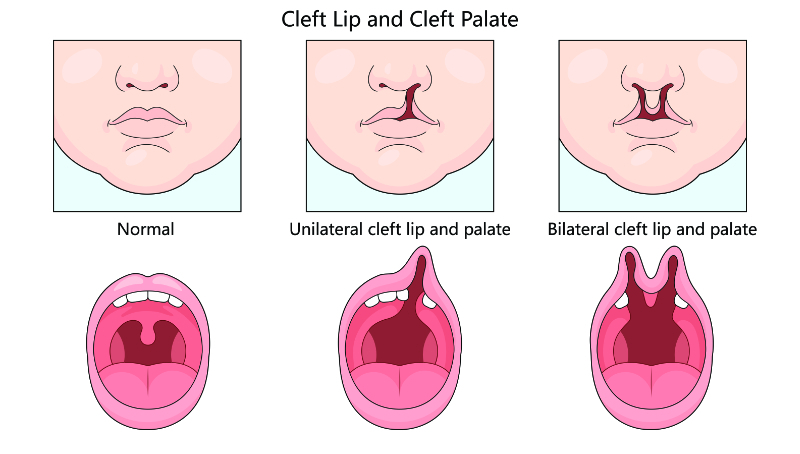
The early days of lactation may present many common problems, such as engorgement, nipple soreness or cracking, plugged ducts, mastitis, improper latch, and exhaustion in the mother. These issues are quickly addressed with minor adjustments and reassurance (worries over inadequate supply are typically unfounded, especially in the early days when colostrum in small quantities is entirely healthy and normal) (ACOG, 2021).
Actual problems with supply or oropharyngeal problems that inhibit a proper latch (such as cleft palate) exist. They must be addressed appropriately, but these issues are rare, and the majority of breastfeeding challenges can be successfully addressed by a skilled lactation professional (ACOG, 2021).
Complex medical issues:
Parents with complex medical issues may struggle with the physical demands of breastfeeding or may require much more assistance or support than their medically well or able-bodied peers. Mothers may worry that taking multiple medications will be harmful to the infant if they are exposed through breastmilk. Often, the actual drug exposure is low, and the benefits still outweigh the risks, so clinicians are encouraged to discuss a patient’s specific case with them and determine the best course of action.
Mental health issues:
Similar to complex medical issues, a mother’s mental health may also impact her desire to or ability to successfully breastfeed. Women experiencing postpartum depression or anxiety may struggle with the physical demands of breastfeeding, the impact on sleep, and the demands of being the primary caregiver (ACOG, 2021).
Women with a history of trauma, particularly physical violence or sexual abuse, may feel negative connections with the physical touch and bodily exposure of breastfeeding. Conversely, some women report feeling empowered or more connected to their bodies when breastfeeding and find it healing after a sexual assault (ACOG, 2021).
About 5-9% of women will also experience a phenomenon called Dysphoric Milk Ejection Reflex (D-MER) which causes a brief but intense period of negative emotions during let-down (Cleveland Clinic, 2023a). This can look like 1-2 minutes of intense unhappiness, sadness, self-loathing, dread, anger, anxiety or other unpleasant emotions (Cleveland Clinic, 2023a). Little is known about this condition, but it is believed to be hormonally linked and may be from a steep drop in dopamine during the surge in oxytocin with let-down (Cleveland Clinic, 2023a).
LGBTQ+ parents:
For members of the LGBTQ+ family, particularly transgender men, lactation may be linked to body dysmorphia and the decision whether to breastfeed may be closely linked with mental health considerations (ACOG, 2021). Transgender men may also desire to resume testosterone treatment after pregnancy or may have undergone breast reduction surgery, both of which could negatively impact their milk supply.
Transgender women may attempt to induce lactation with medications and nipple stimulation, but this is not always successful. Knowledge and respect for lactating patients’ gender identity and pronouns is also an important part of caring for this population (ACOG, 2021).
Substance use:
The effects of substances on breastmilk vary by specific substance and therefore, recommendations are also unique to the substance in question (ACOG, 2021). Illicit substances like methamphetamine or cocaine are complete contraindications to breastfeeding. However, mothers with an opioid use disorder who are currently stable on Medication-Assisted Treatment (MAT) drugs are encouraged to breastfeed as the benefits outweigh the risks (ACOG, 2021). Marijuana use during lactation is discouraged but not fully contraindicated. Mothers in recovery for drug or alcohol use are also encouraged to breastfeed if they would like to. It is important for clinicians to use current evidence and careful communication with these patients rather than arbitrary restrictions that may not be based in evidence (ACOG, 2021).
Incarcerated parents:
Many prisons and jails lack policies or designated spaces for breastfeeding or milk expression. For mothers who give birth while incarcerated or are lactating when taken into custody, this creates a disruption in milk supply. Even if support for milk expression is in place for incarcerated and lactating women, there is still the added challenge of milk storage and transferring the milk to the infant’s caregiver (ACOG, 2021).
Adolescent parents:
Teenage mothers are less likely to breastfeed (74%) compared to mothers older than 20 (up to 85%) (ACOG, 2021). Poor availability of social support and potential effects of breastfeeding on social relationships are both deterrents for young mothers who may already be struggling to adjust to parenthood during adolescence. For teen parents who are in school, there are likely to be inadequate facilities to pump or express milk. Young parents may also have minimal education and knowledge about the benefits of breastfeeding (ACOG, 2021).
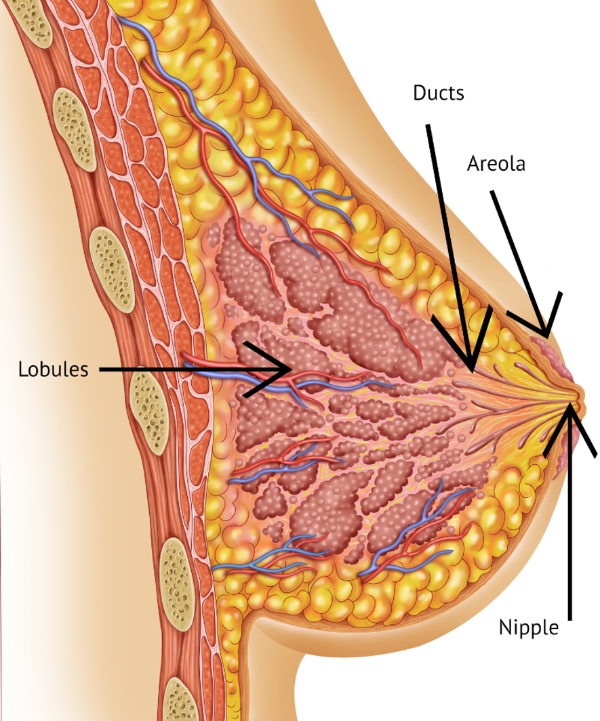
To provide high-quality support and care to breastfeeding women, healthcare professionals must first have a solid grasp of the physiology behind lactation. The anatomy of breasts includes two main parts, lobules and ducts (Mayo Clinic, n.d.) See image 5.
Image 5: Breast Anatomy
Lobules are clusters of tiny sacs called alveoli that fill with milk during lactation. The lobules are connected by small tubes called ducts which carry milk from the lobules to the nipple. Lobule development first occurs during puberty when estrogen and progesterone levels begin to fluctuate with menstruation.
Young women in their teens will have lobules that are small in size with few alveoli, known as Type 1 Lobules, and increase to slightly larger lobules with more alveoli, known as Type 2 Lobules, by the end of puberty if pregnancy has not occurred. During early pregnancy, the increased exposure to progesterone causes large clusters of alveoli, Type 3 Lobules, to develop, and the epithelial cells lining them mature, preparing to secrete milk (Pillay, 2023). Type 4 Lobules are fully mature in size and number during active breastfeeding and remain this way until the child is weaned.
All women experience lobule development once puberty begins, but only women who experience pregnancy will have lactogenesis. Lactogenesis is the process by which alveolar cells mature and secrete milk. Lactogenesis I, or secretory initiation, begins around 16-20 weeks gestation. The high levels of progesterone supplied by the placenta help mature the epithelial cells of the alveoli, and colostrum secretion begins in small amounts. Some women can even leak or express colostrum before delivery, though the ability to do this has nothing to do with breastfeeding success after delivery. Once the placenta is delivered after birth, there is a sharp drop in progesterone levels, accompanied by an increase in prolactin, cortisol, and insulin which stimulate lactogenesis II, or secretory activation, and the body begins to make an increased (and often overabundant) supply of milk around 2-3 days after delivery.
Lactogenesis II may be delayed slightly in women who have never lactated before, resulting in a lower initial milk volume or closer to 3-6 days for full milk volume to come in; this is completely normal (Pillay, 2023). This process may be interrupted by anything that disrupts the hormone response following delivery, such as retained placenta fragments, cesarean deliveries, diabetes, or difficult vaginal deliveries. Lactogenesis I and II are hormonally driven and occur whether or not a woman chooses to breastfeed her baby (Pillay, 2023).
Suppose a baby is put to breast and nipple stimulation occurs via suckling. Around postpartum day 10-14, milk production regulates and moves into lactogenesis III, maintained through a supply and demand process involving the hormones prolactin and oxytocin (Pillay, 2023). During lactogenesis III, the number and size of lobules reach their highest capacity, known as Type 4 Lobules. Nipple stimulation and emptying of the lobules stimulate the anterior pituitary gland to secrete prolactin, the hormone responsible for milk production. Nipple stimulation also triggers the release of oxytocin from the posterior pituitary. This hormone triggers the contraction of the tiny muscles around the alveoli, pushing milk from the lobules into the ducts and out through the nipple via the milk ejection reflex. Oxytocin release also provides mothers with a sense of calm and relaxation and increases bonding with the baby during feedings (Pillay, 2023).
Continued milk production becomes an autocrine function, dependent on supply (if the breasts are full or being emptied) and demand (if nipple stimulation continues). Prolactin secretion (and therefore milk produced) increases when the nipples are stimulated but decreases when the breasts are unemptied and pressure builds within the lobules (Pillay & Davis, 2023). Milk secretion is fastest when the breasts are empty; therefore, frequent or on-demand feeding is the best way to increase milk production. Breasts that are full or not being emptied completely or as often will produce milk at a slower rate (Pillay & Davis, 2023).
As long as milk removal and nipple stimulation continue, a woman will continue to lactate. Once milk removal slows or stops, such as with weaning, milk production drops off and eventually stops as well. Milk making epithelial cells within the alveoli die off, and the breast tissue shrinks back to mostly type 2 and 3 lobules until the next pregnancy; this is called lactogenesis IV(Pillay, 2023).
Table 2: Lactogenesis & Associated Breast Changes
Phases of Lactogenesis
Breast Changes
Lactogenesis I
Begins around week 16 of pregnancy. Epithelial cells mature and begin to secrete colostrum.
Lactogenesis II
Birth triggers a hormonal shift that increases the volume of milk that is produced, usually around 4 days postpartum.
Lactogenesis III
Milk production shifts to autocrine control and is based on supply and demand from around ten days postpartum until weaning occurs.
Lactogenesis IV
Milk production decreases, epithelial cells decrease in number, and breast tissue involution occurs.
For women in lactogenesis III, the ejection of milk occurs in a few stages, known as let-down. When a baby is not feeding, milk is simply stored in the lobules, awaiting ejection and impacting the pressure in the lobules and subsequent production (or lack thereof) of more milk (Cleveland Clinic, 2023c). Gentle squeezing with the hand, from the middle of the breast down toward the nipple may allow a few drops of milk to be expressed during this time.
Whenever a baby is put to the breast, or a pump is attached, nipple stimulation triggers a release of oxytocin and the small muscles around the alveoli contract, moving milk through the ducts and towards the nipple. This stimulation may take 1-2 minutes to reach a point where the oxytocin levels are high enough for milk ejection (Cleveland Clinic, 2023c).
When this first occurs, known as let-down, there may be a pins and needles sensation within the breasts and milk may spray out forcefully for a few seconds. Not all women experience the pins and needles sensation during let-down, however. If a letdown is too forceful, the infant may cough or choke and momentarily break the latch.
After a few moments, the force of the let-down subsides, and milk should begin to flow in steady droplets. When a breast is nearly empty, the droplets will cease flowing on their own, though the pump or baby may still be able to draw out more with sucking (Cleveland Clinic, 2023c).
Besides a proper understanding of the normal lactation process, it is extremely important to gather a thorough history of each mother's history surrounding her general health, pregnancy, and delivery to properly care for her individual breastfeeding needs.
Many important factors may affect a woman's breast anatomy, hormone secretion, and progression through the phases of lactogenesis and may affect her plan of care. Historical information that should be assessed should include (Wagner, 2024):
The mother's medical history and current medications she may be taking need to be addressed. Maternal conditions that may negatively impact milk production and breastfeeding can include:
Diabetes
Obesity
Thyroid imbalance
Polycystic ovary syndrome (PCOS)
Hypertension
Mental health conditions such as depression, anxiety, post-traumatic stress disorder (PTSD), or mood disorders such as bipolar I disorder, that are diagnosed before or after delivery can also present unique challenges to breastfeeding success (Wagner, 2024).
Medications, particularly any beta-blockers, antihistamines, corticosteroids, methergine, antipsychotics, or hormones including hormonal birth control due to their potential drying effects or disruption of hormones necessary for milk production need to be asked about as well.
It is important to ask about a history of any breast problems or surgical procedures that have impacted a woman’s breasts. This might include mastitis, breast augmentation, breast size reduction, or potentially cancer. Any changes to the breast anatomy, including tissue removal or presence of scar tissue can impact breastfeeding.
The ability to breastfeed after a breast augmentation depends on the placement of the implant as well as the incisions. Implants placed below the muscle of the chest have less of an impact than implants placed above the muscle which may come in more direct contact with lobules and ducts. For both augmentation and reduction, incision placement may impact breastfeeding. Sometimes incisions are made underneath the breasts or even near the axilla, which has less of an impact on future breastfeeding. Other times, incisions are made around the areola or nipple and may sever the ducts or nerves of the nipple. Sometimes the nerves will heal and regenerate over time but not always. A lack or reduction of nerve endings to the nipple reduces the response to nipple stimulation and may reduce milk supply.
The mother’s past obstetrical history should be reviewed including all past pregnancies as well as the most recent one, of course. When asking about past obstetric history, make sure to ask about specific dates, outcomes, and about any complications that occurred (Kesavan, 2024).
The most basic components of obstetrical history include gravidity and parity (Kesavan, 2024). Gravidity is the number of confirmed pregnancies that a woman has had. Parity is the number of deliveries that a woman has had ≥ 20 weeks of gestation. When asking about parity, it is important to ask about the number of term deliveries (≥ 37 weeks) and how many preterm deliveries (≥ 20 and < 37 weeks) she has had. When asking about past abortions, it is important to remember that “abortions” include pregnancy losses that were spontaneous before 20 weeks, induced abortions, ectopic pregnancies, or a rare complication of molar pregnancy (mass or tumor develops in the uterus instead of an embryo) (Kesavan, 2024).
The history of the labor and delivery experience, from beginning to end, with this infant should be high on the list of priorities for this conversation. It is a good idea to ask about medications that were administered during labor, the length of labor, the delivery method, and if there were any complications.
Labor medications that may have an impact on breastfeeding can include:
Opioids like fentanyl or meperidine: These are medications that are sometimes given for pain, and can cross the placenta, causing drowsiness and ineffective latch in the infant until the medications wear off.
Oxytocin (Pitocin): This is often given to augment or induce labor. When it is given at high doses, it can impact a mother’s natural release of oxytocin and sometimes impact or delay the onset of lactation.
Prostaglandins: These are used to induce labor, which can negatively impact breastfeeding initiation.
While all of these medications can have some impact on breastfeeding, none of these medications are actually contraindicated for breastfeeding. It is more important to note their use when assessing a mother-baby dyad than to debate their necessity for use during labor and delivery.
Some studies suggest that prolonged labor may be inversely related to duration of breastfeeding. Mothers may be stressed or exhausted, or have experienced intense or prolonged pain, all of which can delay or cause difficulties with initial breastfeeding and ultimately long-term breastfeeding goals.
Deliveries by cesarean section may be negatively impacted for breastfeeding success, as these deliveries have lower initiation rates and delayed time for the first feeding. Separation after delivery, resistance from operating room staff or protocol about immediate skin to skin and breastfeeding, as well as recovery time for mothers and their abdominal incisions all make breastfeeding more challenging to start. For mothers who are supported through these initial challenges, however, there is not typically a long-term impact.
Complications during delivery can also negatively impact breastfeeding initiation due to pain, stress, or health concerns that impact the ability of mothers to position and latch their infant. Potential complications not already listed include postpartum hemorrhage, fetal distress, shoulder dystocia, perineal tears, and use of general anesthesia.
It is a good idea to discuss past breastfeeding experiences for the mother. Questions that can be asked can include how many other children she has breastfed, what those experiences were like, and how long she breastfed for.
Any past experiences with breastfeeding are likely to impact, either positively or negatively, how a mother feels about breastfeeding this time around and her overall confidence level. A mother who has successfully breastfed before is more likely to know what to expect, trust the process, and feel confident in her ability to learn a new relationship with this infant. A mother with a negative experience or who did not meet her goals last time is more likely to feel discouraged or unsure from the very start or may take any challenges as confirmation that she is unable to successfully breastfeed.
It should go without saying that asking specific questions regarding the infant’s birth history is important. Inquire about the infant’s gestational age at birth, their weight, if a NICU stay was necessary and what it was comprised of, and about any complications.
Premature or low birth weight infants may be more likely to struggle with initial latch and establishing lactation or may have more intense monitoring for weight gain that puts pressure on the mother to establish lactation quickly or supplement.
Any complications that require the newborn to be separated from the mother, including NICU admission, also makes establishing breastfeeding more difficult due to the inability to room-in and the need to work around various monitors and equipment when trying to position and latch the baby.
Ask about the feeding of an infant up to this point. Ask if her child was put to the breast within the first hour of birth, about the support she received in the hospital, about any formula/bottles/pacifiers that have been offered to the infant up to this point, about mom’s understanding of infant hunger cues, and about how often feeding on demand occurs.
It is important to identify what the caregivers currently know or believe about breastfeeding, both correct and accurate information as well as any inaccurate information or misconceptions.
This is also a good place to assess who the mother’s support person(s) are and their own attitudes and knowledge about breastfeeding. Is the mother being supported and encouraged or is her partner or family unsure or unsupportive of breastfeeding? Is she being given outdated or incorrect information from family about expectations or feeding patterns? Is there any shame associated with breastfeeding? What are the cultural considerations?
Note: Remember to utilize the goals and principles of trauma-informed care (TIC) when asking these questions because of the highly sensitive nature of what some of the answers might be, particularly those that relate to obstetrical history or prior birth trauma. It is important to use good communication skills, remain respectful, establish trust, and demonstrate cultural sensitivity so as not to re-traumatize a woman who has experienced any form of trauma surrounding her history, pregnancy, and birth experience(s) (CDC, 2018).
Table 3: Factors That Can Reduce Supply or Breastfeeding Success
Special effort should be made for those professionals who work directly in labor and delivery to support the Golden Hour when possible. As we talked about a bit above, Golden Hour is when an infant is placed skin-to-skin with its mother as soon as possible after birth and left uninterrupted to bond and feed (La Leche League, n.d.-b). Ideally, this occurs within the first hour after birth, if not immediately.
Skin-to-skin contact has a calming and regulatory effect on both the infant and mother and helps stabilize vital signs for both after delivery. If left alone, infants will go through a period of being highly alert and calm and will even scoot or "crawl" across a mother's chest or abdomen to find the breast and latch (La Leche League, n.d.-b). This first feeding is incredibly important to coincide with the hormone shifts experienced by the mother after birth and help move towards lactogenesis II and give the baby that first colostrum feeding before they enter a period of deep sleep following birth. It is much easier to help coach new mothers in breastfeeding when the infant is alert and cooperative, and this is the perfect time to get the infant to start feeding and stooling for optimum health (La Leche League, n.d.-b).
For most other healthcare professionals, you will encounter breastfeeding women and their babies later in their breastfeeding journey, usually hours, days, or weeks after birth and those first initial feedings. Lactation may already be affected by perceived problems, ineffective habits/practices, and frustration or discouragement in the mother (Wagner, 2024). It is important to approach the process with patience and optimism and remind mothers that this “natural act” does not necessarily occur naturally. She and her baby are learning and practicing together to get it right. Assisting mothers during the first two weeks of lactation affords the most opportunity to help establish good practices. Still, the latch and mother-baby relationship can be adjusted and improved at any time in the breastfeeding journey. All interventions should be made with gentle suggestions and guidance rather than abrasive action that may cause a mother to feel she is not in control or may violate her personal space. Always ask permission before touching a woman's breast or her baby to adjust positioning (Wagner, 2024).
The first few weeks postpartum can be a very emotionally volatile time for mothers and their families, so sensitive communication is particularly important. Qualities of positive communication with this population include:
Being positive and affirming: Provide praise for the decision and commitment to breastfeeding.
Asking open-ended questions: Allow mothers time to talk openly about their experiences and concerns.
Using non-judgmental language: Any pressure or criticism should be avoided, including absolutes like “always,” “never,” “should,” or “must.”
Validating feelings: Statements like “That sounds very stressful,” or “That is really difficult” provide validation for patients and make them feel heard and understood, strengthening the rapport and making them more likely to trust advice from you throughout the relationship.
Focusing on the baby’s needs: Discuss the baby’s growth and development and their feeding needs.
Offering practical advice: Tangible and actionable advice about positioning, latching, milk supply, and common problems are discussed in more detail below.
Respecting privacy: Do not ask overly personal questions, allow women to remain as covered as they would like, and make sure only people they are comfortable with are in the room during a feeding.
Additionally, there are communication patterns that should be avoided when working with breastfeeding women. These can include:
Giving unsolicited advice: Do not offer solutions or blanket statements without knowing the specific details of a patient’s unique situation.
Making comparisons: Avoid comparing their unique breastfeeding journey to that of other patients or even yourself.
Pressuring: If a patient chooses to wean or supplement with formula, you should respect this decision and not pressure them to continue with breastfeeding.
Making assumptions: Ask questions to assess a patient’s unique needs, but do not claim to understand their unique situation or feelings.
Once historical data has been collected, the healthcare professional should observe a feeding. Ideally, the area for lactation support will be private, relaxing, and have comfortable seating. Watch how the mother interacts with her baby. Is she nervous or uncomfortable handling them? Does she seem stressed or relaxed, frustrated or patient? Assess a mother's understanding of hunger cues; rooting, sucking on hands, alert but quiet, etc. Teach mothers that crying is a late sign of hunger and that a frustrated and very hungry infant will be much more difficult to get to latch effectively (Howland, 2024; La Leche League, 2023).
Once you are ready to assess a feeding, allow the mother to get comfortable and position the infant. You may even hand her the baby once she is seated comfortably. There are various possible positions, and mothers should try different ones to see which they find most comfortable. Regardless of position, a baby should be turned towards the mother, with the ear, shoulder, and hip aligned to effectively achieve a proper latch and transfer of milk (Howland, 2024; La Leche League, 2023). Common positions that you can witness or teach mom about are outlined below.
Cradle Position: One of the most common breastfeeding positions used in the first weeks, the cradle position, is when the baby's head rests on the mother's forearm on the same side as the breast he is feeding on, and her arm and palm cradle his back. The mother's opposite hand supports her breast in a C-shape and helps guide it into the baby's mouth (La Leche League, 2023).
Image 6: Cradle Position
Cross Cradle Position: This is a variation of the cradle position, and many mothers find it useful during the first weeks as well (Howland, 2024). The baby should be supported on a pillow across the mother's lap. Using the hand opposite the breast, the baby is feeding on. The mother should support the baby's head and neck by placing her hand in a C-shape behind his neck near the ears. The hand on the same side as the breast should be holding the breast (La Leche League, 2023).
Image 7: Cross Cradle Position
Clutch or Football Position: This position is good for mothers who have had a cesarean section, as it keeps the baby off the mother's abdomen. The baby should be positioned along the mother's side, with their legs and feet tucked under the mother's arm, with hips flexed and soles of their feet pointing upward to avoid the baby kicking off the chair or couch behind him. The baby's feet are on the mother's side on the same side, and the mother can support his head with the same-sided hand. The mother's opposite hand can then support the breast (La Leche League, 2023).
Image 8: Clutch or Football Position
Side-lying Position: This position may require more practice, and many mothers may not find it useful until they feel they have mastered the other positions. This position may be more comfortable and help mothers rest during nighttime feedings. Mother and baby should both lie on their side facing each other. The baby should be cradled in the mother's bottom arm and fed from the bottom breast. The baby should have hips flexed, and the mother may be more comfortable with a pillow between her legs or behind her back. She can use her top hand to support the breast if needed (La Leche League, 2023).
Once a comfortable position for mother and baby has been achieved, it is time to assist with the latch.
A deep latch is necessary for the proper transfer of milk and to avoid damaging the skin of the nipple. Since the tongue is in the bottom half of the baby's mouth, the deepest latch is achieved by aiming the nipple slightly higher, in the top half of the mouth, pointing upward towards the roof of the baby's mouth (Howland, 2024).
Have the mother tickle the baby's mouth with the nipple until he opens his mouth wide. Allow the baby to tip his head back and bring the baby close to the breast. The baby's chin should first touch the breast, and then, once he is latched, his nose should almost touch the breast as well. The infant’s lips should be flanged outward, with the mouth opened to a wide angle (ideally around 140°F).
Initially, the baby will suck quickly without swallowing while he positions the nipple and waits for the milk let-down to occur. Once the milk is flowing, the baby's sucking should slow, and you will be able to hear him swallowing, audibly. The baby's jaw should move in a rocker motion, not up and down, and he should suck in irregular bursts of around two sucks per swallow. When the nipple is removed, it should still be rounded and a similar shape to before the feeding, though it may be elongated. If the nipple looks pinched, flat, or asymmetrically slanted like a tube of lipstick, this indicates an ineffective latch and corrections need to be made in order to prevent discomfort and potential nipple injury for mom (La Leche League, 2023). Please see the image below to help you understand what a proper latch should look like.
Image 10: Proper Latch
If the latch feels uncomfortable at any point, the mother should be instructed to break the latch and start over. This can be done by simply inserting a finger into the corner of the baby’s mouth, slowly pushing down to separate and break the suction (La Leche League, 2023). Let the mother know that practicing and correcting an uncomfortable latch is completely normal and how good breastfeeding habits are achieved. There is no shame in it taking time to get it right. Allowing a baby to continue with an improper latch will only lead to nipple trauma and more pain in the long run (La Leche League, 2023). If a baby is overly hungry and too frantic to cooperate with repositioning, a small amount of milk can be given via a bottle or syringe to soothe the infant enough to proceed with the rest of the feeding at the breast.
During the early weeks, infants may feed for 10 to 15 minutes on each side, making full feedings last a half hour or more. Time between feedings is measured from the start of one feeding to the start of the next, so if 45 minutes of that time is spent at the breast, it can make new mothers feel that they are breastfeeding extremely frequently, however this is normal. As infants grow and become more efficient, they may shorten their feedings to 5-10 minutes on each side, finishing a feeding in only 20 minutes or less.
Even when a proper latch has been achieved, many mothers worry that their infant is not feeding properly or getting enough milk. When an infant takes a bottle of formula or expressed milk, it is easy to visualize just how much milk they have taken. However, the same assessment is not possible when feeding at the breast. There are many other ways to assess that an infant is effectively transferring milk and getting adequate nutrition. Mothers should be cautioned to assess these factors rather than getting caught up in knowing "exactly how much" an infant is eating each feeding. These assessments are also useful for healthcare professionals who are monitoring the infant's health and ensuring proper growth in the first few weeks and months of life. Rather than assessing feeding by volume, healthcare professionals might ask “how long” an infant feeds on each breast and how often they are feeding. Additional assessments can include (Howland, 2024; La Leche League, n.d.-a):
Urine output: During the first day or two of life, newborns may not produce much urine, but after that period of time, well-hydrated infants should have 8-10 wet diapers per day.
Stool transitioning: During the first few days of life, an infant's stool transitions from tarry meconium to soft, yellow, and seedy. This transition is a good indication that the baby is transferring adequate milk. By four days old, most infants are having several stools per day. Around one month of age, the intestines begin to mature, and breastfed infants may decrease the number of stools per day. This is because breastmilk is so high in nutrient content that there is very little waste. As long as stools are soft, this is not cause for concern.
Satisfied in between feedings: Infants should be relaxed and sleeping often in the first few weeks of life, waking only to feed and for intermittent periods of alertness. Sleeping or being content after feedings are positive signs that the infant's hunger has been satiated for the time being. Often it is observed that an infant will begin feeding with a clenched fist but finish a feeding with a relaxed and open hand. While it is recommended that infants be fed at least every 3 hours (or 8-12 times per day), breastfed infants certainly can be fed more often if they are exhibiting hunger cues, and feeding on demand is an important part of establishing supply. Mothers should be reassured that wanting to eat often, but being satisfied between feedings, is perfectly normal and not a sign of inadequate supply.
Weight gain: It is normal and expected for all newborns to lose some weight within the first few days of life, typically no more than 10% of their birth weight. After the first week, most infants begin gaining weight at a rate of around an ounce per day and should be back to their birth weight by two weeks of life. Adequate weight gain is a good indication that infants are getting enough to eat at the breast. Tracking infant growth on a standard growth chart is generally practiced in pediatric offices and can be useful as the baby grows. However, make sure to pay close attention to the type of growth chart being utilized. CDC growth charts are made using decades of data from primarily formula-fed infants in the United States, who grow at different rates than breastfed infants (typically bigger weights more quickly). WHO growth charts compile data from children worldwide, where breastfeeding is much more prominent, so breastfed infants should be plotted on a WHO growth chart for a more accurate representation of their growth in relation to the "norm".
It should be noted that pumping can be used to relieve discomfort from engorgement, start storing milk for a return to work, or allow others a chance to feed the baby once breastfeeding is well established. Still, pumping is not an accurate depiction of supply. Often pump flanges are ill-fitting, or pump settings are not being used correctly. Mothers are not even aware of this, resulting in an inaccurate representation of how much milk can be removed from each breast. Further, the average pump is not as efficient and does not elicit the same hormonal response from the mother as directly feeding her baby. Mothers should be cautioned to observe their infants for the above signs of adequate feedings rather than using pumped milk amounts as a sole gauge to quantify their supply (Howland, 2024; La Leche League, n.d.-a).
Whether for medical complexities in the mother or infant that make breastfeeding difficult or impossible, or personal preference, there are some mothers who choose to feed their infants breast milk through exclusively expression/pumping and bottle feeding. This still offers the many benefits of breastmilk to the infant as well as protective benefits of lactation to the mother but does come with its own unique considerations and challenges in order to keep milk supply up and maintain lactation long term.
Mothers who plan to exclusively pump will need to carefully consider the equipment they choose. There are two main forms of pumps, manual or electric, and they serve different needs. Suction strength and motor life of the pump should be considered since the device will be used very frequently.
Battery operated or cordless pumps are beneficial for increased portability and convenience. Some are even “wearable” and fit inside the bra to allow women to pump discreetly and while completing other tasks.
Other helpful equipment includes hands-free pumping bras, storage bags, and replacement parts. Backup options like manual pumps should be considered in case of problems with an electric pump.
Flanges are the funnel-shaped part of the breast pump that directly sits over the areola and nipple. See the image below. They need to be the proper size and fit in order to comfortably express the most milk possible. The nipple should be centered in the flange and be able to move back and forth freely without rubbing against the sides of the flange. Typically, only a small amount of areola is drawn into the flange during pumping and if more is being pulled in, the flange size may be too large. The fit should be snug and sealed but not cause any pinching, pain, or skin breakdown.
Image 11: Breast Pump
All pump parts that come in contact with the breast or breast milk need to be cleaned with warm soapy water each time after pumping.
In order to build an adequate milk supply, pumping will need to mirror the infant’s feeding pattern in the beginning, ideally at regular intervals and about 8-12 times every 24 hours. Just like with feeding patterns, pumping does not have to be at rigidly spaced intervals, however it is necessary to pump and empty the breasts around every 2-3 hours in order to stimulate and maintain milk supply. A common misconception is that mothers can delegate nighttime feedings to their partner or another caregiver and have uninterrupted sleep, when in reality, they will still need to wake at least every 3 hours to pump or their supply will dwindle (Sheldon & Williams, 2020).
After 3-4 months, the pumping schedule can be spaced out a little further, instead pumping every 4-5 hours, just as the infant is spacing their time between feedings as well.
Exclusively pumping is a major time commitment and can take anywhere from 15 to 45 minutes to empty both breasts completely. Some mothers find that they prefer shorter, more frequent sessions, while others prefer fewer, longer sessions. Mothers should be encouraged to keep track of pumping times and milk output to help identify what works best for each individual.
Without the skin-to-skin contact of the baby to encourage oxytocin release and let-down, some mothers find it helpful to look at pictures of their baby or have a small article of clothing (like an infant sock) that smells like them. For moms who have easy access to their babies, even holding them or being near them during a pumping session can help.
For mothers of NICU babies who are not yet eating by mouth due to prematurity, it may be an option to participate in skin-to-skin with their baby and then immediately pump afterwards, to help in maintaining or even increasing supply. Other than making sure mom is hydrating, other ways to optimize milk volume can include things such as warm compress, gentle massage, or even a special nipple stimulation setting on the pump for 1-2 minutes before pumping that can also help with oxytocin release and milk ejection reflex.
A calm, quiet, and low-stress environment is also helpful, and mothers should be encouraged to relax with music, reading, or watching tv while pumping.
For infants fed at the breast, the amount of milk intake varies from feeding to feeding, and this may be the same for pumping. On average, infants will consume around 750-1040 mL of breastmilk per day, depending on their age, so this is a good range to aim for when pumping (Sheldon & Williams, 2020).
Paced feeding can mimic breastfeeding and helps to prevent overfeeding, fussiness, and gas in infants. In order to pace a feeding, the infant should be held at around a 45° angle and be given control over drawing the bottle nipple into their mouth, taking frequent breaks, and using a slow or regular flow nipple to allow them more control over the pace of the feeding (Sheldon & Williams, 2020). For premature infants, preemie nipples are available.
While quantifying the volume of breastmilk the infant takes while breastfeeding is difficult, when feeding via bottle, it is important to know the appropriate amount an infant should be taking, based on their age. Because breastfeeding mothers often fear they are not producing enough for their child, especially in the first couple of weeks, it is very helpful to educate them about the approximate size of babies’ bellies to reduce quantity-related anxieties. The following chart is a helpful tool to give you a better idea of how big an infant’s stomach is and about how much pumped breastmilk they should be consuming in the first few weeks. Remember, that this quantity can vary with each child and should only be used as a general estimation.
Expressed milk should be stored in bags specifically designed for breastmilk storage, or plastic or glass food-grade containers with tight fitting lids (CDC, 2023). Freshly expressed milk may be kept at room temperature (77°F or cooler) for up to 4 hours. It can be stored in the refrigerator for 4 days, after which point it should be frozen. It is ideal to use frozen milk within 6 months, but it can still be safely used as much as 12 months later. It is recommended to freeze it 2-4 oz at a time to avoid wasting milk as it must be used within 24 hours once it is thawed. Warmed or room temperature milk must be used within 2 hours and should never be refrozen(CDC, 2023).
Table 5: Breastmilk Storage Guide
Freshly Pumped Breastmilk
Thawed (Previously Frozen) Breastmilk
Room Temperature (77°F or cooler)
4 hours
1-2 hours
Refrigerator (40°F)
4 days
24 hours
Freezer (0°F or lower)
Ideally 6 months, max 12 months
NEVER REFREEZE
(CDC, 2023)
It is important to note that it is not advised to mix freshly expressed breastmilk with already cooled or frozen breast milk because it can increase the temperature and potentially rewarm the older stored milk (CDC, 2023). It is recommended to allow fresh breastmilk to completely cool prior to combining it with previously cooled breast milk samples. The reason for strict guidelines for breastmilk storage rules is because the properties to slow the growth of bad bacteria that breast milk has begin to decline if it is not properly stored. Proper storage is required to prevent bacterial growth to ensure that breastmilk remains safe and of the highest quality for the infant (CDC, 2023). It is helpful to note and label each pumping product with the date and time that that sample was pumped to easily keep track. Pumped breastmilk should be discarded if it is past its expiration date at the temperature in which it is being stored.
Exclusively pumping can be very labor intensive and draining. It does allow mothers some flexibility with feedings and promotes bonding of other caregivers with the baby, but it can be physically and mentally demanding. Problems like pump malfunctions, spilled or spoiled milk, plugged ducts, and mastitis can all contribute to feelings of guilt and frustration (Sheldon & Williams, 2020). Support groups, even online, for exclusively pumping mothers may be beneficial for patients who are struggling with this balancing act and want to connect with others sharing similar experiences. Pumping mothers are no less than breastfeeding mothers and should be very proud of the work they put in to provide nutrition for their baby!
Even mothers who have established a consistent milk supply might occasionally see sudden dips in her supply. A breast pump can be used to help to increase milk supply as well. One such method of increasing milk supply via pump is known as “power pumping”. While regularly pumping on a schedule is very effective in maintaining and even increasing supply, when necessary, power pumping can help in the case that women are not seeing the results as quickly and as effectively as they are needing for their baby and their situation (Pregnancy Birth & Beyond, 2020).
Power pumping is a pumping technique that is meant to mimic the frequent feeding of a baby who is experiencing a growth spurt and/or requiring cluster feedings (Higuera, 2019; Pregnancy Birth & Beyond, 2020). The action of more vigorous, more frequent suckling triggers the release of prolactin from the anterior pituitary gland to tell the body to make more breastmilk (Pregnancy Birth & Beyond, 2020). It is a short-term solution to increase breastmilk supply and should not replace normal pumping or be continued long-term (Higuera, 2019; Pregnancy Birth & Beyond, 2020; Lansinoh, 2018).
To power pump, the general guidelines are to pick one hour a day (8 am every morning) to dedicate to power pumping and repeat this one-hour session at around the same time each day, for between 3-7 days consecutively (Pregnancy Birth & Beyond, 2020). The pumping pattern that is most often used is (Pregnancy Birth & Beyond, 2020; Higuera, 2019; Lansinoh, 2018):
Pump for 20 minutes
Rest for 10 minutes
Pump for 10 minutes
Rest for 10 minutes
Pump for 10 minutes
End of power pumping session
With the action of repeatedly emptying the breast, it signals to the body to make more breastmilk, more quickly. Again, standard routine pumping should be done for the rest of the pumping sessions throughout the day. Some women will experience an increase in their milk supply within 48 hours, whereas others might take a few more days (Pregnancy Birth & Beyond, 2020). It is important to note here that power pumping can take time to work. It also may not work for everyone (Higuera, 2019).
Some women find it more effective to do shorter bursts of pumping (5-10 minutes), others prefer to pump for 5 minutes and then rest for 5 minutes, others wish to repeat the power pumping schedule for more than one hour a day, and others find it more effective to spend a weekend attempting to increase their supply power pumping, occasionally termed a “power pumping boot camp” by lactation professionals (Pregnancy Birth & Beyond, 2020). Regardless of the exact algorithm that is used, it is typically only needed for a couple of days to see a positive result and a normal pumping routine can be resumed until milk supply might need another kick start again in the future.
Whenever a mother is ready to stop breastfeeding, even when exclusively pumping, weaning needs to take place gradually to avoid blocked ducts and mastitis. This can be done by gradually reducing the length of pumping sessions by a few minutes at a time and also increasing the intervals between pumping sessions. These gradual changes should take place over a period of weeks (Sheldon & Williams, 2020).
One of the biggest determinants for a woman meeting her breastfeeding goals is the support she receives, particularly when encountering problems. Healthcare professionals play an important role in providing that support and helping women navigate common issues that may arise during a breastfeeding journey. Some of the most common problems and their solutions are listed below.
Some soreness in the early days is normal, but persistent pain or cracked and bleeding nipples are typically due to improper or shallow latch and will continue to worsen if the latch is not corrected (Wagner, 2024). Observe a feeding and identify the latch aspects that need adjustment and coach the mother through how to do this. Encourage her to check the latch every feeding until good habits are established.
Nipple cream emollients like lanolin or MediHoney ® can be applied to cracked or sore nipples after feedings. Breasts should be washed with warm water, avoiding fragrances or harsh soaps that may be irritating or drying (Wagner, 2024). Breast shells (not the same as nipple shields) can be applied in between feedings to keep clothing from chafing on the nipples. Encourage mom to try different feeding positions throughout the day so that the infant's gums rotate where they are coming in contact with the nipple and not irritating the same spot each and every feeding. With these methods, mothers will typically see improvement in just a few days, but it is important to continue nipple care for 2-3 weeks for full healing to occur (Wagner, 2024).
First, remind mothers that the size and shape of the nipple are mostly irrelevant once the baby takes breast tissue into his mouth. With a proper latch, the baby should pull the skin of the nipple and breast into the back of the mouth, forming a teat and sucking milk out that way, regardless of nipple shape (La Leche League, 2022). However, learning how to draw the nipple out and properly latch can still be a learning curve for newborns.
Some methods to help mothers elongate their nipples before feeding include wearing breast shells inside the bra, pumping before feeding, and nipple stimulation (La Leche League, 2022). Breast shields are a potential temporary solution that fit more readily into the infant’s mouth and provide a supportive shape for the nipple beneath. Because they take some of the work out of a proper latch, they can create habits in the infant that are difficult to break. They are also another item that must be cleaned and poses a risk for contamination and infection like thrush. While useful in some situations, nipple shields do have their limitations and should not be used routinely or as the first solution that is offered (La Leche League, 2022).
Sometimes, the milk flow becomes blocked within the duct, and the breast may become red, tender, or have a hardened area; this is referred to as a plugged duct. Usually, gentle massage, warm compress, drinking water, and frequent feedings (and trying different positions for different suction angles and milk flow) will clear a plugged duct up quickly.
Sometimes, a plugged duct or blockage can persist, and an entire section of the breast becomes affected, resulting in increased tenderness and redness. This is known as mastitis.
Image 12: Mastitis
Antibiotics used to be routinely recommended for mastitis, but recent updates from the Academy of Breastfeeding Medicine (ABM) are more conservative, focusing on decreasing inflammation and pain by recommending feeding on demand, applying cold compresses and NOT hot compresses, and medications like ibuprofen (Mitchell et al., 2022).
Mothers may pump for comfort to relieve engorgement pressure but should be discouraged from pumping excessively or performing deep massage as this does not resolve mastitis more quickly and may actually worsen inflammation (Mitchell et al., 2022). Current evidence suggests that the disruption of normal breast colonization with the use of antibiotics may actually worsen mastitis or at the very least contribute to antibiotic resistance and the development of “superbugs.”
Even if blood or drainage is in the breast milk, often affecting the color, it is safe for the infant to continue feeding, and avoiding feeding on that side may worsen the engorgement or even lead to an abscess (Mitchell et al., 2022). Systemic symptoms like fever, chills, and body-aches, as well as redness and inflammation that are worsening, may indicate a true bacterial infection and evaluation by a healthcare professional and possible antibiotic treatment may be warranted (Mitchell et al., 2022).
When a breastfed infant does not gain well, healthcare providers must strike a balance between giving the baby adequate nourishment and working to increase the mother's supply. Supplemental feeds may be necessary, and healthcare professionals can help the mother commence pumping to support her supply to work toward providing all the breastmilk her infant requires for good growth. Failure to thrive and insufficient milk are also complex problems that typically require collaboration between primary care providers and lactation professionals.
When healthcare providers suggest supplemental feedings for infants, it is important to advise the mother to continue to put the infant to the breast at each feeding before providing the supplement. Pumping then after putting the baby to breast is especially important if the infant does not drain the breasts well. The mother must try to simulate the work of the baby with pumping in order to stimulate the nipples and continue establishing a sufficient milk supply.
Advising a "triple feeding" plan will help support breastfeeding until the family can get in to see a lactation professional and the problems can be better sorted out. “Triple feeding” might look slightly different or in a different order depending on the source or who you ask. However, “triple feeding” generally includes the following components when the baby is:
Fed at the breast
Mom pumps to empty the breasts
Offered a supplement (the expressed breast milk just pumped, donor milk, or formula)
It is important to note that “triple feeding” is not something that continues indefinitely; it is a temporary measure, generally to help increase supply and ensure the baby is gaining the appropriate weight. Also, advise the mother that the supplement offered may be expressed breastmilk or donor milk in most cases and does not necessarily need to be formula (Wagner, 2024).
Hyperbilirubinemia is a common problem, but if it is severe or is not resolving, it can become life-threatening. In addition to phototherapy, appropriate treatment consists of ensuring adequate oral intake, since bilirubin is excreted in the stool. The more a baby eats, the more they pass stool, and the more quickly they can clear the excess bilirubin.
Certain factors regarding the birth, such as bruising, bleeding, or ABO incompatibility with the mother can increase the risk of dangerously high bilirubin levels. In these instances, supplementing with either expressed or donor milk, or formula, is warranted and lactation professionals should work together with the neonatal or pediatric team to ensure breastfeeding goals are respected while also still keeping the infant’s overall health as the top priority.
It is important to note that any interruptions to phototherapy, while required to treat hyperbilirubinemia, should be generally minimized (Wong & Bhutani, 2024). For infants with a total serum bilirubin level below 20 mg/dL, depending on unit policy and provider’s orders, phototherapy can potentially be interrupted occasionally for breastfeeding, bottle feeding, or parent/caregiver holding, typically for up to 20-30 minutes at a time (Wong & Bhutani, 2024b). For infants with total serum bilirubin levels above or equal to 20 mg/dL, phototherapy should be continuous, without interruption for holding or feeding (Wong & Bhutani, 2024b). An infant can be fed via bottle while still undergoing phototherapy. Continuous phototherapy still requires periodic discontinuation for a couple of minutes while eye protection is adjusted, and diaper changes need to take place.
As discussed previously, perceptions about feeding frequency and duration are not good indicators about actual supply and the mother should be encouraged to use the previously listed indicators of satiety after a feeding and adequate supply over time. It should also be noted that a truly deficient supply in the presence of good latch and appropriate feeding techniques is extremely rare and requires collaboration with the obstetrical or primary care team.
For mothers who have established a good supply and breastfeeding relationship, sometimes there may be a perception that supply is decreasing, either through a decrease in the amount able to be pumped or in a sudden decrease in satiety in the infant.
In these cases, is it important to assess what is different or recently changed (Sandhi et al., 2020):
Did the mother recently go back to work?
Did she start taking a new medication?
Did she experience a recent illness?
Is the mother pregnant?
A common culprit of a decrease in supply starts innocently enough and may occur when a partner begins taking a nighttime feeding with a bottle so the mother can sleep more. While well intentioned, sleeping through a feeding tells the body that the infant is actually sleeping through this time and no feeding occurs (Sandhi et al., 2020). It is the basic principle of supply and demand that is at play here. This reduces the amount of breastmilk that is expressed and therefore produced during this time, which has an overall negative impact on the amount of breastmilk produced in a 24-hour period. An appropriate solution to this problem is for the mother to complete a pumping or hand expression session while the partner feeds the baby. This is still quicker and allows her to get back to sleep more easily than caring for the baby through an entire feeding but still empties the breasts and signals to the body that milk production is still needed at this time (Sandhi et al., 2020).
In the presence of a perceived supply decrease, mothers may wish to invest in products or supplements marketed to increase breastmilk supply. Fenugreek, Brewer’s yeast, fennel, and various legumes are often credited with galactagogue properties, however the evidence to support this claim is actually quite limited. Often a perceived drop in supply can be managed by troubleshooting recent changes in routine or exploring the timing and methods of milk expression. The only truly evidence-based way to increase milk supply is to empty the breasts and stimulate the nipples more often (Bazzano et al., 2016).
Keeping the mother and infant together is the best way to support regular breastfeeding. However, this is not always possible, especially if the mother works outside of the home. Breastmilk should be expressed when a mother is separated from the infant for an extended time. Expressing milk while separated helps to prevent engorgement and decreased milk supply. Expressed milk should be stored in bags specifically designed for breastmilk storage, or plastic or glass food-grade containers with tight fitting lids (CDC, 2023).
Milk can be expressed by hand or by using a breast pump. Good handwashing is important anytime milk is expressed. As mentioned earlier, special attention should be paid to the flange's size as the correct sizing of the breast flange will help the mother pump comfortably and express the most milk.
Some mothers may find that hand expression is easy and sufficient for their requirements (La Leche League GB, 2016). To express milk with hand expression, manually put a container under the breast and massage the breast gently toward the nipple. Place a thumb about 1 inch back from the tip of the nipple, and the first finger is placed opposite. Press back toward the chest, gently press the areola between the thumb and finger, then release. Do this in a rhythmic motion until the milk flows or squirts out (La Leche League GB, 2016).
Many nursing mothers dread the appearance of teeth because they assume that the child will soon begin biting and end the nursing relationship. When a child bites at the breast, he is not breastfeeding, likely forgetting where he is and perhaps trying to soothe sore gums.
Most children can be taught that biting is not acceptable. If the baby bites, the mother should respond quickly and firmly. A firm "NO!" and stern face, removal of the child from the lap, and the mother walking away for a period of even less than a minute will communicate that biting ends a feeding session (Wagner, 2024).
If an infant has been breastfeeding well and suddenly refuses to nurse, it is probably a nursing strike. Advise the mother that most nursing strikes are over within two to four days (Wagner, 2024). They happen for many reasons, and the best plan is to work through the strike with persistence and patience while trying not to take it personally. Seeking out a quiet, dim room and avoiding unnecessary stimulation may also be helpful (Wagner, 2024). An infant who is truly ready to wean will usually do so gradually over weeks or months, not suddenly like in these cases.
Breastfeeding mothers with their infants full-time and nursing on demand typically do not have menses for several months. Nursing tends to postpone fertility, though breastfeeding women are not recommended to assume that they cannot get pregnant while nursing (La Leche League, 2018a).
Caution should be exercised when taking hormonal contraceptives. Some, but not all, women find that using a birth control pill, shot, or intrauterine device (IUD) can reduce their milk supply. Women should talk with their healthcare providers about choosing the best option for their needs (La Leche League, 2018a).
Many medications are compatible with breastfeeding. Generally, the decision to use medications while breastfeeding should reflect the relative risks and benefits to both the mother and the child. For example, most antidepressants, which are most commonly selective serotonin reuptake inhibitors (SSRIs), are only present in small amounts in breastmilk, and very little is detectable in infant serum. The mother who needs the antidepressant can benefit greatly from it and be reassured that her infant is at a very low risk (Mayo Clinic, 2022). The nurse should check the available references and provide the family with the most current recommendations and the studies, if any, to support them (Mayo Clinic, 2022).
Typically, there is no need to "pump and dump" after most procedures, even if general anesthesia is required (Mayo Clinic, 2022). The same applies to dental procedures and most radiological exams, including those with contrast (Mayo Clinic, 2022). The breastfeeding mother can request a list of the drugs that will be used in procedures in advance and ask clinic staff to check the available sources so that she knows how to proceed. The Hale Guide, Medications & Mother's Milk, as well as the LactMed ® database website or phone/tablet application are highly accurate and trusted resources for checking medication compatibility with breastfeeding (Mayo Clinic, 2022).
In addition to the common struggles and questions that many lactating mothers face, there are some special circumstances that not all mothers experience. The potential issues here are numerous and many beyond even the scope of this course. However, listed below are a few of the more common special circumstances that you may encounter when working with breastfeeding mothers.
Many studies show that human milk, either from a baby's mother or donor milk, is extremely beneficial to premature infants and helps to reduce the occurrence and severity of complications such as NEC, sepsis, retinopathy, and more. Premature breast milk is a dynamic fluid composed of macro and micronutrients especially suited to meet the preterm infant's needs and provide endless benefits to the immature and vulnerable gastrointestinal tract and immune systems of preterm infants (Stanford Children's Health, n.d.).
If the infant can feed at the breast, that is ideal, and skin-to-skin contact may have added benefits to stabilizing the baby's vital signs and minimizing distress (Stanford Children's Health, n.d.). Preterm infants often cannot feed at the breast right away, and mothers will need to hand express or pump to supply their babies with breastmilk. Early and frequent hand expression followed by an efficient, comfortable mechanical pump in the early days post-birth can provide effective nipple stimulation to promote high levels of circulating hormones responsible for adequate milk production and ejection (Stanford Children's Health, n.d.).
Infants who are born with physical and/or developmental abnormalities, ranging from very mild to more severe, are excellent candidates for breast milk nutrition. Particularly in cases when a physical abnormality might put the infant at a higher risk for developmental delays, respiratory issues, or potential infections, breastmilk is especially beneficial for these babies (CDC, 2024f). However, infants born with cleft lip and/or cleft palate, where their oval cavity might not be adequately separated from their nasal cavity, breastfeeding can be a challenge (CDC, 2024f).
Image 13: Cleft Lip and Cleft Palate
Infants born with cleft lip and/or cleft palate might have a hard time forming a suction, creating an added obstacle in successful breastfeeding (CDC, 2024f). Suction is required to adequately attach at the breast, maintain a stable feeding position, and allow the proper mechanisms to trigger the let-down reflex (Boyce et al., 2019). As a result, the infant may require longer feeding times, which can contribute to tiring the infant before full feedings are completed (CDC,2024f). In addition to struggles with suction, these infants can experience reflux of milk through their nose or even milk into their airway, due to the incomplete lip or palate (Boyce et al., 2019; CDC, 2024f).
According to the Academy of Breastfeeding Medicine’s (2019) clinical protocol specifically containing guidelines for the breastfeeding of infants with cleft lip and/or cleft palate, the following general recommendations are made (Boyce et al., 2019):
Mothers should be encouraged to start milk expression within the first couple hours of birth.
The size and location of the cleft, mom’s breast anatomy, the parent’s wishes, and any previous experience the mother might have with breastfeeding all need to be considered when working with these families.
Parents should be educated about the benefits of breastmilk, to encourage either breastfeeding or expressing breastmilk to be fed.
Specialized bottles can be used to optimize milk flow for either short-term or long-term use if necessary for adequate growth.
Guidance must be provided to parents of these infants of expected feeding outcomes based on their child’s cleft type. This guidance is most beneficial when it is shared prior to the infant’s arrival in the antenatal period as well as the postnatal period. This guidance must come from lactation professionals who have clinical expertise in feeding infants with cleft lip and/or palate.
Infants with cleft lip only may very well be able to form a sufficient suction and breastfeed successfully, without additional support.
Infants with cleft lip and/or cleft palate should be offered breastfeeding attempts, as tolerated, to both assess the infant’s ability to empty the breast, and to assist mom in initiating and maintaining her milk supply as well as to provide comfort and bonding opportunities for the new dyad.
The infant’s hydration and nutrition need to be monitored while a feeding method is being established. Some infants with cleft lip and/or cleft palate might require additional supplementation, sometimes even more than expressed breastmilk, for adequate growth.
If the cleft lip and/or palate has occurred as part of a known or suspected genetic syndrome or sequence, all of this must be considered when deciding if breastfeeding is appropriate for any additional features of their genetic syndrome/sequence.
If a prosthesis for the palate is utilized prior to the infant is sent for surgical repair, caution should be taken when advising a family to use the device during breastfeeding, as these devices likely do not increase breastfeeding efficiency.
Support and education is essential for families of infants with cleft lip and/or palate and should be timely and expected to be ongoing as feeding challenges arise.
Families can benefit from peer support through support groups and associations such as Wide Smiles.
The specific, clinical bedside recommendations for infants with cleft lip and/or cleft palate that have been made by the Academy of Breastfeeding Medicine through clinical experience and expert opinion of healthcare professionals include (Boyce et al., 2019):
Infants with a cleft lip might benefit from being positioned, while breastfeeding, with the cleft oriented toward the top of the breast. Example: An infant with a right cleft lip may have better success in a cross-cradle position at the right breast and a football position at the left breast.
Infants with a cleft palate or both a cleft lip and palate should be positioned semi-upright to help to reduce the flow of breastmilk from going up their nose or into their eustachian tubes. Therefore, a football position may be more effective than a cross-cradle breastfeeding position for these babies.
Clinical evidence suggests that immediately following a cleft lip repair, defined as even 1 day following surgery, that breastfeeding can begin or rebegin.
Because cleft lip repairs often do not occur right after birth, it is important to consider offering mom and baby additional support to learn how to breastfeed appropriately following repair.
Mom can try to occlude a cleft lip with a finger or thumb and support the infant’s cheeks to help with closure around the breast.
For larger cleft palates, it is suggested to position the breast downward to stop the nipple from being pushed into the cleft.
Mothers can try manually expressing breast milk directly into the baby’s mouth to make up for the inability to form a suction.
Other “tips of the trade” that have been shared for feeding positioning are changing the feeding position so that the breast fills the cleft, burp the infant often (about every 5 minutes) because these babies do often take in a lot of air as they are feeding, keep the infant upright during the feeding and for about 20-30 minutes after in order to decrease the chances or severity of nasal congestion that occurs when milk refluxes into the nose through the cleft, and feedings should only take 30 minutes at a maximum to ensure adequate caloric intake without the infant burning extra calories working too hard and too long for milk (Nemours KidsHealth, 2019). For babies who are unable to breastfeed at the breast, offering them the opportunity to do short sessions of non-nutritive sucking (suckling at the breast after it has been pumped and drained of breastmilk) for both theirs and mom’s benefit is a wonderful thing to suggest.
The specialized bottles mentioned above generally have specially designed nipples/teats that can properly control milk flow that is most appropriate, comfortable, and tolerable for an infant with cleft lip and/or cleft palate (Boyce et al., 2019). There are several brands available out there. The specialty bottles are built to allow flow of breastmilk without the need for pressure while suckling (Nemours KidsHealth, 2019). The following are examples of the specialty bottles that are available specifically for babies with cleft lip and/or cleft palate (Nemours KidsHealth, 2019; Texas Children’s, n.d.):
Medela “Special Needs” Feeder (formerly known as the Haberman Bottle):
This bottle has a one-way valve to keep milk in the nipple.
It allows babies to push the nipple against their gums to cause a flow of milk into the mouth.
In other cases, the caregiver feeding the infant can squeeze the bottle to match their sucking and swallowing pace.
To follow pace, as the baby sucks, squeeze the bottle, then release. Listen to the infant for the sound of swallowing. If the infant pauses to breathe, the caregiver should also pause from squeezing.
There are 3 lines on the nipple; the longest corresponding to the “fast flow”. Whichever flow rate line that is desired should be lined up under the middle of the infant’s nose.
Dr. Brown’s Specialty Feeding System:
This bottle also has a one-way feeding valve that prevents back-flow of milk into the bottle.
The baby can bite down on the nipple to allow milk flow without suction.
There are multiple nipples available to change out to customize the flow rate based on the baby’s age (preemie to level 3).
Pigeon Feeder:
This bottle also has a one-way feeding valve that prevents back-flow of milk into the bottle.
It has a Y-cut nipple that is thicker on one side and thinner on the other.
The thick side is intended to be placed along the infant’s upper gums.
The thinner side is meant to go on the baby’s tongue.
There is also a notch marking under the rim of the nipple that is meant to line up under the baby’s nose to ensure good positioning.
The flow rate can be adjusted by loosening or tightening the nipple.
Enfamil Mead Johnson Cleft Lip/Palate Nurser:
This bottle does not have a one-way value.
It is used by the caregiver squeezing and timing the pace of the squeezes to match the infant’s sucking pattern.
Take a look at the next image which is an example of a specialty bottle that is available for infants with cleft lip and/or cleft palate.
Image 14: Specialty Bottles
What is vital is that postpartum units as well as neonatal and pediatric units keep a supply of these types of bottles/nipples to be shared with families of infants born with cleft lip and/or palate, so that they have the opportunity to practice using them and the option of offering their breast milk even if direct breastfeeding is not or not yet an option for the mom/baby dyad.
For infants with cleft lip and/or cleft palate, the following signs and symptoms must be observed during feedings to assess whether or not they are feeding well. Signs of discomfort and not tolerating a feeding include (Nemours KidsHealth, 2019):
Coughing (during or even after feeding)
Watery eyes
Choking
Arching back during feeding
Furrowing eyebrows
Splaying hands
Refusing to open mouth
Grunting
Increased respiratory rate
Vomiting
Hiccups
In the case that these signs and symptoms are witnessed, the feeding strategy must be reassessed and changed as necessary. Even allowing for more pauses (slower pace), tipping the bottle sideways after every few swallows, or using a slower flow rate nipple can help (Nemours KidsHealth, 2019).
Additional research is still needed to provide better clinical recommendations for parents who wish to breastfeed their infants with cleft lip and/or cleft palate. It is important to note that with the proper support, it is safe for an infant with cleft lip and/or cleft palate to breastfeed right at the breast, in many cases, or drink mom’s breastmilk via alternative methods (CDC, 2024f). Alternative methods can include the specialty bottles we reviewed, cups, syringes, or supplemental nursing systems, which we will discuss more in depth shortly (CDC, 2024f). It is also important, however, that careful consideration must be taken for these infants and close monitoring should take place to ensure they are receiving adequate calories to gain weight and grow appropriately (CDC, 2024f). The sooner a mother can receive professional lactation assessment, support, and direction in the case of cleft lip and/or cleft palate, the better the inpatient experience and overall outcome for both the infant and the family unit.
Tongue-tie, or ankyloglossia, is a condition where the infant’s tongue range of motion is restricted due to the existence of a short or tight band of tissue (lingual frenulum) that anchors the tongue’s tip to the floor of the infant’s mouth (Thomas et al., 2024; Cleveland Clinic, 2024). Tongue-ties can potentially interfere with breastfeeding as the tongue is being restricted from being extended and elevated appropriately (Thomas et al., 2024; Cleveland Clinic, 2024). However, it has been seen that not all anatomic variations of the lingual frenulum lead to difficulties with breastfeeding (Thomas et al., 2024). In fact, less than 50% of infants with the physical findings of what would be consistent with a “tongue-tie” had issues with breastfeeding (Thomas et al., 2024). Most children with tongue-ties can feed well from bottles, but it should not have to be the reason a mother has to stop breastfeeding and bottle feed instead.
Tongue-ties are often first noticed by the sound of clicking or popping during breastfeeding, which is a sound that is made by the movement of the tongue (Nemours KidsHealth, 2024). Take a look at the image below for an example of what a tongue-tie might look like. It has also been described as making the tongue look heart-shaped or like it has a notch in it (Cleveland Clinic, 2024).
Image 15: Tongue-Tie
The diagnosis of tongue-tie has increased substantially over the past several years, with some year ranges having seen a 10-fold increase (Thomas et al., 2024). Because there is an overall lack of consensus for the diagnosis and treatment of tongue-tie, there is quite a wide practice variation across the country and internationally (Thomas et al., 2024). Based on research and peer-reviewed journals, the American Academy of Pediatrics (AAP) published a clinical report with their recommendations for the diagnosis and treatment of tongue-tie for the breastfeeding infant (Thomas et al., 2024). While the guidelines are extensive (see link in reference list for full review), a few of the important points to know include (Thomas et al., 2024):
Symptomatic ankyloglossia has been defined by AAP as a restrictive frenulum anatomy that results in nipple pain, poor latch, AND poor weight gain in the infant.
Newborn infants with potential tongue-tie require close monitoring and support while in the hospital as well as post-discharge.
In the case of suggested or suspected tongue-tie, the AAP recommends that the infant be evaluated by a pediatric provider, involving a lactation professional as well. It might even be helpful to bring in a dentist for a consultation to evaluate the child with a team approach.
During a clinical evaluation and physical examination, possible differential causes of these symptoms need to be reviewed first. Potential other infant causes can include other oral anatomic variations of the lip or palate, prematurity, sleepiness at the breast, high intraoral pressure, or even bottle preference over breast. Other potential mother-related causes can be nipple variation, infection, or low milk supply due to ductal tissues or numerous other medical problems).
After the rule-out of other causes for the issues with feeding and the poor weight gain during feedings, if a tongue-tie cannot be confirmed, it is important for the mother/baby dyad to work with their primary care provider to see what else might be going on.
If the rule-out of other causes helps to confirm tongue-tie, then a frenotomy is recommended.
After frenotomy, post-operative stretching exercises, said to prevent reattachment of the frenulum, are not evidence-based, could lead to an oral aversion, and are simply not recommended.
Most babies can begin feeding shortly after frenotomy. While some infants have improved feeding very quickly, others take a little more time to adjust.
The AAP makes note that they do not recommend costly non-evidence-based treatments for tongue-tie. Instead, they recommend a frenotomy. Historically, the most common frenotomy was done with the use of surgical scissors to simply cut the frenulum, generally without anesthetic or sutures (Thomas et al., 2024). More recently physicians, oral surgeons, and dentists have been performing frenectomies with the use of lasers (Thomas et al., 2024). It is important to emphasize here that not all babies with tongue-tie require a frenotomy (Thomas et al., 2024). Infants with a physical tongue-tie but normal feeding patterns need no intervention (Thomas et al., 2024). Some do quite well after working with a lactation professional who can recommend a change in breastfeeding positioning that might be all that is needed to improve latch and allow the infant to receive nutrition and mom to not be in more pain than is normal. With that being said, sometimes, even if the baby is growing appropriately, but the latch does not seem to be deep enough and mom is in pain, a frenotomy can be considered to improve breastfeeding for the mother (Children’sHealth, n.d.).
Tongue-tie and the use of frenectomies have been a huge topic of interest on social media. While it has increased awareness of a potential issue that could impact breastfeeding, it has contributed to parents rushing to the doctor with misinformation and has had a part in tongue-tie being over-diagnosed and over-treated (Thomas et al., 2024). Tongue-tie can very well be a normal variation in mouth/tongue anatomy for an infant, without any impact to breastfeeding.
Surgery to breast tissue, which can be for the purposes of breast augmentation or breast reduction, does have the potential to impact breastfeeding success. Breast surgery can interfere with milk production and flow, blood flow, nerve response, and hormonal response because of incisions or scar tissue (Wagner, 2024). The ability to breastfeed in these situations is entirely individualized and depends on what damage occurred to the lobules and ducts due to the surgery (Wagner, 2024).
For women who have undergone a breast reduction, the amount of tissue remaining and the integrity of the ducts will determine how possible lactation will be. If a mother with a previous reduction is able to successfully breastfeed, as is still a possibility, it may be necessary that she may need to supplement, in the case that supply is not quite enough (Wagner, 2024).
On the other hand, breast augmentation surgery may not interfere with breastfeeding at all. In fact, one study, the Breast Implant Follow-Up Study, was a 10-year observational study working with more than 3,500 lactating women, that found that 79.4% of these women were successful in breastfeeding at least one child (Jewell et al., 2018). Typically, the implant is placed beneath the chest muscle, and there is little impact on the ducts. Incisions on the underside of the breasts typically result in less damage to the duct than incisions made around the nipple (Wagner, 2024).
In the past, human immunodeficiency virus (HIV) infection was an absolute contraindication for breastfeeding, however recent evidence includes new updates for parents with HIV who may want to breastfeed.
Current evidence now suggests that the risk of HIV transmission through breast milk is less than 1% for mothers receiving antiretroviral therapy with an undetectable viral load sustained during pregnancy (National Institute of Health [NIH] Office of AIDS Research, 2023). Assuming that being HIV+ is an absolute contraindication to breastfeeding may actually further disparities already experienced by this population by restricting the benefits gained from breastfeeding. HIV+ mothers should be counseled on the risks and benefits and encouraged to make a choice that feels right to them (NIH Office of AIDS Research, 2023).
There are some breastfeeding circumstances where a Supplemental Nursing System (SNS) may be useful. This device consists of a container of either expressed breastmilk or formula connected to a flexible tube that delivers milk to the baby as they nurse at the breast (WebMD, 2025). Feeding via this method allows the infant to receive supplemental nutrition while still working on a breastfeeding relationship. It may be indicated for use in the following scenarios (WebMD, 2025):
Low maternal supply due to hormonal issues, breast surgery, or complex medical diagnoses.
Premature or low birth weight infants who are experiencing difficulty latching or sucking efficiently, particularly due to very small size. Size and oral motor skills will improve as the infant grows, so SNS may be useful in the interim when a long-term breastfeeding relationship is desired.
Adoptive mothers who wish to induce lactation through frequent nipple stimulation (via the SNS) in combination with medications to induce milk production.
Mothers who have previously breastfed and wish to induce lactation again through nipple stimulation.
Babies with medical challenges that make latching more difficult such as cleft palate, tongue-tie, or other anatomical challenges.
Babies who are accustomed to bottle feeding with expressed breast milk, but the mother would like them to learn to feed at the breast. This can be useful for infants with extended early hospitalizations who were unable to feed at the breast initially.
Using an SNS is fairly straightforward. A container is filled with supplemental milk (expressed breastmilk or donor milk or formula) which is hung higher than the breast to allow gravity to assist with milk flow. The tubing from the container is taped to the mother’s breast and the tip should align with the nipple and the baby’s mouth. The baby latches to the breast and dually feeds from the breast and the tube, receiving nutrition from the SNS as well as stimulating the mother’s nipple and extracting any milk if she is already lactating. Adjustments to latch and flow rate of the SNS are made as needed.
Image 16: Supplemental Nursing System
This method of feeding does have its uses but overall is not very popular or frequently used due to significant challenges. The challenges that have been identified can include (Pearson-Glaze, 2025):
There is a learning curve to positioning tubing and latching an infant outside of the norms of lactation.
Setting up and cleaning the system is time consuming.
Extended use of an SNS may make transitioning fully to the breast difficult and infants may become frustrated with taking the free-flowing milk away.
The cost of the supplies may be a hardship for some families.
There may be social stigma, making the SNS feel awkward or “less-than” a more conventional breastfeeding experience.
Fortunately, few contraindications to breastfeeding exist.
Infants born to women who have active untreated tuberculosis should not breastfeed. Also, women undergoing chemotherapy or receiving antimetabolites or radioactive treatments should not breastfeed (CDC, 2024d).
Galactosemia, an inborn error of metabolism, is an absolute contraindication to breastfeeding (CDC, 2024d). Infants who have this disorder cannot utilize galactose, a component of the lactose sugar in human milk. Accumulation of galactose that goes unused and builds up in the body can lead to adverse consequences, including failure to thrive, liver dysfunction, cataracts, and mental retardation (CDC, 2024d). Breastfeeding is not contraindicated with other inborn errors of metabolism, such as phenylketonuria, but infants should be monitored closely for their blood phenylalanine levels (CDC, 2024d).
Women who use street drugs should not be encouraged to breastfeed. Still, women undergoing a Methadone treatment program are encouraged to breastfeed to reduce the effects of drug withdrawal in the infant (CDC, 2024d).
A first-time mother presents to the lactation clinic with her five-week-old infant. The mother, Maria, is concerned about perceived low supply and slow weight gain in her infant, Selena. Maria is a healthy 27-year-old woman with a past medical history of mild exercise-induced asthma and a medication list of PRN albuterol. She reports a healthy pregnancy complicated by breech presentation and delivery by scheduled cesarean section at 39 weeks gestation.
Selena was first put to the breast at 90 minutes old once Maria was out of recovery. The mother reports that the baby has latched well from the beginning, with occasional pain if her latch is shallow, but she is easily corrected and relatched. She reports that her supply began increasing around day five postpartum, and she was pumping after feedings to relieve engorgement. Selena gained weight well and had surpassed her birth weight by two weeks of age.
Maria reports that her milk supply seemed to level off around this time and she stopped feeling engorged. She said that because of this, she stopped pumping. She reports that she had quite a bit of stored milk collected, and that Selena’s father, Luis, began using it for feedings during the night so that Maria could sleep uninterrupted. At Selena’s four-week appointment at the pediatrician last week, it was observed that she was no longer gaining weight at an acceptable rate, and it was advised that the parents offer a supplement after each feeding.
Maria wanted to supplement with expressed breastmilk but reports that she could not get even an ounce of expressed milk after each feeding and has had to offer formula instead. She reports that Selena is feeding around every 2 hours, sometimes up to 4 hours at night. One nighttime feeding is via a bottle given by Luis where she takes 3 oz. She continues to latch well and feeds for around 10 minutes on each side. She is also taking 1-1.5 oz of formula after most feedings for the last week. She has 2-4 stools and 8-12 wet diapers per day.
A feeding is assessed in the clinic, and Maria seems comfortable handling Selena. She latches well, taking an appropriate amount of nipple into the top half of her mouth, lips flanged, and has a rocker motion to her jaw. She can be heard sucking and swallowing. A weight check before and after the feeding shows a 1 oz weight gain. She does not seem completely satisfied after the feeding and is still somewhat fussy.
The lactation professional reassures Maria that Selena’s latch is effective but cautions that some of her current feeding habits may be contributing to a decrease in supply. The lactation professional reviews some of the physiology of supply and demand and works with Maria to create a plan to maximize this pattern. A few points that are reviewed with Maria include:
Breasts that are emptied regularly will produce more milk more quickly. Skipping feedings and allowing milk to build up in the breasts will slow the production of milk. Any time others feed the baby, she should express milk to empty the breasts and signal to the body that more milk is needed.
Attempt to express milk after each feeding to signal a higher demand and increase supply. Check flange sizes on the pump and swap out for an appropriate size if they do not fit correctly. Consider hand expression as an alternative method of expression as well.
A surplus supply during lactogenesis II is fairly normal. It does usually level off during lactogenesis III, so the goal will be for the infant's weight gain to increase and to be able to stop formula supplements, not necessarily to return to a surplus of pumped milk.
Maria enacts the above plan and returns in 2 weeks for reassessment. At that time, she reports that Luis is still doing one nighttime feeding but that she is waking to pump once as well. She hand-expressed breastmilk after most feedings for the first week until she was able to get around 1 oz of extra milk. At that point, she stopped supplementing with formula and attempted a longer feeding at the breast. Selena was more satisfied after feedings, and at her follow-up visit to the pediatrician, her weight gain was back to 1 oz per day.
By understanding the supply and demand relationship of milk production, the lactation professional identified that increased supplementation and skipping feedings was decreasing the demand, and therefore the supply of breastmilk. Increasing nipple stimulation and milk expression during the nighttime and after feedings was an effective method to increase supply and return to adequate milk production. Also, providing reassurance to Maria that not being able to pump a large excess of milk is not an indication of a drop in supply is beneficial to her confidence as a mother.
Continuing to offer supplementation after each feeding does run the risk of further decreasing demand and therefore supply. There is a fine balance between getting the infant adequate calories during this time and not further damaging the supply. This is why hand expression or pumping after each feeding is important. Assessing pump flange fit and teaching hand expression is also very important and, if not included in the plan of care, could make attempts at increasing supply ineffective. A non-expert may have assessed the infant's latch and, since it was effective, not have known what approach to take. Assessing the whole feeding history is very important to understanding where problems may be occurring and assisting mothers with formulating an effective plan.
A 31-year-old, second-time mother, Daniela, presents to the lactation clinic with her 6-week-old infant, Mateo. She has concerns of a painful lump in her right breast that started 2 days ago. There is localized pain and mild redness. She denies fever, chills, or body aches. She does note that milk flow has decreased from the affected breast.
She is otherwise healthy, and her only medication is a prenatal supplement.
Daniela explains that her pregnancy was healthy and that she delivered Mateo via spontaneous vaginal delivery at 39-week 6 days gestation. Breastfeeding was initiated within the first hour of life. In general, Daniela reports that the latch is good, sometimes shallow when Mateo is tired. He feeds every 2-3 hours during the day, sometimes going as long as 4 hours at night. He has passed his birth weight and is wetting 8-10 diapers per day.
Upon assessment, the right breast is swollen with a visible 3 cm area of redness to the outer upper quadrant. A firm, palpable lump is tender to the touch. A feeding is observed, and Mateo’s latch is effective, with visible and audible swallowing. There is no difference in the lump after the feeding.
This is determined to be a plugged duct. Daniela is advised to nurse/pump more frequently on the affected breast, at least every 2-3 hours, and always starting on the right side to ensure drainage.
Mateo should be positioned with the chin pointing towards the plugged duct to direct suction to the affected area. Daniela is also advised to use warm compress and gentle massage to the affected area. Daniela is told to do 10-15 minutes of warm compress prior to feeding and gentle massage for 1-2 minutes in a circular motion and towards the nipple. She is also encouraged to hydrate and rest.
Daniela is instructed on how to assess the pump flange size she is using at home, as an improper fit can cause incomplete emptying and contribute to future plugged ducts.
She is also taught to monitor for signs of worsening redness, swelling, and pain, which may indicate mastitis has developed.
One week later, Daniela follows up and reports significant improvement with the suggested interventions. The lump has completely resolved, and her right breast no longer feels engorged or painful. She did change the flange size on her pump as it seemed the fit was not quite right. She reports increased confidence in managing her breastfeeding and pumping routine.
The interventions addressed the underlying issue of plugged ducts, which is milk stasis. Increasing the frequency of milk removal and optimizing feeding and pumping techniques helps to improve milk flow and clear the blockage.
The first major strength of this case study includes Daniela’s willingness to seek help and commitment to breastfeeding. In addition, the lactation professional’s evidence-based assessment and recommendations resolved the current issue as well as worked to prevent future issues. As far as weaknesses, initially Daniela was only massaging the area rather than implementing increased feeding frequency, leading to her physical complaints. It would have been very helpful and potentially even preventative if Daniela had been taught more about flange fit. This, however, is a common problem and one that might not have been addressed thoroughly given Daniela had breastfed another infant previously. That fact alone should serve as a reminder that even experienced breastfeeding moms can experience new issues they had not before. It is important to provide them with as much anticipatory guidance as we can.
The nurse at the lactation clinic is caring for a 17-year-old first time mother, Elena, and her 3-week-old infant, Mia. Elena reports that the latch is painful and that Mia is fussy and unsatisfied after feedings. She reports increasingly sore and cracked nipples over the last week and that Mia only latches for brief periods before pulling off crying. She feels overwhelmed and is considering switching to formula which is what her family is encouraging her to do anyway. However, she would really like to try to make breastfeeding work.
Elena explains that her pregnancy was uncomplicated and that Mia was delivered at 40 weeks gestation via vaginal delivery after artificial rupture of membranes. Breastfeeding was initiated within an hour.
Elena says that Mia has not yet regained birth weight and is still 4 oz below it. She is having around 6 wet diapers per day and stooling small amounts about 1-2 times daily. Mia is feeding every 2-3 hours for only a few minutes and then falls asleep at the breast. Elena reports not trying to pump or supplement as she does not know how to use the pump and feels intimidated by it.
Elena says she is otherwise healthy and does not take any medications. She lives with her parents, the baby’s grandparents.
The nurse performs an assessment and notes that Elena’s nipples are cracked with some scabbing and redness. While observing a feeding, Mia latches briefly and the nurse notes a shallow latch. Lips are not flanged, and Mia’s tongue is not positioned under the nipple. She does not sustain active sucking and swallowing for more than a few seconds before pulling off and crying. Elena struggles to hold her in a comfortable position and her alignment is not good. After a 10-minute attempt at feeding, a post-feed weight indicates 0.5 oz gained.
A poor latch is identified as the primary issue here. The nurse teaches Elena how to hold Mia in a cross-cradle, to give her more control of her head. She is shown how to align Mia’s ear, shoulder, and hip. She is also shown how to allow Mia to tip her head back before bringing her to the breast, so her lips are wide and can take in more breast tissue. Using the sandwich technique to hold her breast, Elena tickles Mia’s lip with her nipple and guides the nipple into the top half of her mouth, making sure her chin and nose touch the breast.
Elena is also given lanolin to use on her nipples after feedings and throughout the day, as well as breast shells to keep her bra and shirt off of her nipples while they heal.
She is advised that she can also supplement with pumped milk to help the baby reach her weight gain goals and allow others to bond with the baby. The nurse teaches Elena how to assemble and use her pump.
Elena is reassured that this is a learning process and that she is doing great. She is connected to a local breastfeeding group and a local group for young mothers.
Two weeks later, this mother-baby dyad follows up and Elena reports significantly improved feedings. Mia is latching more deeply and feeding for 15-20 minutes, appearing more satisfied after feeding. She has also gained 9 oz and surpassed her birth weight. Elena reports that her nipples are healing and, while not completely painless, they are much improved. She is also pumping once a day to build a supply of frozen breastmilk.
The assessment of a shallow latch and thorough education on how to properly hold and latch the infant helped this mother develop confidence in her ability to breastfeed. She experienced reduced pain and frustration as well as appropriate weight gain for the infant.
The first strength of this case study is the mother’s determination to seek help and persist over challenges. It also demonstrated a hands-on approach of the nurse to demonstrate appropriate hold and latch, a hands-on teaching of how to properly use a pump, and an appropriate intervention for painful and cracked nipples. As far as its weaknesses are concerned, the family encouraging formula feeding over breastfeeding is a true disservice to this young mother. The mother’s young age already puts her at risk for early cessation of breastfeeding because it can be a barrier to successful breastfeeding. In addition, being discharged from the hospital without appropriate education on how to use a pump negatively impacted this mother’s confidence and breastfeeding experience. And finally, a delay in lactation services when the infant was not gaining weight contributed to significant problems that could have been addressed sooner.
Sandra is a new mom with a 3-month-old baby, Matthew. She has joined a lactation group due to concerns with the occupation of breastfeeding. The lactation group is led by an occupational therapist (OT) who collaborates with a lactation specialist to ensure their services complement each other. Sandra comes to the group without specific questions at this time, but she is unsure she wants to continue breastfeeding after she returns to work because she is very worried about this transition and finding the time with everything back on her plate. Overall, Sandra is just feeling overwhelmed and not sure what questions to ask.
To try to get more information about Sandra’s current situation, the OT conducts an occupational profile, an occupation-based assessment that identifies difficulties related to Sandra’s personal priorities, habits, and values, as well as body changes related to childbirth.
Based on Sandra’s OT profile, she is encouraged to attend classes designed to help her develop new routines and habits that promote her transition to breastfeeding. These classes include helping to address stressors related to breastfeeding, such as managing her time and addressing Sandra’s concerns about self-worth and competence in breastfeeding and her new role as a mother, concerns that come up while Sandra is present in class. When it is discussed about the transition of back-to-work and maintaining breastfeeding habits, Sandra is encouraged to reach out to her human resources department to learn about what services are available and the policies that exist to support moms.
The OT sessions also address ergonomic concerns related to breastfeeding, as Sandra had been experiencing back and neck pain during breastfeeding but had thought this was normal. The group sessions demonstrated and educated Sandra about ergonomic techniques to promote body mechanics and alignment between Sandra and her baby.
After attending the sessions, Sandra felt more confident in her new role as a breastfeeding mother. She gained increased self-confidence and self-worth, as well as improved strategies for managing stress and addressing ergonomic concerns related to breastfeeding. Sandra gained greater insight into her new role as a breastfeeding mom and how the occupation of breastfeeding impacts numerous areas of her life. While she is still nervous about the transition when she goes back to work, she feels better about the services and accommodations her workplace has to support new mothers to include a private lactation room, small refrigerator, and an understanding that she will have time to pump when it is needed.
Occupational therapy sessions can address the unique occupation-based perspective of breastfeeding. The sessions generally take place once a week in a group format with various topics related to the new mother's roles as they relate to breastfeeding and the support and tools they need to address this occupation. There has been an increasing role for occupational therapy practitioners in being involved and helping new mothers to obtain their personal wellness goals (Sponseller et al., 2021). OT sessions can be a valuable option for breastfeeding mothers to learn and obtain more support focused on their bodies and should be considered or recommended by healthcare professionals who work with postpartum mothers.
Although Sandra was not sure what support she needed at first, she did know that she needed it. She had been given the resources to find a group like this who could help her, and she took the initiative to do so, which is a true strength of this situation. The OT professional who was the leader of the group was uniquely placed to be of valuable help to this new mother who was struggling with just where to go from here. It is already known that breastfeeding can be like a full-time job for a mother, but what might be less known is that it is also considered an occupation in the OT world, for which there is support for both mom and baby’s well-being that can be readily available when working with these healthcare professionals. This case has helped to bring this to light. In terms of weaknesses, this case featured the worries of a breastfeeding mom who will soon need to return to work and is concerned about how she will continue to provide her milk for her child when this happens. It is essential that breastfeeding moms be accommodated whenever possible to ensure that the decision to breastfeed their child is theirs and not ceased early due to an unsupportive work environment.
The benefits of breastfeeding are numerous and well documented. Thankfully, the culture of support around breastfeeding seems to be trending in the right direction in the United States in the last few years. This country is still far from reaching its goals for breastfeeding rates, and efforts must continue to educate, support, and encourage women to experience breastfeeding success. Healthcare professionals are at the front lines of this effort and should take the responsibility to impact lactating women positively. While there are many more breastfeeding issues beyond the scope of this course, a basic knowledge of lactation, how it works, why it is important, and how to troubleshoot common issues is a great place to start to improve the health of society through human milk.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
OR
No TestAttest that you have read and learned all the course materials.
Implicit Bias Statement
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
American Academy of Pediatrics. (AAP). (2024). Your premature baby’s nutrition needs: Breast milk, fortifiers and preterm formulas. Healthychildren.org. Visit Source.
American College of Obstetricians and Gynecologists. (ACOG). (2021). Barriers to breastfeeding: Supporting initiation and continuation of breastfeeding: ACOG Committee Opinion Summary, Number 821. Obstetrics and gynecology, 137(2), 396–397. Visit Source.
Baby-Friendly USA. (2024). About us: The Baby-Friendly Hospital Initiative. Baby-Friendly USA. Visit Source.
Bazzano, A. N., Hofer, R., Thibeau, S., Gillispie, V., Jacobs, M., & Theall, K. P. (2016). A review of herbal and pharmaceutical galactagogues for breast-feeding. The Ochsner Journal, 16(4), 511–524. Visit Source.
Beauregard, J. L., Hamner, H. C., Chen, J., Avila-Rodriguez, W., Elam-Evans, L. D., & Perrine, C. G. (2019). Racial disparities in breastfeeding initiation and duration among U.S. infants born in 2015. Morbidity and Mortality Weekly Report (MMWR), 68(34), 745-748. Visit Source.
Boyce, J. O., Reilly, S., Skeat, J., Cahir, P., Young, M., Noble, L., Reece-Stremtan, S., Bartick, M., Calhoun, S., Dodd, S., Elliott-Rudder, M., Kair, L. R., Lappin, S., Larson, I., Lawrence, R. A., Lefort, Y., Marinelli, K. A., Marshall, N., Mitchell, K., … Winter, L. (2019). ABM Clinical Protocol #17: Guidelines for Breastfeeding Infants with Cleft Lip, Cleft Palate, or Cleft Lip and Palate—Revised 2019. Breastfeeding Medicine, 14(7), 437–444. Visit Source.
Burbidge, A., & Williams, E. (2020). Breastfeeding and the environment. La Leche League GB. Visit Source.
Centers for Disease Control and Prevention (CDC). (2018). 6 guiding principles to a trauma-informed approach. Centers for Disease Control and Prevention. (CDC). Visit Source.
Centers for Disease Control and Prevention (CDC). (2023). Breastmilk storage and preparation. Centers for Disease Control and Prevention. (CDC). Visit Source.
Centers for Disease Control and Prevention (CDC). (2024a). About breastfeeding. Centers for Disease Control and Prevention. (CDC). Visit Source.
Centers for Disease Control and Prevention (CDC). (2024b). NIS-child data results. Centers for Disease Control and Prevention. (CDC). Visit Source.
Centers for Disease Control and Prevention (CDC). (2024c). Breastfeeding report card. Centers for Disease Control and Prevention. (CDC). Visit Source.
Centers for Disease Control and Prevention (CDC). (2024d). Contraindications to breastfeeding or feeding expressed breast milk to infants. Centers for Disease Control and Prevention. (CDC). Visit Source.
Centers for Disease Control and Prevention (CDC). (2024e). Signs your child is hungry or full. Centers for Disease Control and Prevention. (CDC). Visit Source.
Centers for Disease Control and Prevention (CDC). (2024f). Birth defects and breastfeeding. Centers for Disease Control and Prevention. (CDC). Visit Source.
Chiang, K. V., Li, R., Anstey, E. H., & Perrine, C. G. (2021). Racial and ethnic disparities in breastfeeding initiation ─ United States, 2019. Morbidity and Mortality Weekly Report (MMWR), 70(21), 769–774. Visit Source.
Children’sHealth. (n.d.). Tongue-tie and breastfeeding. Children'sHealth. Visit Source.
Cleveland Clinic. (2023c). What to know about breastfeeding let-down. Cleveland Clinic. Visit Source.
Cleveland Clinic. (2023d). Feeding your baby: The first year. Cleveland Clinic. Visit Source. Visit Source.
Engelbrecht, B. (2025). Understanding your baby’s hunger cues. Babylist. Visit Source.
Higuera, V. (2019). Can power pumping increase your milk supply? Healthline. Visit Source.
Howland, G. (2024). Breastfeeding positions: Have you tried them all? Mama Natural. Visit Source.
Jewell, M. L., Edwards, M. C., Murphy, D. K., & Schumacher, A. (2018). Lactation outcomes in more than 3500 women following primary augmentation: 5-year data from the Breast Implant Follow-Up Study. Aesthetic Surgery Journal, 39(8), 875. Visit Source.
Kesavan, S. (2024). Obstetric and gynecologic history. Merck Manual Professional Version. Visit Source.
Krol, K. M., & Grossmann, T. (2018). Psychological effects of breastfeeding on children and mothers. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz, 61(8), 977–985. Visit Source.
La Leche League. (2023). Positioning. La Leche League International. Visit Source.
La Leche League. (2022). Flat and inverted nipples. La Leche League International. Visit Source.
La Leche League. (n.d.-a). Is my baby getting enough milk? La Leche League International. Visit Source.
La Leche League. (n.d.-b) Frequency of feeding. La Leche League International. Visit Source.
La Leche League. (n.d.-c). Importance of breastfeeding. La Leche League International. Visit Source.
La Leche League. (2018a). Birth control. La Leche League International. Visit Source.
La Leche League. (2018b). Colostrum: General. La Leche League International. Visit Source.
La Leche League GB. (2016). Hand expression of breastmilk. La Leche League GB. Visit Source.
The Lactation Network. (2018). 7 factors that may affect breastfeeding. The Lactation Network. Visit Source.
Lansinoh. (2018). Power pumping: How to increase your milk supply. Lansinoh. Visit Source.
Lincoln, J. (2024). Understanding your newborn’s stomach size. The Birth Book Companion. Visit Source.
Mayo Clinic. (n.d.). Female breast anatomy. Mayo Clinic. Visit Source.
Mayo Clinic. (2022). Breastfeeding and medications: What’s safe? Mayo Clinic. Visit Source.
Mitchell, K. B., Johnson, H. M., Rodriguez, J. M., Eglash, A., Scherzinger, C., Zakarija-Grkovic, I., Cash, K. W., Berens, P., and Miller, B. (2022). Academy of breastfeeding medicine clinical protocol #36 the mastitis spectrum, revised 2022. Academy of Breastfeeding Medicine, 17 (5), 360-376. Visit Source.
Munn, A. C., Newman, S. D., Mueller, M., Phillips, S. M., & Taylor, S. N. (2016). The impact in the United States of the Baby-Friendly Hospital Initiative on early infant health and breastfeeding outcomes. Breastfeeding Medicine: The Official Journal of the Academy of Breastfeeding Medicine, 11(5), 222–230. Visit Source.
National Conference of State Legislatures (NCSL) (2021). Breastfeeding state laws. National Conference of State Legislatures. (NCSL). Visit Source.
National Institute of Health (NIH) Office of AIDS Research. (2023). Update to clinical guidelines for infant feeding supports shared decision making: Clarifying breastfeeding guidance for people with HIV. National Institute of Health. (NIH). Visit Source.
Office of Disease Prevention and Health Promotion. (n.d.). National immunization survey- Child (NIS-Child). Healthy People 2030. U.S. Department of Health and Human Services. (HHS). Visit Source.
Pearson-Glaze, P. (2025). Supplementing at the breast. Breastfeeding.Support. Visit Source.
Pillay, J. (2023). Physiology, lactation. In StatPearls. StatPearls Publishing. Visit Source.
Sandhi, A., Lee, G. T., Chipojola, R., Huda, M. H., & Kuo, S. Y. (2020). The relationship between perceived milk supply and exclusive breastfeeding during the first six months postpartum: A cross-sectional study. International Breastfeeding Journal, 15(1), 65. Visit Source.
San Diego Breastfeeding Center. (2019). I’m told that my breastfed baby needs to be supplemented…. What should I do? San Diego Breastfeeding Center. Visit Source.
Sheldon, N. & Williams, E. (2020). Exclusively expressing breastmilk for your baby. La Leche League GB. Visit Source.
Sponseller, L., Silverman, F., & Roberts, P. (2021). Exploring the role of occupational therapy with mothers who breastfeed. American Journal of Occupational Therapy, 75(5), 7505205110. Visit Source.
Stanford Children's Health. (n.d.). The benefits of mother's own milk. Stanford Children's Health. Visit Source.
Thomas, J., Bunik, M., Holmes, A., Keels, M. A., Poindexter, B., Meyer, A., Gilliland, A., Long, S., Richter, M., Hannon, E., Kellams, A., Williams, T., Feldman-Winter, L., Mass, S., Noble, L., St. Fleur, R., Stellwagen, L., Younger Meek, J., O’Connor, M., … Thorne, V. B. (2024). Identification and management of ankyloglossia and its effect on breastfeeding in infants: Clinical Report. Pediatrics (Evanston), 154(2), 1-. Visit Source.
Thompson, L. (2024). How breast milk feeding amounts vary by age. Dr. Brown’s. Visit Source.
University of California Los Angeles (UCLA) David Geffen School of Medicine. (2023). Overcoming common breastfeeding challenges. UCLA David Geffen School of Medicine. Visit Source.
U.S. Preventative Services Task Force. (USPSTF). (2025). Breastfeeding: Primary care behavioral counseling interventions. U.S. Preventative Services Task Force. Visit Source.
Wagner, C. L. (2024). Counseling the breastfeeding mother. Medscape. Visit Source.
Walls, D. (2018). ICEA supports the international code of marketing breastmilk substitutes. International Childbirth Education Association. Visit Source.
Walters, D. D., Phan, L. T. H., & Mathisen, R. (2019). The cost of not breastfeeding: Global results from a new tool. Health Policy and Planning, 34(6), 407–417. Visit Source.
WebMD. (2025). What is a supplemental nursing system? WebMD. Visit Source.
Wong, R. J., & Bhutani, V. K. (2024). Unconjugated hyperbilirubinemia in term and late preterm newborns: Initial management. UpToDate. Visit Source.
World Health Organization (WHO). (n.d.-a). Promoting baby friendly hospitals. World Health Organization. (WHO). Visit Source.
World Health Organization (WHO). (n.d.-b). Ten steps to successful breastfeeding. World Health Organization. (WHO). Visit Source.
World Health Organization (WHO). (1981). International code of marketing of breastmilk substitutes. World Health Organization. (WHO). Visit Source.
Xiong, X., Wang, Y., Chen, X., Lin, B., Zhuang, Y., Luo, L., Wang, H., & Yang, C. (2023). Mixed feedings and necrotizing enterocolitis: The proportion of human milk matters. Breastfeeding Medicine: The Official Journal of the Academy of Breastfeeding Medicine, 18(6), 469–474. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.