This course will be updated or discontinued on or before Monday, April 5, 2027
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will know how to differentiate between BPH and prostate cancer.
Objectives
After completing this continuing education course, the participant will be able to:
List the common symptoms of benign prostatic hyperplasia (BPH).
Describe the workup for BPH.
Compare and contrast the medical and surgical treatment options for BPH.
Determine the screening for prostate cancer.
Explain the diagnostic workup for prostate cancer.
Review treatment options for prostate cancer.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Benign prostatic hyperplasia (BPH) is a common disease among older men, and its incidence increases as men age. The enlargement of the prostate and prostatic obstruction is associated with lower urinary tract symptoms (LUTS), which reduce the quality of life and may lead to prostatic and bladder outlet obstruction. LUTS describes symptoms associated with the bladder and urethra and can be caused by multiple conditions, including BPH. LUTS is classified as symptoms of voiding, symptoms of urine storage, or post-void symptoms. Symptoms of voiding include dysuria, hesitancy, urinary intermittency, and straining. Symptoms of urinary storage include urinary frequency, urgency, or nocturia. Post-void symptoms include post-void dribbling or incomplete bladder emptying.
BPH is a common cause of LUTS, but LUTS can result from many conditions, not just BPH. Men affected with BPH do not always suffer from LUTS. An enlarged prostate leads to many problems, including increasing LUTS, urinary retention, and the need for surgical intervention on the prostate (Lin, 2017).
Multiple risk factors are linked to BPH, and age is the best predictive risk factor. Research suggests that men in their fourth decade have an eight percent prevalence of BPH, which increases to 80% for men in their eighties (Wei et al., 2005). In older men, the prostate volume grows 2 to 2.5% yearly (Lim, 2017).
BPH is genetic, and research proposes inheritance demonstrates an autosomal dominant pattern(Na et al., 2017). Individuals who require surgery for BPH at a younger age are more likely to have a genetic form of the disease (Lim, 2017). Genetic BPH is associated with larger prostate size and diagnosis at an earlier age than sporadic BPH (McVary, 2021a).
Race is not highly linked to BPH, and research tends to be variable, but no strong pattern has been demonstrated. Some research suggests that BPH is less common in Asian men compared to white men (Sanda et al., 1997). One study showed that moderate to severe LUTS is more prevalent in black men when compared to white men (McVary, 2021a).
Many lifestyle factors, including diet, exercise, and alcohol use, are linked to BPH (Lin, 2017). Dietary factors associated with an increased risk of BPH include excessive calories, a fatty diet, red meat, milk, dairy products, and a high-protein diet. Dietary factors associated with a reduced risk of BPH include vitamin D, fruits, vegetables, polyunsaturated fats, and linoleic acid. Blood concentrations of lycopene, selenium, vitamin E, and carotene are inversely linked to BPH.
Exercise and physical activity are associated with reduced BPH risk, with higher degrees of physical activity linked to a greater protective effect (Lim, 2017). Interestingly, alcohol may reduce the risk of BPH with a 35 percent reduction in the chances of BPH in men who drink daily (Negri, 2005).
Features of metabolic syndrome are associated with BPH. Obesity and waist circumference is associated with an increased risk for BPH (Lim, 2017). Increased fat levels, body mass index, and waist circumference are associated with increased prostate volume (Calogero et al., 2019). Obesity not only increases the risk of BPH but increases the risk of urinary symptom progression and BPH surgery (Lim, 2017). Diabetes, elevated insulin, and glucose levels are linked to increased prostate size and BPH (Calogero et al., 2019).
Other factors linked to BPH (Maserejian et al., 2013; Lim, 2017; Andriole, 2022):
Erectile dysfunction.
A family history of bladder cancer.
Increased coffee and caffeine intake increases the risk of BPH progression.
Citrus juice intake was associated with 50% lower odds of LUTS/BPH progression.
High levels of alcohol may lower the risk of BPH due to reduced androgen levels.
Inflammation is linked to BPH. Inflammation is often seen on prostate biopsies in those with BPH. In addition, inflammatory cytokines are overexpressed in BPH tissues. Potential causes of prostatic inflammation include an autoimmune response, obesity-related inflammation, and tissue infection.
BPH affects 14 million people in the United States and is more common in the older population. About one in three men in their fifties have BPH symptoms, while about 90% of men at age 85 suffer from some degree of BPH (Deters, 2021). Certain medical conditions are associated with BPH, including cardiovascular disease and cardiovascular risk factors like hypertension. Alpha-adrenergic fibers and receptors are associated with symptoms of BPH and hypertension, and autonomic hyperactivity is linked to the development of LUTS. Those with heart failure may have increased urine production due to B-type natriuretic peptide production and fluid overload, which may exacerbate urinary symptoms (McVary, 2021a).
Neurological disease can affect urinary function. Individuals with Parkinson's disease, multiple sclerosis, and cerebral vascular accidents can all be affected by voiding dysfunction. Diabetes can also worsen LUTS for multiple reasons, including polyuria, decreased bladder sensation, incomplete bladder emptying, and reduced detrusor contractility (McVary 2021a).
The pathophysiology of BPH is not entirely understood, and multiple factors are likely associated with the disease. Inflammation and metabolic factors are contributory to BPH. Histologically, BPH forms mainly in the periurethral or transitional zone of the prostate (the area around the urethra). Hormones, including testosterone, dihydrotestosterone (DHT), and estrogen, are likely involved in developing BPH. Enlargement of the prostate gland can result in prostatic obstruction and lead to urethral resistance via increased smooth muscle tone, leading to detrusor instability and an overactive bladder.
Image 1: BPH
Androgens are involved in prostatic cell proliferation. Inflammation is linked to LUTS/BPH, and inflammation may occur due to chronic infections, obesity-related inflammation, or an autoimmune process (McVary, 2021a). Obesity is associated with increased inflammatory cytokines, and dietary fats lead to prostatic inflammation. Alpha-1-adrenergic receptors are present in the smooth muscle around the prostate and bladder neck. When these receptors are stimulated, smooth muscle contracts leading to symptoms of BPH (Deters, 2021).
The lumen of the prostatic urethra eventually narrows as the increased prostatic volume pushes on the urethra and may lead to urinary obstruction. Bladder distention results from increased pressure, which may progress to bladder detrusor hypertrophy, diverticula, and trabeculation (thickened bladder wall with a reduced ability to contract). Urinary retention may lead to urinary stasis, infection, bladder stones, hydronephrosis, and impaired renal function.
Signs and symptoms of BPH can be variable. Some patients are asymptomatic, but others develop severe symptoms and severe LUTS with bladder neck obstruction. Common symptoms of BPH can be classified as obstructive or irritative (See Table 1). Obstructive symptoms include urinary hesitancy, straining to void, slow stream, splitting of the stream, terminal dribbling, and intermittent urinary stream. Irritative symptoms include urgency, urinary incontinence, urinary frequency, and nocturia. Symptoms vary over time, and the size of the prostate does not correlate with the severity of the symptoms. Typically, the obstructive symptoms are more troublesome than irritative symptoms. Symptoms are graded on severity; typically, those with more severe diseases are more likely to seek treatment.
Table 1: Symptoms of BPH
Obstructive symptoms: WISE
W – Weak Stream
I – Intermittent flow
S – Straining to urinate
E – Incomplete emptying
Irritative symptoms: FUN
F – Frequency
U – Urgency
N – Nocturia
The physical exam includes a complete exam. The abdomen should be examined for abdominal distention, costal vertebral angle tenderness, suprapubic distention, or tenderness. The neurological exam should assess for any sensory or motor deficits.
The exam should also include a digital rectal exam (DRE) to evaluate the size of the prostate and check for any nodules that may be suggestive of malignancy. The prostate size is often reported as how many fingerbreadths wide; each fingerbreadth correlates to about 15-20 grams. The typical size is about 7 to 16 grams, and the gland should be firm and non-tender. Abnormal findings include a tender prostate (suggestive of prostatitis), asymmetry or nodules (cancer), decreased sphincter tone, or reduced perineal sensation (neurological disease). The prostate size is not correlated with symptom severity.
The disease progresses slowly over the years, but some patients may notice spontaneous improvement. About one in four patients progress to severe LUTS over six years (Platz et al., 2013). BPH can lead to complications. Acute urinary retention is a significant complication of BPH. Chronic urinary retention can increase the risk of urinary tract infection, bladder diverticula, bladder stones, and kidney damage. BPH does not increase the risk of prostate cancer. Prostate cancer mainly develops in the peripheral region of the gland, whereas BPH occurs in the central or transitional zone of the prostate.
Patients who present with LUTS may have conditions that should be considered before jumping directly to BPH. Urological conditions can lead to signs and symptoms similar to BPH, including urinary tract infection, prostatitis, prostate cancer, and bladder cancer. When obstruction is the primary symptom, diagnoses to consider include prostate cancer (will be discussed later), urethral stricture, and bladder neck contracture. Bladder tumors may present with irritative symptoms.
Conditions not related to the urinary tract, including neurological diseases such as Parkinson's disease, Multiple Sclerosis, and cerebrovascular accidents, can present with voiding dysfunction. Individuals afflicted with edema, such as in heart failure, may present with symptoms similar to BPH when fluid shifts lead to diuresis. Poorly controlled diabetes can mimic symptoms of BPH, as elevated glucose levels lead to osmotic diuresis. In addition, complications of long-standing diabetes are associated with reduced bladder sensation, reduced detrusor contractility, and incomplete bladder emptying. Some medications can lead to symptoms suggestive of BPH, including diuretics, antihistamines, and decongestants.
As discussed above, the history should differentiate between irritative and obstructive symptoms. The workup of a patient who has signs and symptoms suggestive of BPH includes a history-focused physical exam (as discussed above) and targeted diagnostic tests. Patients not impacted significantly by disease symptoms should not have intensive workup, and targeted laboratory tests are used to rule out other causes. The clinician should evaluate for hematuria, urinary retention, or incontinence, which, if present, are referred to urology.
The clinician should evaluate other features of the history. Patients with a history of cigarette smoking are at increased risk for bladder cancer. Hematuria is suggestive of bladder cancer or stones in the bladder. Hematuria may be present with BPH, but anyone with hematuria should be worked up for cancer after an infection has been ruled out. Urethral stricture may be present if the patient complains of a history of urethral trauma or urethritis.
Other key features of the history include the presence of neurological disease, which could suggest a neurogenic bladder. A complete medication history is important, as certain medications may lead to LUTS. Diuretics increase urinary output and may mimic BPH. Anticholinergic medications and decongestants have the potential to cause urinary retention.
A voiding diary is a helpful tool to help assess the disease. It offers information regarding the total volume of urine, frequency of urination, nocturnal fracture of urine voided, fluid intake, and incontinence. This tool will help the patient see patterns and help the patient manage lifestyle choices to optimize symptom control. Nocturnal polyuria occurs when greater than one-third of urine output is expelled at night. If present, other causes, such as congestive heart failure, should be investigated.
Patients who present with LUTS should have focused laboratory tests. A urinalysis looks for any abnormalities which may suggest diseases other than BPH. A urinalysis may point the clinician toward infection or diabetes. Hematuria present on the urinalysis should raise suspicion of cancer. A urine culture should be performed if an infection is suspected based on symptoms and urinalysis (the presence of hematuria, pyuria, or bacteria).
Blood work may include a test for renal function and a prostate-specific antigen (PSA). Testing for the glomerular filtration rate (GFR) is typically unnecessary unless there is a concern for kidney damage due to increased post-void residual (PVR). A reduced GFR should be followed by a renal ultrasound to assess for any degree of upper tract hydronephrosis.
A PSA can be used for two primary reasons. The first is screening for prostate cancer (discussed later). Second, it assesses prostate volume. A prostate volume above 35 grams correlates with a PSA greater than 1.5 ng/dL (McVary, 2021b). The use of 5 alpha-reductase inhibitors tends to lower PSA levels and can affect the use of the PSA for cancer screening.
The International Prostate Symptoms Score (IPSS) is a commonly used scale to quantify the severity of LUTS and monitor response to therapy or disease progression. It is a series of seven questions, each scored from 0 to 5, and the scores are totaled, and the final score is given. A total sum score of:
0-7 = Mild
8-19 = Moderate
20-35 = Severe
Post-void residual should be assessed in all patients with LUTS or BPH symptoms. The two most popular methods to assess PVR include using a bladder scanner or performing a straight catheterization after a spontaneous void. Bladder palpation cannot accurately measure the degree of urinary retention. Worsening PVR suggests treatment is ineffective and has an increased likelihood of needing a surgical intervention to control symptoms. A high baseline PVR is associated with more severe disease.
Treatment of BPH/LUTS includes lifestyle changes, medications, and surgical options. All patients should be taught lifestyle changes that may improve symptoms of BPH/LUTS. Patients who do not get adequate relief from lifestyle changes should be considered for medical therapy. Those who do not experience symptom control or develop a red flag should be referred to a urologist to consider invasive therapy, including surgical options, to manage symptoms.
The patient and clinician should engage in shared decision-making when discussing therapy options. The patient should be educated regarding the risks and benefits of all treatment options. All BPH patients should engage in lifestyle changes. For those on medical therapy, regular follow-up should ensure adequate control of symptoms and monitoring for side effects.
Routine follow-up should include monitoring for any changes in treatments for other diseases. Patients with BPH are often older and are treated for other comorbid conditions. Many treatments for other disease states result in side effects that may worsen BPH symptoms. Medications contributing to worsening LUTS symptoms include diuretics, anticholinergics, antidepressants, bronchodilators, and sympathomimetics.
All men with BPH should be educated on lifestyle interventions to help minimize symptoms of LUTS and BPH. General recommendations include maintaining or obtaining an ideal body weight, regular exercise, and a healthy diet. These interventions reduce factors associated with metabolic syndrome and the risk of BPH.
Other lifestyle interventions that can assist in controlling LUTS include:
Reducing the volume of fluids consumed close to bedtime or before travel
Limiting caffeine (acts as a diuretic)
Limiting alcohol (acts as a diuretic)
Avoiding constipation
Limiting bladder irritants such as highly seasoned foods
Smoking cessation (a relationship exists between smoking and LUTS and its overall health risks)
Kegel exercises (may reduce some LUTS)
For patients with obstructive symptoms, using timed voiding can help reduce disease symptoms. These patients should be instructed to void at timed intervals, such as every two hours. Double voiding can be helpful in those with obstructive symptoms in reducing LUTS. This involves attempting to urinate about two minutes after the initial void.
Medications are often used as first-line agents to manage BPH/LUTS before surgical intervention. First-line medications are alpha-1adrenergic receptor antagonists (A1RA). They are used to treat symptoms of BPH and are often used as first-line agents. Alpha-1 adrenergic receptors are located on the prostate's smooth muscle, and this class of medications blocks these receptors, leading to smooth muscle relaxation of the bladder neck, and reducing bladder outlet obstruction. A1RAs improve symptoms within days.
A1RAs are classified as either selective or non-selective. Selective agents are used in the treatment of BPH. Selective A1RAs have fewer side effects when compared to non-selective agents (see table 2 for agents in this class). These agents are typically dosed once daily, and common side effects include rhinitis and dizziness. Tamsulosin and silodosin (which have better prostate selectivity) are associated with fewer side effects but are more likely to be associated with ejaculatory side effects. A less common but significant side effect is intraoperative floppy iris syndrome which is most common in tamsulosin resulting in iris abnormalities that increase the risk of iris trauma and posterior capsular rupture during cataract surgery. While rare, it is essential to ask all patients prescribed A1RAs about plans for cataract surgery.
Hypotension is seen and is most common with doxazosin and terazosin, and these agents should be titrated over weeks to reduce the risk of hypotension. In addition, these agents are given at bedtime to reduce the risk of postural lightheadedness. Phosphodiesterase 5 (PDE5) inhibitors, such as sildenafil, tadalafil, and vardenafil, can potentiate the hypotensive effects of doxazosin and terazosin.
The A1RAs are generally equally effective and are more effective than placebo. Side effects include:
Dyspepsia
Headache
Nasal congestion
Myalgia
Flushing
Back pain
Hypotension
Ejaculatory dysfunction
Sinusitis
Silodosin is associated with a higher risk of sexual side effects when compared to older agents.
Men with enlarged prostates are often treated with 5-alpha reductase inhibitors (5ARI). 5ARIs stop the conversion of testosterone to dihydrotestosterone (DHT) and improves LUTS caused by an enlarged prostate. These agents are typically classified as second-line agents, and the onset of action is slow as it works by shrinking the prostate volume. Patients started on these medications should be counseled that it may take months to notice benefits, with maximal benefits noticed after 6-12 months of treatment (Gormley et al., 1992).
The two agents in this class include finasteride and dutasteride. These medications prevent BPH progression and are used in patients who have prostate sizes over 35 grams. As mentioned, the PSA can be used to estimate the prostate volume, and a PSA of 1.5 ng/mL or higher should be present before these agents are used. Any level below 1.5 ng/mL suggests the prostate is too small to see treatment benefit. These agents decrease outlet obstruction and reduce the need for surgical intervention. 5ARIs lower PSA levels – typically about 50%. It is essential to obtain a baseline PSA level as the pretreatment value should be known, so on follow-up testing, if any increased level is seen, another cause should be looked for.
Initial research on finasteride showed significant improvements in LUTS, demonstrating a 23% reduction in obstructive symptoms while reducing nonobstructive symptoms and increasing urinary flow rates (Gromley et al., 1992). Dutasteride also improves LUTS. The drug increases urinary flow rates, reduces the risk of urinary retention, reduces prostate volume, and the need for surgery on BPH (McVary, 2022). Finasteride and dutasteride result in an equal reduction of prostate volume (Nickel et al., 2011).
Research shows that treatment with these agents lowers the risk of prostate cancer but may increase the risk of high-grade prostate cancer (McVary, 2022). Other side effects of these agents include:
Gynecomastia
Erectile dysfunction
Reduced libido
Ejaculatory dysfunction
Tender breast tissue
These agents can affect fetal development if taken by pregnant women. Persistent sexual dysfunction can continue even after the drug is stopped and has been termed "post-finasteride syndrome." Not all clinicians believe that this is a genuine concern.
Some patients benefit from combination therapy. The combination of alpha-adrenergic blockers with 5ARIs is commonly used in those with at least moderate symptoms and prostate enlargement (the IPSS score is used to quantify moderate symptoms). Combination therapy improves multiple parameters, including lower rates of clinical progression, reduced incidence of renal insufficiency, fewer urinary tract infections, less acute urinary retention, and less urinary incontinence compared to those who engage in monotherapy (Deters, 2021).
For men who suffer from erectile dysfunction and LUTS, a phosphodiesterase 5 (PDE5) inhibitor can be used as a first-line treatment as they reduce urinary urgency, hesitancy, and frequency. Research has demonstrated that PDE5 inhibitors improve symptom scores with LUTS/BPH, but no significant changes in flow rates have been shown (McVary, 2021a). Studies have demonstrated that symptom scores are reduced with PDE5 inhibitors compared to placebo (Pattanaik et al., 2018). Used together with A1RAs, PDE5 inhibitors show similar improvements compared to A1RAs alone (Dhaliwal & Gupta, 2022).
Beta-3 adrenoceptor agonists (B3AR) or anticholinergic agents can be used in BPH when irritative symptoms are present and there is a low-post-void residual. B3ARs are often recommended over anticholinergic agents because they are less likely to be associated with dry mouth. The two B3ARs include mirabegron and vibegron.
Mirabegron helps improve incontinence, reduces urgency, and does not increase urinary retention. Elevated blood pressure is a significant side effect of mirabegron. Vibegron improves urinary urgency, urge incontinence, and increases urination volume. Vibegron does not have elevated blood pressure as a significant side effect. The combination of mirabegron with alpha-adrenergic blockers is not as well studied but has been shown to improve overactive bladder symptoms in patients with LUTS and overactive bladder (Mullen & Kaplan, 2021). Individuals on a combination of mirabegron and tamsulosin had fewer daily micturitions (Kaplan et al., 2020). The combination leads to less urgency, but not a significant improvement in overall symptoms score on the IPSS.
Anticholinergic agents are used to treat overactive bladder and BPH, and it is only recommended for those who do not have an increased PVR. Anticholinergics have the potential to lead to urinary retention, so caution must be used to avoid this medication in men with increased PVR. Anticholinergics can be combined with A1RA in men with BPH and irritative symptoms when monotherapy with A1RA is ineffective. Side effects of anticholinergics include:
Urinary retention
Constipation
Blurred vision
Dry mouth
Headache
Somnolence
Dyspepsia
Nausea
Table 2: Medications to Treat BPH
Drug
Dose
Alpha-1adrenergic receptor antagonists
Doxazosin immediate-release (Cardura®)
Start at 1 mg; titrate up to 8 mg every day at bedtime
Doxazosin extended-release (Cardura® XL)
Start at 4 mg; titrate up to 8 mg (after 21 days) once a day
Alfuzosin (Uroxatral®, Xatral®)
10 mg once a day
Silodosin (Rapaflo®)
8 mg once a day
Tamsulosin (Flomax®)
Start at 0.4 mg; may titrate up to 0.8 mg
Terazosin (Hytrin®)
Start at 1 mg, titrating to 10 mg; some titrate to 20 mg. Give once a day at bedtime
5-alpha reductase inhibitors
Finasteride (Proscar®)
5 mg once a day
Dutasteride (Avodart®)
0.5 mg once a day
Phosphodiesterase 5 (PDE 5) inhibitor
Tadalafil (Cilais®)
5 mg once a day
Beta-3 adrenergic agonists
Mirabegron (Myrbetiq®)
25 mg once a day, may increase to 50 mg once a day after 4-8 weeks
Vibegron (Gemtesa®)
75 mg once a day
Anticholinergic agents
Darifenacin (Enablex®)
7.5 mg once a day; may be increased to 15 mg once a day
Fesoterodine (Toviaz®)
4 mg once a day; may be increased to 8 mg once a day
Tolterodine IR (Detrol®)
1-2 mg twice a day
Tolterodine ER (Detrol® LA)
2-4 mg once a day
Oxybutynin IR (Ditropan®)
5 mg, 2 to 4 times a day
Oxybutynin ER (Ditropan® XL)
5 to 10 mg once a day; maximum dose of 30 mg a day
While many herbal agents have been purported to manage BPH effectively, studies do not demonstrate efficacy or safety. Herbal therapies are not approved by the Food and Drug Administration but are frequently used to manage BPH. The American Urological Association recommends against these agents (Lerner et al., 2021a). Agents that have been used to manage BPH include willow herb, rye pollen, saw palmetto, Hypoxis rooperi, pygeumafricanum, pumpkin seed, tomato, maritime pine bark, and nettle root (Csikós et al., 2021).
Surgical procedures are done much less frequently with the advent of newer medical therapies. Welliver et al. (2020) suggested that medication use is much more common, and surgery is less common. Although, patients who fail medical therapy may be candidates for surgery. Multiple surgical treatments are available to improve symptoms and quality of life. If symptoms are mild, the use of medications and surveillance may be appropriate, but if symptoms are bothersome, advancing to surgical intervention is reasonable. Failure of medical therapy could be suggested when conditions in table 3 are present. At this point, referral to a urologist is indicated to rule out more severe disease or for the consideration of surgical therapy.
Table 3: Indications for Urology Referral
Refractory urinary retention – PVR greater than 100 to 200 mLs
Increasing post-void residual
Bilateral hydronephrosis
Gross hematuria
Recurrent bladder stones
Renal insufficiency
Recurrent urinary tract infections
Persistent symptoms not managed by basic treatments
Severe symptoms
To understand surgical intervention for BPH, a quick review of the pathophysiology is helpful. BPH is an increase in the number of prostatic stromal cells and prostatic glandular epithelial cells in the prostate's transition zone (Han et al., 2020). The transition zone is the area that surrounds the urethra and is where benign prostatic hyperplasia occurs. In BPH, the individual prostate cells increase without any nodules. If the prostate becomes enlarged (not related to prostate cancer) and there is a subsequent obstruction at the bladder neck, it is called benign prostatic obstruction (BPO).
The prostate is made up of zones:
Peripheral zone
Transition zone
Central/periurethral zone
Anterior zone
Image 2: Prostate
Surgery often involves the manipulation of the transition zone, the region closes to the ejaculatory duct, which may be injured during the procedure. Painful or dysfunctional ejaculation may occur as a result. Although many other options exist, transurethral resection of the prostate (TURP) is considered the gold-standard surgical treatment for BPH (Bortnick et al., 2020).
Multiple reasons exist to consider surgical intervention. Indications include:
Failure of medical therapy
Moderate to severe symptoms associated with BPH
Recurrent urinary tract infection
Recurrent gross hematuria
Refractory urinary retention (failure of at least two voiding trials)
Persistent elevated post-void residual
Bilateral hydronephrosis with renal impairment
Recurrent bladder stones
Before any surgical intervention, a complete evaluation should occur, including an evaluation using the IPSS. Diagnostic testing could include evaluating post-void residual volume and considering pressure flow studies and uroflowmetry (Lerner et al., 2021b). Uroflowmetry is a test that measures urine flow rates, and when rates are less than 10 mL/second, there is likely some degree of bladder outlet obstruction (McVary, 2021b). Pressure flow studies are done when initial treatment fails, or it is unclear if there is bladder outlet obstruction.
Prostate imaging can be done in patients to determine prostate size and anatomic variables. Prostate anatomical variables may help plan intervention or help predict the success of the intervention. Imaging options include ultrasound, magnetic resonance imaging, computed tomography, or cystoscopy.
Multiple procedures are available to manage BPH. The treating urologist will base procedure choice after discussion with the patient based on prostate size/shape, side effects, patient characteristics, symptom severity, and bleeding risk. Procedures used to treat BPH include:
Holmium laser enucleation of the prostate (HLEP)
Photoselective vaporization of the prostate (PVP)
Thulium laser enucleation of the prostate (TLEP)
Transurethral incision of the prostate (TUIP)
Transurethral microwave therapy (TUMT)
Transurethral resection of the prostate (TURP)
Transurethral vaporization of the prostate (TVP)
Robotic waterjet treatment (RWT)
Prostatic urethral lift (PUL)
Water vapor thermal therapy (WVTT)
The choice of procedure depends on multiple factors, including prostate size. At the same time, many urologists vary in the interpretation of size; one standard method of prostate size includes small (less than 30 grams), average size (30-80 grams), and large (greater than 80 grams).Large prostates are typically better treated with laser eneculation or prostatectomy. Minimally invasive surgeries are best suited for prostates between 30 and 80 grams, including WVTT and PUL. Most procedures are done transurethrally. Prostatic artery embolization and simple prostatectomy are two procedures not done transurethral.
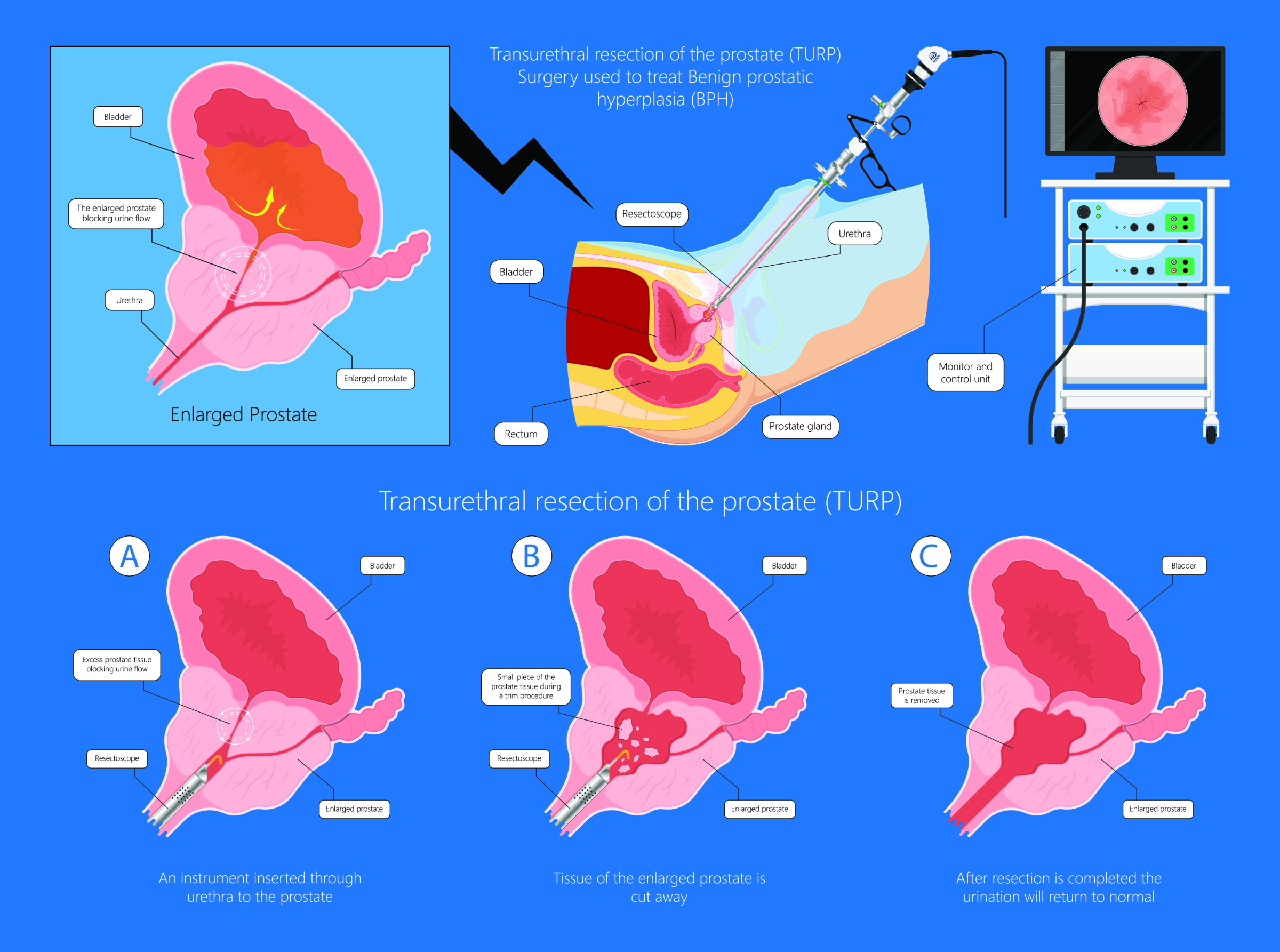
Transurethral resection of the prostate (TURP) is one of BPH's most common surgical treatments. A resectoscope is placed in the urethra, and excess tissue is removed, reducing the amount of tissue blocking urine flow. Monopolar transurethral resection of the prostate resects the prostate from the bladder neck to the verumontanum. TURP has been around for many years and is a standard by which other treatments are measured. This procedure uses a solution that can get absorbed into the systemic circulation and potentially lead to dilutional hyponatremia; therefore, monitoring electrolytes is often carried out after this procedure. Other prostate complications of a transurethral resection include urethral stricture, urinary tract infection, ejaculatory dysfunction, and urinary incontinence. Using the bipolar transurethral resection of the prostate allows for a more prolonged treatment time. It is associated with less bleeding, shorter postoperative catheter use, less need for bladder irrigation, and less hyponatremia (Cornu et al., 2015).
Image 3: TURP
(*Please click on the image above to enlarge.)
Transurethral vaporization of the prostate (TVP) utilizes an electrical current to vaporize the prostatic tissue. It is a modification of the TURP. The procedure improves flow rates and symptom scores and is associated with few complications compared to standard TURP (Wroclawski et al., 2016).
Individuals at high risk of bleeding are better suited for holmium laser enucleation of the prostate (HLEP), photoselective vaporization of the prostate (PVP), and thulium laser enucleation of the prostate (TLEP). These procedures are less likely to cause bleeding and may be done without stopping anticoagulation therapy. Individuals concerned with sexual side effects of erectile dysfunction or ejaculatory dysfunction could be considered for PUL or WVTT. However, these procedures are associated with an increased risk of retreatment.
Water vapor thermal therapy (WVTT) is a procedure that ablates the prostatic tissue with convective water vapor energy (McVary et al., 2016). It results in a 51.4 percent improvement in IPSS scores at three months (Elterman et al., 2021). It is used for patients with medium-sized prostates. WVTT is classified as a minimally invasive treatment and is often done in the office setting and necessitates minimal anesthetic or pain medication. Tissue outside the treatment zone is not affected, and WVTT is less likely to lead to sexual dysfunction. The procedure improves flow rates over four years (McVary et al., 2019).
Prostatic urethral lift (PUL) is a procedure that opens the prostatic urethra, thereby reducing obstruction. Patients with middle lobe obstruction are not good candidates for this procedure. It results in a 49.9% improvement in IPSS scores at three months (Elterman et al., 2021). This procedure is most effective on medium-sized prostates and is less likely to lead to sexual dysfunction. PUL is associated with few side effects and generally provides good relief, although some patients see the return of symptoms requiring further treatment over five years (Roehrborn et al., 2017). Surgical retreatment was higher in PUL (10.7%) when compared to WVTT (4.4%) (Elterman et al., 2021).
Other procedures include transurethral incision of the prostate, transurethral vaporization of the prostate, laser enucleation of the prostate, and photoselective vaporization of the prostate (PVP). Transurethral incision of the prostate is used to treat patients with LUTS and small prostates. This procedure is associated with much less ejaculatory dysfunction compared to TURP and is often used in younger men who are concerned about fertility as it is more likely to preserve antegrade ejaculation.
Photoselective vaporization of the prostate (PVP) uses a laser to vaporize the prostate tissue allowing more room for the bladder to excrete urine. It is indicated for those with prostates between 30 and 80 grams (but better results are often seen in those with prostates less than 60 grams). PVP is safer for those with medical comorbidities and those on anticoagulants. It can be done in an office and typically does not require overnight hospitalization. PVP may be associated with a more prolonged need for catheterization (compared to a TURP) and delayed bleeding (McVary, 2021b; Sun et al., 2019).
PVP has similar effectiveness to TURP in improving symptoms, improving urinary flow, reducing post-void residual, and reducing prostate volume (Cimino et al., 2017). The GreenLight PVP reduces hospitalization times, catheterization times, and healthcare costs. The newest generation is most effective when compared to older models (Sandhu et al., 2019).
Holmium laser enucleation (HLEP) and thulium laser enucleation (TLEP) of the prostate uses energy from a laser to destroy the prostate tissue and only minimally affect deep tissue (Kuntz et al., 2008). This technique can be used in patients with LUTS with any prostate size. HLEP is better for men with large prostates, over 100 grams, as it is associated with less bleeding, shorter hospital stays, and shorter catheter use times (McVary, 2021b). Both procedures demonstrate similar symptom improvement and voiding improvements (Hartung et al., 2022). TLEP and HLEP are equal when measuring postoperative voiding parameters, and both procedures are associated with low rates of complications (Hartung et al., 2022).
Robotic waterjet (RWT) uses a waterjet that is controlled robotically to ablate the prostate tissue. The technique works best on prostates between 30 and 80 grams. More research with longer follow-up is needed to determine the long-term safety and effectiveness of RWT (Lim Ng & Barber 2019). Transurethral microwave thermotherapy (TUMT) uses electromagnetic waves to heat the prostate. While not frequently used, TUMT may still be a valuable option in treating BPH as it improves urinary symptoms without decreasing erectile function (Ziętek & Ziętek, 2021).
Image 4: TUMT
A simple prostatectomy enucleates the prostate tissue with its capsule. The procedure is done robotically, laparoscopically, or via an open procedure. This procedure is most typically done in those with large prostates and is considered major surgery, typically requires hospital admission, and is associated with more blood loss.
Steve is a 62-year-old male who presents to his primary care physician with the chief complaint of having difficulty starting his urination stream and urinating 4-5 times per night. Upon further questioning, Steve was found to have a weak urination stream, needing to urinate every hour, and staining his pants with urine as he leaks after urinating. The patient denies any history of a sexually transmitted disease and denies previous endoscopy or surgery on the urinary tract. His past medical history is significant for hypertension, for which he takes hydrochlorothiazide; hyperlipidemia, for which he takes atorvastatin; and depression/anxiety, for which he takes sertraline.
On exam, Steve is a man who appears of stated age with no significant abnormality noted on the physical exam, including a normal abdominal exam, no costovertebral tenderness, normal anal sphincter tone, normal perianal sensation, and no signs of congestive heart failure. The digital rectal exam demonstrates an enlarged firm prostate without nodules. The physician orders a urinalysis and some basic blood work, including glycated hemoglobin, a basic metabolic panel, and a prostate-specific antigen. The physician performs the IPSS, which shows a score of 15, equating to moderate symptoms.
The physician recommends that the patient reduce caffeine intake, reduce fluid intake within three hours of bedtime, changes his hydrochlorothiazide to lisinopril, and schedules a follow-up appointment in three weeks to review the effectiveness of the interventions and review the blood work. Upon return exam, the patient reports that his symptoms are somewhat improved. The IPSS score is 12, which is improved but still considered a moderate degree of symptoms. The urinalysis is negative for any white or red blood cells. The blood work shows normal serum creatinine (to help assure there is no obstructive uropathy) and a prostate-specific antigen of 4.2 ng/dL. The patient is started on tamsulosin (Flomax) at 0.4 mg daily. After two months, his IPSS remains elevated at ten, and he is referred to a urologist due to persistent symptoms and an elevated PSA.
The urologist discusses the possibility of performing a prostate biopsy but, instead, opts to check the PSA in six months to see if there is any significant increase. The urologist performs urodynamic testing, including uroflowmetry, to assess the severity of BPH and determines the patient has a ten milliliters per second flow rate. The patient was evaluated for post-void residual volume, and it was determined that he had 150 milliliters of urine in the bladder after a complete void.
The urologist increases the dose of tamsulosin to 0.8 mg daily, adds finasteride, and schedules a follow-up in three months. At the three-month follow-up, there is some improvement, but the patient continues to be plagued by nocturia, urinary frequency, and hesitancy. Steve asks the urologist about the possibility of a surgical intervention to help with symptoms and decides to undergo a transurethral resection of the prostate (TURP). After the procedure, his symptoms dramatically improved.
Worldwide, prostate cancer is the second most common cancer in men and the fourth most common cancer (World Cancer Research Fund International, 2022). The National Cancer Institute (2022) estimates that there will be 268,490 new prostate cancer cases this year, accounting for 14% of all new cancer cases. While prostate cancer accounts for 14% of all new cancer cases, it only accounts for 5.7% of deaths and has a 96.8% five-year survival rate (National Cancer Institute [NCI], 2022).
During men's lives, it is estimated that 12.6% will be diagnosed with prostate cancer (NCI, 2022). In 2022 in the United States, 1,918,030 new cancer cases will be detected, and 609,360 people will die of cancer (Siegel et al., 2022). In the United States, the leading cause of cancer death is lung cancer accounting for 350 deaths per day. The incidence of prostate cancer has been stable since 2014, but a four to six percent annual increase in advanced disease has been seen since 2011, with an increased proportion of late-stage prostate cancer being diagnosed (Siegel et al., 2022). Mortality rates for prostate cancer have been stable over the last ten years (Siegel et al., 2022). The high rates of PSA screening drive the increased incidence of prostate cancer, and many prostate cancers found by routine PSA screening would often not become clinically significant if they were never detected (Sartor, 2022). Countries that do not use PSA frequently have fewer cases of prostate cancer.
Risk factors for prostate cancer include age, genetics, ethnicity, and dietary factors. Age is highly correlated to prostate cancer. The incidence of prostate cancer is highest between the ages of 65 and 74, and occult prostate cancer is common. Researchers who looked at autopsy studies demonstrated that autopsy-proven prostate cancer significantly increased with age, with up to 46% of people in their 50s and 70% in their 70s, and up to 83% in their 80s having prostate cancer on autopsy (Delongchamps, 2006). The prevalence of prostate cancer is higher in older men, but younger men are at higher risk of having severe disease. Bleyer et al. (2020) showed that men less than 40 with prostate cancer suffered higher death rates than older men.
Ethnicity is linked to prostate cancer. Black men are at the highest risk for prostate cancer, and Asian Americans have the lowest risk (see table 4). In addition, black men tend to have an earlier onset of disease when compared to white men. Also, when diagnosed, black men tend to have higher PSA scores, worse Gleason scores, more advanced diseases, and receive less guideline-concordant treatment (Sartor, 2022).
Table 4: Incidence Rate of Prostate Cancer by Race for Americans
Race
Incidence rate per 100,000
Black
1600
White
1000
Asian
700
(Adapted from Sartor, 2022)
Prostate cancer runs in families. According to Sartor (2022), those with a family member diagnosed with prostate cancer before age 65 are at increased risk. In addition, other risks of prostate cancer include a family history of early-onset breast cancer, male breast cancer, pancreatic cancer, melanoma, colorectal cancer, and ovarian cancer. The genetic risk for prostate cancer results from genetic variants, single-nucleotide polymorphisms (SNPs), or mutations (American Cancer Society [ACS], 2020; Sartor, 2022).
Certain dietary factors affect the risk of prostate cancer. High levels of animal fat, especially high intake of alpha-linolenic acid, are associated with prostate cancer risk (Harvard School of Public Health, 2019; Orlich et al., 2022; Sartor, 2022). Lycopene, found in tomato-based products, is associated with a lower risk of prostate cancer (Zu et al., 2014.). Other foods that may lower prostate cancer risk include broccoli, cauliflower, soy, tomatoes, and salmon (Harvard School of Public Health, 2019). Consumable products associated with an increased risk of prostate cancer include red meat, processed meat, fish oil, and dairy intake (Harvard School of Public Health, 2019; Orlich et al., 2022; Sartor, 2022).
Other factors that influence prostate cancer risk (Sartor, 2022; Wilson et al., 2011; Murphy et al., 2013; Pernar, 2018; Xu et al., 2021; Olivas & Price, 2021):
Consumable products associated with mixed results on the risk of prostate cancer include alcohol, multivitamin use, calcium, and vitamin D.
Coffee has been shown to reduce the risk of prostate cancer. In a study over twenty years, the reduction in lethal prostate cancer correlated with increased coffee consumption in those who drank six or more cups per day.
The effect of cigarette smoking on prostate cancer is somewhat conflicting, and most research finds an increased risk of prostate cancer and more severe disease at diagnosis in smokers. Research does suggest that smoking raises risks in African Americans much more than in white Americans. Smoking at the time of diagnosis is associated with higher death rates and higher rates of metastasis.
5-alpha reductase inhibitors lower PSA levels and may delay diagnosis, increasing the risk of more advanced prostate cancer.
A slightly increased risk of prostate cancer and advanced prostate cancer is associated with vasectomy, but no increase in prostate cancer mortality.
Obesity is associated with an increased risk of prostate cancer, a risk of recurrent disease, and prostate cancer mortality.
The effect of physical activity on reducing the risk of prostate cancer is uncertain, but older men who engaged in vigorous exercise had a lower risk of fatal or advanced disease.
Prostatitis possibly increases the risk of prostate cancer, but data is of low quality. However, prostatitis increases PSA and may lead to more biopsies and, thereby, more diagnoses of prostate cancers, even though many of these cancers may have never become clinically apparent.
Radiation to the pelvis may increase the risk of prostate cancer.
The most common presentation of prostate cancer is an asymptomatic patient who underwent a screening test. Most screen-detected prostate cancer cases are asymptomatic and never progress to clinical significance. Occasionally, patients with symptoms are diagnosed with prostate cancer. Symptoms are non-specific and may include:
Urinary frequency
Urinary urgency
Hematuria
Hemospermia
Although, most presentation of non-specific lower urinary tract symptoms is associated with a condition other than prostate cancer (Kang et al., 2021). Prostate cancer grows slowly and typically disseminates in a predictable pattern, starting in the prostate, moving to the pelvic lymph nodes, and then to the bones of the pelvis and spine.
At the time of prostate cancer diagnosis, 73% of men have localized cancer, 14% spread to a lymph node, 7% have metastasized, and 6% of cases are unknown (NCI, 2022). Those with metastatic prostate cancer may present with:
Bone pain
Weight loss
Pathological fractures
Urinary retention
Hematuria
Lower extremity weakness secondary to spinal cord compression
Fatigue
When patients present with LUTS, prostate cancer should be considered. Still, LUTS is commonly caused by other diagnoses, including BPH, urinary tract infection, interstitial cystitis, prostatitis, bladder outlet obstruction, or chronic pelvic pain syndrome.
Physical exam findings of prostate cancer are typically confined to an abnormal prostate on a digital rectal exam, and findings may include prostate asymmetry, nodules, or induration. A prostate that is symmetrical and firm is more suggestive of BPH. The DRE can only assess the prostate's posterior and lateral aspects, so the DRE may miss cases of prostate cancer. DRE is not sensitive to detecting small tumors and will not detect tumors in other prostate regions. DRE is less successful at detecting prostate cancer when compared to a PSA but helps detect cancer in those with normal PSA levels.
Prostate-specific antigen (PSA) testing can detect prostate cancer along with the DRE. The higher the PSA, the more likely prostate cancer is present. Other conditions can elevate PSA readings, including BPH, prostatitis, and perineal trauma. A normal PSA does not rule out prostate cancer. Most prostate cancers are detected with slightly elevated PSA readings (typically less than 10.0 ng/dL).
Multiple measures can be used to differentiate prostate cancers from other findings. The PSA may be compared to typical ranges for the patient's age, and the PSA typically increases as someone ages. Some clinicians consider further evaluation for prostate cancer for any PSA above 4.0 ng/dL. The rate at which the PSA rises, the percentage of free PSA, the PSA density, and the Prostate Health Index (PHI) test can help predict prostate cancer's likelihood.
A repeat PSA should be done a few weeks after an initial high reading to verify the reading. Certain factors discussed above may elevate the PSA that are not prostate cancer and, if present, should be addressed before repeating the PSA (for example, antibiotics for an infection). If the repeat PSA is normal, no nodule, induration, or asymmetry is felt on DRE, and it has not significantly increased over the last year, an intensive workup is likely not indicated.
Screening slightly reduces prostate cancer death rates, but screening is associated with risks (Ilic et al., 2018). Shared decision-making with PSA should be done with all patients at risk, and screening should be more strongly considered in patients with risk factors. In 2018, the United States Preventative Services Task Force (USPSTF) (2018) recommended that prostate cancer screening be offered with PSA based on patient preference and patient judgment in men between 55 and 69 (United States Preventative Services Task Force, 2018). It is not recommended for patients over the age of 70.
Most with elevated PSA readings do not have prostate cancer, but what do we do with an elevated PSA reading? The diagnostic evaluation of an elevated PSA includes a good history and physical; it is essential to determine if any other factors contribute to the elevated PSA (for example, UTI or prostatitis). A DRE is an essential part of the evaluation of an elevated PSA. A repeated PSA often normalizes, so this should be done before moving to a prostate biopsy.
When clinical findings are equivocal, prostate imaging or other diagnostic tests may help determine if a prostate biopsy is warranted. The PSA density is the ratio of PSA to ultrasound-measured prostate volume. Those with a small prostate and a high PSA are more problematic than a large prostate with a relatively lower PSA. Another PSA test that can be used is free to total PSA ratio. Patients with prostate cancer more often have a lower percentage of free PSA. When readings are less than 10 to 15%, prostate cancer is more likely, and readings above 25% are more likely due to BPH. The free-to-total ratio is often used when a repeat biopsy is considered in those who had a previous negative biopsy.
Based on clinical evaluation, a prostate biopsy is performed in those suspected of prostate cancer. The biopsy takes multiple tissue samples but may miss the cancerous tissue. Adenocarcinoma accounts for 99% of prostate malignancies, although lymphomas, sarcomas, and small-cell neuroendocrine tumors may cause prostate cancer. Prostate biopsy is associated with infection, blood in the urine, blood in the semen, urinary retention, and rectal bleeding. Due to the side effects and the pain associated with the procedure, it may not be desired by all patients.
After discussion with the patient, a prostate biopsy may ensue if life expectancy is at least five to ten years and clinical factors suggest prostate cancer (elevated PSA, a rapid increase of PSA, or an abnormality of the DRE). A biopsy may not be indicated for patients with short life expectancies and severe medical comorbidities. After the initial biopsy, a repeat biopsy may be indicated if PSA increases or DRE abnormalities change significantly.
Magnetic resonance imaging (MRI) has become essential to evaluating an elevated PSA. An MRI helps visualize prostatic tumors and helps clinicians better determine who needs a prostate biopsy. A normal MRI is associated with a low risk of invasive prostate cancer, and an abnormal MRI can detect tumors and improve the prostate biopsy's accuracy. The MRI helps clinicians stage the tumor and evaluate the response to treatment. In addition to imaging, newer diagnostic tests (IsoPSA, miR Sentinel tests, and polygenic single-nucleotide panels) are currently being studied to determine who will most likely benefit from a prostate biopsy (Chang et al., 2021).
The biopsy can be done in two ways: transrectal or transperineal. Transrectal biopsy uses a probe in the rectum; the biopsy needle enters the rectum to access the prostate after the anesthetic. Typically, ten to twelve cores are taken to look for cancer. The transperineal technique involves placing a needle in the perineum. This is a cleaner area associated with lower infection rates but is often associated with more pain and requires more sedation. This procedure has similar efficacy to the transrectal biopsy in detecting prostate cancer (Lo et al., 2019). Both techniques use imaging with ultrasound or MRI or both to help assure a safe and accurate procedure. An MRI-guided biopsy is associated with a higher cancer detection rate when compared to an ultrasound-guided biopsy (Das et al., 2020).
The Gleason score and Grade Group are determined after prostate biopsy. The Gleason score is an older system that offers scores based on primary and secondary biopsy grades and is scored on a range from 6-10. The International Society of Urological Pathology revised the grading system into a Grade Group in 2014 (Epstein et al., 2016). The grading system grades cancer from one to five, constructed on primary and secondary Gleason patterns.
The Gleason score and grade are used to classify the severity of the disease. The Gleason grade is based on the features of the prostate cancer cells, and a higher score is associated with an increased risk of severe disease:
Grade Group 1 – Gleason score of 6
Grade Group 2 – Gleason score 3+4=7
Grade Group 3 – Gleason score 4+3=7
Grade Group 4 – Gleason score of 8
Grade Group 5 – Gleason score of 9 or 10
Increased Grade Group is associated with an increased hazard ratio for death. When compared to Grade Group 1, Grade Group 2 is associated with a hazard ratio for death of 2.8, Grade Group 3 is associated with a hazard ratio of 6.0, Grade Group 4 has a hazard ratio of 7.1, and Grade Group 5 has a hazard ratio of 12.7 (Ham et al., 2017). Five-year recurrence-free survival is 95% for Grade Group 1, 83% for Grade Group 2, 65% for Grade Group 3, 63% for Grade Group 4, and 35% for Grade Group 5 (Carter et al., 2012).
Imaging studies are used selectively in the workup of prostate cancer. Common tests include ultrasound, MRI, computed tomography (CT), and bone scan. These studies evaluate the prostate and look for metastatic disease and regional adenopathy. Generally, imaging is not used for very low and low-risk patients, but MRI is sometimes used in very-low and low-risk disease to ensure high-grade disease is not present. Multiparametric MRI can improve the yield of prostate biopsy. The use of bone scans and pelvic imaging are used when the risk is intermediate or higher (Wong et al., 2019).
Prostate MRI is sometimes used to help make decisions regarding the necessity of a prostate biopsy. A patient with an elevated PSA and no suspicious findings on MRI could be considered to forgo a biopsy, especially in an older patient. Transrectal ultrasound can also be considered to evaluate an abnormal DRE. Still, transrectal ultrasound often misses prostate tumors, and even a normal ultrasound in the face of other concerning finding warrants a biopsy (Taplin & Smith, 2022). A biopsy can be performed using a transrectal biopsy with imaging guidance. Transrectal ultrasound or MRI can be used. An MRI-targeted biopsy is more expensive but likely more accurate (Taplin & Smith, 2022).
Prostate-specific membrane antigen positron emission tomography (PSMA-PET) is a more accurate test and can show local disease in the prostate. PSMA-PET demonstrates moderate sensitivity of 68% and a specificity of 94% to detect local prostate cancer (Woo et al., 2020).
Before treatment of prostate cancer, it is essential to fully understand the patient's characteristics, including age, medical comorbidities, overall health, the extent of the disease, the PSA score, the histological grade, and the tumor's molecular characteristics. When these facts are known, the clinician and patient should engage in a conversation to determine optimal treatment options. The clinician should discuss the following:
Treatment options
The probable outcome of each treatment
Complications of each treatment
Patients are risk-stratified using categories created by the National Comprehensive Cancer Network (NCCN). Patients are risk classified as very low, low, favorable, unfavorable, high, and very high (National Comprehensive Cancer Network, 2022):
Very-low-risk disease is associated with a PSA less than 10 ng/mL, PSA density less than 0.15 ng/mL/g, T1c, Grade Group 1, and less than three biopsy cores being positive.
Low-risk disease entails a PSA of less than 10 ng/mL, T1 to T2a, and Grade Group 1.
Favorable intermediate-risk disease includes no high-risk features, no more than one intermediate risk factor - PSA 10-20 ng/mL, T2b to T2c, Grade Group 2-3, and less than 50% positive core biopsies.
Unfavorable intermediate-risk disease includes no high-risk features, two or more of the following - PSA 10-20 ng/mL, T2b to T2c, Grade Group 2-3, and Grade Group 3 and/or more than 50% positive core biopsies.
The high-risk group includes PSA over 20 ng/mL, T3a, or Grade Group 4 or 5.
The very high-risk group includes T3b to T4, more than four cores with Grade Group four or five, or primary Gleason pattern 5.
Localized prostate cancer can be treated in multiple ways. In some cases, it does not need to be treated. Low-risk disease is not associated with a survival benefit from treatment, and treatment is likely not beneficial for those with less than a ten-year life expectancy (Klein, 2022).
Expectant management includes watchful waiting and active surveillance. Active surveillance involves actively looking for progression and treating cancer before progression. All low-risk patients should be considered for active surveillance.Young patients who do not want to experience the potential complications of interventions could be considered for this option. If disease progression is noted in this population, then re-evaluating treatment options need to be considered. Expectant management can also be used in those with Gleason 7. Watchful waiting involves watching for symptoms and palliating symptoms if they occur. Watchful waiting is appropriate for those with significant co-morbidities or older adults.
Localized disease can be treated with radiation or surgery. All patients are candidates for both treatments, so each treatment needs to be considered for all patients. Radiation is less invasive, well tolerated, with lower incontinence rates, and requires less recovery time (Klien, 2022). Surgery offers better pathological staging and more salvage options, and follow-up with recurrence is easier. Surgery following radiation is complex, but radiation following surgery is easier and often done. In addition, when significant LUTS are present, surgery can help relieve the symptoms.
Radiation kills cancer cells by damaging their DNA, and cancer cells have a more challenging time repairing themself when compared to non-cancerous cells. It seeks to radiate cancer cells and minimize radiation exposure to normal tissue. In prostate cancer, radiation can be delivered in two ways, external beam radiation (EBR) and brachytherapy. EBR emits radiation from a machine into the body, and brachytherapy radiation is delivered internally with the radioactive source placed inside the prostate.
The treatment targets the entire prostate, and radiation therapy has similar efficacy to radical prostatectomy for low-risk prostate cancer. As opposed to radical prostatectomy, radiation therapy leaves some normal prostate tissue. Therefore, PSA levels are detectable after treatment, and if PSA rises by two ng/mL or more is suggestive of treatment failure.
Pelvic nodes are often radiated, especially in those with a high spread risk. In low risk of spread, pelvic node radiation may be omitted. Tools are available to predict pelvic lymph node involvement and are often used by radiation oncologists to decide if pelvic node radiation will occur. The spread risk increases with the Gleason score, PSA level, and clinical staging (Klien, 2022).
Complications of EBR include radiation proctitis (occurring in about 5-30% of men), abdominal pain, diarrhea, and tenesmus (DiBiase & Roach, 2022). Treatment involves controlling symptoms with anti-diarrheal agents, which typically resolve within two months. A small percentage of patients have long-term symptoms. Secondary cancers from radiation may take years to decades to develop.
Urinary frequency, urgency, and dysuria are experienced in about 50% of patients, and symptoms typically resolve in a few weeks. Long-term complications are rare. Erectile dysfunction affects about 50% of males two years after EBR (Mahmood, 2016).
Brachytherapy involves implanting radiation in the prostate and typically only involves one or two treatments. The radiation seeds are implanted under ultrasound guidance transperineally. Brachytherapy is used for those with very low, low, or favorable intermediate-risk diseases (NCCN, 2022). Brachytherapy is generally not used for those with a large prostate, after a TURP, or those with significant LUTS(Klein, 2022). Complications of brachytherapy are similar to EBR, including:
Erectile dysfunction
Diarrhea
Rectal urgency
Rectal bleeding
Urinary urgency
Urinary frequency
Dysuria
Patients with unfavorable intermediate- and high-risk localized prostate cancer may be given combined EBR and brachytherapy (Chin et al., 2017). Patients with unfavorable intermediate-risk and high-risk disease are given androgen deprivation therapy (ADT) with radiation therapy (NCCN, 2022). ADT blocks testosterone and deprives cancer cells of testosterone. For patients with unfavorable intermediate-risk, the use of ADT is started two to three months before radiation therapy and continues for four to six months after treatment. ADT with EBR is often used for those with high-or very-high-risk diseases. ADT is often given two to eight months before treatment with radiation, and ADT is continued for about two years.
Both radical prostatectomy and radiation therapy are considered definitive therapies, and the choice is made after a collaborative discussion between provider and patient. Radical prostatectomy is a definitive treatment option for those diagnosed with prostate cancer, and it can be used for intermediate-risk, unfavorable risk disease, and high or very high-risk disease(Tourinho-Barbosa et al., 2018). Radical prostatectomy is often chosen when obstructive LUTS are present, as the surgery may also help relieve symptoms. For younger patients with a longer life-expectancy radical prostatectomy may be preferred as it tends to have improved long-term outcomes.
The robotic approach removes the prostate, sutures the bladder to the urethra, and excises the lymph nodes. This allows staging and may reduce the risk of recurrence. Robotic radical prostatectomy is a two to a four-hour operation that requires a bladder catheter for one week, and the patient is often back to normal in 4-6 weeks. Complications are uncommon, but postoperative issues may occur. Stress incontinence is often seen, but this typically resolves within a year of surgery. Erectile dysfunction may occur and resolve if the nerves can be preserved. Unfortunately, these complications may be permanent.
After surgery, cancer recurrence can occur. Recurrence can be treated. Surveillance involves monitoring PSAs; the level should be undetected or very low. Recurrence is likely if the PSA rises above 0.1 or 0.2 ng/mL. The recurrence risk depends on initial pathology and is highest in individuals with a high PSA, a high Gleason Score, involvement of lymph nodes, positive margins, and extraprostatic extension. If recurrence occurs, salvage radiation may be considered.
Androgens, mainly testosterone and dihydrotestosterone, stimulate prostate cancer cells, and by lowering the levels of androgens, can retard cancer growth. Reducing androgen levels is accomplished by removing the testicles (orchiectomy) or giving medication. Androgen deprivation therapy (ADT) can be used across many prostate cancer stages, localized to metastatic disease.
Luteinizing hormone-releasing hormone (LHRH) agonists lower testosterone and will eventually shrink the testicles. These agents are as effective as orchiectomy in reducing androgens and are reversible. These agents are given periodically from every month to every six months. LHRH agonists include:
Goserelin (Zoladex®)
Leuprolide (Lupron, Eligard®)
Triptorelin (Trelstar®)
Leuprolide mesylate (Camcevi®)
These agents can cause a tumor flare as they briefly spike testosterone levels and may cause the tumor to increase in size, potentially leading to urinary symptoms and bone pain.
LHRH antagonists can also treat prostate cancer but do not cause tumor flare. Agents in this class include:
Degarelix (Firmagon®)
Relugolix (Orgovyx®)
Side effects of hormonal therapy include:
Reduced libido
Depression
Erectile dysfunction
Hot flashes
Memory loss
Anemia
Fatigue
Gynecomastia
Weight gain
Metabolic syndrome
Muscle atrophy
Bone loss
Other treatments target other body parts that make androgens (Kristal et al., 2008). Specific treatments are used to block the adrenal gland and the prostate cancer cells from making androgens, including abiraterone (Zytiga®) and ketoconazole (Nizoral®). Medications that stop androgens from working (anti-androgens) include bicalutamide (Casodex®), flutamide (Eulexin®), and nilutamide (Nilandron®), which are taken as daily pills. Anti-androgens may be used as solo agents but are more often added after orchiectomy or if an LHRH agonist or antagonist is not working as a solo agent. The anti-androgen is sometimes used during the initiation phase of an LHRH agonist to reduce the risk of tumor flare.
Newer anti-androgens, including darolutamide (Nubeqa®), enalutamide (Xtandi®), and apalutamide (Erleada®), are taken as once-daily medications and are often used for castrate-resistant prostate cancer. Enzalutamide is used for both castrate-resistant and castrate-sensitive prostate cancer, and apalutamide and darolutamide are used for metastatic castrate-sensitive prostate cancer. Side effects of these medications include:
Radical prostatectomy and radiation are not effective definitive treatments for metastatic disease. There are two types of metastatic disease, castrate-sensitive and castrate-resistant. These terms discuss the responsiveness of cancer to hormone therapy.
Castrate-sensitive disease (or hormone-sensitive disease) is controlled by maintaining low androgen levels. Prostate cancer is dependent on androgens, and in castrate-sensitive disease, androgen deprivation will control the disease. Reducing androgens can be accomplished by orchiectomy or taking an LHRH antagonist or agonist. Castrate-sensitive metastatic prostate cancer is often treated with agents co-administered with ADT. Popular combination therapies include docetaxel (chemotherapy) with hormone therapy, abiraterone/prednisone/hormone therapy, apalutamide/hormone therapy, and enzalutamide/hormone therapy (Cancer.net, 2021).
Castrate-resistant disease is where cancer progresses even when androgens are suppressed (a serum testosterone level less than 50 ng/dL). Treatments include hormone therapy, abiraterone, or a newer anti-androgen. Other treatment options for prostate cancer include chemotherapy, targeted treatment, and immunotherapy. Chemotherapy can be used in metastatic disease, especially in castrate-resistant disease. It can be given when hormone therapy is ineffective and sometimes may be given along with hormone therapy. Chemotherapeutic agents used to treat prostate cancer include cabazitaxel, mitoxantrone, docetaxel, and estramustine. Targeted treatment includes olaparib (Lynparza®) and rucaparib (Rubraca®), which are classified as PARP inhibitors, and are used for metastatic castrate-resistant prostate cancer.
Immunotherapy uses medication to enhance the immune response to treat cancer cells. A cancer vaccine, individually made for each person, called sipuleucel-T, can be used to treat advanced prostate cancer. While not a cure, it can extend life expectancy.
Immune checkpoint inhibitors are used to help manage advanced prostate cancer. "Checkpoints" are proteins that reside on immune cells that behave like switches to start an immune response. Cancer cells utilize checkpoints to protect themselves from the immune system. These medications are utilized in metastatic disease, recurrent disease, or after chemotherapy. Pembrolizumab (Keytruda®) is a medication given intravenously every two to three weeks, and it targets the PD-1 checkpoint to boost the immune system's fight against prostate cancer. This medication removes the breaks from the immune system and may lead to certain autoimmune diseases.
John is a 58-year-old male diagnosed with Gleason 6 prostate cancer five years ago and treated with radical prostatectomy. He has his annual checkups with his urologist, who performs regular PSA tests. His PSA was undetectable for the first two years, and then the levels rose to 0.6 ng/dL in the third year and 1.3 ng/dL in the fourth year.
In the fifth year, he neglects to return for his follow-up exam. He had recently retired and was enjoying traveling with his wife. In the sixth year after his prostate surgery, he started to feel fatigued. Over the next month, he reported having increased back pain and had a 10-pound weight loss. One evening his back pain became severe, and he presented to the emergency department. The workup in the emergency department showed that the patient had anemia, an elevated creatinine level, and elevated alkaline phosphatase. Further workup showed a PSA of 103 ng/dL.
A lumbar spine x-ray is negative, but a bone scan shows scattered metastatic lesions in the spine. The oncologist decides to treat with androgen deprivation therapy and docetaxel. Over the next few months, the patient does well, resulting in a PSA reduction to 22.0 ng/dL.
The patient's prostate cancer is controlled over three years with a stable PSA while on ADT. Eventually, the PSA increases, and the patient is referred back to the oncologist to assess treatment options.
Benign prostatic hyperplasia and prostate cancer are diseases that typically affect elderly patients. BPH presents with symptoms localized to the urinary tract. With BPH, treatment involves controlling symptoms with medical interventions before surgical interventions.
In patients with prostate cancer, treatment decisions are made under two main paradigms: disease control and cure. The decision is made with the patient's input, keeping in mind their quality of life and life expectancy. Physicians, nurses, and other clinical providers are responsible for empowering patients in making decisions regarding treatment options, including the decision not to pursue any treatment.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
American Cancer Society. (ACS). (2020). Prostate cancer risk factors. American Cancer Society (ACS). Visit Source.
Andriole, G. (2022). Benign prostatic hypertrophy (BPH). Merck Manual: Professional Version. Visit Source.
Bleyer, A., Spreafico, F., & Barr, R. (2020). Prostate cancer in young men: An emerging young adult and older adolescent challenge. Cancer, 126(1), 46–57. Visit Source.
Bortnick, E., Brown, C., Simma-Chiang, V., & Kaplan, S. (2020). Modern best practice in the management of benign prostatic hyperplasia in the elderly. Therapeutic Advances in Urology, 12, 1756287220929486. Visit Source.
Calogero, A. E., Burgio, G., Condorelli, R. A., Cannarella, R., & La Vignera, S. (2019). Epidemiology and risk factors of lower urinary tract symptoms/benign prostatic hyperplasia and erectile dysfunction. The Aging Male: The Official Journal of the International Society for the Study of the Aging Male, 22(1), 12–19. Visit Source.
Cancer.Net. (2021). Prostate cancer: Types of treatment. Cancer.Net. Visit Source.
Carter, H. B., Partin, A. W., Walsh, P. C., Trock, B. J., Veltri, R. W., Nelson, W. G., Coffey, D. S., Singer, E. A., & Epstein, J. I. (2012). Gleason score 6 adenocarcinoma: Should it be labeled as cancer? Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 30(35), 4294–4296. Visit Source.
Chang, E. K., Gadzinski, A., & Nyame, Y. (2021). Blood and urine biomarkers in prostate cancer: Are we ready for reflex testing in men with an elevated prostate-specific antigen? Asian Journal of Urology, 8(4), 343–353. Visit Source.
Chin, J., Rumble, R. B., Kollmeier, M., Heath, E., Efstathiou, J., Dorff, T., Berman, B., Feifer, A., Jacques, A., & Loblaw, D. A. (2017). Brachytherapy for patients with prostate cancer: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 35(15), 1737–1743. Visit Source.
Cimino, S., Voce, S., Palmieri, F., Favilla, V., Castelli, T., Privitera, S., Giardina, R., Reale, G., Russo, G. I., & Morgia, G. (2017). Transurethral resection of the prostate (TURP) vs. GreenLight photoselective vaporization of benign prostatic hyperplasia: Analysis of BPH6 outcomes after 1 year of follow-up. International Journal of Impotence Research, 29(6), 240–243. Visit Source.
Cornu, J. N., Ahyai, S., Bachmann, A., de la Rosette, J., Gilling, P., Gratzke, C., McVary, K., Novara, G., Woo, H., & Madersbacher, S. (2015). A systematic review and meta-analysis of functional outcomes and complications following transurethral procedures for lower urinary tract symptoms resulting from benign prostatic obstruction: An update. European Urology, 67(6), 1066–1096. Visit Source.
Csikós, E., Horváth, A., Ács, K., Papp, N., Balázs, V. L., Dolenc, M. S., Kenda, M., Kočevar Glavač, N., Nagy, M., Protti, M., Mercolini, L., Horváth, G., Farkas, Á., & On Behalf Of The Oemonom (2021). Treatment of benign prostatic hyperplasia by natural drugs. Molecules (Basel, Switzerland), 26(23), 7141. Visit Source.
Das, C. J., Netaji, A., Razik, A., & Verma, S. (2020). MRI-Targeted prostate biopsy: What radiologists should know? Korean Journal of Radiology, 21(9), 1087–1094. Visit Source.
Delongchamps, N. B., Singh, A., & Haas, G. P. (2006). The role of prevalence in the diagnosis of prostate cancer. Cancer Control: Journal of the Moffitt Cancer Center, 13(3), 158–168. Visit Source.
Deters, L. (2021). Benign prostatic hypertrophy (BPH). Medscape. Visit Source.
DiBiase, S. J. & Roach, M. (2022). External beam radiation therapy for localized prostate cancer. UpToDate. Visit Source.
Dhaliwal, D. & Gupta, M. (2022). PDE5 Inhibitors. National Library of Medicine. StatPearls. Visit Source.
Elterman, D., Shepherd, S., Saadat, S. H., Alshak, M. N., Bhojani, N., Zorn, K. C., Rijo, E., Misrai, V., Lajkosz, K., & Chughtai, B. (2021). Prostatic urethral lift (UroLift) versus convective water vapor ablation (Rezum) for minimally invasive treatment of BPH: A comparison of improvements and durability in 3-year clinical outcomes. The Canadian Journal of Urology, 28(5), 10824–10833. Visit Source.
Epstein, J. I., Egevad, L., Amin, M. B., Delahunt, B., Srigley, J. R., Humphrey, P. A., & Grading Committee (2016). The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason grading of prostatic carcinoma: Definition of grading patterns and proposal for a new grading system. The American Journal of Surgical Pathology, 40(2), 244–252. Visit Source.
Gormley, G. J., Stoner, E., Bruskewitz, R. C., Imperato-McGinley, J., Walsh, P. C., McConnell, J. D., Andriole, G. L., Geller, J., Bracken, B. R., & Tenover, J. S. (1992). The effect of finasteride in men with benign prostatic hyperplasia. The Finasteride Study Group. The New England Journal of Medicine, 327(17), 1185–1191. Visit Source.
Ham, W. S., Chalfin, H. J., Feng, Z., Trock, B. J., Epstein, J. I., Cheung, C., Humphreys, E., Partin, A. W., & Han, M. (2017). New prostate cancer grading system predicts long-term survival following surgery for Gleason score 8-10 prostate cancer. European Urology, 71(6), 907–912. Visit Source.
Han, I. H., Song, H. O., & Ryu, J. S. (2020). IL-6 produced by prostate epithelial cells stimulated with Trichomonas vaginalis promotes proliferation of prostate cancer cells by inducing M2 polarization of THP-1-derived macrophages. PLoS Neglected Tropical Diseases, 14(3), e0008126. Visit Source.
Hartung, F. O., Kowalewski, K. F., von Hardenberg, J., Worst, T. S., Kriegmair, M. C., Nuhn, P., Herrmann, T., Michel, M. S., & Herrmann, J. (2022). Holmium versus thulium laser enucleation of the prostate: A systematic review and meta-analysis of randomized controlled trials. European Urology Focus, 8(2), 545–554. Visit Source.
Harvard School of Public Health. (2019). Diet may affect prostate cancer risk. Harvard School of Public Health. Visit Source.
Ilic, D., Djulbegovic, M., Jung, J. H., Hwang, E. C., Zhou, Q., Cleves, A., Agoritsas, T., & Dahm, P. (2018). Prostate cancer screening with prostate-specific antigen (PSA) test: A systematic review and meta-analysis. BMJ (Clinical research ed.), 362, k3519. Visit Source.
Kang, T. W., Kim, S. J., Kim, M. H., & Jung, J. H. (2021). Beta 3 adrenoreceptor agonist for the management of lower urinary tract symptoms in men with benign prostatic hyperplasia: A systematic review. International Neurourology Journal, 25(3), 182–191. Visit Source.
Kaplan, S. A., Herschorn, S., McVary, K. T., Staskin, D., Chapple, C., Foley, S., Cambronero Santos, J., Kristy, R. M., Choudhury, N., Hairston, J., & Schermer, C. R. (2020). Efficacy and safety of mirabegron versus placebo add-on therapy in men with overactive bladder symptoms receiving tamsulosin for underlying benign prostatic hyperplasia: A randomized, phase 4 study (PLUS). The Journal of Urology, 203(6), 1163–1171. Visit Source.
Klein, E. A. (2022). Localized prostate cancer: Risk stratification and choice of initial treatment. UpToDate. Visit Source.
Kuntz, R. M., Lehrich, K., & Ahyai, S. A. (2008). Holmium laser enucleation of the prostate versus open prostatectomy for prostates greater than 100 grams: 5-year follow-up results of a randomised clinical trial. European Urology, 53(1), 160–166. Visit Source.
Kristal, A. R., Schenk, J. M., Song, Y., Arnold, K. B., Neuhouser, M. L., Goodman, P. J., Lin, D. W., Stanczyk, F. Z., & Thompson, I. M. (2008). Serum steroid and sex hormone-binding globulin concentrations and the risk of incident benign prostatic hyperplasia: Results from the prostate cancer prevention trial. American Journal of Epidemiology, 168(12), 1416–1424. Visit Source.
Lerner, L. B., McVary, K. T., Barry, M. J., Bixler, B. R., Dahm, P., Das, A. K., Gandhi, M. C., Kaplan, S. A., Kohler, T. S., Martin, L., Parsons, J. K., Roehrborn, C. G., Stoffel, J. T., Welliver, C., & Wilt, T. J. (2021a). Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA GUIDELINE PART I-Initial workup and medical management. The Journal of Urology, 206(4), 806–817. Visit Source.
Lerner, L. B., McVary, K. T., Barry, M. J., Bixler, B. R., Dahm, P., Das, A. K., Gandhi, M. C., Kaplan, S. A., Kohler, T. S., Martin, L., Parsons, J. K., Roehrborn, C. G., Stoffel, J. T., Welliver, C., & Wilt, T. J. (2021b). Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA GUIDELINE PART II-surgical evaluation and treatment. The Journal of Urology, 206(4), 818–826. Visit Source.
Lim Ng, K., & Barber, N. (2019). Prostatic hydroablation (Aquablation): A new effective ultrasound guided robotic waterjet ablative surgery for treatment of benign prostatic hyperplasia. Archivos Espanoles de Urologia, 72(8), 786–793. Visit Source.
Lim, K. B. (2017). Epidemiology of clinical benign prostatic hyperplasia. Asian Journal of Urology, 4(3), 148–151. Visit Source.
Lo, K. L., Chui, K. L., Leung, C. H., Ma, S. F., Lim, K., Ng, T., Wong, J., Li, J., Mak, S. K., & Ng, C. F. (2019). Outcomes of transperineal and transrectal ultrasound-guided prostate biopsy. Hong Kong Medical Journal, 25(3), 209–215. Visit Source.
Mahmood, J., Shamah, A. A., Creed, T. M., Pavlovic, R., Matsui, H., Kimura, M., Molitoris, J., Shukla, H., Jackson, I., & Vujaskovic, Z. (2016). Radiation-induced erectile dysfunction: Recent advances and future directions. Advances in Radiation Oncology, 1(3), 161–169. Visit Source.
Maserejian, N. N., Wager, C. G., Giovannucci, E. L., Curto, T. M., McVary, K. T., & McKinlay, J. B. (2013). Intake of caffeinated, carbonated, or citrus beverage types and development of lower urinary tract symptoms in men and women. American Journal of Epidemiology, 177(12), 1399–1410. Visit Source.
McVary, K. T., Gange, S. N., Gittelman, M. C., Goldberg, K. A., Patel, K., Shore, N. D., Levin, R. M., Rousseau, M., Beahrs, J. R., Kaminetsky, J., Cowan, B. E., Cantrill, C. H., Mynderse, L. A., Ulchaker, J. C., Larson, T. R., Dixon, C. M., & Roehrborn, C. G. (2016). Minimally invasive prostate convective water vapor energy ablation: A multicenter, randomized, controlled study for the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia. The Journal of Urology, 195(5), 1529–1538. Visit Source.
McVary, K. T., Rogers, T., & Roehrborn, C. G. (2019). Rezūm water vapor thermal therapy for lower urinary tract symptoms associated with benign prostatic hyperplasia: 4-year results from randomized controlled study. Urology, 126, 171–179. Visit Source.
McVary, K. T. (2021a). Epidemiology and pathophysiology of benign prostatic hyperplasia. UpToDate. Visit Source.
McVary, K. T. (2021b). Clinical manifestations and diagnostic evaluation of benign prostatic hyperplasia. UpToDate. Visit Source.
McVary, K. (2022). Medical treatment of benign prostatic hyperplasia. UpToDate. Visit Source.
Mullen, G. R., & Kaplan, S. A. (2021). Efficacy and safety of mirabegron in men with overactive bladder symptoms and benign prostatic hyperplasia. Current Urology Reports, 22(1), 5. Visit Source.
Murphy, A. B., Akereyeni, F., Nyame, Y. A., Guy, M. C., Martin, I. K., Hollowell, C. M., Walker, K., Kittles, R. A., & Ahaghotu, C. (2013). Smoking and prostate cancer in a multi-ethnic cohort. The Prostate, 73(14), 1518–1528. Visit Source.
Na, R., Helfand, B. T., Chen, H., Conran, C. A., Crawford, S. E., Hayward, S. W., Tammela, T., Hoffman-Bolton, J., Zheng, S. L., Walsh, P. C., Schleutker, J., Platz, E. A., Isaacs, W. B., & Xu, J. (2017). A genetic variant near GATA3 implicated in inherited susceptibility and etiology of benign prostatic hyperplasia (BPH) and lower urinary tract symptoms (LUTS). The Prostate, 77(11), 1213–1220. Visit Source.
National Cancer Institute. (NCI). (2022) Cancer stat facts: Prostate cancer. National Institute of Health (NIH). Visit Source.
National Comprehensive Cancer Network. (2022). Prostate cancer. Official Journal of the National Comprehensive Cancer Network. Visit Source.
Negri, E., Pelucchi, C., Talamini, R., Montella, M., Gallus, S., Bosetti, C., Franceschi, S., & La Vecchia, C. (2005). Family history of cancer and the risk of prostate cancer and benign prostatic hyperplasia. International Journal of Cancer, 114(4), 648–652. Visit Source.
Nickel, J. C., Gilling, P., Tammela, T. L., Morrill, B., Wilson, T. H., & Rittmaster, R. S. (2011). Comparison of dutasteride and finasteride for treating benign prostatic hyperplasia: The Enlarged Prostate International Comparator Study (EPICS). BJU International, 108(3), 388–394. Visit Source.
Olivas, A., & Price, R. S. (2021). Obesity, inflammation, and advanced prostate cancer. Nutrition and Cancer, 73(11-12), 2232–2248. Visit Source.
Orlich, M. J., Mashchak, A. D., Jaceldo-Siegl, K., Utt, J. T., Knutsen, S. F., Sveen, L. E., & Fraser, G. E. (2022). Dairy foods, calcium intakes, and risk of incident prostate cancer in Adventist Health Study-2. The American Journal of Clinical Nutrition, 116(2), 314–324. Visit Source.
Pattanaik, S., Mavuduru, R. S., Panda, A., Mathew, J. L., Agarwal, M. M., Hwang, E. C., Lyon, J. A., Singh, S. K., & Mandal, A. K. (2019). Phosphodiesterase inhibitors for lower urinary tract symptoms consistent with benign prostatic hyperplasia. BJU International, 124(1), 27–34. Visit Source.
Pernar, C. H., Ebot, E. M., Wilson, K. M., & Mucci, L. A. (2018). The epidemiology of prostate cancer. Cold Spring Harbor Perspectives in Medicine, 8(12), a030361. Visit Source.
Platz, E. A., Joshu, C. E., Mondul, A. M., Peskoe, S. B., Willett, W. C., & Giovannucci, E. (2012). Incidence and progression of lower urinary tract symptoms in a large prospective cohort of United States men. The Journal of Urology, 188(2), 496–501. Visit Source.
Roehrborn, C. G., Barkin, J., Gange, S. N., Shore, N. D., Giddens, J. L., Bolton, D. M., Cowan, B. E., Cantwell, A. L., McVary, K. T., Te, A. E., Gholami, S. S., Moseley, W. G., Chin, P. T., Dowling, W. T., Freedman, S. J., Incze, P. F., Coffield, K. S., Herron, S., Rashid, P., & Rukstalis, D. B. (2017). Five year results of the prospective randomized controlled prostatic urethral L.I.F.T. study. The Canadian Journal of Urology, 24(3), 8802–8813. Visit Source.
Sanda, M. G., Doehring, C. B., Binkowitz, B., Beaty, T. H., Partin, A. W., Hale, E., Stoner, E., & Walsh, P. C. (1997). Clinical and biological characteristics of familial benign prostatic hyperplasia. The Journal of Urology, 157(3), 876–879. Visit Source.
Sandhu, J. S., Leong, J. Y., & Das, A. K. (2019). Photoselective vaporization of the prostate: Application, outcomes and safety. The Canadian Journal of Urology, 26(4 Suppl 1), 8–12. Visit Source.
Sartor, A. O. (2022). Risk factors for prostate cancer. UpToDate. Visit Source.
Siegel, R. L., Miller, K. D., Fuchs, H. E., & Jemal, A. (2022). Cancer statistics, 2022. CA: A Cancer Journal for Clinicians, 72(1), 7–33. Visit Source.
Sun, I., Yoo, S., Park, J., Cho, S. Y., Jeong, H., Son, H., Oh, S. J., Paick, J. S., & Cho, M. C. (2019). Quality of life after photo-selective vaporization and holmium-laser enucleation of the prostate: 5-year outcomes. Scientific Reports, 9(1), 8261. Visit Source.
Taplin, M., & Smith, J. A. (2022). Clinical presentation and diagnosis of prostate cancer. UpToDate. Visit Source.
Tourinho-Barbosa, R., Srougi, V., Nunes-Silva, I., Baghdadi, M., Rembeyo, G., Eiffel, S. S., Barret, E., Rozet, F., Galiano, M., Cathelineau, X., & Sanchez-Salas, R. (2018). Biochemical recurrence after radical prostatectomy: What does it mean? International Brazilian Journal Urology: Official Journal of the Brazilian Society of Urology, 44(1), 14–21. Visit Source.
United States Preventive Services Task Force, Grossman, D. C., Curry, S. J., Owens, D. K., Bibbins-Domingo, K., Caughey, A. B., Davidson, K. W., Doubeni, C. A., Ebell, M., Epling, J. W., Jr, Kemper, A. R., Krist, A. H., Kubik, M., Landefeld, C. S., Mangione, C. M., Silverstein, M., Simon, M. A., Siu, A. L., & Tseng, C. W. (2018). Screening for prostate cancer: US Preventive Services Task Force Recommendation Statement. Journal of the American Medical Association (JAMA), 319(18), 1901–1913. Visit Source.
Wei, J. T., Calhoun, E., & Jacobsen, S. J. (2008). Urologic diseases in America project: benign prostatic hyperplasia. The Journal of Urology, 179(5 Suppl), S75–S80. Visit Source.
Welliver, C., Feinstein, L., Ward, J. B., Fwu, C. W., Kirkali, Z., Bavendam, T., Matlaga, B. R., McVary, K. T., & Urologic Diseases in America Project (2020). Trends in lower urinary tract symptoms associated with benign prostatic hyperplasia, 2004 to 2013: The Urologic Diseases in America Project. The Journal of Urology, 203(1), 171–178. Visit Source.
Wilson, K. M., Kasperzyk, J. L., Rider, J. R., Kenfield, S., van Dam, R. M., Stampfer, M. J., Giovannucci, E., & Mucci, L. A. (2011). Coffee consumption and prostate cancer risk and progression in the Health Professionals Follow-up Study. Journal of the National Cancer Institute, 103(11), 876–884. Visit Source.
Wong, S. K., Mohamad, N. V., Giaze, T. R., Chin, K. Y., Mohamed, N., & Ima-Nirwana, S. (2019). Prostate Cancer and Bone Metastases: The Underlying Mechanisms. International Journal of Molecular Sciences, 20(10), 2587. Visit Source.
Woo, S., Ghafoor, S., Becker, A. S., Han, S., Wibmer, A. G., Hricak, H., Burger, I. A., Schöder, H., & Vargas, H. A. (2020). Prostate-specific membrane antigen positron emission tomography (PSMA-PET) for local staging of prostate cancer: A systematic review and meta-analysis. European Journal of Hybrid Imaging, 4(1), 16. Visit Source.
World Cancer Research Fund International. (2022). Prostate cancer statistics. World Cancer Research Fund International. Visit Source.
Wroclawski, M. L., Carneiro, A., Amarante, R. D., Oliveira, C. E., Shimanoe, V., Bianco, B. A., Sakuramoto, P. K., & Pompeo, A. C. (2016). 'Button type' bipolar plasma vaporisation of the prostate compared with standard transurethral resection: A systematic review and meta-analysis of short-term outcome studies. BJU International, 117(4), 662–668. Visit Source.
Xu, Y., Li, L., Yang, W., Zhang, K., Ma, K., Xie, H., Zhou, J., Cai, L., Gong, Y., Zhang, Z., & Gong, K. (2021). Association between vasectomy and risk of prostate cancer: A meta-analysis. Prostate Cancer and Prostatic Diseases, 24(4), 962–975. Visit Source.
Ziętek, R. J., & Ziętek, Z. M. (2021). Transurethral Microwave Thermotherapy (TUMT) in the Treatment of Benign Prostatic Hyperplasia: A Preliminary Report. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research, 27, e931597. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.