This course will be updated or discontinued on or before Monday, August 31, 2026
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will know what the risks and complications are of a cesarean section delivery.
Objectives
After completing this continuing education course, the participant will be able to:
Identify why cesarean sections are necessary.
Determine the complications that are associated with cesarean sections.
Explain how to prevent complications from a cesarean section.
List the long-term risks that are associated with cesarean sections.
Examine the psychological impact that is associated with cesarean sections.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Cesarean section, more commonly known as “c-section”, rates vary across the United States. According to the most recent birth statistics from the Centers for Disease Control and Prevention’s National Center for Health Statistics, the rates of c-sections have increased substantially from 5% in 1970 to 32.1% in 2022 (Centers for Disease Control and Prevention [CDC], 2024; Sung & Mahdy, 2023). In the United States, the c-section is the most common surgery, with over one million c-sections performed each year (Sung & Mahdy, 2023). There are risks and benefits to both vaginal birth and c-sections. There are certain circumstances in which a c-section is the safest delivery route for the mother and/or the fetus, even with the increased risks of surgery (Sung & Mahdy, 2023).
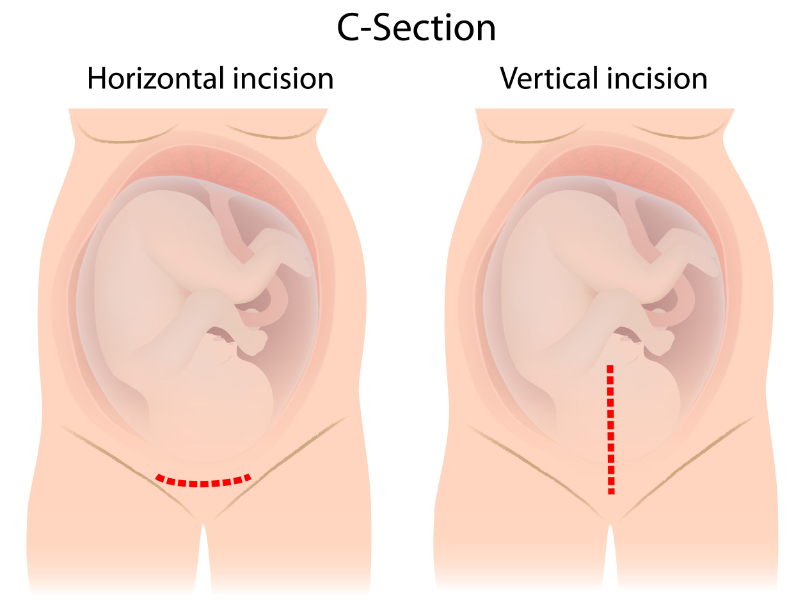
Maternal indications can include a prior c-section. One (or even two) c-sections does not mean that a woman must have a c-section delivery with her next pregnancy. The woman should be evaluated and have discussions with her provider. The risk of uterine rupture is slightly higher, but she can be monitored for signs of uterine rupture during labor.
A vertical incision in the uterus, however, would not make her a candidate for a trial of labor after cesarean (TOLAC) (American College of Obstetricians and Gynecologists [ACOG], 2019).
Image 1: Horizontal vs. Vertical C-Section Incisions
Other maternal reasons for c-sections can include (Sung & Mahdy, 2023):
Maternal request
Pelvic deformity
Previous perineal trauma
Prior pelvic or anal reconstructive surgery
Cardiac disease
Pulmonary disease
Herpes simplex virus (HSV) infection
HIV infection
Cerebral aneurysm
Arteriovenous malformations
Perimortem c-section
Both HIV and active HSV can be spread easier to the fetus in a vaginal delivery.
Uterine or anatomic conditions that are an indication for c-section include abnormal placentation, such as placenta previa or accreta, because the fetus cannot be delivered vaginally through the placenta. A prior classical hysterotomy (vertical incision, as mentioned above) during a c-section is also a reason for a c-section, as this increases the risk of uterine rupture (MedlinePlus, 2022). A prior myomectomy or history of uterine incision dehiscence, as well as invasive cervical cancer, a genital tract obstructive mass, or a permanent cerclage are all indications for a c-section (Sung & Mahdy, 2023).
Fetal indications for a c-section include (Sung & Mahdy, 2023):
A non-reassuring fetal status
Umbilical cord prolapse
Failed operative vaginal delivery
Malpresentation
Macrosomia
Congenital anomaly
Thrombocytopenia
Previous delivery with a neonatal birth trauma
Fetal heart monitoring is often used during labor. Fetal heart monitoring is complex and requires additional, specialized training of the nurse. Changes in the fetal heart pattern can help to assess the fetal oxygenation status. During labor fetal position changes and uterine contractions have the potential to lead to fetal hypoxia (Kauffmann & Silberman, 2023). Fetal heart monitoring is not perfect, but there are no better options at this point to assess the fetal status during labor. Low risk women are not recommended to have continuous fetal monitoring, as it has been shown to cause a higher rate of c-sections (Kauffmann & Silberman, 2023).
Some other miscellaneous reasons have also likely increased the risk of a c-section over time. Possible miscellaneous reasons for c-section can include (Bjorklund et al., 2022; Njogu et al., 2022; Mayo Clinic, 2022a; Rydahl et al., 2019):
Increased maternal age during pregnancy
Increased obesity
Incidences of gestational diabetes
Increased use of fertility treatments
Another factor that may increase the c-section rate is the medical-legal aspect of labor and delivery. Malpractice rates and no cap limits on birth injuries may possibly influence a provider’s decision to perform a c-section.
The cesarean section mortality rate in the United States is 2.2 per 100,000 c-sections (Sung & Mahdy, 2023). The mortality rate for vaginal deliveries is only 0.2 per 100,000 (Sung & Mahdy, 2023).
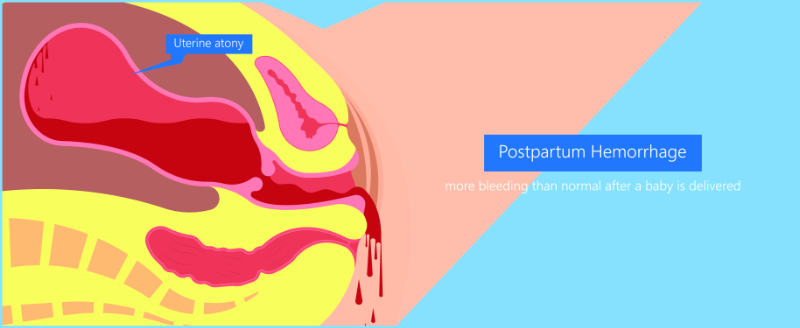
Postpartum hemorrhage (PPH) is the leading cause of maternal morbidity in the United States (Sung & Mahdy, 2023). C-sections are one major factor that can increase the risk of hemorrhage.
Image 2: Postpartum Hemorrhage
C-sections put the patient at risk of having abnormal placentation, uterine rupture, and adhesions in future pregnancies, which further increases the risk of PPH (Burke & Allen, 2020). PPH is complex, but can lead to transfusion, need for intensive care, and unplanned hysterectomy (Burke & Allen, 2020).
Other intraoperative complications that could occur during a c-section can include:
Surgical injury to the mother, such as a bladder injury
Surgical injury to the fetus, such as a facial laceration
Bowel obstruction
Incisional hernia
Following c-section delivery, there is generally more intense pain associated with a c-section recovery versus an uncomplicated vaginal birth (Larsson et al., 2021). Because of this, a woman may have more difficulty moving and caring for her newborn.
Endometritis, infections, and wound complications all can occur with a c-section. Surgical site infections (SSI) affect between 3% to 18% of all patients who have a c-section (Erritty et al., 2023). SSI’s can be superficial or deep, which can result in an abscess, which can lead the wound to dehisce (open). Endometritis can occur when the infection involves the decidual layer of the uterus (Larsson et al., 2021).
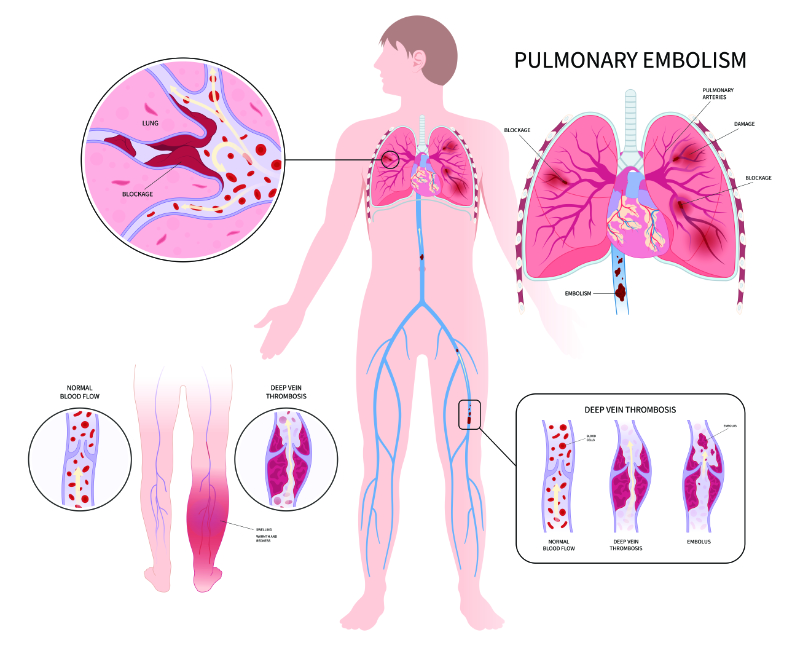
A thrombotic event such as ischemic stroke, acute myocardial infarction, or venous thromboembolism (VTE) during the first 6 weeks postpartum occurs significantly more often after a c-section birth than vaginal birth because these patients have a higher coagulopathy activation, making them four times more at risk of developing a VTE than a patient who had a vaginal delivery (Burke & Allen, 2020).
Image 3: Venous Thromboembolism (VTE)
Approximately 80% of VTEs are deep vein thrombosis (DVT) and 20% are pulmonary embolism (PE). PEs are less common but may account for up to 10% of maternal deaths (Burke & Allen, 2020).
C-section surgery anesthesia-related complications are possible. A woman undergoing a c-section could react to the given anesthesia. Neuraxial anesthesia is often used with few complications and is the gold standard for c-sections, but general anesthesia may be used in an emergency case (Ring et al., 2021). Failed intubation is a complication of general anesthesia that is more common in pregnant women (Ring et al., 2021). In addition, changes in a pregnant patient’s respiratory system can put them at risk for rapid onset profound hypoxemia (Ring et al., 2021). Aspiration is rare, but serious and can also occur with general anesthesia as can malignant hyperthermia. General anesthesia can also lead to poor neonatal outcomes, such as lower neonatal APGAR scores, more assisted ventilation and more admissions to the neonatal intensive care unit (NICU) (Ring, et al., 2021).
Many of the associated complications we have reviewed can be prevented. Hemorrhage cannot always be prevented, but recognition and treatment can help to reduce morbidity and mortality (Wormer et al., 2023). Patients need to have their hemodynamic status monitored and treat blood loss quickly. Every labor unit should use hemorrhage protocols and have supplies readily accessible. A multidisciplinary team who is educated and performs drills can help to manage these patients best (Burke & Allen, 2020).
Infections can be prevented by using a strict sterile technique, providing intravenous (IV) antibiotics within 60 minutes before incision, and using a chlorhexidine-alcohol or betadine scrub before the surgery (Burke & Allen, 2020).A vaginal cleanse should also be performed if the woman has labored before the c-section. It is also important to warm the patient, using active and passive measures (such as warmed air, warm blankets, and warmed IV fluids). Preventing hypothermia can also help to prevent infection (Burke & Allen, 2020).
If hair removal is needed, this should be done by clipping, not shaving. For all women undergoing cesarean delivery, mechanical thromboprophylaxis (with pneumatic compression devices) is recommended. For women with a high risk of venous thromboembolism (VTE), mechanical thromboprophylaxis and pharmacologic thromboprophylaxis (Lovenox, Heparin) is recommended. Mechanical and pharmacologic prophylaxis should be continued until the woman is fully ambulating (Burke & Allen, 2020).
Multimodal pain relief options should help the woman move easier and care for her baby while preventing the overuse of narcotics. Early ambulation and oral intake have been shown to promote recovery.
Long-term risks from a c-section can be serious. A cesarean delivery significantly increases the risk of abnormal placentation in future pregnancies, often due to scarring from the c-section itself (Mayo Clinic, 2022b). This risk increases with each subsequent c-section.
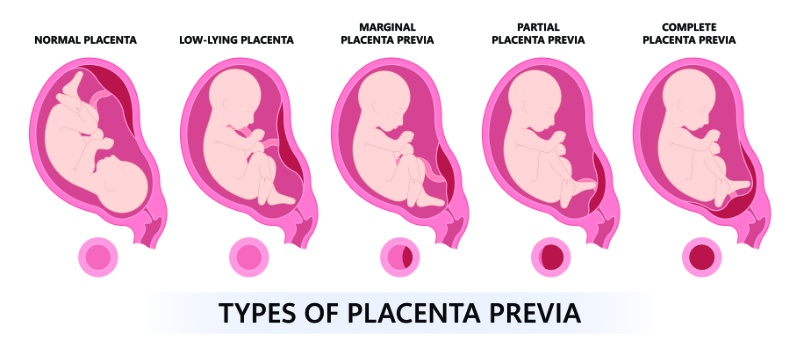
Placenta previa can occur when the placenta implants and covers part or all of the woman’s cervix, making vaginal delivery impossible (Mayo Clinic, 2022c).
Image 4: Types of Placental Previa
This can cause bleeding throughout pregnancy or significant hemorrhage. The severity of bleeding will determine the delivery timing and may lead to preterm delivery (Mayo Clinic, 2022c).
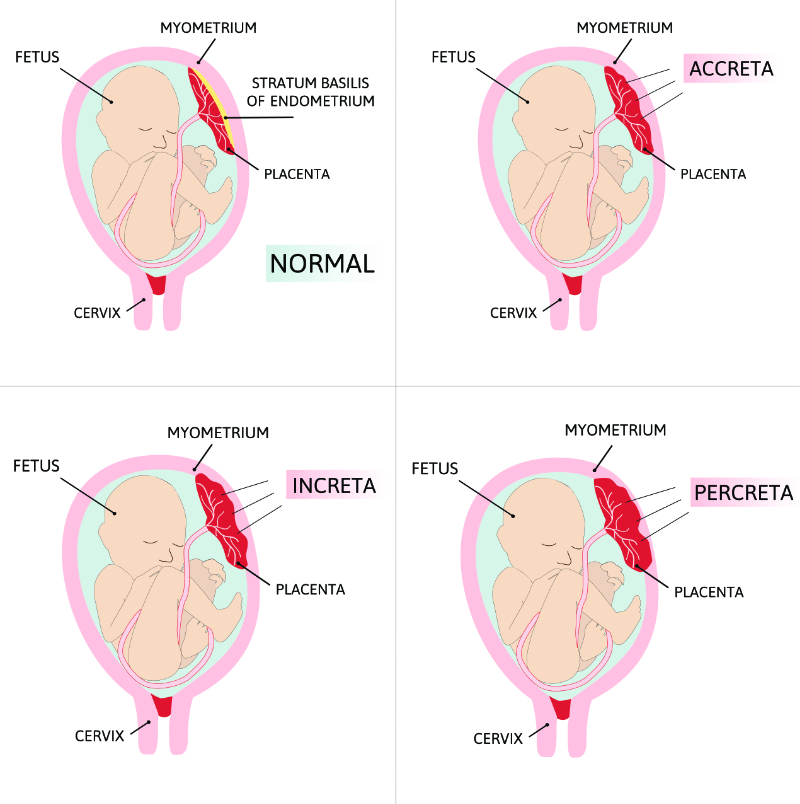
The placenta accreta spectrum refers to the range of adherence of the placenta, including placenta accreta, placenta increta, and placenta percreta (Cleveland Clinic, 2022).
Image 5: Types of Placenta Accreta
The placenta accreta spectrum is the invasion of part or all of the placenta into the myometrium of the uterine wall. As pictured above, the three types of placenta accreta can include (Cleveland Clinic, 2022):
Placenta accreta: Attachment to the wall of the uterus, but it does not pass through the wall and impact the uterine muscle.
Placenta increta: Deeply embedded in the wall of the uterus, still not passing through the uterine wall, but securely attached to the uterine muscle.
Placenta percreta: Placental development through the wall of the uterus and potentially impacting other organs, such as the bladder or intestines.
Placenta accreta is serious and requires extensive surgery (Cleveland Clinic, 2022). The woman may require a hysterectomy to prevent death from hemorrhage. A surgical team must plan blood product replacements and hemodynamic monitoring for the woman (Rathbun & Hildebrand, 2022).
Women with c-sections are also at risk for uterine rupture in future pregnancies. This risk increases with a trial of labor after a cesarean, although this risk is low and does not always prevent a vaginal delivery after cesarean (ACOG, 2019).
A c-section can have short- and long-term psychological effects for the woman. Women may be more likely to experience postpartum depression. A c-section may lead to Post-traumatic Stress Disorder (PTSD) for a woman who required an emergency c-section, with some reporting an intense fear of death or injury for themselves or their babies during delivery (Benton et al., 2019). These women may complain of poorer physical functioning, as well as issues with maternal-infant bonding as well.
It is important to remember that many women who deliver via c-section may feel a loss of perceived control of their birth experience, as well as helplessness, and disappointment at the birth experience that they had (Benton et al., 2019). Women who are having these feelings may need extra support and resources.
Cecilia comes to your labor and delivery unit. She wants to have a trial of labor after cesarean (TOLAC). Her first c-section was for a non-reassuring fetal heart rate. That baby was born with an umbilical cord around the neck but was fine after delivery.
Cecilia is 6cm dilated and contracting every 2 minutes. Her vital signs are normal.
Is Cecilia a candidate for a TOLAC?
Yes, Cecilia is a candidate for TOLAC. She had her first c-section due to fetal distress. She is a candidate as long as she did not have a vertical uterine incision with her first baby.
What is the biggest risk for Cecilia during labor, given that the pregnancy has been normal until labor?
The biggest risk for Cecilia with a TOLAC is that of a uterine rupture because having had a c-section, she has scarring on her uterus.
Cesarean sections are necessary to prevent maternal or fetal risks or death in certain circumstances. A c-section is not the appropriate method of delivery for every woman. There are risks to both the mom and fetus. The benefits and risks must be weighed before a c-section delivery should take place.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
American College of Obstetricians and Gynecologists. (ACOG). (2019). ACOG Practice Bulletin No. 205: Vaginal birth after cesarean delivery. Obstetrics and gynecology, 133(2), e110–e127. Visit Source.
Benton, M., Salter, A., Tape, N., Wilkinson, C., & Turnbull, D. (2019). Women's psychosocial outcomes following an emergency cesarean section: A systematic literature review. BMC pregnancy and childbirth, 19(1), 535. Visit Source.
Bjorklund, J., Wiberg-Itzel, E., & Wallstrom, T. (2022). Is there an increased risk of cesarean section in obese women after induction of labor? A retrospective cohort study. PLoS ONE, 17(2). Visit Source.
Burke, C., & Allen, R. (2020). Complications of cesarean birth: Clinical recommendations for prevention and management. MCN. The American Journal of Maternal/Child Nursing, 45(2), 92–99. Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024). Births: Method of delivery. Centers for Disease Control and Prevention (CDC) National Center for Health Statistics. Visit Source.
Erritty, M., Hale, J., Thomas, J., Thompson, A., Wright, R., Low, A., Carr, M., George, R., Williams, L., Dumitrescu, A., Rees, J., Irukulla, S., Fry, C. H., Fluck, D., & Han, T. S. (2023). Reduction of adverse outcomes from cesarean section by surgical-site infection prevention care bundles in maternity. International Journal of Gynecology & Obstetrics, 161(3), 963-968. Visit Source.
Kauffmann, T., & Silberman, M. (2023). Fetal monitoring. In StatPearls. StatPearls Publishing. Visit Source.
Larsson, C., Djuvfelt, E., Lindam, A., Tunón, K., & Nordin, P. (2021). Surgical complications after caesarean section: A population-based cohort study. PloS One, 16(10), e0258222. Visit Source.
Mayo Clinic. (2022a). Gestational diabetes. Mayo Clinic. Visit Source.
Mayo Clinic. (2022b). Placenta accreta. Mayo Clinic. Visit Source.
Mayo Clinic. (2022c). Placenta previa. Mayo Clinic. Visit Source.
MedlinePlus. (2022). C-section-Procedure, Part 3. MedlinePlus.gov. Visit Source.
Njogu, P. K., Makunyi, E. G., & Musau, J. (2022). Risk factors for caesarean delivery and fetal macrosomia among women with gestational diabetes in Nyeri County, Kenya: A cross-section study. The Pan African Medical Journal, 41. Visit Source.
Rathbun, K. M., & Hildebrand, J. P. (2022). Placenta abnormalities. In StatPearls. StatPearls Publishing. Visit Source.
Ring, L., Landau, R., & Delgado, C. (2021). The current role of general anesthesia for cesarean delivery. Current Anesthesiology Reports, 11(1), 18–27. Visit Source.
Rydahl, E., Declercq, E., Juhl, M., & Maimburg, R. D. (2019). Cesarean section on a rise—Does advanced maternal age explain the increase? A population register-based study. PLoS ONE, 14(1). Visit Source.
Sung, S., & Mahdy, H. (2023). Cesarean section. In StatPearls. StatPearls Publishing. Visit Source.
Wormer, K. C., Jamil, R. T., & Bryant, S. B. (2023). Acute postpartum hemorrhage. In StatPearls. StatPearls Publishing. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.