This course will be updated or discontinued on or before Sunday, August 30, 2026
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will understand what obstetric complications are possible and how to treat them.
Objectives
After completing this continuing education course, the participant will be able to:
Identify the potential obstetric complications.
Distinguish between the different types of intrapartum complications.
Determine the risk factors for complications.
Describe the necessary care of the woman experiencing complications.
Explain how to prevent obstetric complications.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Although pregnancy, labor, and delivery are normal physiological processes, many complications can arise. These complications can occur in the antepartum, intrapartum, and postpartum periods. Many of these complications are high-risk and low volume, meaning that they can be devastating, but do not occur often. Some of the most common complications will be discussed below.
Obstetric infections may require intensive care unit (ICU) admission, especially when the infection amounts to severe sepsis or septic shock. These infections are a significant cause of maternal morbidity and mortality (Reardon & Chen, 2023). These infections can also cause complications in the neonate, such as neonatal pneumonia, sepsis, meningitis, or even death (American College of Obstetricians and Gynecologists [ACOG], 2017).
There are different types and causes of infection. Antenatal infections occur before delivery and can include (ACOG, 2017):
Intra-amniotic infection (chorioamnionitis)
Pyelonephritis
Cases of pneumonia caused by streptococcus pneumonia and influenza
Chorioamnionitis is an infection that can occur during labor and can affect the amniotic fluid, placenta, fetal, fetal membranes, and decidua. This type of infection can cause dysfunctional labor and put the woman at risk for postpartum uterine atony and hemorrhage (ACOG, 2017).
Postpartum infection can also occur. The most common postpartum infection is endometritis or mastitis. Other postpartum infections can include (Berens, 2023):
Surgical site infections
Necrotizing fasciitis
Septic pelvic thrombophlebitis
Urinary tract infection (UTI)
Clostridium difficile colitis
Urinary tract infections (UTIs) can occur with foley catheter use during labor. Therefore, foley catheter use should be limited as much as possible.
The management of infection and sepsis should be similar to that of the non-pregnant patient and use the same targets and treatment, including antibiotics and fluid management.
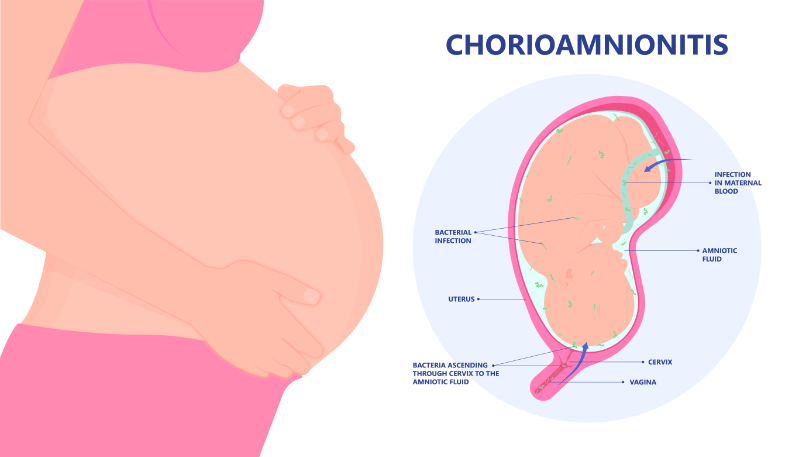
Chorioamnionitis is the most common of all infections, usually occurs during labor, and should be treated. Clinical chorioamnionitis is characterized by acute inflammation of the membranes and chorion of the placenta, generally due to a bacterial infection in women whose membranes have ruptured. It is common and may be associated with potentially serious adverse maternal and neonatal effects (ACOG, 2017). Preterm birth and dysfunctional labor, as well as sepsis and postpartum infection are all complications that can occur (Tita, 2023).
Image 1: Chorioamnionitis
Risk factors for chorioamnionitis can include (Tita, 2023; Arnold & Gawrys, 2020):
Longer duration of labor
Longer length of time of ruptured membranes
Multiple vaginal examinations (especially with ruptured membranes)
Cervical insufficiency
Nulliparity
Meconium-stained amniotic fluid
Internal fetal or uterine contraction monitoring
Presence of genital tract pathogens (group B Streptococcus, bacterial vaginosis)
The American College of Obstetrics and Gynecology (ACOG) suggests that patients with isolated fever ≥39.0°C (102.2°F) without another clear source of infection should be managed as having suspected chorioamnionitis. Treatment includes both antibiotic therapy and delivery (Tita, 2023).
The fetus of a mother with chorioamnionitis may experience tachycardia and they are at risk for early-onset sepsis, as well as asphyxia, respiratory distress syndrome (RDS), pneumonia, meningitis, intraventricular hemorrhage (IVH), necrotizing enterocolitis (NEC), and bronchopulmonary dysplasia (BPD). The ways to possibly reduce the risk of infection are to administer antibiotics for preterm premature rupture of membranes (PPROM), use a speculum instead of a hand for vaginal exams with PPROM, minimize vaginal exams in all patients, and administer antibiotics for all GBS+ patients (Tita, 2023).
Acute fatty liver of pregnancy (AFLP) is an obstetric emergency. AFLP occurs in the third trimester of pregnancy. In AFLP, free fatty acids increase in later pregnancy and if there is any defect in maternal-fetal acid metabolism, the products of metabolism can accumulate and affect maternal hepatocytes (Lee, 2023). Patients experiencing acute fatty liver may see their provider or go to the hospital with (Lee, 2023):
Nausea
Vomiting
Right upper quadrant pain
Jaundice
Increased serum aminotransferase levels
Treatment of AFLP is delivery of the fetus and supportive measures such as mechanical ventilation for coma, dialysis for renal failure, and blood products for coagulopathy. This rare but serious complication requires hospitalization and prompt delivery (Lee, 2023).
Liver disease may occur in women with preeclampsia or eclampsia. Liver disease associated with preeclampsia or eclampsia includes HELLP syndrome, liver hematoma, and liver failure (Lee, 2023). HELLP syndrome is a group of symptoms that includes (Reardon & Chen, 2023):
Hemolysis of red blood cells
Elevated Liver enzymes
Low Platelets
Patients may not exhibit any signs, other than abnormal lab tests, or they may have right upper quadrant pain, an enlarged liver, nausea or vomiting, or rarely, jaundice (Sharma & John, 2023). The only treatment for these preeclampsia-related liver diseases is supportive care and delivery of the fetus. It is important to assess for non-pregnant related causes of liver disease including hepatitis, gallstone disease, or drug-induced liver injury (Lee, 2023).
Viral hepatitis may occur during pregnancy and can lead to liver failure. Hepatitis A, B, or C can affect a pregnant patient. Hepatitis C is rarely transmitted to the fetus, but pregnant women with hepatitis B should be treated with antivirals to prevent transmission to the fetus (Sharma & John, 2023). Herpes simplex virus (HSV) can cause severe hepatitis. There is usually no jaundice, but herpetic lesions may be observed on the skin (Sharma & John, 2023). The diagnosis of HSV hepatitis may be treated with antiviral medication (Sharma & John, 2023).
Intrahepatic cholestasis of pregnancy (ICP) is a reversible disease that usually occurs in the third trimester of pregnancy. The exact cause is unknown, and it is diagnosed through exclusion. The most common findings are abnormal liver function tests (LFTs) and itching. Total and fasting serum bile acid concentrations are elevated. Treatment usually includes ursodeoxycholic acid (10 to 20 mg/kg/day), which can improve itching and fetal outcomes. ICP usually resolves 4 to 6 weeks after delivery (Sharma & John, 2023).
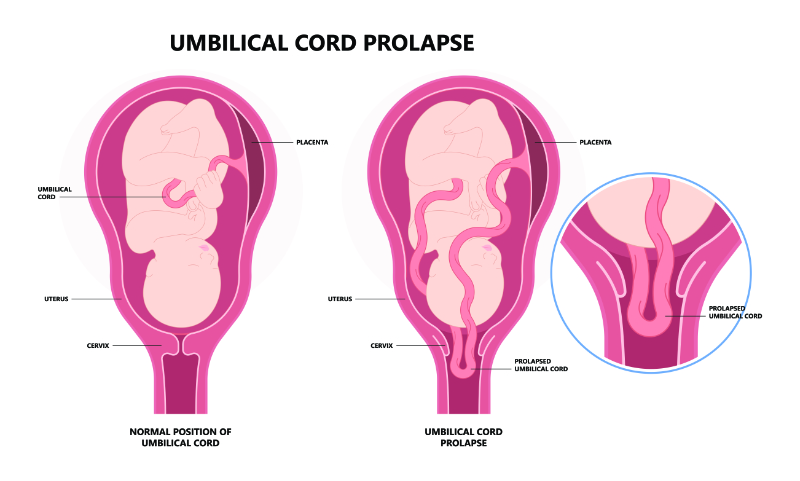
With an umbilical cord prolapse, the cord presents ahead of the presenting part of the fetus into the cervical canal or vagina.
Image 2: Umbilical Cord Prolapse
Umbilical cord prolapse is an obstetric emergency because the prolapsed cord can be compressed, leading to umbilical vein occlusion and umbilical artery vasospasm, which can compromise fetal oxygenation. Membranes are usually ruptured before this occurs.
Cord prolapse is rare, and the cause is not always known. However, some factors that increase the risk can include (Bush, 2023):
Malpresentation (breech, transverse, oblique, or unstable lie)
Multiparity
Prematurity
Polyhydramnios
Prolonged labor
Low birth weight
Low-lying placenta
Uterine malformations/tumors
Pelvic deformities
Fetal anomalies
Long umbilical cord
Unengaged presenting part of fetus
Atypical placental cord insertions
With a cord prolapse, the nurse may observe an abrupt, severe, prolonged fetal bradycardia or moderate to severe variable fetal heart rate decelerations. This complication usually occurs after amniotic membranes rupture or an obstetric intervention that moves the presenting fetal part from the birth canal, allowing the umbilical cord to come out before the fetus (Bush, 2023). The provider or nurse also may palpate a pulsating cord while performing a vaginal examination, done to assess labor progress, or a patient with ruptured membranes may report seeing or feeling something within the vagina.
Obstetric interventions are reported in 50% of cases of cord prolapse (Bush, 2023). Possible obstetric interventions can include (Bush, 2023; Arnold & Gawrys, 2020):
Cervical ripening with a balloon catheter
Rupture of membranes (more common with unengaged presenting part)
Induction of labor
Insertion of intrauterine pressure catheter (IUPC) or fetal scalp electrode
Manual rotation of head
Amnioinfusion (replacing amniotic fluid lost during labor)
Version (process to rotate fetus)
Assisted birth with forceps or vacuum
Obstetric management of a cord prolapse requires prompt delivery to avoid fetal compromise or death from compression of the cord between the presenting fetal part and the birth canal (Bush, 2023).
When a cord prolapse is detected, the nurse or provider should call for assistance and prepare for an emergency delivery. The nurse or provider should initiate maneuvers for intrauterine resuscitation, primarily aimed at moving the fetus off the umbilical cord to prevent compression. Intrauterine resuscitation may include maneuvers such as manual elevation of the presenting part by keeping a hand in the vagina pushing up on the head to prevent cord compression or retro-filling the bladder. It may be beneficial to place the patient in Trendelenburg or knee-chest position and administer a tocolytic because these interventions may reduce pressure on the cord (Bush, 2023). The fetal heart rate should be continuously monitored to determine whether resuscitative interventions are effective, which can impact the urgency of the delivery (Bush, 2023). The nurse or provider should also minimize manipulating a prolapsed cord and avoid exposing it to a cold environment. The nurse or provider should gently replace a prolapsed cord in the vagina and keep it moist with wet gauze. The provider should then perform an emergency delivery by the most rapid and safe route, typically a cesarean section (Bush, 2023).
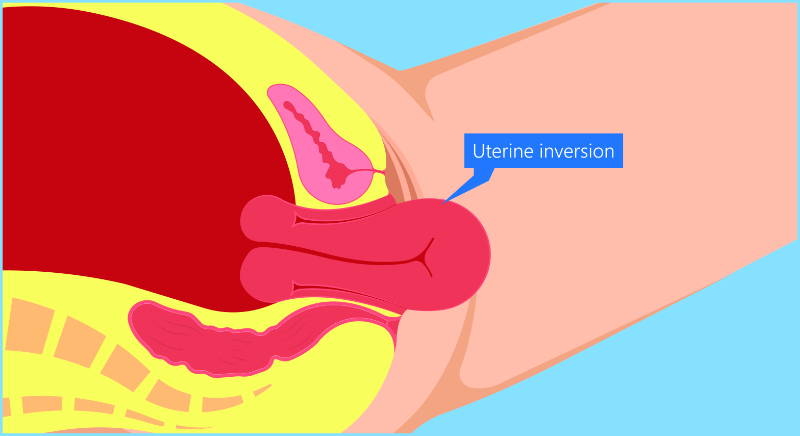
Uterine inversion occurs when the top of the uterus, called the fundus, falls into the endometrial cavity, turning the uterus partially or completely inside out.
Image 3: Uterine Inversion
It is a rare complication of vaginal or cesarean delivery, but when it occurs, it can be a life-threatening obstetric emergency (Macones, 2023). If a uterine inversion is not promptly recognized and treated, it can lead to severe hemorrhage and shock, which can result in maternal death (Macones, 2023).
There are 3 types of uterine inversion (Macones, 2023):
Acute occurs within 24 hours of delivery
Subacute occurs more than 24 hours but less than four weeks postpartum
Chronic occurs ≥ 1 month postpartum
Over 80% of cases of uterine inversion are acute (Macones, 2023).
The reason for uterine inversion is unknown, but excessive cord traction and fundal pressure during the third stage of labor, especially in an atonic uterus with fundal implantation of the placenta, may increase the risk of uterine inversion. A vaginal exam revealing "something" in the vagina and severe hemorrhage are the most common findings that suggest an inversion (Macones, 2023).
Treating uterine inversion means replacing the uterus, treating hemorrhage, and preventing reoccurrence. Uterotonic medications should be discontinued because the uterus needs to relax to be put back in. An emergency call for assistance, including anesthesia, is important. A second intravenous access, blood products, and fluids are needed to treat the hemorrhage. The provider should try to replace the uterus manually. Nitroglycerin is a good uterine relaxant with a short half-life, which is useful in women with severe hemorrhage and hemodynamic instability. Terbutaline or magnesium sulfate are other options for uterine relaxation. Surgical intervention is the last option. Once the uterus is replaced, the provider can hold it in place until the uterus is firm and stays in place. Uterotonic medications must then be given to treat the uterine atony. These medications can include (Macones, 2023):
Uterine rupture is a life-threatening complication of pregnancy for both mother and fetus. Most uterine ruptures in developed countries are associated with a trial of labor after cesarean delivery (TOLAC), although the risk is very low (Frey & Landon, 2023). The women with the highest risk are those with previous uterine rupture or previous fundal or high vertical hysterotomy (ACOG, 2019).
Induction of labor increases the risk of uterine rupture over spontaneous labor, with misoprostol causing the highest risk of rupture (ACOG, 2019; Frey & Landon, 2023).
Some of the risk factors for uterine rupture can include (ACOG, 2019; Frey & Landon, 2023):
Increasing maternal age
Gestational age >40 weeks
Birth weight >4000 grams
First pregnancy less than 18 to 24 months prior
More than one previous cesarean delivery
Previous second-trimester cesarean delivery
There is no reliable method to determine the risk of uterine rupture.
It is important to know the signs of uterine rupture. Signs may include a sudden abnormal fetal heart rate, which may include variable and prolonged decelerations, or bradycardia (Frey & Landon, 2023). Abdominal pain may be present but could be missed due to an epidural. Vaginal bleeding may occur. Loss of station of the fetal presenting part could occur if the fetus is partially extruding through the rupture (Frey & Landon, 2023). Hematuria may occur if the rupture extends into the bladder. Changes in contraction pattern could also be associated with uterine rupture. Unstable patients should be stabilized with fluids and blood transfusion, as appropriate, and prepared for cesarean delivery immediately. Anesthesia and neonatology should be notified urgently. The rupture may require a hysterectomy, although repair might be possible (Frey & Landon, 2023).
A 37-year-old patient, Darcy, was admitted for early labor. Darcy had had a previous cesarean section for the arrest of labor, about 15 months ago.
Darcy went into spontaneous labor. She progressed to full dilation.
An hour later, once she had been pushing for 40 minutes, the fetal monitoring tracing changes suddenly and records prolonged atypical variable decelerations (see Image 4).
Image 4: Prolonged Atypical Variable Decelerations of Fetal Heart Rate
It was decided that an emergency cesarean section was required for Darcy as instrumental delivery was not considered appropriate. During surgery, uterine rupture was noted.
Let’s consider a few questions:
What was the first sign that there could be uterine rupture?
The fetal heart tracing after the patient begins pushing becomes abruptly abnormal, indicating a possible uterine rupture.
Should Darcy have been managed differently?
No, appropriate care was given. She was a candidate for a trial of labor after cesarean and a cesarean was decided upon as soon as the fetal heart tracing indicated a problem.
If Darcy was pushing, what other sign may have been seen?
A patient who is fully dilated and pushing may have a loss of presenting part when uterine rupture occurs. If the head was at 0 station and all of a sudden is floating, this should signal a possible rupture.
Although obstetric complications occur infrequently, they can be life-threatening to the mother and the fetus. It is very important that labor and delivery (L&D) nurses are aware of all of the complications that can occur. Treatment depends on the condition but is often urgent.
Nurses should also be aware of all of the risk factors that increase a patient’s chance of having a complication. It is important to remember that the conditions can be scary and cause trauma to the patient and families that are involved. It is important that culturally sensitive and compassionate care is offered at all times. Nurses can check-in often with the patient to see how they are coping. Communication, in a calm manner, is important and should include the support person whenever possible (Vogel & Coffin, 2021).
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
American College of Obstetricians and Gynecologists. (ACOG). (2017). Committee Opinion No. 712: Intrapartum management of intraamniotic infection. Obstetrics & Gynecology, 130(2), e95-e101. Visit Source.
American College of Obstetricians and Gynecologists. (ACOG). (2019). Vaginal birth after cesarean delivery. American College of Obstetricians and Gynecologists (ACOG). Visit Source.
Arnold, J., & Gawrys, B. (2020). Intrapartum fetal monitoring. American Family Physician, 102(3), 158-167. Visit Source.
Berens, P. (2023). Overview of the postpartum period: Disorders and complications. UpToDate. Retrieved September 25, 2023. Visit Source.
Bush, M. (2023). Umbilical cord prolapse. UpToDate. Retrieved September 25, 2023. Visit Source.
Frey, H. & Landon, M. (2023). Uterine rupture: After previous cesarean delivery. UpToDate. Retrieved September 25, 2023. Visit Source.
Lee, R. (2023). Acute fatty liver of pregnancy. UpToDate. Retrieved September 25, 2023. Visit Source.
Macones, G. (2023). Puerperal uterine inversion. UpToDate. Retrieved September 25, 2023. Visit Source.
Reardon, C. & Chen, F. (2023). Critical illness during pregnancy and the peripartum period. UpToDate. Retrieved September 25, 2023. Visit Source.
Sharma, A., & John, S. (2023). Liver disease in pregnancy. StatPearls. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.