This course will be updated or discontinued on or before Saturday, October 16, 2027
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
CEUFast, Inc. is an AOTA Provider of professional development, Course approval ID#11256. This distant learning-independent format is offered at 0.15 CEUs Intermediate, Categories: OT Service Delivery, Foundational Knowledge.
AOTA does not endorse specific course content, products, or clinical procedures. AOTA provider number 9757.
FPTA Approval: CE25-687795, CE26-687795. Accreditation of this course does not necessarily imply the FPTA supports the views of the presenter or the sponsors.
CEUFast, Inc. is recognized by the New York State Education Department's State Board for Physical Therapy as an approved provider of physical therapy and physical therapist assistant continuing education.
Outcomes
≥ 92% of participants will know how to care for a postpartum patient.
Objectives
After completing this continuing education course, the participant will be able to:
Define the postpartum period.
Describe the physiologic changes that occur in the postpartum period.
Explain the essential postpartum assessments.
Identify the needs of a postpartum patient.
Determine the complications that may occur in the postpartum patient.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
The postpartum period begins at the time of delivery of the infant and ends approximately 6 to 8 weeks after that time, once most of the woman's body systems have returned to their pre-pregnancy state. The American College of Obstetricians and Gynecologists (ACOG) believes that postpartum care should extend up to 12 weeks after birth (Berens, 2024). ACOG refers to this period of time as the fourth trimester of pregnancy (Berens, 2024).
The first change that occurs after delivery is uterine involution. After the placenta is delivered, the uterus returns to a non-pregnant shape and condition. The uterus contracts, and the vessels at the placental site thrombose. Breastfeeding can help to cause the uterus to contract. These contractions can be felt for days after delivery (Mayo Clinic Staff, 2023; Mayo Clinic Staff, 2022). These steps help to prevent postpartum hemorrhage (Berens, 2024). The fundus (top) of the uterus can be located around the area of the umbilicus after delivery. Within 2 weeks, the fundus cannot be palpated, and it is back to its prepregnant size by 6 to 8 weeks after delivery. This process may cause pain or discomfort for the new mom (Berens, 2024).
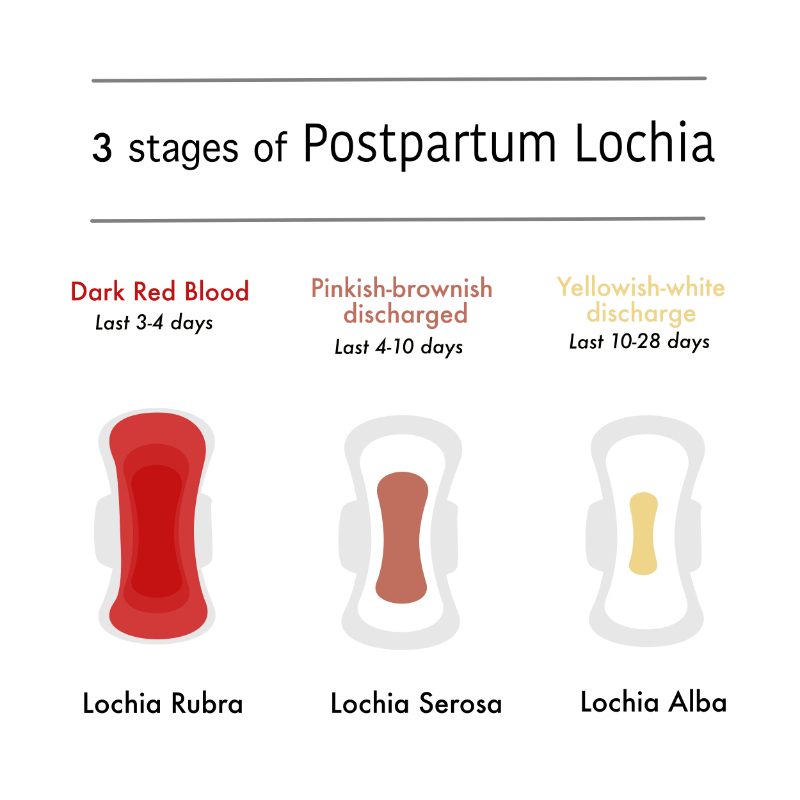
Bleeding will occur after delivery. This blood is called lochia. Lochia rubra is bright red to red-brown and can occur up to a few days after delivery, when it then turns to lochia serosa (pinkish-brown and thinner) (Berens, 2024). After about 2 to 3 weeks, lochia turns to lochia alba, which is white or yellow in color, which can last up to 6 weeks (Berens, 2024).
Image 1: Lochia Description
Reproductive hormones will gradually return to normal. Return of menstruation typically ranges from 45 to 64 days postpartum (Berens, 2024). The average time for the return of ovulation ranges from 45 to 94 days but it can occur as early as 25 days postpartum, meaning that the woman can get pregnant at this time (Berens, 2024). Approximately 40% of exclusively breastfeeding women will remain amenorrhoeic at six months postpartum (Berens, 2024).
Breast changes occur in the postpartum period. Lactation will begin. Women may have breast tenderness. Women who are not breastfeeding should be taught to wear a tight bra and avoid breast stimulation (Mayo Clinic Staff, 2022). Women who are breastfeeding, especially first-time mothers, will need breastfeeding support to get the baby to latch and feed appropriately and successfully.
There are also changes to the woman's heart. Cardiac output and stroke volume increase after delivery but will gradually decrease in cardiac output from 7.42 L/min at 38 weeks of gestation to roughly 4.96 L/min at 24 weeks after birth (Berens, 2024). As early as only two weeks postpartum, reductions in left ventricular size and contractibility already take place, adjusting from the full-term pregnant state to a postpartum state (Berens, 2024). Postpartum hypertension can also occur after giving birth (Berens, 2024).
The woman's hematologic state returns to baseline 6 to 12 weeks after delivery, but because the prothrombotic state from pregnancy takes weeks to normalize, she remains at risk for thromboembolic events for a few weeks after delivery (Berens, 2024).
Weight loss is normal and may increase with breastfeeding (Sissons, 2023). Hair loss and changes in the skin may result too as hormones continue to change.
Once a woman delivers, she should have her blood pressure (BP) and pulse monitored every 15 minutes for 2 hours, and her temperature monitored every 4 hours for the first 8 hours. All vital signs should then be monitored at least every 8 hours while the woman is in the hospital (American Academy of Pediatrics [AAP] & American College of Obstetricians and Gynecologists [ACOG], 2017).
In addition to vitals, the nurse should also assess her fundus to check for uterine tone and placement. A fundus that is not midline or is rising could indicate a full bladder or other complications. Uterine atony is the leading cause of postpartum hemorrhage.
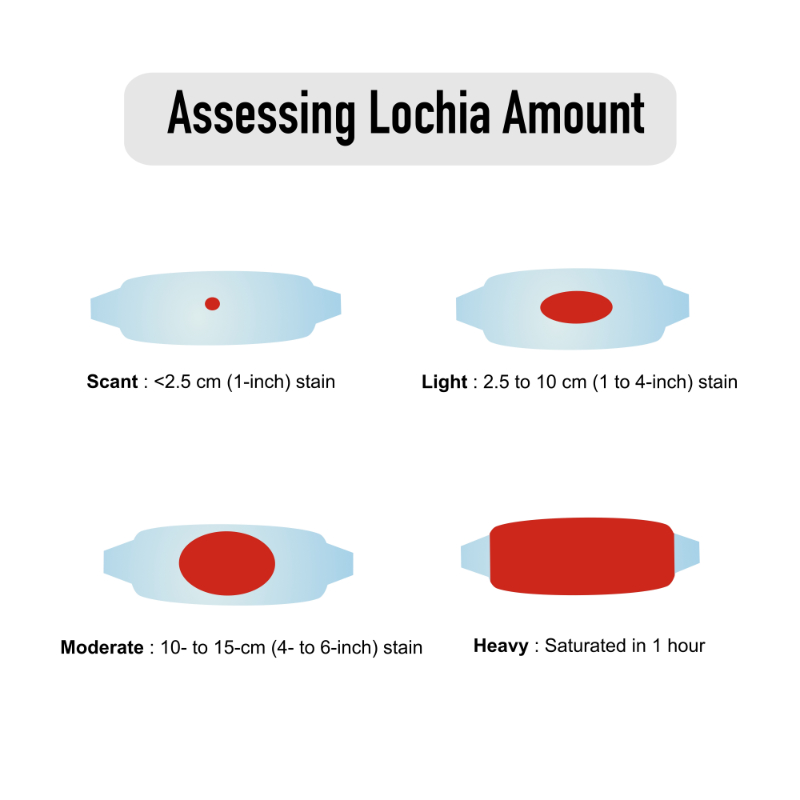
The nurse should also monitor and assess her lochia, for both color and volume. The lochia may be moderate right after delivery but should decrease over time. Any significantly increased or large amount of bleeding (soaking a pad in an hour) should be reported to the provider (Lopez-Gonzalez & Kopparapu, 2022).
Image 2: Lochia Amount
Postpartum women will likely have their hemoglobin and hematocrit levels checked the day after delivery. The woman should always be assessed for signs of anemia that can include(Berens, 2024):
Dizziness
Pale color
Lightheadedness
Low blood pressure
Elevated heart rate
If the woman had a laceration or episiotomy, it needs to be fully assessed to look for signs of infection. Women should be assessed for any signs of infection in the perineum, episiotomy or laceration site, or abdominal incision site (AAP & ACOG, 2017). Signs of possible infection could include (AAP & ACOG, 2017):
Pain
Redness
Swelling
Tenderness
Discharge
Fever
The woman will need to have her perineum inspected to look for signs of a hematoma. A hematoma is a blood collection under the skin that can be painful. A large amount of blood can be collected in a hematoma, so a provider must be notified immediately (AAP & ACOG, 2017).
Women in the postpartum period also need their bladder assessed to ensure they are frequently voiding and without difficulty. The woman’s bladder should be assessed to ensure that she is emptying it regularly. If there is any concern for bladder emptying, a bladder scan may be done. Women should be encouraged to void regularly. Leaking of urine could occur after delivery and should resolve within a week (Mayo Clinic Staff, 2023). Bowel movements may be irregular, especially after a cesarean section and with the use of some pain medications. Nurses should assess this and ask the provider for medications as needed to improve bowel function.
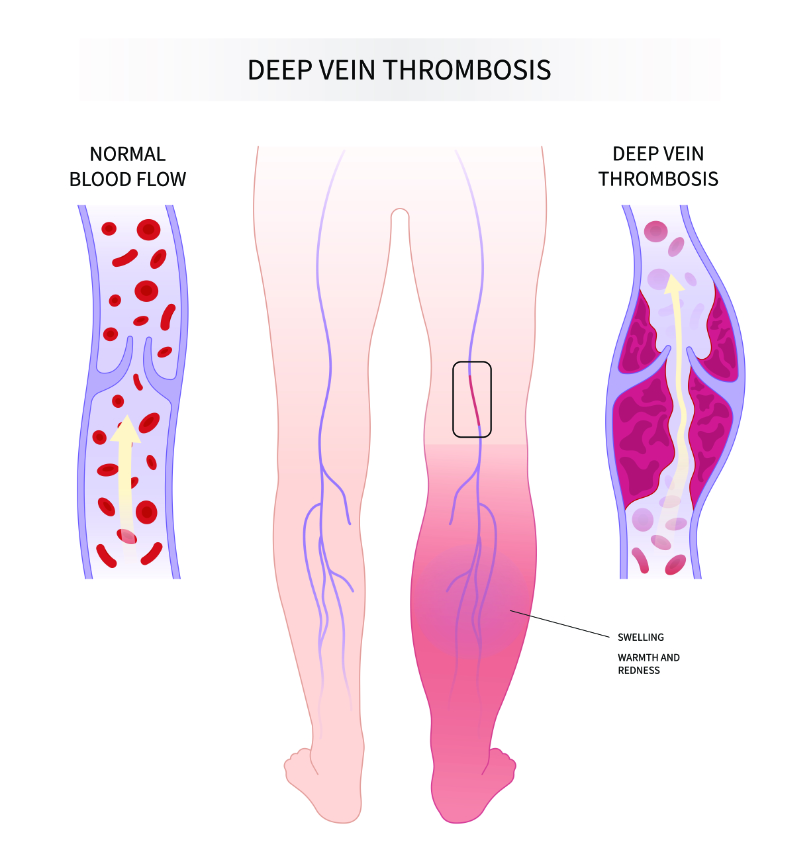
Venous thromboembolism (VTE) is more common in postpartum women, so these women should be assessed for VTE. Any signs or symptoms such as calf redness or tenderness should be reported to the provider (Berens, 2024). Women with thrombophilia, sickle cell disease, obesity, and cesarean delivery are at an increased risk of deep vein thrombosis (DVT), as are women who smoke or had a postpartum hemorrhage (Berens, 2024).
Image 3: Deep Vein Thrombosis
Women with any cardiac or hypertensive disorders will also need specialized monitoring, which could include cardiac monitoring if necessary. These women may need an increased frequency of vital signs as ordered by the provider. They may also need continuous pulse oximetry monitoring as ordered.
Perinatal mental health conditions are a big part and a major concern of the pregnancy and postpartum periods that need to be addressed. A nurse should regularly perform a general assessment to see how the mother is emotionally and how she is bonding with the baby. As many as 1 in 5 pregnant patients can experience these conditions during pregnancy or within 1 year postpartum (American College of Obstetricians and Gynecologists [ACOG], 2023). Screening should begin with the provider in the prenatal period and continue up to 6 months in the postpartum period (Hawkins, 2023). Screening should include assessing for signs and symptoms of depression and anxiety. Suicide and overdose associated with substance use disorder (SUD) make up almost a quarter of pregnancy-related deaths and are all preventable (ACOG, 2023). All women in the postpartum period should undergo depression screening while still in the hospital (ACOG, 2018b). The Edinburgh scale is the most commonly used tool, but any validated tool is acceptable. It is important to teach women about postpartum mood disorders and that this is not something they should be embarrassed about and must speak up about. Women should also receive resources that they can call if they need extra support.
The entire healthcare team can provide such excellent knowledge and support for postpartum mothers. Occupational therapists (OTs) are tasked with engaging patients in meaningful occupations and activities. These occupations include activities of daily living (ADLs), instrumental activities of daily living (IADLs), rest, health management, sleep, work, play, education, leisure, and social activity participation (American Occupational Therapy Association [AOTA], 2020). OTs also support individuals in transitioning to new roles and occupations and address their overall health and well-being. OTs can support postpartum women by addressing potential postpartum depression (PPD), supporting women’s occupation of breastfeeding, and addressing pelvic floor dysfunction (PFD). We will discuss all of these issues shortly.
The most important need for a healthy postpartum woman is education. Women and their partners have expressed their desire to learn competence in caring for their babies. Newborn care is the major education point, especially for first-time mothers. These new moms need reassurance that they can care for their babies. This education must include basic newborn care such as bathing and circumcision care to more complex education such as when to call the doctor. Education should also include safe sleep practices and shaken baby syndrome. There is much information, and it can be overwhelming. Giving resources for the woman to refer to at home may be useful (Mayo Clinic Staff, 2023).
It is also important to teach the mom about self-care. The woman should be taught to rest because sleep is difficult with a new baby. It is also important to teach the woman to walk to prevent VTE. The nurse must teach the patient about the signs and symptoms of complications that can occur in the postpartum period, even though the complications can be scary. The maternal morbidity and mortality rates are too high in the United States, in fact, they continue to exceed those of other high-income countries (Gunja et al., 2024). In the United States, in the year 2022 alone, there were about 22 maternal deaths for every 100,000 births (Gunja et al., 2024). Over 65% of maternal deaths occur within the first year after childbirth (Gunja et al., 2024). The most common causes of maternal mortality include (Gunja et al., 2024):
Severe bleeding
Cardiovascular conditions
Coronary conditions
Cardiomyopathy
Venous thromboembolism (VTE)
Hemorrhage
Infection
Mental health conditions
Preeclampsia and eclampsia
High blood pressure
ACOG looks at the "fourth trimester," which is the 12 weeks following delivery. During this time, a woman is tasked with recovery, adapting to changing hormones, and learning to feed and care for her newborn (Tully et al., 2017). During this fourth trimester, many women experience common challenges, often including pain, fatigue, depression, difficulties navigating breastfeeding, lack of sexual desire, and incontinence, and may consider this normal and, because of this, choose not to seek care (Tully et al., 2017). Women should not suffer during this time and should receive appropriate care. Because more than 65% of all maternal morbidity occurs after delivery, ACOG believes that women who gave birth should be monitored closely for those first 12 weeks (ACOG, 2018a).
Every woman who has given birth should be educated about signs and symptoms to look for that could indicate a potential complication. The woman should be told to get emergency help for (Mayo Clinic Staff, 2021):
Chest pain
Shortness of breath
Seizures
Thoughts of harming self or baby
The patient should be instructed to call their provider if they have (Mayo Clinic Staff, 2021):
Bleeding that soaks through a pad in an hour or blood the size of an egg or larger
An incision that is not healing
A temperature of 100.4°F or higher
A red or swollen leg that is warm and/or painful
A headache that does not get better after taking medication
Pain is another problem that postpartum women may experience that can interfere with the woman's ability to care for herself and her new baby. Pain can also increase the risk of postpartum depression and should be managed (ACOG, 2021). Women who have had a vaginal birth may experience uterine cramping, which can increase with each delivery and perineal pain, which can be severe with a laceration or episiotomy. These women may also have hemorrhoids. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually effective at treating cramp pain. Ice packs, topical sprays, and creams can help with perineal and hemorrhoidal pain. Women who have had a cesarean section will have abdominal pain. Multimodal pain management, including nonpharmacologic and pharmacologic therapies, is important. There is a variation in the types and level of pain women experience during the beginning of the postpartum period (ACOG, 2021). For postoperative cesarean pain, standard oral and parenteral analgesic medications, including acetaminophen, NSAIDs, and mild opioids, should be used first (ACOG, 2021). Stronger opioids should be reserved for use when the other medications do not relieve pain. It is also important to educate the woman that opioids can pass through breastmilk and sedate the baby. Acetaminophen, ibuprofen, and ketorolac are acceptable pain medications for breastfeeding infants. The length of prescribed opioids should be as short as possible for treating acute pain (ACOG, 2021).
Breastfeeding is an occupation that the Centers for Disease Control and Prevention (CDC) estimates that approximately 84% of mothers engage in after childbirth (CDC, 2024). While lactation support professionals including Certified Lactation Counselors (CLCs) and International Board-Certified Lactation Consultants (IBCLCs) are the ideal professionals to assist postpartum mothers and babies in their initial breastfeeding experiences, many nurses have the training to assist the postpartum mother and child dyad.
Providing breastfeeding guidance and support as a nurse means teaching postpartum mothers comfortable positions, how to assess for a proper latch, how to and how long to breastfeed for in a single session, what tools and supports can be used to improve baby’s position and milk intake, and what cues to watch her new infant for, that might indicate the child is hungry and wants to feed. Because every baby is different, even postpartum mothers who have breastfed a child before could benefit from the hands-on breastfeeding assistance at the bedside.
OTs can support breastfeeding mothers as well during this transitionary period and support the formation of new routines around this occupation. A lack of time, lack of awareness about available supports, and stress can all contribute to breastfeeding mothers not meeting their mothering and personal goals (Sponseller et al., 2021). OTs can support mothers in creating routines and habits that ease their transition to breastfeeding.
A pilot study with 14 mothers, explored if OT services, provided in an individual and group format, could successfully assist breastfeeding mothers at lactation centers to accomplish personal wellness goals while continuing to breastfeed their child (Sponseller et al., 2021). The study indicated that after OT interventions, mothers experienced an increased sense of competence and self-worth, improving their psychological well-being and confidence in addressing their needs and the needs of their infants and families (Sponseller et al., 2021). OTs can also support breastfeeding mothers by addressing their ergonomic concerns, including concerns related to the physical discomfort experienced by some women while breastfeeding (Barbic et al., 2021).
As mentioned above, the most common causes of maternal morbidity and mortality are cardiovascular and coronary conditions, cardiomyopathy, venous thromboembolism, hemorrhage, severe bleeding, infection, high blood pressure, mental health conditions, and preeclampsia and eclampsia (Gunja et al., 2024). These are important potential complication conditions to teach the postpartum woman about.
A woman with known cardiac conditions should follow up with her cardiologist immediately. The woman with preeclampsia and other hypertensive disorders needs to know the signs of any problems, such as elevated blood pressure, headache, blurred vision, or epigastric pain. Bleeding, that soaks more than one pad an hour, is too much, and the woman should call her provider. A woman also needs to know about the risk of VTE and the signs and symptoms to look for, such as swelling, redness, or pain in their calf (Mayo Clinic Staff, 2023).
Infection is also a complication possibility that should be discussed. Possible sources of infection include the bladder (urinary tract infection), especially if the woman had a foley catheter, the perineum, especially if the woman has an episiotomy or laceration, the breasts (mastitis), especially if breastfeeding, and the abdominal incision if the woman had a cesarean section (Mayo Clinic Staff, 2023). Women should be taught to report any redness, swelling, pain, or discharge at these sites, as well as difficulty or pain with urination (Mayo Clinic Staff, 2023).
Alana is a 39-year-old woman who just had her first baby at 35 weeks gestation. After 16 hours of labor, Alana had a cesarean section to deliver her twin sons. She is exhausted and tearful because one of her babies is in the Neonatal Intensive Care Unit (NICU) for difficulty breathing.
Alana tells you that she has not had much experience with babies and is worried about how she will care for these babies. Her medical history is negative, except for some mild anxiety that she says comes and goes over time. When you first speak to her about postpartum depression, she expresses that she could not possibly get postpartum depression because she has wanted and tried for a baby for many years and could not be happier.
Is Alana at risk for postpartum depression?
Alana is at risk for postpartum depression. Any woman is, but at her age, with twins, these being her first babies, an unplanned NICU stay, and her having a history of anxiety, all increase her risk of developing postpartum depression.
How can you educate Alana about postpartum depression?
It is important to teach Alana that postpartum depression does not mean she is unhappy with having her babies. It is a postpartum condition caused by changing hormones and sleep deprivation and it can happen to any woman. It does not signify that she is not a good mom. The nurse must give her resources for when she goes home if she develops postpartum depression. It may also be helpful to educate Alana when her partner is also present to hear the information.
As has been discussed earlier in this course, during the “fourth trimester”, a woman must navigate recovery and learn to feed and care for her newborn, all while adapting to their fluctuating hormones (Tully et al., 2017). This is such an exciting but equally stressful, even daunting time in a woman’s life. Just as a lack of quality sleep, inadequate diet, and deficiency of exercise can affect one’s mental health in “normal” conditions, the postpartum period can be especially impactful for these women.
Postpartum depression (PPD) can significantly impact the well-being and mental health of both women and their children. Mothers who experience PPD can have difficulties engaging in meaningful occupations and activities. This occupational disruption can impact their ability to care for themselves and their newborns. Nurses, as well as OTs, can support new mothers in finding resources, helping them adapt to changes, fostering self-care, perseverance, and flexibility during this vital role transition (Barbic et al., 2021).
A scoping article by Barbic et al., (2021) reviewed research on risk factors for PPD and interventions related to the scope of OT. The study found evidence to support the role of OT in assessment and treatment of PPD. OT assessments may be more sensitive to changes in functioning and occupational performance that occur as a result of having a child, a life-changing transition (Barbic et al., 2021). Results of the study showed OTs can provide interventions that address clients’ needs, including considering their cultural and societal environment and home needs. OTs can also support the emotional and cognitive transitions related to child-rearing (Barbic et al., 2021). This can occur through leading group therapy sessions that incorporate mindfulness and psychosocial support for mothers experiencing PPD (Barbic et al., 2021). OTs can also support engagement between mother and child, provide psychoeducation, and partner with mothers and families to understand their lived experiences and provide them with hope and encouragement, thereby improving healthy development and postpartum recovery (Barbic et al., 2021).
As early as 1946, the need for physical therapy (PT) in postpartum care was recognized. A program was initiated at Station Hospital located in Fort George Meade, Maryland, to provide obstetrical patients with beneficial postpartum exercises (Harvey, 1949). There is moderate evidence that postpartum women are at risk for pelvic floor, abdominal, hip, and back impairments following pregnancy and delivery (Simonds et al., 2022). Evidence shows that PT effectively treats these impairments; however, in the United States, physical therapists maintain a primarily peripheral role in providing postpartum care (Critchley, 2022). There is an increasingly supported recommendation to include physical therapy within 6-8 weeks following delivery as a standard of care.
It is estimated that by 2050, 43.8 million women are expected to experience pelvic floor symptomology (Dieter et al., 2015). While most pelvic floor dysfunction (PFD) spontaneously resolves within a few months following delivery, it is reported that 25% of American women suffer from pelvic floor disorders, with 20% requiring surgical intervention during their lifetime (DeLancey et al., 2024).
PFD is a public health issue impacting many women after giving birth. The female pelvic floor is made up of layers of muscles and connective tissues that support and aid the functions of the reproductive system, bladder, and rectum. During pregnancy, the pelvic floor is subjected to compressive and strenuous forces and must open and expand to give birth (Burkhart et al., 2021). The uterus enlarges to accommodate the growing infant, which increases pressure on the pelvic floor. Trauma to the pelvic floor can result in PFD and fecal incontinence (Burkhart et al., 2021). PFD can range from pelvic girdle pain and stress incontinence to prolapse and can pose distressing lifelong consequences, greatly affecting quality of life (DeLancey et al., 2024; Simonds et al., 2022).
One study that included 255 women in the United States aged 18 to 45 who had given birth to at least one child, aimed to explore the influence of PFD on women’s occupations and to examine how severely PFD impacted their lives (Burkhart et al., 2021). The study found that PFD symptoms limited women’s occupational performance and negatively impacted their perception of daily life (Burkhart et al., 2021). This study highlights the need for OTs to support women experiencing PFD. OTs use their skillset to provide musculoskeletal rehabilitation in addition to individualized treatment and education that addresses functional deficit areas (Baker et al., 2017). Specifically, OTs can address postnatal coping strategies, maternal attachment, and musculoskeletal dysfunction of PFD through manual therapy and even electrical stimulation (Podvey, 2018).
OTs can address pelvic floor rehabilitation and address lifestyle modifications (Jundt et al., 2015). The numerous symptoms associated with PFD can impact an individual’s ability to perform occupations related to (AOTA, 2020):
Self-care
Managing a home
Sexual activity
Work
Rest and sleep
Social participation
Leisure activities
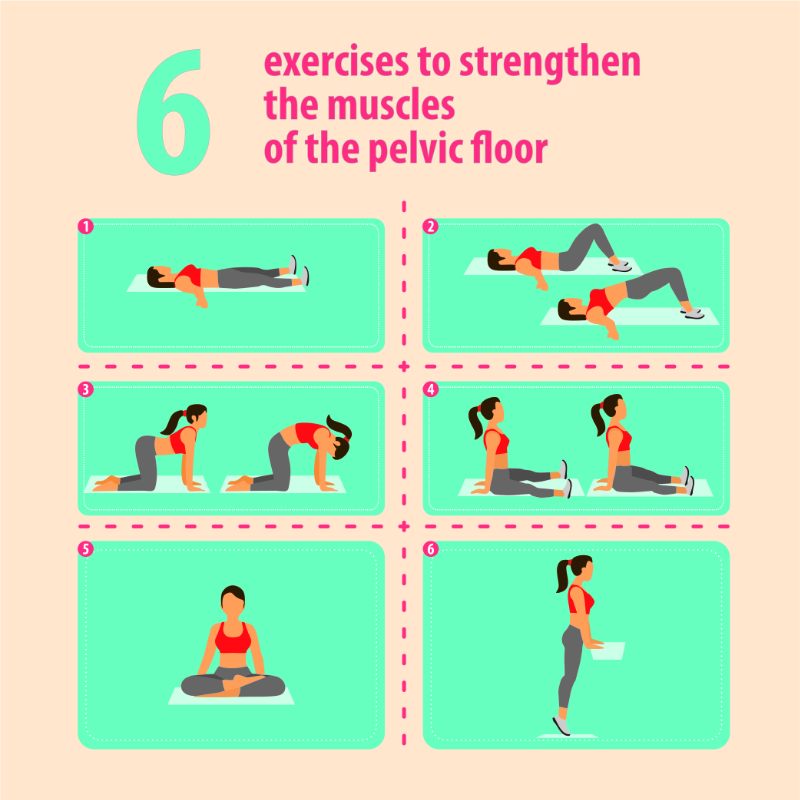
A PT examination for PFD may consist of internal and external evaluations to evaluate muscle tone, strength, coordination, and pain (Critchley, 2022). PT interventions for PFD are designed to strengthen, relax, and facilitate proper pelvic floor coordination (Critchley, 2022).
Image 4: Exercises to Strengthen the Muscles of the Pelvic Floor
Pelvic floor PT may also include manual PT, biofeedback techniques, and electrical stimulation. The 2019 Cochrane review demonstrated that women who received pelvic floor PT were 5 to 8 times more likely to eliminate urinary incontinence than women who received general education, motivational phone calls, lifestyle advice, or no interventions at all (Critchley, 2022). It is, however, important to see a PT who is trained specifically to treat PFD.
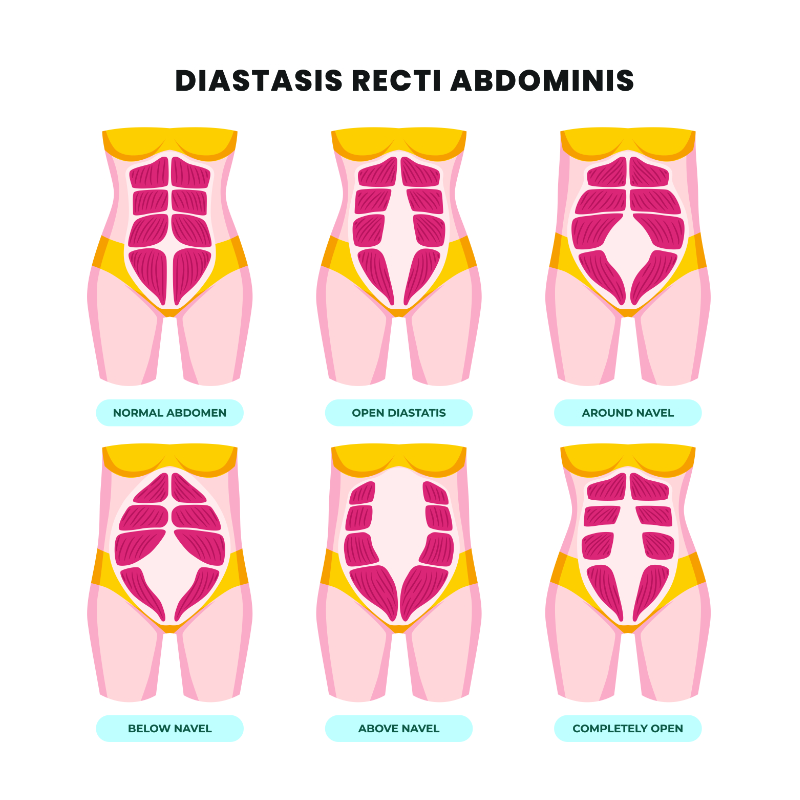
Diastasis recti abdominus (DRA) is a common consequence of pregnancy and childbirth, where the linea alba widens and the rectus muscles separate. DRA is reported to occur in 60% of people, with the separation naturally decreasing within eight weeks post-delivery (Cleveland Clinic, n.d.). Studies have found, however, that 45% of women exhibited DRA at six months postpartum and 33% at 12 months postpartum (Critchley, 2022). DRA often causes a bulging or “pooch” of the lower abdominal region and can lead to negative self-perception and body image, possibly leading to depression (Critchley, 2022).
Image 5: Diastasis Recti Abdominis
A PT examination is performed externally, often using finger palpation and measurements to determine the length, width, and depth of the separation. These measurements are also used to measure healing. DRA can lead to pelvic pain, increased back pain, umbilical hernia, painful sex, and urinary incontinence (Cleveland Clinic, n.d.). Through proper PT, it is possible to completely heal DRA without surgery.
PT approaches may involve bracing, strapping, movement and biomechanical education and specific, safe core strengthening exercises. It is important to consult a PT as many of the core exercises that first come to many women’s minds may actually make DRA worse. This includes many yoga or Pilates-based movements.
Low back pain is a common experience for many women following delivery. However, it is not uncommon for women to also experience pain in their thoracic spine, hips, and pubic symphysis. Pain in the sacroiliac joints, lumbosacral region, pubic symphysis, or any combination of these joints has been termed pelvic girdle pain(Fiani et al., 2021).
It has been estimated that almost half of all pregnant women experience pelvic girdle pain, with 8-10% continuing to have pain for one to two years postpartum (Fiani, et al., 2021). Many of the biomechanical and hormonal changes that occur during pregnancy lead to abdominal and hip weakness, tightness in the lumbar musculature, and joint instability.
PT assessment is important to develop an appropriate treatment plan to address the above impairments. Manual therapy including joint manipulation, stretching, dry needling, and core and hip stabilization exercises have all been proven to be effective in treating back and pelvic girdle pain in postpartum patients, with strong evidence of significantly higher improvements when manual therapy and stabilization exercises are used in conjunction as part of a treatment plan (Simonds et al., 2022).
Education on proper biomechanics following delivery is also a key PT intervention. Despite the weakness, back tightness, and pelvic instability that occurred following delivery, the postpartum woman is now lifting more than previously, carrying heavy baby carriers, bending over cribs, and changing tables more frequently. This can also lead to increased stress on the neck, thoracic spine, and shoulder girdle.
Women are often advised to return to exercise and activity as early as 6 weeks postpartum, despite significant physical and physiological changes that have occurred over the past nine to ten months (Schulz et al., 2023). Schulz et al. investigated 33 studies, with most stating that return to sport postpartum can begin once “medically safe” and around 6 weeks postpartum. Additionally, most recommended engaging in 150 minutes of moderate-vigorous physical activity per week after 6 weeks, but the type of exercise was non-specific (Schulz et al., 2023).
According to Schulz et al., it was reported that many general physicians do not feel they have the education and adequate training in postpartum exercise prescription (Schulz et al., 2023). As a result, many women are left to their own devices and aggressively go to aerobic gym classes, Pilates classes, or engage in running as a means to lose weight. Just as it is common to use PT in the post-operative or post-injury populations to return to higher-level activities, PTs can help optimize recovery and assist a postpartum woman in safely returning to sport.
PTs can help develop a graduated return-to-exercise plan for the postpartum patient that corresponds to a time- and criterion-based approach, similar to a return-to-running program following injury. A proposed outline for postnatal performance is described by Selman et al. (2022), which recommends beginning light exercises of postural work, initial safe core and pelvic floor exercises, and household walking at 0-2 weeks postpartum. Exercise guidelines and strengthening recommendations gradually increase on a weekly basis based on the ability of the patient, pain, and demonstration of appropriate healing.
According to Selman et al. (2022) it is recommended that endurance walking can gradually increase to 30 minutes between weeks 5-6 but should be kept below a jogging speed. High-impact activities have been shown to increase intraabdominal pressures and ground reaction forces as much as 1.6-2.5x body weight. Consequently, increased speed and eventual mileage are recommended between 12-13+ weeks post-delivery. Each phase of this recommended protocol should preferably be monitored by a PT who can best make determinations on a patient’s readiness to progress to the next phase and confirm that pelvic floor muscles are contracting and relaxing correctly (Selman et al., 2022).
Sarah, a 31-year-old athletic female, recently gave birth and is now eight months postpartum. A dedicated runner with a passion for competitive racing, Sarah is eager to return to her pre-pregnancy fitness level. However, she faces challenges such as urinary incontinence, rectus diastasis, and low back pain, which have emerged postpartum. These issues hinder her training progress and performance goals.
Sarah presents to a PT with complaints of urinary incontinence during high-impact activities, such as running, as well as visible separation of the rectus abdominis muscles (rectus diastasis). Additionally, she experiences low back pain when her running mileage and pace increase. Despite her athleticism and determination, these symptoms significantly impede her ability to resume competitive running.
Upon assessment, Sarah demonstrates a mild to moderate separation of the rectus abdominis muscles, measuring approximately 2.5 cm in width at the umbilicus. Pelvic floor muscle weakness is evident, contributing to her urinary incontinence during running. Sarah also exhibits lumbar spine hypermobility and weakness in the deep core stabilizers, particularly the transverse abdominis and multifidus muscles. Her pelvic alignment shows anterior pelvic tilt, exacerbating the strain on her lumbar spine during running.
A multidimensional approach is adopted to address Sarah's concerns and facilitate her return to competitive running:
Pelvic Floor Rehabilitation: Sarah undergoes pelvic floor muscle training focusing on strength, endurance, and coordination. This includes exercises such as Kegels, pelvic tilts, and functional movements to enhance pelvic floor control during running.
Core Strengthening: Emphasis is placed on activating and strengthening the deep core stabilizers, particularly the transverse abdominis and multifidus muscles. Progression includes exercises like dead bugs, bird dogs, and plank variations to stabilize the lumbar spine and pelvis during dynamic movements.
Manual Therapy: Soft tissue mobilization and myofascial release techniques are employed to address muscle tightness and fascial restrictions contributing to Sarah's low back pain and pelvic malalignment.
Postural Education: Sarah receives education on proper posture and body mechanics during running to reduce stress on her lumbar spine and optimize running efficiency.
Progressive Return to Running: A gradual return-to-run program is developed, focusing on increasing mileage and pace incrementally while monitoring symptoms and pelvic floor function closely.
Over the course of several weeks, Sarah demonstrates significant improvements in her symptoms and functional abilities:
Urinary incontinence during running decreases, indicating improved pelvic floor muscle function and control.
Rectus diastasis narrows, and abdominal wall strength improves, enhancing core stability and support.
Low back pain diminishes as core strength and lumbar spine stability improve, allowing Sarah to tolerate increased running intensity and duration.
Sarah successfully completes her return-to-run program and resumes competitive racing, achieving her pre-pregnancy fitness level with confidence and without debilitating symptoms.
This case highlights the importance of comprehensive postpartum rehabilitation in addressing pelvic floor dysfunction, abdominal wall separation, and musculoskeletal issues in athletic females aiming to return to competitive sports. Through targeted PT interventions, Sarah not only resolves her urinary incontinence, rectus diastasis, and low back pain but also restores her athletic performance and achieves her running goals.
Childbirth is a natural process. However, women having babies are getting older and have more co-morbidities than in the past. Nurses must know how to care for each of these women in the acute postpartum period and be able to teach them to care for themselves and report any problems immediately. OTs and PTs can be extremely valuable resources to assess and assist the postpartum woman in her healing journey as well.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
American Academy of Pediatrics (AAP) & American College of Obstetricians and Gynecologists (ACOG). (2017). Postpartum care of the mother. In: Guidelines for perinatal care. (8th Ed). American Academy of Pediatrics (AAP) Publications. 284-285. View Source.
American College of Obstetricians and Gynecologists. (ACOG). (2023). Screening and diagnosis of mental health conditions during pregnancy and postpartum: ACOG clinical practice guideline No. 4. (2023). Obstetrics and Gynecology, 141(6), 1232–1261. View Source.
American College of Obstetricians and Gynecologists. (ACOG). (2021). Pharmacologic stepwise multimodal approach for postpartum pain management: ACOG Clinical Consensus No. 1. (2021). Obstetrics and Gynecology, 138(3), 507–517. View Source.
American College of Obstetricians and Gynecologists. (ACOG). (2018a). Committee Opinion No. 736: Optimizing postpartum care. Obstetrics and Gynecology, 131(5), e140–e150. View Source.
American College of Obstetricians and Gynecologists. (ACOG). (2018b). ACOG Committee Opinion No. 757: Screening for perinatal depression. Obstetrics and Gynecology, 132(5), e208–e212. View Source.
American Occupational Therapy Association. (AOTA). (2020). Occupational therapy practice framework: Domain and process. (4th Ed.). American Journal of Occupational Therapy, 74(Suppl. 2), 7412410010. View Source.
Baker, A., Boetel, W., Powell, K., & Washburn, T. (2017). Certification in pelvic floor rehabilitation: A guide for occupational therapists. View Source.
Barbic, S. P., MacKirdy, K., Weiss, R., Barrie, A., Kitchin, V., & Lepin, S. (2021). Scoping review of the role of occupational therapy in the treatment of women with postpartum depression. Annals of International Occupational Therapy, 4(4), e249-e259. View Source.
Berens, P. (2024). Overview of the postpartum period: Normal physiology and routine maternal care. UpToDate. Retrieved January 31st, 2024. View Source.
Burkhart, R., Couchman, K., Crowell, K., Jeffries, S., Monvillers, S., & Vilensky, J. (2021). Pelvic floor dysfunction after childbirth: Occupational impact and awareness of available treatment. Occupational Therapy Journal of Research: OTJR, 41(2), 108-115. View Source.
Centers for Disease Control and Prevention. (CDC). (2024). Breastfeeding. Centers for Disease Control and Prevention (CDC). View Source.
Critchley, C. J. C. (2022). Physical therapy is an important component of postpartum care in the fourth trimester. Physical Therapy & Rehabilitation Journal, 102(5), pzac021. View Source.
DeLancey, J. O., Masteling, M., Pipitone, F., LaCross, J., Mastrovito, S., & Ashton-Miller, J. A. (2024). Pelvic floor injury during vaginal birth is life-altering and preventable: What can we do about it? American Journal of Obstetrics and Gynecology, 230(3), 279-294.e2. View Source.
Dieter, A. A., Wilkins, M. F., & Wu, J. M. (2015). Epidemiological trends and future care needs for pelvic flood disorders. Current Opinion in Obstetrics & Gynecology, 27(5), 380-384. View Source.
Fiani, B., Sekhon, M., Doan, T., Bowers, B., Covarrubias, C., Barthelmass, M., De Stefano, F., & Kondilis, A. (2021). Sacroiliac joint and pelvic dysfunction due to symphysiolysis in postpartum women. Cureus, 13(10), e18619. View Source.
Gunja, M., Gumas, E., Masitha, R., & Zephyrin, L. (2024). Insights into the U.S. maternal mortality crisis: An international comparison. The Commonwealth Fund. View Source.
Harvey, W. R. (1949). The need for physical therapy in postpartum care. Physical Therapy, 29(5), 206-217. View Source.
Hawkins, S. S. (2023). Screening and the new treatment for postpartum depression. Journal of Obstetric, Gynecologic, and Neonatal Nursing: JOGNN, 52(6), 429–441. View Source.
Jundt, K., Peschers, U., & Kentenich, H. (2015). The investigation and treatment of female pelvic floor dysfunction. Deutsches ÄRzteblatt International, 112(33-34), 564-574. View Source.
Lopez-Gonzalez, D. M., & Kopparapu, A. K. (2022). Postpartum care of the new mother. In StatPearls. StatPearls Publishing. Retrieved February 10, 2024. View Source.
Mayo Clinic Staff. (2023). Postpartum care: What to expect after a vaginal birth. Mayo Clinic. View Source.
Mayo Clinic Staff. (2022). C-section recovery: What to expect. Mayo Clinic. View Source.
Mayo Clinic Staff. (2021). Postpartum complications: What you need to know. Mayo Clinic. View Source.
Selman, R., Early, K., Battles, B., Seidenburg, M., Wendel, E., Westerlund, S. (2022). Maximizing recovery in the postpartum period: A timeline for rehabilitation from pregnancy through return to sport. International Journal of Sports Physical Therapy, 17(6), 1170-1183. View Source.
Schulz, J. M., Marmura, H., Hewitt, C. M., Parkinson, L. J., & Thornton, J.S. (2023). Navigating the ‘new normal’: What guidelines exist for postpartum return to physical activity and sport? A scoping review. British Journal of Sports Medicine, 57(24), 1573-1578. View Source.
Simonds, A. H., Abraham, K., & Spitznagle, T. (2022). Clinical practice guidelines for pelvic girdle pain in the postpartum population. Journal of Women’s Health Physical Therapy, 46(1), E1-E28. View Source.
Sissons, B. (2023). Does breastfeeding help with weight loss? Why it may or may not happen. Medical News Today. View Source.
Sponseller, L., Silverman, F., & Roberts, P. (2021). Exploring the role of occupational therapy with mothers who breastfeed. American Journal of Occupational Therapy, 75, 7505205110. View Source.
Tully, K. P., Stuebe, A. M., & Verbiest, S. B. (2017). The fourth trimester: A critical transition period with unmet maternal health needs. American Journal of Obstetrics and Gynecology, 217(1), 37–41. View Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.