This course will be updated or discontinued on or before Sunday, February 14, 2027
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will be able to identify common pediatric respiratory illnesses.
Objectives
After completing this continuing education course, the participant will be able to:
Describe pediatric respiratory anatomy, physiology, and pathophysiology of pediatric respiratory illnesses.
Differentiate between the signs and symptoms of common pediatric respiratory illnesses.
Identify methods of definitive diagnosis for common pediatric respiratory illnesses.
Describe clinical care and interventions for pediatric respiratory illnesses.
Explain infection prevention methods for common pediatric respiratory illnesses.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Respiratory illnesses are a significant cause of sickness and healthcare utilization in children. These illnesses can rapidly progress from mild to life-threatening in the vulnerable pediatric population. Healthcare providers must have the knowledge and skills to accurately assess and differentiate between various respiratory illnesses to provide timely intervention and treatment. Clinicians must provide patients and caregivers with comprehensive and clear education regarding treating and preventing the respiratory illness.
Understanding the pathophysiology of common pediatric respiratory infections requires an appreciation for the normal anatomy and physiology of the pediatric respiratory system.
The respiratory system is split into two tracts at a basic level, the upper and the lower. The upper respiratory system provides a patent path for air to enter and exit the lungs through the nose and mouth while also filtering, warming, and humidifying the air. The lower respiratory system serves to provide gas exchange.
Table 1: Upper vs. Lower Respiratory Tract
Upper Respiratory Tract
Lower Respiratory Tract
Nose
Nasal cavity
Mouth
Sinuses
Pharynx
Larynx (above vocal folds)
Larynx (below vocal folds)
Trachea
Lungs
Bronchi
Bronchioles
Alveoli
Diaphragm
Image 1: Pediatric Respiratory Tract
The primary role of the respiratory system is to exchange gases. When children breathe, air enters the body through the upper respiratory tract and the nose and travels down the lower respiratory tract from the larynx and the trachea to the lungs through the main-stem bronchi to the right lung and the left lung. The main-stem bronchi divide into small bronchi, and even smaller tubes called bronchioles. The bronchioles end in tiny balloon-like air sacs called alveoli. Oxygenation occurs as oxygen is taken into the lungs through inspiration and diffuses across the alveoli into the blood to dissolve in the plasma and attach to the hemoglobin. Carbon dioxide diffuses from the blood across the capillaries into the alveoli, and is excreted through expiration, known as ventilation.
Image 2: Alveolus Gas Exchange
When the pediatric respiratory system inadequately functions due to respiratory illness, poor oxygenation results in hypoxemia, and poor ventilation results in hypercarbia. Because children have a high metabolic rate and oxygen demand is higher per kilogram of body weight versus an adult, children decompensate more rapidly than adults:
Understanding pediatric respiratory anatomy and physiology provides a foundation for classifying pediatric respiratory problems and associated clinical signs and symptoms. Respiratory conditions can be categorized individually or in combination as upper airway, lower airway, parenchymal disease, and disordered control of breathing.
Parenchymal disease is a group of conditions that affect the substance of the lung tissue. It is characterized by alveolar and small airway collapse. Common causes include:
Disordered control of breathing is an abnormal pattern that produces respiratory symptoms such as inadequate respiratory rate or effort. Common causes include:
Assessing the pediatric patient's clinical signs and symptoms indicates the severity of respiratory distress and classification of respiratory illness to help determine the underlying cause and potential treatments.
The components of the complete respiratory assessment include inspection, palpation, auscultation, and percussion. These components and their included parts are listed in Table 2 below.
Table 2: Pediatric Respiratory Assessment
Assessment Component
Elements
Inspection
Rate (best to do prior to hands-on assessments)
Depth
Ease
Symmetry
Rhythm
Palpation
Tracheal position
Symmetry of chest wall movement
Vibration with vocalization
Auscultation
Quality of breath sound
Fine/Course crackles
Wheezing
Rhonchi
*consider lung anatomy to identify the location of abnormal sounds
Percussion
Tympanic vs. dull sounds
Because children can rapidly decompensate, the healthcare provider must identify red flags during the assessment. Extrapulmonary manifestations of respiratory disease or respiratory disorders may be secondary to disease in other systems. Therefore, assessing the patient and identifying critical symptoms is crucial.
Consider the following questions or ABC approach during the assessment:
There are several types of pediatric respiratory conditions. Bacteria, viruses, or fungi cause many illnesses that affect the respiratory tract. Common pediatric respiratory illnesses include bronchiolitis, croup, pertussis, and pneumonia.
Bronchiolitis is a respiratory disorder caused by lower respiratory tract infections in infants. It is the most common cause of lower respiratory tract infection in children less than two years of age and hospitalization of infants younger than 12 months(Ralston et al., 2014). The incidence of bronchiolitis hospitalizations has decreased from 2000-2016 from 17.9 to 13.5 per 1000 person-years in U.S. children. However, hospital costs increased from $449 million to $734 million nationally from 2003-2016 (Fujiogi et al., 2019). Characteristics of bronchiolitis include:
Acute inflammation
Edema
Necrosis of epithelial cells lining small airways
Increased mucous production
Bronchiolitis typically presents with rhinitis and cough, further progressing to tachypnea, wheezing, rales, increased work of breathing, and nasal flaring (Agency for Healthcare Research and Quality [AHRQ], 2003).
The most common cause of bronchiolitis is the respiratory syncytial virus (RSV), which was first discovered in 1956. The highest incidence of infection is typically between December and March in North America, and the severity and occurrence can vary from year to year(Ralston et al., 2014).
Greenough et al. (2001) cited that 90% of children are infected with RSV in the first two years of life, and Silver and Nazif (2019) identified RSV in 80% of bronchiolitis cases. Presenting symptoms in young children typically include (Centers for Disease Control and Prevention [CDC], 2020):
Decreased appetite
Rhinorrhea
Followed by a cough 1-3 days later
Fever
Wheezing
In very young infants, presenting symptoms of RSV can include (CDC, 2020):
Irritability
Lethargy
Apnea
Rhinovirus is another common culprit associated with children's respiratory tract infections and bronchiolitis. It commonly occurs in spring and fall (Hasegawa, 2019). Human rhinoviruses cause the common cold, and there are over 170 serotypes. Also, bronchiolitis is caused by other viruses, including adenovirus, human metapneumovirus, influenza, and parainfluenza. Of note, prior to the arrival of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), coronavirus-related bronchiolitis infections were often coinfections with RSV (Mansbach et al., 2020).
Diagnosis of bronchiolitis should be made by clinical assessment of disease severity through history and physical exam (Wade, 2020). Additional testing may be indicated based on clinical concerns. A chest x-ray may be considered if there is suspicion of an alternative diagnosis, such as pneumonia. If there is clinical concern for respiratory failure, lab tests, such as blood gas, may be indicated. Infants under three months old with persistent fever and severe symptoms should have additional blood work, including blood cultures.
For pediatric patients who may be admitted and cohorts in a hospital setting or children in group childcare settings where the spread is a concern, a respiratory viral panel or swab may be indicated to confirm the causative agent, such as influenza or SARS-CoV-2. Clinicians need to note that clinical features alone cannot confirm the specific type of viral infection, and careful deliberation in diagnostic testing for respiratory viruses remains important for accurate diagnoses to prevent unnecessary prescriptions of antivirals (Ma et al., 2018; Wang et al., 2020).
Children with mild to moderate bronchiolitis may be managed in the outpatient setting. Clinicians shall instruct caregivers on supportive interventions and worsening illness signs and symptoms. Supportive measures in the home include hydration and nutrition support, fever management, and suctioning.
In cases of worsening or severe bronchiolitis, children may require admission to the acute care hospital setting. Educate caregivers of signs or symptoms of worsening illness such as:
Increased respiratory effort cyanosis
Lethargy
Persistent fever
Not responding to antipyretics
Inability to maintain nutrition/hydration status
Indications for admission include a requirement for supplemental oxygen, dehydration, apnea, severe respiratory distress, and underlying risk factors for severe disease. The recommended treatment in the hospital includes supportive care. Supportive care in this case includes(Wade, 2020):
Supplemental oxygen to maintain oxygen saturation greater than 90%
Supportive hydration
Supportive nutrition measures, such as nasogastric feeds or intravenous fluids
Fever management
In severe cases, high-flow oxygen, non-invasive ventilation, and possibly intubation might be indicated (Wade, 2020).
Infants with bronchiolitis who present with significant respiratory distress and are not responding to supportive care interventions may benefit from additional treatment considerations. Research does not demonstrate evidence to support the routine use of albuterol treatment for infants with bronchiolitis. However, a trial for infants who present with clinical features more suggestive of asthma (recurrent wheezing episodes and previous treatments with inhaled corticosteroids) could be considered and only continued if they respond favorably to the test dose (Dunn et al., 2020). Clinicians may also consider Racemic Epinephrine in cases of increasing severe respiratory distress.
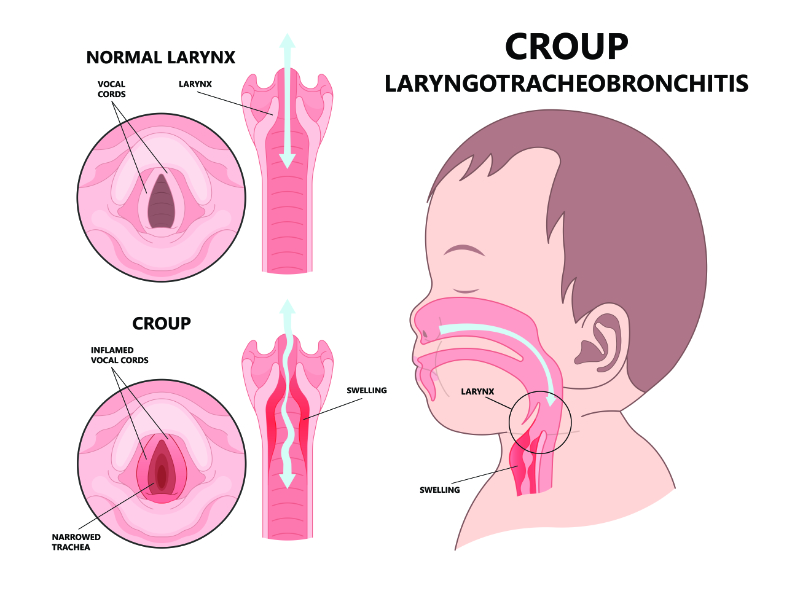
Croup is an encompassing term for illnesses affecting the larynx, trachea, and bronchi. It is a common upper respiratory illness in children characterized by inspiratory stridor, barking cough, and hoarseness. Laryngotracheitis, laryngotracheobronchitis, laryngotracheobronchopneumonitis, and spasmodic croup are all categorized in the croup spectrum. Typically, croup is differentiated into two distinct types: viral croup and spasmodic croup. A review of emergency department visits in the United States between 2007 to 2014 estimated there were approximately 400,000 croup-related visits annually(Hanna, 2019). About 3% of children are affected by croup annually, and the age range is typically between six months and three years(Sizar & Carr, 2022). Croup is characterized by swelling of the larynx, trachea, and large bronchi due to infiltration of white blood cells—the inflammation results in narrowing of the airway and partial obstruction, causing increased work of breathing and stridor.
Image 3: Croup
Children with croup typically present with one to two days of upper respiratory infection, followed by a signature seal-like barking cough, stridor, hoarseness, and difficulty breathing. Symptoms are often worse at night and may be accompanied by fever. The duration of illness is usually three to seven days, with the most severe presentation on day three or four (Sizar & Carr, 2022).
Clinicians need to observe for rapid progression of symptoms or for signs of lower airway involvement, which may suggest a more severe illness that requires rapid intervention.
A viral infection usually causes croup in the fall or early winter. Like bronchiolitis, common viral pathogens of croup include(Johnson, 2014):
Parainfluenza or influenza
Adenovirus
RSV
Measles
Rhinovirus
Enterovirus
Human coronaviruses
Metapneumoviruses
The Parainfluenza viruses account for more than 75% of croup diagnoses(Johnson, 2014). Parainfluenza virus type 1 is the most common cause, especially in the fall and winter months (Woods, 2022). Parainfluenza virus type 2 usually presents with milder disease than type 1, while Parainfluenza virus type 3 cases are often more severe than those of type 1 or 2 (Woods, 2022). Pediatric patients with SARS-CoV-2, particularly during the 2022 Omicron surge, have increasingly manifested with croup (Murata et al., 2022).
Bacterial infection is rarely the cause of pediatric croup illnesses. Mycoplasma pneumonia can present as a mild croup-like illness. Bacterial infections may occur secondarily to croup, and pathogens commonly include (Sizar & Carr, 2022):
Corynebacterium diphtheria
Staphylococcus aureus
Streptococcus pneumoniae
Hemophilus influenzae
Moraxella catarrhalis
Evaluation and diagnosis of suspected croup in children should focus on identifying those with severe or rapidly professing upper airway obstruction. Healthcare workers must foster an environment that is comfortable and calming to minimize fear and anxiety, which can exacerbate subglottic narrowing, leading to the progression of the illness. Diagnosis is primarily made on clinical assessment through observation of symptoms like:
Barking cough
Hoarseness
Inspiratory stridor
History of recent upper respiratory infection symptoms like runny nose or cough
It is not recommended to pursue diagnostic testing, such as respiratory lab panels or x-rays, to diagnose croup. If an etiologic diagnosis is necessary to make decisions or inform regarding isolation and prevention practices, secretions from the nasopharynx may be obtained for viral etiology.
When symptoms are progressing rapidly or patients are not responding to routine croup treatment, ruling out other obstructive conditions is essential. Assessment findings may indicate another condition. Findings that might indicate something else is going on include(Bhatia, 2018):
Drooling
Dysphagia
Expiratory wheezes
Toxic appearance
Prolonged stridor
Loss of voice
Other obstructive conditions that might explain these findings may include (Bhatia, 2018):
Epiglottitis
Foreign body airway obstruction
Subglottic stenosis
Congenital airway anomalies
Allergic reaction/angioedema
Peritonsillar or retropharyngeal abscess
Bacterial tracheitis
Treatment of croup is associated with the severity of illness, primarily determined by the presence or absence of stridor at rest, work of breathing with chest wall retractions, air entry, presence or absence of pallor or cyanosis, and mental status (Woods, 2022). Most pediatric patients with croup can be managed as outpatients, but those who present with moderate to severe symptoms may require the emergency department or inpatient care.
Caregivers of children with mild croup should be instructed to treat them symptomatically with humidity, antipyretics, and hydration. Although no systematic research exists, exposure to cold night air may reduce symptoms. Mild croup may also be treated with a single dose of oral dexamethasone or prednisolone (Woods, 2021).
Furthermore, caregivers should be educated on signs and symptoms to observe for worsening conditions requiring medical attention. These symptoms include:
Stridor at rest
Difficulty breathing
Pallor or cyanosis
Severe coughing
Drooling or difficulty swallowing
Fatigue or lethargy
Persistent or worsening fever
Increased work of breathing with retractions
Symptoms that persist for more than seven days
For those patients with moderate to severe croup, treatment in an emergency department or acute care setting includes corticosteroids (dexamethasone is preferred) and nebulized epinephrine directed towards decreasing airway edema(Woods, 2021). Supportive care includes humidified air, oxygen supplementation to maintain saturation > 90%, antipyretics, and nutrition and hydration support. Patients who respond to initial treatment should be observed for four hours and may continue supportive home treatment if they have no stridor at rest, normal oxygenation and good air exchange, no cyanosis can tolerate fluids orally, and caregivers are instructed and understand signs and symptoms of worsening and when to seek medical attention.
The child may need to be admitted for further management under the following conditions:
Because croup is most commonly a viral illness, antibiotics are indicated only when a primary or secondary bacterial infection is suspected (Sizar & Carr, 2022). For most cases of pediatric croup, the prognosis is excellent, and the illness resolves in a few days.
Pneumonia is an inflammatory condition of the lungs associated with fever, respiratory symptoms, and parenchymal involvement. According to the World Health Organization, pneumonia is the single largest cause of death in children related to infection worldwide, and in 2019, pneumonia accounted for 14% of deaths of children under five (World Health Organization [WHO], 2022).
Pneumonia can be caused by several different microorganisms, including bacteria, viruses, and fungi, and varies according to the child's age and the setting in which the infection is acquired. Pneumonia commonly presents after an upper respiratory tract illness that travels to the lower respiratory tract triggering an immune response that produces inflammation. Bronchiole and alveoli fill with white blood cells, fluid, and cellular debris, causing reduced lung compliance, increased resistance, airway obstruction, and altered ventilation and perfusion(Barson, 2022).
Image 4: Pneumonia
Pneumonia can be described in different categories, often associated with its etiology. Different types of pneumonia will be reviewed shortly.
The presenting signs and symptoms of pneumonia in children are nonspecific. Children may present with fever, cough, and other respiratory findings, such as increased work of breathing. Infants may show signs of difficulty eating, restlessness, or fussiness. Some children will complain of pleuritic chest pain with breathing.
Diagnosis can be based on history and physical exam with a previous history of the infectious process and signs and symptoms of respiratory distress (Barson, 2022; Schuster et al., 2017). Radiographs are not necessary for the diagnosis of mild pneumonia. In cases where the diagnosis is not specific, for children with other risk factors, such as those who are immunocompromised, cystic fibrosis, or sickle cell disease, or those who present with severe symptoms requiring hospitalization, radiographs should be obtained. Microbiologic testing may be used with radiographic diagnostics for children with severe disease, potential complications, hospitalization, an unusual pathogen is suspected, or if they fail to respond to therapy.
The Pediatric Infectious Disease Society and the Infectious Diseases Society of America offer links to government-sponsored guidelines from countries and regions around the world based on environmental trends and available treatments. Treatment for pneumonia is dependent on the causative agent. Viral cases of pneumonia do not require antibiotic therapy unless a secondary bacterial infection is suspected. Antimicrobial therapy is crucial in treating community-acquired pneumonia but depends on the pathogen, susceptibility, tolerability, and cost. Additional treatment for severe cases where hospitalization is indicated may include antipyretics, analgesics, respiratory support, fluid management, and chest physiotherapy.
Community-acquired pneumonia, aspiration pneumonia, and hospital-acquired pneumonia have different agents responsible for the infection.
Community-acquired pneumonia (CAP) in children < 5 years old is most commonly caused by viruses. However, bacterial pathogens can include Streptococcus pneumoniae, Staphylococcus aureus, and Streptococcus pyogenes(Barson, 2022; Schuster et al., 2017). Streptococcus pneumonia is the most common cause of bacterial pneumonia in children, and respiratory syncytial virus (RSV) is the most common viral cause in children(WHO, 2022).
Healthy children ≥ 5 years are most commonly infected with S. pneumoniae, Mycoplasma pneumoniae, and Chlamydia pneumonia(Barson, 2022). Community-associated methicillin-resistant S. aureus is an increasingly important pathogen for all ages. Cases of necrotizing pneumonia include bacteria S. pneumoniae, S. aureus, and S. pyogenes(Barson, 2022).
Aspiration pneumonia occurs when a child breathes either food or liquid into the airways or lungs, rather than swallowing them and the contents passing down the esophagus. This type of pneumonia is most commonly caused by anaerobic oral flora.
Gram-negative bacilli or S. aureus are the agents typically associated with hospital-acquired pneumonia, usually seen in intensive care settings where patients are mechanically ventilated, have indwelling catheters, and receive broad-spectrum antibiotics.
Pertussis, also known as whooping cough, is a respiratory infection caused by Bordetella pertussis.
Pertussis was one of the most prevalent pediatric diseases and major causes of U.S. childhood mortality in the 20th century, with more than 200,000 cases annually (CDC, 2022). With the development of the pertussis vaccine in the 1940s, the incidence has decreased by more than 75% than pre-vaccine(CDC, 2022). However, from the late 1980s through the start of the COVID-19 pandemic in 2022, the number of cases of pertussis has increased.
The highest rates of pertussis are in infants younger than age one year (Bhuiyan et al., 2021). In 2018, pertussis incidence per 100,000 was 72.3 in infants younger than age six months and 32.7 in infants aged 6 to 12 months, compared to 1.4 in persons aged 20 years or older (Havers et al., 2021). One-third of infants less than 12 months with pertussis need hospitalization for care (CDC, 2022). The Centers for Disease Control and Prevention (CDC) reported 48,277 cases of pertussis in 2012, the last peak year. The CDC suggested the increase may be related to increased awareness and recognition of diagnosis, increased surveillance and reporting to public health departments, greater acceptance of diagnostics, and waning immunity from historical vaccinations.
The clinical course of pertussis has three stages: Catarrhal, paroxysmal, and convalescent. The disease may present differently in certain children; therefore, it is vital to have awareness and recognition of pertussis and differential diagnoses in this population.
In the initial phase, catarrhal, pertussis presents like the common cold, but coughing can progress for weeks to months. Cold-like symptoms, runny nose, sneezing, low fever, and mild cough are generally minimal. However, patients are most contagious at this time.
The later symptoms start one to two weeks after the first symptoms, the paroxysmal phase, when the cough may progress to rapid, violent, uncontrollable fits. The coughing fits worsen over time and can last up to 10 weeks.
The "whoop" associated with the name “whooping cough” comes from the high-pitched "whoop" sounds that children make when they can inhale at the end of a coughing fit. Additional symptoms children experience during this phase and due to cough paroxysms are vomiting during and after coughing, feeling tired, and struggling to breathe (CDC, 2022).
Paroxysmal attacks commonly occur more at night, with an average of 15 attacks per 24 hours (Havers et al., 2021). Apnea is also a symptom during this phase. Infants may not have the classic symptoms and may only present with apnea and minimal or absent cough(CDC, 2022).
In the last phase, recovery or convalescence, occasional paroxysmal coughing spells may continue for two to three weeks. Patients with a history of pertussis may have reoccurring paroxysms with subsequent respiratory infections for many months (Havers et al., 2021).
Image 5: Pertussis Disease Progression
Source: Centers for Disease Control and Prevention
Diagnosis of pertussis can be made through clinical assessment, typically during the paroxysmal stage because of the persistent, chronic cough or infant with reported apnea. Additional laboratory tests can be used to confirm the diagnosis. The preferred diagnostic test is a culture; however, particular growth requirements make B. pertussis challenging to culture. Cultures should be obtained within the first two weeks of illness and be collected from the posterior nasopharynx using polyester, rayon, nylon, or calcium alginate swabs (Havers et al., 2021). A PCR test, or polymerase chain reaction test, is another reliable test with excellent sensitivity and the ability to obtain rapid results by detecting the presence of a virus (Vicentini et al., 2022). PCR tests are also from nasopharyngeal specimens but may be accurate for up to 4 weeks of symptomatic infants or unvaccinated patients. In the later phase of illness, serologic testing specimens may be obtained between 2 to 8 weeks following cough onset and up to 12 weeks. The single-point serologic assay is part of many states’ public health testing practices.
Pertussis may be treated with antibiotics if administered within the first one to two weeks of cough before paroxysms(Vincentini et al., 2022). Antibiotic selection is based on age and other patient-specific indications. The American Academy of Pediatrics (AAP) recommends a five-day azithromycin course as a first-line treatment(Kline et al., 2021).
Infants and children with high suspicion of illness should begin antibiotics before confirming test results (CDC, 2022). Although the antimicrobials do not affect the severity or duration once the cough is present, they should still be prescribed to prevent disease spread. Additional treatment for pertussis includes supportive care such as secretion management, supplemental oxygen, and respiratory support in severe cases.
Unvaccinated or partially vaccinated infants less than 12 months old have the most significant risk of severe disease or death in infants (Havers et al., 2021). Immunity following pertussis is not everlasting. Vaccination is the primary means of prevention and spread. DTaP (diphtheria, tetanus toxoids, and acellular pertussis vaccine) is an intramuscular injection recommended for children aged six weeks through 6 years. The typical schedule is a primary series of 3 doses at ages 2, 4, and 6 months, a booster dose between ages 15 and 18 months, and another booster dose between ages 4 through 6 years (CDC, 2022). The CDC website (Vaccines Help Protect against Whooping Cough | CDC) provides an immunization schedule for children at risk or who may have contraindications to the routine vaccination recommendations.
Image 6: Pertussis Disease Progression
Source: Centers for Disease Control and Prevention (CDC)
Unfortunately, respiratory illnesses remain common in children. It is vital to encourage caregivers and children to stay current on immunizations that may prevent or decrease the severity of respiratory illnesses. Practicing and teaching patients and caregivers good hand hygiene is another effective preventative strategy. The CDC estimates that handwashing could protect 1 in 5 children from respiratory illness(CDC, 2022). Furthermore, the importance of nutrition and sleep should not be overlooked. Sleep and nutrition are critical in immune regulation response. Children should have a consistent bedtime routine and adequate sleep (Peck, 2022).
Parents present to the clinic with their seven-month-old infant stating she has episodes where it appears she stops breathing. Upon obtaining her history, it is noted the infant was born via vaginal delivery at 42 weeks gestation in a home birth. There is no pediatrician of record listed on file. You ask the parents if the patient is up to date on immunizations and the mother explains they have chosen not to vaccinate their child for personal reasons. What common pediatric respiratory infection is important to consider in this situation?
Make sure to keep in mind that Pertussis is a vaccine-preventable respiratory illness that could be to blame for these symptoms. Also, remember that apnea may be the only presenting symptom in infants.
After considering pertussis as a potential diagnosis, you gather additional information from the parents. The parents state they have noticed the apnea on occasion for about three weeks, but it always appeared brief. The mother also reports the infant had a few episodes of cough but did not think much of it because it was only a few times and did not seem to bother the baby. After a physical exam, there are no other concerning signs and symptoms. How do you move forward with a diagnosis and treatment?
It is important to confirm the diagnosis with either PCR or serologic testing per the local health department. Do not wait for positive results and start the patient on a five-day course of azithromycin dosing according to the patient weight and AAP recommendations. Additionally, educate the parents on the importance of immunizations and the recommended timeline.
A 15-month-old with visible respiratory distress presents to the emergency department, being carried by his mother. The mother tells you that he has had a runny nose for a few days and a cough for the past two days. She noticed overnight she could hear on the monitor that he was struggling to breathe and was whimpering, so she went to check on him. He felt warm, so she gave him Tylenol, but he was breathing so fast that he vomited immediately afterward. She reports he attends daycare, and today when she picked him up, the teacher said he did not eat or drink much and only had one wet diaper.
Upon physical assessment, you note copious nasal secretions, tachypnea with intercostal retractions, nasal flaring, rales upon auscultation, dry mucous membranes, and acrocyanosis. Vital signs include HR: 122, RR: 56, Pox 88%, Temp: 100.6 degrees Fahrenheit.
What common pediatric respiratory illness could the patient have? What are some interventions to consider? What diagnostics should be obtained?
Bronchiolitis is likely to be blamed for this patient’s symptoms and current presentation. Given the respiratory distress and abnormal vital signs, the patient needs to be placed on oxygen and begin additional supportive care. Additional respiratory care should include frequent suctioning to maintain a clear airway. While suctioning, consider obtaining a nasopharyngeal specimen for respiratory panel testing. Because the patient is in daycare and likely will require admission, confirming the potential pathogen is important to prevent spread and provide necessary notifications in the childcare facility. Given the patient's decreased oral intake and output, place an IV and provide hydration assistance. Also, consider rectal acetaminophen for fever reduction.
After spending three days admitted receiving care for bronchiolitis due to RSV, the patient has not been able to tolerate oral intake, is now coughing more frequently, the supplemental oxygen requirement increased, and fevers are trending up, persistently over 102 degrees Fahrenheit without antipyretics around the clock. Upon physical examination you now note decreased air exchange and crackles in the left lower lobe. What additional diagnosis do you consider? Do you need to do additional testing to confirm the diagnosis?
At this point, it is important to consider viral pneumonia. Respiratory syncytial virus (RSV) is the most common viral of pneumonia cause in children (WHO, 2022). Although a radiograph is not necessary to confirm a pneumonia diagnosis in children with mild cases, for those who present with severe symptoms requiring hospitalization, radiographs should be obtained.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Agency for Healthcare Research and Quality. (AHRQ). (2003). Management of bronchiolitis in infants and children. Evidence report/technology assessment No. 69. Agency for Healthcare Research and Quality: Publication N. 03-EO14. Visit Source.
Barson, W. (2022). Pneumonia in children: Epidemiology, pathogenesis, and etiology. UpToDate. Retrieved October 2022. Visit Source.
Bhatia, R. (2018). Croup (Laryngotracheobronchitis). Merck Manual (Professional Version). Retrieved October 2022. Visit Source.
Bhuiyan, M. Stiboy, E., Hassan, M., Chan, M., Islam, M., Haider, N., Jaffe, A., & Homaira, N. (2021). Epidemiology of COVID-19 infection in young children under five years: A systematic review and meta-analysis. Vaccine, 39(4): 667-677. Visit Source.
Centers for Disease Control and Prevention. (CDC). (2020). Respiratory syncytial virus (RSV). Centers for Disease and Prevention. (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2022). Handwashing in communities: Clean hands save lives. Visit Source.
Dunn, M., Mathu, N., Burlingame, C., Gahman, A., McCloskey, M., Tyler., L., Ware, R., & Zorc, J. (2020). Reducing albuterol use in children with bronchiolitis. Pediatrics, 145. Visit Source.
Greenough, A., Cox, S., Alexander, J., Lenny, W., Turnbull, F., Burgess, S., Chetcuti, P., Shaw., N., Woods, A., Boorman, J., Coles, S., & Turner, J. (2001). Health care utilization of infants with chronic lung disease related to hospitalization for RSV infection. Archives of Disease in Childhood, 85: 463-468. Visit Source.
Fujiogi, M., Goto, T., Yasunga, H., Fujishiro, J., Mansbach, J., & Carmargo, C., Hasegawa, K. (2019). Trends in bronchiolitis hospitalization in the United States: 200-2016. Pediatrics, 144(6). Visit Source.
Hanna, J, (2019). Epidemiological analysis of croup in the emergency department using two national datasets. International Journal of Pediatric Otorhinolaryngology, 126. Visit Source.
Havers, F., Moro, P., Hariri, S., & Skoff, T. (2021). Pertussis. Centers for Disease Control and Prevention. (CDC). Epidemiology and Prevention of Vaccine-Preventable Diseases, 14. 239-254. Visit Source.
Hasegawa, K. (2019). Respiratory virus epidemiology among U.S. infants with severe bronchiolitis: Analysis of 2 multicenter, multiyear cohort studies. The Pediatric Infectious Disease Journal. Visit Source.
Johnson, D. (2014). Croup. BMJ Clinical Evidence. Visit Source.
Kline, J., Smith, E., & Zavala, A. (2021). Pertussis: Common questions and answers. American Family Physician, 104(2), 186–192. Visit Source.
Mansbach, J., Hasegawa, K., Piedra, P., Sullivan, A., & Camargo, C. (2020). Severe coronavirus bronchiolitis in the pre-covid-19 era. Pediatrics, 146(3). Visit Source.
Ma, X., Conrad, T., Alchikh, M., Reiche, J., Schweiger, B., & Rath, B. (2018). Can we distinguish respiratory viral infections based on clinical features? A prospective pediatric cohort compared to systematic literature review. Reviews in Medical Virology, 28(5), e1997. Visit Source.
Murata, Y., Tomari, K., & Matsuoka, T. (2022). Children with croup and SARS-CoV-2 infection during the large outbreak of Omicron. Pediatric Infectious Disease Journal, 41-46. Visit Source.
Neill, S. & Dean, N. (2019). Aspiration pneumonia and pneumonitis: A spectrum of infectious/noninfectious diseases affecting the lung. Current Opinion in Infectious Diseases. 32(2): 152-157. Visit Source.
Peck, J. (2022). Infection control in pediatrics: Primary preventions to promote child health. Infection Control Today, 26(9). Visit Source.
Ralston, S., Lieberthal, A., Meissner, H. Alverson, B., Baley, J., Gadomski, A., Johnson, D,. Light, M., Maraqa, N., Mendonca, E., Phelan, K., Zorc, J., Stanko-Lopp, D., Brown, M., Nathanson, I., Rosenblum, E., Sayles, S., & Hernandez-Cancio. (2014). Clinical practice guideline: The diagnosis, management, and prevention of bronchiolitis. Pediatrics, 136(5): e1474-e1502. Visit Source.
Schuster, B., Hoare, C., Mukherjee, A., & Paul, S. (2017). Managing acute respiratory tract infections in children. British Journal of Nursing, 26(11): 602-609. Visit Source.
Silver, A., & Nazif, J. (2019). Bronchiolitis. Pediatrics in Review, 40(11): 568-576. Visit Source.
Sizar, O., & Carr, B. (2022, July 25). Croup. In StatPearls. StatPearls Publishing. Visit Source.
Vicentini, C., Vola, L., Previti, C., Brescia, V., Dal Mas, F., Zotti, C., & Bert, F. (2022). Antimicrobial stewardship strategies including point-of-care testing (POCT) for pediatric patients with upper respiratory-tract infections in primary care: A systematic review of economic evaluations. Antibiotics, 11(8): 1139. Visit Source.
Wade, T. (2020). Approach to bronchiolitis from PedsCases Notes. Medical Diagnosis and Treatment. Visit Source.
Wang, X., Li, Y., O’Brien, K., Madhi, S., Widdowson, M., Byass, P., Omer, S., Abbas, Q., Ali, A., Amu, A. Azziz-Baumgartner, E., Basset, Q., Abdullah Brooks, W., Chaves, S., Chung, A., Cohen, C., Echavarria, M., Fasce, R., Gentile, A., . . . Nair, H. (2020). Global burden of respiratory infections associated with seasonal influenza in children under 5 years in 2018: A systematic review and modeling study. The Lancet: Global Health, 8(4): e497-e510. Visit Source.
Woods, C. (2022). Croup: Clinical features, evaluation, and diagnosis. UpToDate. Retrieved October 2022. Visit Source.
Woods, C. (2021). Management of croup. UpToDate. Retrieved October 2022. Visit Source.
World Health Organization. (WHO). (2022). Pneumonia in children. World Health Organization (WHO). Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.