This course will be updated or discontinued on or before Thursday, December 10, 2026
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will know how to interpret neonatal blood gases.
Objectives
After completing this continuing education course, the participant will be able to:
Interpret why obtaining neonatal blood gases is necessary.
List normal blood gas parameters for pH, PaCO2, and HCO3.
Explain acid-base balance and how it works.
Determine the clinical status of arterial blood gases with acid-base disorders.
Analyze compensated versus uncompensated blood gases.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
In addition to physical assessment to determine respiratory disease, chemical assessment via blood gases is necessary. The purpose of obtaining a blood gas for a neonate is to determine if the baby is adequately ventilating and perfusing. Blood gases are the basis for analyzing if oxygenation is adequate and deducing the acid-base balance in a particular neonate.
The medical plan of care for the neonatal patient includes the frequency of blood gas determination, and it is every care provider's responsibility to be cognizant of each blood gas sample drawn on the patient. The value of timely and accurate interpretation of blood gas results cannot be questioned.
Advances in technology and neonatal care, including artificial surfactant and high-frequency ventilation, have increased the need for a rapid response to quickly changing clinical conditions. Equipment that will allow for in-line blood gas monitoring with an indwelling probe is now available. This allows for more frequent sampling without excessive blood loss, which is a major concern, especially for the tiniest of neonates.
Let’s take a moment to review some definitions that are pertinent to blood gases (Fraser, n.d.; Arias-Oliveras, 2016):
pH: The symbol used to measure the hydrogen ion (H+) concentration.
As the H+ concentration increases, the pH decreases (acidosis).
As the H+ decreases, the pH increases (alkalosis).
A severely depressed pH indicates acute decompensation.
Acid-Base Balance: The pH is the result of the plasma bicarbonate/plasma carbonic acid relationship.
Acid: A substance that can donate H+. An excess of an acid causes decreased pH (< 7.25).
Base: A substance capable of accepting H+. A decrease of H+ causes increased pH (> 7.45).
Lungs: Controls the pH by altering the amount of CO2 that is excreted.
Kidneys: Controls the pH by altering the rate of excretion of HCO3-.
Acidosis: This is a physiologic state where a significant base deficit is present.
Metabolic Acidosis: This acid-base imbalance occurs when a disorder adds acid to the body or causes alkali to be lost faster than the buffer system, which is either the lungs or the kidneys, can regulate the load.
Respiratory Acidosis: This acid-base imbalance occurs when the lungs do not promptly vent carbon dioxide, and carbon dioxide combines with bicarbonate to form carbonic acid.
Alkalosis: This is a physiologic state in which there is more than a normal base present.
Metabolic Alkalosis: This acid-base imbalance occurs whenever acid is excessively lost, or alkali is excessively retained. The acid-base ratio of the body is, therefore, altered.
Respiratory Alkalosis: This acid-base imbalance occurs when carbon dioxide is excreted by the lungs in excess of its production rate by the body. When this happens, the level of carbonic acid falls, which produces an excess amount of bicarbonate in relation to the acid content.
Compensation: This is the secondary physiologic process occurring in response to a primary disturbance in the acid-base balance by which the deviation of pH is lessened, or essentially, compensated for.
Correction: This is a change in the system originally affected by the primary disturbance by an intervention using available therapy or treatment modality.
The classification and interpretation of blood gas results are based on the use of and the understanding of normal values.
The normal values for the term and preterm infants do differ slightly from values for the adult because of immaturity and the presence of fetal hemoglobin. In addition, the exact values accepted as what would be classifiedas “normal” may vary from institution to institution, based on the reference ranges utilized (Fraser, n.d.):
The acid-base balance is maintained within narrow limits by internal interactions that are complex between the respiratory system and the kidneys.
There are four main components to the arterial blood gas results:
pH
PaCO2
Bicarbonate (HCO3-) or base excess
PaO2
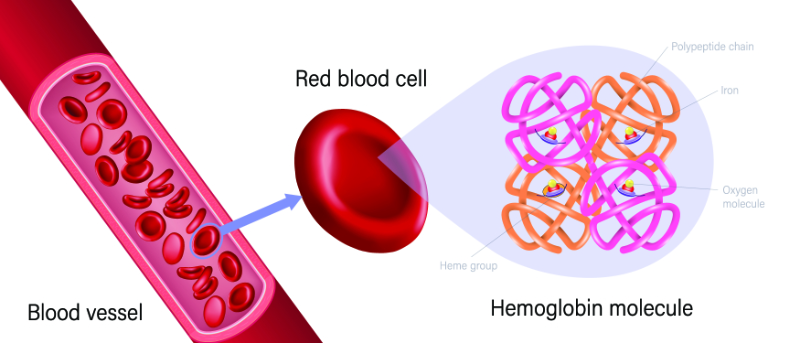
Oxygen diffuses across the alveolar-capillary membrane, moved by the difference in oxygen pressure between the alveolus and the blood. In the blood, oxygen dissolves in the plasma and binds to hemoglobin.
Image 2: Hemoglobin
Arterial oxygen content (CaO2) is the sum of dissolved and hemoglobin-bound oxygen as described by the following equation (Rosen & Manaker, 2024):
CaO2 = (1.34 x Hb x SaO2) + (0.0031 x PaO2)
In this formula(Rosen & Manaker, 2024):
CaO2 = Arterial oxygen content (ml/100 ml of blood)
1.34 = Milliliters of oxygen-bound to 1 g of hemoglobin at 100% saturation
Hb = Hemoglobin concentration (g/dl)
SaO2 = Percent of hemoglobin bound to oxygen (%)
0.0031 = Solubility factor of oxygen in plasma (mL/mmHg)
PaO2 = Oxygen partial pressure in arterial blood (mmHg)
In the equation for arterial oxygen content, the first term (1.34 x Hb x SaO2) is the amount of oxygen bound to hemoglobin. The second term (0.0031 x PaO2) is the amount of oxygen dissolved in plasma. Most of the oxygen in the blood is carried by hemoglobin (Rosen & Manaker, 2024).
For example, if a premature infant has a PaO2 of 60 mmHg, a SaO2 of 92%, and a hemoglobin concentration of 14 g/dL:
CaO2 is the sum of oxygen bound to hemoglobin, plus the oxygen dissolved in plasma.
(1.34 x 14 x 92/100) + (0.0031 x 60) 17.3 mL + 0.186 mL = 0.18 mL
In this example, less than 2% of oxygen in the blood is dissolved in plasma. The other 98% is carried by hemoglobin (Rosen & Manaker, 2024).
If an infant has an intraventricular hemorrhage (IVH) and their hemoglobin concentrations drop to 10.5 g/dL, but PaO2 and SaO2 remain the same, CaO2 equals 12.9 mL/dL of blood. Thus, without any change in PaO2 or SaO2, a 25% drop in hemoglobin concentration reduces the amount of oxygen in arterial blood by 25%. This concept is important to understand and remember when taking care of patients with respiratory disease. These patients need to be monitored and, if found to have low oxygen, this must be corrected for them to maintain an adequate level of oxygenation.
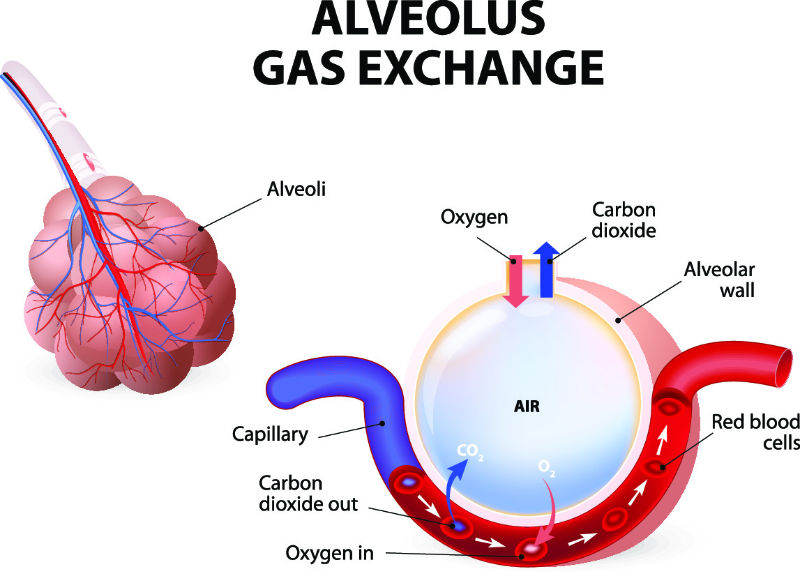
The difference in partial pressure of oxygen is the force that loads hemoglobin with oxygen in the lungs and then unloads it in the tissues (Rosen & Manaker, 2024). In the lungs, alveolar oxygen partial pressure is higher than capillary oxygen partial pressure so that oxygen moves to the capillaries and binds to the hemoglobin. Tissue partial pressure of oxygen is lower than that of the blood, so oxygen moves from hemoglobin to the tissue (Rosen & Manaker, 2024).
Image 3: Alveolar Gas Exchange
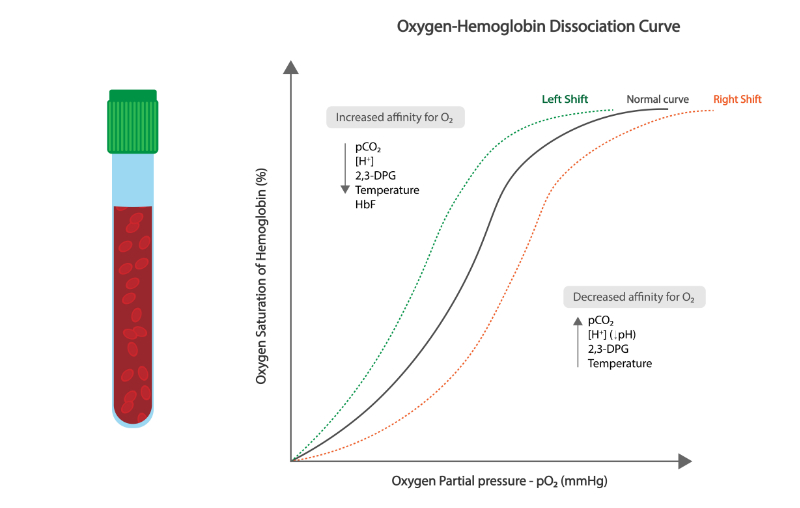
Numerous factors can affect the affinity of hemoglobin for oxygen. The relationship between the partial pressure of oxygen and hemoglobin is referred to as the oxyhemoglobin dissociation curve (Kaufman et al., 2023).
The following factors increase the affinity of hemoglobin for oxygen (Kaufman et al., 2023):
Hypocapnia
Alkalosis
Hypothermia
Decreased levels of 2, 3-diphosphoglycerate (2, 3 DPG)
These following factors have the opposite effect, that is, they decrease the affinity of hemoglobin for oxygen (Kaufman et al., 2023):
Hyperthermia
Acidosis
Hypercapnia
Increased 2, 3 DPG
This effect is referred to as the hemoglobin dissociation curve shifting to the right (Kaufman et al., 2023).
This characteristic of hemoglobin eases oxygen loading in the lungs and unloading into the surrounding tissue where the pH is lower and the PaCO2 is higher (Kaufman et al., 2023). Fetal hemoglobin, which has a higher affinity for oxygen than adult hemoglobin, is more fully oxygenated at lower PaO2 values (Kaufman et al., 2023). This high affinity is represented by a left shift on the dissociation curve of hemoglobin (Kaufman et al., 2023). Take a moment to review the following image to help illustrate the oxygen-hemoglobin dissociation curve.
Image 4: Oxygen-Hemoglobin Dissociation Curve
Once loaded with oxygen, the blood should reach the tissues to transfer oxygen to the cells (Kaufman et al., 2023). Oxygen delivery to the tissue depends on cardiac output (CO) and arterial oxygen content (CaO2): Oxygen delivery = CO x CaO2.
The key concept here is that more data than just PaO2 and SaO2 should be considered when assessing a patient's oxygenation status. The PaO2 and SaO2 may be normal, but if the hemoglobin concentration is low or cardiac output is decreased, oxygen delivery to the tissue will also be decreased (Fraser, n.d.).
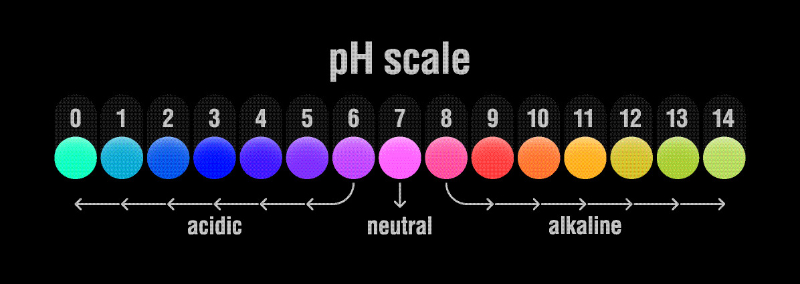
The pH scale is a mathematical expression of the acid-base balance of a solution. The number of hydrogen ions in a solution determines the acidity of that solution. An acid solution can donate hydrogen ions while a base solution can accept hydrogen ions. Blood pH is determined by the balance between acids, which results from the byproducts of metabolism, and the body's buffer systems. For example, if the carbon dioxide is not excreted effectively by the lungs, it combines with water to form carbonic acid, which leads to an excess of hydrogen ions and the development of acidemia in the blood.
There are multiple major blood buffers that exist to help neutralize the acid to maintain the acid-base balance, that is, to maintain equilibrium. The bicarbonate system is predominant among the three main buffers (Hopkins et al., 2022):
Bicarbonate
Hemoglobin
Serum protein
Bicarbonate combines with hydrogen to form carbon dioxide and water, buffering the acids and balancing the pH. If the lungs cannot excrete the carbon dioxide, the hydrogen ions can be returned to the solution, resulting in acidemia (Hopkins et al., 2022).
The lungs are primarily responsible for the carbon dioxide level (PaCO2), and the kidneys control the plasma bicarbonate (HCO3-) (Fraser, n.d.). Acting as an acid, carbon dioxide will add hydrogen ions, and bicarbonate acting as a base, accepts ions. As the PaCO2 rises or HCO3- falls, the pH will become more acidotic. As the CO2 falls or HCO3- rises, the pH will become more alkalotic (Fraser, n.d.).
PaCO2 is directly related to respiratory status. Therefore, abnormalities of pH resulting from abnormal PaCO2 are considered respiratory in origin.
Any abnormalities in HCO3- are considered metabolic in origin.
Base excess (BE) reflects the concentration of buffer. Normal range is 0 +/- 2 mEq/liter of base. Positive values express an excess of base or a deficit of acid while negative values express a deficit of base or an excess of acid. When the base excess is negative, it is sometimes called the base deficit (Simham, 2023).
The body attempts to maintain a normal pH in two main ways(Time of Care, n.d.):
By correcting or altering the factor responsible for the abnormality. For example, if an increased level of carbon dioxide in the blood is causing respiratory acidosis, the body will attempt to increase the excretion of carbon dioxide by the lungs and attempt to bring the causative factor, increased CO2, back to normal levels.
By compensating through alterations in the factor that is not primarily responsible for the abnormality, carbon dioxide or bicarbonate will be excreted or retained to attempt to balance the abnormal value. For example, if a high PaCO2 is causing respiratory acidosis, the body will attempt to excrete more acid and conserve HCO3- to compensate, although compensation by renal function is a slow mechanism and may take several days. If the PaCO2 is low, the body will rid itself of bicarbonate. The inverse is also seen. High HCO3- will be compensated by a high PaCO2, and a low HCO3- will be compensated by a low PaCO2. Thus, subsequent abnormal values of carbon dioxide or bicarbonate may result from the compensation mechanism of the body attempting to bring the ratio of HCO3- to CO2 back to 20:1.
Critically ill neonates may be limited in their ability to compensate for problems. Respiratory disease limits the body's ability to lower PaCO2 effectively, and the neonatal kidney may be ineffective in conserving bicarbonate properly.
The terms utilized when discussing acid-base disorders can be a source of confusion for many. Acidemia and alkalemia refer to measurements of blood pH specifically. And then, acidosis and alkalosis refer to the underlying pathologic process that is occurring in the body.
A blood pH of less than 7.35 is considered to be acidic or acidemic.
A blood pH of greater than 7.45 is considered to be alkalemic or alkalotic.
The partial pressure of carbon dioxide and bicarbonate levels determines the respiratory and metabolic contributions to the acid-base equation. For each disorder, compensatory mechanisms are indicated. Correction occurs whenever possible by addressing the underlying problem (Hopkins et al., 2022).
Respiratory acidosis is the result of the formation of excess carbonic acid because of increased carbon dioxide, generally due to hypoventilation, or when the body is breathing too slowly or shallowly, preventing the body from ridding itself of enough carbon dioxide and adequately bringing in enough oxygen (Emmett & Palmer, 2024).
Blood Gas Results: Low pH, High PCO2, Normal bicarbonate
Causes
Mechanism
Central nervous system (CNS) depression due to maternal narcotics during labor, asphyxia, severe intracranial bleeding, neuromuscular disorder, or CNS dysmaturity (apnea or prematurity)
Decreased Ventilation-Perfusion ratio
Obstructed airways, meconium aspiration, choanal atresia, bloody mucus, blocked endotracheal tube, or external compression of the airway
Decreased alveolar ventilation and decreased lung compliance
Respiratory alkalosis is the result of alveolar hyperventilation, or breathing too quickly or too deeply, forcing the body to rid itself of more carbon dioxide than the body can make, leading to a deficiency of carbonic acid (Hopkins et al., 2022).
Blood Gas Results: High pH, Low PCO2, and Normal bicarbonate
Causes
Mechanism
Iatrogenic (mechanical ventilation) Hypoxemia Central nervous system (CNS) irritation (stress or pain)
Compensated respiratory alkalosis is characterized by (Fraser, n.d.):
High normal pH
Decreased/low carbon dioxide
Decreased/low bicarbonate
These blood gas results are caused by the kidneys decreasing hydrogen secretion by retaining chloride and excreting fewer acid salts. Bicarbonate reabsorption is also decreased.
Metabolic acidosis is a deficiency in bicarbonate concentration in the extracellular fluid (Fraser, n.d.).
Metabolic acidosis is the result of any systemic disease that increases the production of acid, acid retention, or problems leading to excessive base losses. Examples of situations like these include hypoxia leading to lactic acid production, renal disease, and base loss because of diarrhea (Fraser, n.d.).
Blood Gas Results: Low pH, Low bicarbonate, Normal PCO2
If the patient is healthy, the lungs will blow off additional carbon dioxide through hyperventilation. If renal disease is not a problem, the kidneys should respond by increasing the excretion of acid salts and the reabsorption of bicarbonate.
Compensated metabolic acidosis is characterized by (Fraser, n.d.):
To best aid in your understanding of the typical results that will be obtained for infants in either respiratory or metabolic, acidosis or alkalosis, use the following chart to see the differences side by side:
The review and analysis of blood gases allows the healthcare professional to have the clinical proof for determining the adequacy of alveolar ventilation and perfusion (Fraser, n.d.). When this blood test is collected and evaluated, it is important to understand appropriate techniques and potential sources of error or universal precautions. It is known that all types of blood gas sampling carry some risk of transmission of infection to the infant by introducing organisms into the bloodstream. However, in addition, the risk of also exposing the healthcare professional to something contained within the infant's blood makes it necessary to always take appropriate precautions, as with any other form of blood or specimen collection (Fraser, n.d.).
Pertaining to bleeding disorders, the potential for the infant bruising and/or experiencing excessive bleeding should be evaluated, particularly if an arterial puncture is considered for specimen collection (Fraser, n.d.).
It is ideal if blood gases are able to measure the infant's current condition while it is in a state of equilibrium (Fraser, n.d.). Therefore, after making any change to the infant’s ventilator settings or disturbing the infant in any way, it is preferable to allow a period of 20 to 30 minutes of no stimulation before the arterial blood chemistry is obtained from the patient. This will allow for the infant’s acid-base status to reach a steady state (Fraser, n.d.). The length of this period will vary from infant to infant.
Arterial blood can be collected from either an invasive indwelling line or through a point-of-care peripheral arterial blood draw (Fraser, n.d.).
The choice of the specimen sample site will depend on the clinical situation. An indwelling arterial catheter line (art line or A-line) should be placed or at least considered when it is anticipated that the neonate will require more frequent arterial blood gases.
There are also several other factors that are considered to determine the need for an indwelling A-line (Fraser, n.d.). These criteria can include (Fraser, n.d.):
Gestational age
Disease process
Amount of oxygen the patient requires
For neonates, the common sites for indwelling arterial lines include (Fraser, n.d.):
Capillary blood can be "arterialized" by warming the skin to increase local blood flow. Blood specimens can best be obtained from the outer aspects of the heel (Fraser, n.d.).
When perfusion is normal, it has been shown that capillary pH and PCO2 correlate well and are in line with arterial values. The PO2 level correlates if the partial pressure of oxygen is < 60 in arterial blood, but not at higher levels (Fraser, n.d.).
The review and interpretation of blood gas results should follow a logical pattern.
First, evaluate the pH to determine if acidemia or alkalemia is present.
Then, take a look at the respiratory parameter, PaCO2, and the metabolic parameter, HCO3-, to determine if the acidemia or alkalemia is respiratory or metabolic in origin.
The clinical picture can become complex if abnormalities exist in both systems simultaneously. A review of the infant's clinical status, previous blood gas values, and treatment measures will help determine whether this is an ongoing compensation mechanism or two independent abnormalities.
As has been discussed, the arterial blood gas results provide information about the pulmonary component of oxygenation, more specifically the PaO2(Fraser, n.d.). Hypoxemia exists when an arterial PaO2 is lower than normal. Whereas hypoxia exists when the oxygen supply to the body tissues is inadequate (Fraser, n.d.). It is acceptable for preterm infants to have a lower PaO2 value because fetal hemoglobin has a higher affinity for oxygen than adult hemoglobin does and, therefore, the presence of fetal hemoglobin results in increased oxygen delivery at lower PaO2(Fraser, n.d.).
Hypoxemia also can result from lung disease or cyanotic congenital heart disease (CHD) (Fraser, n.d.). Hypoxia can also result from a number of factors, including anemia, heart failure, a decreased PaO2, and an abnormal hemoglobin affinity for oxygen (Fraser, n.d.). However, the most common cause of hypoxemia is the mismatching of ventilation and perfusion. This mismatching occurs when the amount of blood perfusing an alveolus or when fresh gas entering the alveolus is not adequate enough for gas exchange. As is a normal occurrence in the lungs, some alveoli are also just simply better ventilated than others. Clinically significant mismatching will occur when decreased ventilation or perfusion interferes with the ability of the lung to provide adequate gas exchange (Fraser, n.d.). PaO2 of less than 45 to 50 mmHg is associated with dilation of the ductus arteriosus and constriction of pulmonary vasculature. Low PaO2s can be implicated in the cause of persistent pulmonary hypertension in the newborn (PPHN) (Fraser, n.d.).
Hyperoxemia, or a PaO2 of > 100 mmHg, should also be prevented, especially in the preterm infant, where high oxygen levels in the blood can be associated with causing retinal injury, primarily retinopathy (Türksever et al., 2021). When interpreting neonatal PaO2s, it is important to note whether the specimen is pre-ductal or post-ductal in its origin because of the likely impact of shunting across the ductus resulting in lower PaO2 in post-ductal specimens (Fraser, n.d.).
Acid-base imbalances are corrected where possible by targeting and intervening in the system that is causing the primary problem. This is done in the following issue-specific ways (Fraser, n.d.):
In the case of respiratory acidosis, we can assist the body in removing carbon dioxide through the application of nasal continuous positive airway pressure (CPAP) or mechanical ventilation (Fraser, n.d.). For infants who are already on mechanical ventilation, carbon dioxide removal can be facilitated by increasing the rate, peak inspiratory pressure (PIP), or positive end-expiratory pressure (PEEP). Sodium bicarbonate is usually not recommended for treating respiratory acidosis because it can react with acids to form carbon dioxide, which would worsen the problem (Fraser, n.d.).
In the case of respiratory alkalosis, if an infant is being mechanically ventilated, we can reduce the rate of pressure on the ventilator to work to correct this (Fraser, n.d.).
For infants with metabolic acidosis, where possible, we need to treat the cause of the acidosis (Fraser, n.d.). If the case of acidosis is critical, sodium bicarbonate can be administered at a dose of 2 mEq/kg or according to the following formula (Fraser, n.d.):
Base deficit x (weight in kg) x (0.3) = Dose of sodium bicarbonate
The dose of bicarbonate that is calculated from this formula should, ideally, be able to correct half of the base deficit (Fraser, n.d.). This dose needs to be administered slowly over 30 to 60 minutes (Fraser, n.d.). Fluid replacement may also be beneficial for treating metabolic acidosis because it can help the infant metabolize the lactic acid (Fraser, n.d.).
In infants in metabolic alkalosis, we need to target the cause of the alkalosis by making sure that acetate is removed from intravenous (IV) fluids, reducing the dose of diuretics, and treating hypokalemia (low potassium), hyponatremia (low sodium), and hypochloremia (low chloride) (Fraser, n.d.).
Compensation occurs in response to the primary disturbance in the acid-base equilibrium whereby the change in the pH is relieved (Emmett & Palmer, 2024). Compensation is a change in the system not originally affected by the primary disturbance.
Correction is a change in the system originally affected by the primary disturbance, using available therapy by the healthcare professional (Emmett & Palmer, 2024).
The retention of bicarbonate characterizes compensated respiratory acidosis due to the adjustment in renal function. The primary disturbance is the accumulation of carbon dioxide, thus increasing carbonic acid concentration. The kidneys respond to this disturbance by holding on to the HCO3. This compensation by the kidneys can take several days if not corrected by ventilation therapy. When fully compensated, the pH is near normal and PaCO2 values and HCO3 are increased (Emmett & Palmer, 2024).
Compensated metabolic acidosis is characterized by hyperventilation activated by the primary disturbance of an accumulation of acid that devours the available base. The CO2 that is excreted through the lungs lowers the carbonic acid concentration to match the lower available bicarbonate. When fully compensated, the pH is near normal, and the PaCO2 and serum HCO3 values are low (Emmett & Palmer, 2024).
Compensated respiratory alkalosis is characterized by the kidneys increasing their bicarbonate secretion to restore the bicarbonate/carbonic acid ratio to normal. The primary disturbance is caused by hyperventilation and excessive elimination of CO2. The pH is near normal when fully compensated, but PaCO2 and serum HCO3 are at the lower end of normal (Emmett & Palmer, 2024).
Compensated metabolic alkalosis is characterized by hypoventilation to diminish the elimination of CO2. The primary disturbance is the accumulation of bicarbonate. By retaining CO2, the appropriate reaction between sodium bicarbonate and carbonic acid is restored. The pH is almost normal when compensated, but the PaCO2 and serum bicarbonate values are elevated (Time of Care, n.d.).
Use the following table to help organize your thoughts about blood gas results in these situations and what can be done to correct the respective acid-base imbalance.
Disorder
pH
Primary Component Affected
Compensatory Effect
Correction
Metabolic Acidosis
pH < 7.35
Decreased HCO3
Decreased PCO2
Give bicarbonate and treat the cause
Respiratory Acidosis
pH < 7.35
Increased PCO2
Increase HCO3
Increase or assist ventilation
Metabolic Alkalosis
pH > 7.45
Increased HCO3
Increased PCO2
Give KCl Stop diuretics Treat cause
Respiratory Alkalosis
pH > 7.45
Decreased PCO2
Decreased HCO3
Attempt to stop hyperventilation
The correction of acidosis-alkalosis can be achieved sooner if one manipulates ventilator settings or administers bicarbonate to achieve the desired value.
If the pressure or rate on the ventilator is increased, CO2 will be blown off.
If the rate or pressure is decreased, CO2 will be retained.
Severe metabolic acidosis may be treated with sodium bicarbonate, unless the PCO2 is elevated, as the pH will not change (Safer Care Victoria, 2019). However, sodium bicarbonate is not generally recommended because most newborn issues are caused by respiratory failure. Ventilation and fluid resuscitation are the first lines of treatment (Ralston, 2024).
For acute correction of HCO3 base deficit: Hypoxemia that is secondary to ventilator perfusion mismatching can be improved by providing supplemental oxygen to the patient. Furthermore, oxygenation can be improved by increasing the mean airway pressure (MAP) in an infant receiving mechanical ventilation (Fraser, n.d.).
Additional ventilator settings can be altered to correct acid-base imbalances. We will take a look at these in table form. First, make sure to keep in mind for the following table that (Nagler & Cheifetz, 2023):
FiO2= Fraction of inspired oxygen (the percentage of oxygen that is inhaled)
PEEP= Positive end expiratory pressure (pressure left in the lungs after exhalation to prevent the alveoli from collapsing completely)
PIP= Peak inspiratory pressure (the max pressure applied to the lungs during inspiration)
Now, review the following table to determine the ventilator tweaks and changes that can be made in order to help correct a clinical problem identified via blood gas results (Nagler & Cheifetz, 2023).
Ventilator Corrections
Blood Gas Imbalance
Ventilator Changes
Hypoxemia (low PaO2)
Increase FiO2 Increase PEEP Increase PIP
Hyperoxia (high PaO2)
Decrease FiO2 Decrease PEEP
Hypercapnia (high PaCO2)
Increase respiratory rate Increase PIP Increase inspiratory time Increase the flow rate Decrease dead space
Hypocapnia (low PaCO2)
Decrease respiratory rate Decrease PIP Decrease inspiratory time Decrease flow rate Increase dead space
Now that we have reviewed all the main components that should be reviewed when obtaining a blood gas, let’s take some time to practice what we have learned.
For our first practice scenario, this 36-week gestational age male infant is on room air.
His blood gas results are as follows:
pH = 7.22 mmHg
PaCO2 = 61 mmHg
PaO2 = 70 mmHg
HCO3- = 24 mEq/L
So, his pH is lower than normal, therefore, it would be labeled acidotic. The PaCO2 is higher than normal, therefore, it would be labeled acidotic. The PaO2 is within the normal range. Is the patient working (using additional respiratory effort) to maintain the PaO2? The HCO3- is within the normal range.
It is obvious that the patient is suffering from acidosis, however, is it respiratory or metabolic? Is it compensated or uncompensated?
Because the HCO3- is normal, it is not metabolic, but respiratory in nature. The blood gas is uncompensated because the pH is not within the normal range. Therefore, this is uncompensated respiratory acidosis. For this patient, we need to consider starting him on CPAP to help correct this.
This 33-week gestational age female infant is receiving mechanical ventilation.
Her current ventilator settings are as follows:
Rate: 25
PIP: 18
PEEP: +4
FiO2: 30%
Her blood gas results are as follows:
pH = 7.49 mmHg
PaCO2 = 26 mmHg
PaO2 = 95 mmHg
HCO3- = 22 mEq/L
Her pH is high, indicating alkalemia. The PaCO2 is low, indicating a respiratory alkalosis. The HCO3 - is normal. There is no compensation because pH is not normal.
PaO2 is also too high.
These results tell us that this is a case of uncompensated respiratory alkalosis. At this point, we need to consider reducing the rate or PIP on the ventilator and weaning oxygen.
This 30-week gestational age female infant is on room air. She was just found to have necrotizing enterocolitis, and she is on continuous gastric suction, total parental nutrition (TPN) with sodium, as well as potassium acetate.
Her capillary blood gas results are as follows:
pH = 7.52 mmHg
PCO2 = 41 mmHg
PO2 = 55 mmHg
HCO3- = 35 mEq/L
Let’s see. So, the pH is high, indicating alkalemia. The PCO2 is high normal. The metabolic component is high, indicating metabolic acidosis. There is no compensation because the pH is not normal. The PO2 is adequate (remember this is a capillary blood gas specimen).
These results tell us that this is a case of uncompensated metabolic alkalosis. For this infant, we must consider eliminating the acetate in the TPN and using chloride salts.
In this next scenario, a premature infant is receiving TPN with adequate calories, but they continue to have weight loss.
When the capillary blood gas is collected, capillary refill is noted as being sluggish. His blood gas results are as follows:
pH = 7.27 mmHg
PCO2 = 36 mmHg
PO2 = 57 mmHg
HCO3- = 15 mEq/L
The pH is low, indicating an acidosis. The PCO2 is normal. The metabolic component is low, indicating a metabolic problem. There is no compensation because the pH is not normal. The PO2 is adequate (capillary blood gas).
These results tell us that this is uncompensated metabolic acidosis. In this scenario, we would need to consider giving volume to help metabolize lactic acid and adding acetates to lower metabolic acid load.
In this final practice scenario, a premature male infant is on mechanical ventilation for respiratory distress.
His current ventilator settings are as follows:
Rate: 30
PIP: 19
PEEP: +5
FiO2: 40%
The infant has lost weight and has a serum sodium of 148 mEq/L.
His blood gas results are as follows:
pH = 7.28
PaCO2 = 49 mmHg
PaO2 = 56 mmHg
HCO3- = 18 mEq/L
When reviewing these results, the pH is low, indicating an acidemia. The PaCO2 is high, indicating respiratory acidosis. The metabolic component is low, indicating a metabolic problem. There is no compensation because the pH is not normal. The PaO2 is adequate.
These results tell us that this is uncompensated mixed respiratory and metabolic acidosis. In this case, we must increase the ventilator rate. We must also consider administering extra volume to correct the hypovolemia, which may be causing the metabolic acidosis.
Now, let’s take a moment to apply what we have learned in this course and in the above practice scenarios for this final case study.
An infant, Jack, who was born at 31-weeks’ gestation is two hours old with the following physical findings:
Respiratory rate: 94 bpm
Heart rate: 162 bpm
Temperature 36.5°C (97.7°F)
Grunting with moderate retractions
His capillary blood gas results are as follows:
pH = 7.30
PCO2 = 56 mmHg
HCO3- = 26 mEq/L
PO2 = 40 mmHg
Using the steps for analysis of this blood gas, we can decide the following:
The pH is low, indicating acidosis.
The PCO2 is high, indicating a respiratory problem.
The metabolic component (HCO3-) is normal.
There is no compensation present (pH is not normal).
This is uncompensated respiratory acidosis.
Oxygenation is adequate.
Treatment for Jack should be aimed at improving his alveolar ventilation. Depending on the infant's clinical status and chest X-ray findings, treatment could consist of nasal CPAP or intermittent positive pressure ventilation.
Acid-base balance disorders are diagnosed almost as frequently as blood gas sampling is undertaken in the neonatal population. Sick neonates have respiratory and metabolic systems that constantly change in response to disease processes and therapeutic interventions. Quick responses to these changes will minimize the time an infant spends outside the desired range of blood pH and potential complications of treatments such as airway pressure (barotraumas) and oxygen.
Arterial blood gas collection allows for the assessment of oxygenation. Capillary blood samples are useful for evaluating CO2 removal and acid-base status but are not useful for evaluating oxygenation. It is imperative to systematically approach blood gas interpretation and incorporate knowledge of physical physiology with the clinical history to provide optimal patient care and to improve patient outcomes. Monitoring a sick infant with a pulse oximeter provides continuous oxygen saturation information. Intermittent review of arterial blood gases will also yield specific, valuable information on the acid-base balance on an as-needed basis.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Arias-Oliveras, A. (2016). Neonatal blood gas interpretation. Newborn and Infant Nursing Reviews, 16(3), 119-121. Visit Source.
Emmett, M., & Palmer, B.F. (2024). Simple and mixed acid-base disorders. UpToDate. Retrieved February 29, 2024. Visit Source.
Fraser, D. (n.d.) 6 Blood gas analysis. Academy of Neonatal Nursing (ANN). Visit Source.
Hopkins, E., Sanvictores, T., & Sharma, S. (2022). Physiology, acid base balance. In StatPearls. StatPearls Publishing. Visit Source.
Kaufman, D. P., Kandle, P. F., Murray, I. V., & Dhamoon, A. S. (2023). Physiology, oxyhemoglobin dissociation curve. In StatPearls. StatPearls Publishing. Visit Source.
Nagler, J., & Cheifetz, I.M. (2023). Initiating mechanical ventilation in children. UpToDate. Retrieved February 29, 2024. Visit Source.
Ralston, M.E. (2024). Primary drugs in pediatric resuscitation. UpToDate. Retrieved February 29, 2024. Visit Source.
Rosen, I.M. & Manaker, S. (2024). Oxygen delivery and consumption. UpToDate. Retrieved February 28, 2024. Visit Source.
Safer Care Victoria. (2019). Blood gas interpretation for neonates. Safer Care Victoria. Visit Source.
Simham, H.N. (2024). Umbilical cord blood acid-base analysis at delivery. UpToDate. Retrieved February 29, 2024. Visit Source.
Time of Care. (n.d.) Compensation for acid-base disorders (Equations, etc.). Time of Care Online Medicine Notebook. Visit Source.
Türksever, C., López Torres, L. T., Valmaggia, C., & Todorova, M. G. (2021). Retinal oxygenation in inherited diseases of the retina. Genes, 12(2), 272. Visit Source.
Wajs, W., Kruczek, P., Szymański, P., Bukowczan, M., Wais, P., & Ochab, M. (2018). Newborn arterial blood gas prediction. IEEE, 1-4. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.