This course will be updated or discontinued on or before Thursday, November 5, 2026
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
CEUFast, Inc. is an AOTA Provider of professional development, Course approval ID#02040. This distant learning-independent format is offered at 0.2 CEUs Intermediate, Categories: OT Service Delivery and Foundational Knowledge.
AOTA does not endorse specific course content, products, or clinical procedures. AOTA provider number 9757.
CEUFast, Inc. (BOC AP#: P10067) is approved by the Board of Certification, Inc. to provide education to Athletic Trainers (ATs).
FPTA Approval: CE25-395565, CE26-395565. Accreditation of this course does not necessarily imply the FPTA supports the views of the presenter or the sponsors.
CEUFast, Inc. is recognized by the New York State Education Department's State Board for Physical Therapy as an approved provider of physical therapy and physical therapist assistant continuing education.
Outcomes
≥ 92% of participants will know risk factors and common causes of traumatic brain injury and identify clinical characteristics, complications, and treatment options associated with TBI.
Objectives
After completing this course, the learner will be able to:
List three common causes of traumatic brain injury (TBI).
Identify three risk factors for TBI.
Outline the clinical characteristics of a TBI.
Relate three medical complications associated with TBI.
Identify two diagnostic tests for TBI patients.
Summarize treatment options in the care of TBI patients.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Traumatic brain injury (TBI) is a major cause of death and disability. Annually, in the United States, there are 214,110 TBI-related hospitalizations, 69,473 TBI-related deaths (Centers for Disease Control [CDC], 2024), and 1.74 million people need at least one day off of work after a TBI (Dawodu, 2023). It is estimated that 2.5 to 6.5 million Americans are living with a disability from TBI, and it is the leading cause of long-term disability in children and young adults worldwide (Dawodu, 2023).
TBI is a sudden trauma that damages the brain. Damage is either focal, in one area, or diffuse. When the head hits an object, and the skull does not break, the injury is considered a closed head injury. When the skull breaks and the object penetrates brain tissue, the injury is considered a penetrating injury. Most TBIs are mild. Repeated TBIs can lead to multiple problems, such as cumulative cognitive or neurological deterioration.
According to the CDC, TBIs can result from various causes, with leading contributors including falls, motor vehicle crashes, being struck by or against objects, and intentional self-harm (CDC, 2024; CDC, n.d.).
Falls are the most common cause of TBI, accounting for nearly half of all cases. The CDC (2024) reports that falls are particularly prevalent among the very young (children aged 0-4 years) and the elderly (adults aged 65 and older). The susceptibility of these age groups to falls is due to factors such as developmental stages in children and balance, vision, and mobility issues in older adults. Falls can result in a range of TBIs, from mild concussions to severe brain injuries that require extensive medical intervention.
Motor vehicle crashes are the second leading cause of TBI (CDC, 2024; CDC, n.d.). These incidents involve collisions between cars, motorcycles, bicycles, or pedestrians and are particularly common among young adults aged 15-24. The forces involved in vehicular accidents can cause significant brain injuries due to rapid acceleration or deceleration, which can result in the brain impacting the interior of the skull. The severity of TBIs from motor vehicle accidents can vary widely, often necessitating emergency medical care and long-term rehabilitation.
Being struck by or against an object represents the third major cause of TBI (CDC, 2024). This category includes sports injuries, workplace accidents, and other scenarios where the individual collides with an obstacle. Sports-related TBIs are a significant concern, particularly in contact sports like football, hockey, and boxing, where athletes are at high risk for concussions. Protective equipment and proper safety protocols are critical to mitigate these risks.
Intentional self-harm, including attempted suicides, is also a notable cause of TBI. Firearm-related injuries are a major contributor to TBIs in this category.TBIs resulting from self-harm are often severe and carry a high fatality rate. Mental health issues play a critical role in these cases, and addressing these underlying problems is essential for prevention.
Other less common causes of TBI include assaults and combat injuries among military personnel. Assault-related TBIs often result from violent attacks and are more prevalent in certain demographic groups, including young adults and men. Combat-related TBIs, also known as blast injuries, are a significant issue for military service members exposed to explosions and other combat-related incidents. Early detection, appropriate medical response, and rehabilitation are important in managing TBIs from these causes.
Gender also plays a role in TBI risk. Males are significantly more likely to sustain a TBI than females. According to the CDC, males are 3.4 times more likely to suffer a TBI (Dawodu, 2023). This disparity is attributed to a higher likelihood of males engaging in high-risk activities such as contact sports, dangerous occupations, and driving at higher speeds. Additionally, males are more likely to be involved in violent encounters, which can lead to TBIs from assaults.
Age is a significant risk factor for TBI. The CDC reports that the incidence of TBI is highest among children aged 0-4 years, adolescents aged 15-24 years, and adults aged 65 and older. Young children are at risk due to their developing motor skills and propensity for falls. In contrast, adolescents and young adults are more likely to engage in high-risk behaviors and activities such as contact sports and driving. Older adults are at higher risk due to decreased balance, vision, bone density, and mobility issues, making them more susceptible to falls(CDC, 2024; Dawodu, 2023).
Other risk factors for TBI include (CDC, 2024; Dawodu, 2023):
A concussion is a form of traumatic brain injury (TBI) resulting from a blow to the head or body, causing the brain to move rapidly within the skull. This movement can lead to chemical changes in the brain and damage brain cells. Common causes of concussion include falls, sports injuries, motor vehicle accidents, and violent incidents. Annually, in the United States, a concussion occurs an estimated 1.4 to 3.8 million times (Ferry & DeCastro, 2024). As many as 50 percent of concussions are unreported (Ferry & DeCastro, 2024).
A concussion is caused by a blow to the head or body, leading to an impulsive force transmitted to the head. It leads to a rapid onset of short-lived impairment of the neurological function and typically resolves on its own. It typically leads to a functional disturbance but not necessarily a structural one and neuroimaging tests are typically normal.
Acute symptoms of concussion include amnesia, confusion, and loss of consciousness. Amnesia usually involves an inability to recall the traumatic event but may also include the inability to remember events before or after the injury. The athlete may also complain of headaches, dizziness, nausea/vomiting, tinnitus, balance impairment, or photophobia. The athlete may not be able to report game details, appear dazed, feel foggy/hazy/sluggish, or be stunned. The athlete may ask the same question repeatedly, even though it has been answered.
Many people will experience headaches after mild TBI. Most commonly, headaches occur within seven days of the traumatic brain injury, but headaches may persist. A small percentage of individuals, some estimate up to 15 percent, have symptoms beyond one year (Permenter et al., 2023). Individuals with a history of headaches are at increased risk for developing a post-traumatic headache (Dwyer, 2018).
After a concussion, the physical exam may show memory problems, slurred speech, a vacant stare, confusion, incoordination, emotional fluctuation, slow answers to questions, and easy distraction.
Athletes who experience any signs and symptoms after a bump, blow, or jolt to the head or body should not participate in sports until a healthcare professional experienced in concussion management clears the patient.
Multiple tests can be used on the field to assess the athlete for a concussion (Graham et al., 2014). The Standardized Assessment of Concussion (SAC) assesses orientation, immediate memory, concentration, delayed recall, neurologic screening, and exertion maneuvers. This test works best when there is a baseline measure and should not be used in isolation to determine if the athlete should go back to play. The SAC is, in fact, just a portion of the Sports Concussion Assessment Tool-6 (SCAT6), and the SAC should not be used as a stand-alone tool.
The Sport Concussion Assessment Tool-6 (SCAT6), a more involved test than the SAC, is used to evaluate an injured athlete on the sideline (Patricios et al., 2022). This test works best when there is a baseline evaluation to determine the degree of impairment after an injury. The test is associated with significant variability among high school students. Because of the test variability (especially balance scores and concentration), it should be used cautiously without a baseline measure. Many schools and organized teams will perform baseline testing at specific intervals for all athletes participating in sports.
Post-concussion syndrome is a combination of symptoms (headache, irritability, concentration impairment, dizziness, fatigue, insomnia, alcohol intolerance, memory impairments, or intellectual difficulties) that occur after a head injury. During this time, it is critical to maintain relative cognitive and physical rest. Evidence shows that strict rest until complete symptom resolution is not beneficial (Patricios et al., 2022). Relative rest is indicated immediately post-injury up to two days after injury. During this time, gentle activities of daily living and reduced screen time are indicated (Patricios et al., 2022). If rest is not maintained, recovery can be prolonged. Symptoms typically resolve in one week to 10 days but may persist for months.
Cerebral perfusion pressure is the blood pressure less the intracranial pressure (ICP) and should be above 70 mmHg in adults and 60 mmHg in children. The pressure on the brain is critical. If the pressure gets too low, below 12ml/mg/min, irreversible brain damage may occur (Tolias, 2021). Autoregulation helps maintain adequate cerebral blood flow. Autoregulation does not work when a traumatic event and cerebral blood flow are decreased. Maintaining adequate blood pressure during a TBI is critical.
Inside the skull is a closed space, and the pressure in the cavity is constant. On average, the adult has an intracranial volume of about 1500 mL. The brain makes up about 85-90% of the volume. The intravascular cerebral blood volume consumes about 10% of the volume, and cerebrospinal fluid (CFS) accounts for less than three percent of the volume (Ainsworth, 2024). Any alteration in one of the components will result in an alteration of the other. When ICP increases, the brain may herniate; this is when part of the brain is pushed through a natural opening.
The CSF acts as a shock absorber for compressive forces. Specific brain areas are more prone to trauma due to rough spots in the skull located in the frontal lobe floor and the top and floor of the temporal lobes.
A stationary head is most likely damaged at the point of impact. When the head is in motion, the injury most commonly occurs on the opposite side of the trauma because the brain lags slightly behind the body falling, and the brain bounces off the other side of the skull (Ainsworth, 2024).
TBI can be primary or secondary. Primary injuries occur at the moment of the injury due to mechanical forces (Pangilinan, 2024). They can occur when the object strikes the head or the brain hits inside the skull due to acceleration-deceleration forces, blast waves, or penetrating injuries (Ainsworth, 2024).
Secondary injury occurs sometime after the trauma and often leads to long-term problems. It often compounds the primary injury. Swelling, bleeding, and increased ICP may result in decreased blood flow to the brain, which leads to cell death. Secondary injury may be noted clinically by low blood pressure, hyperthermia, hypoxia, intracranial hemorrhage, or malignant brain edema(Dawodu, 2023).
A contusion is bruising of the brain and occurs in two ways:
Direct trauma
Acceleration/deceleration injury
Direct trauma causes injury at the site of impact, termed a coup contusion. Acceleration/deceleration causes injury at a site opposite the impact site, termed a contrecoup contusion. Contrecoup typically results in a bruised brain when the brain bounces off the skull and often occurs in shaken baby syndrome or a car accident. It can cause damage to individual nerve cells.
Skull fractures occur when there is a break in the integrity of the skull bone. The most common type of skull fracture is a linear skull fracture, with a break in a cranial bone resembling a thin line without splintering, depression, or distortion of bone. Typically, these fractures are not serious and do not require specific treatment unless there is an underlying brain injury. When the skull pushes into the brain, it is called a depressed skull fracture. When an object penetrates the skull, a penetrating skull fracture occurs. A basilar skull fracture is a fracture at the base of the skull, which often results in bruising around the eyes (raccoon eyes) or behind the ears (Battle's sign) and may involve leakage of cerebrospinal fluid (CSF) from the nose or ears. This fracture is serious and requires careful monitoring and management to prevent complications like infection. A comminuted skull fracture occurs when the bone is broken into three or more pieces. They can be complex and require surgical treatment to ensure proper healing and alignment.
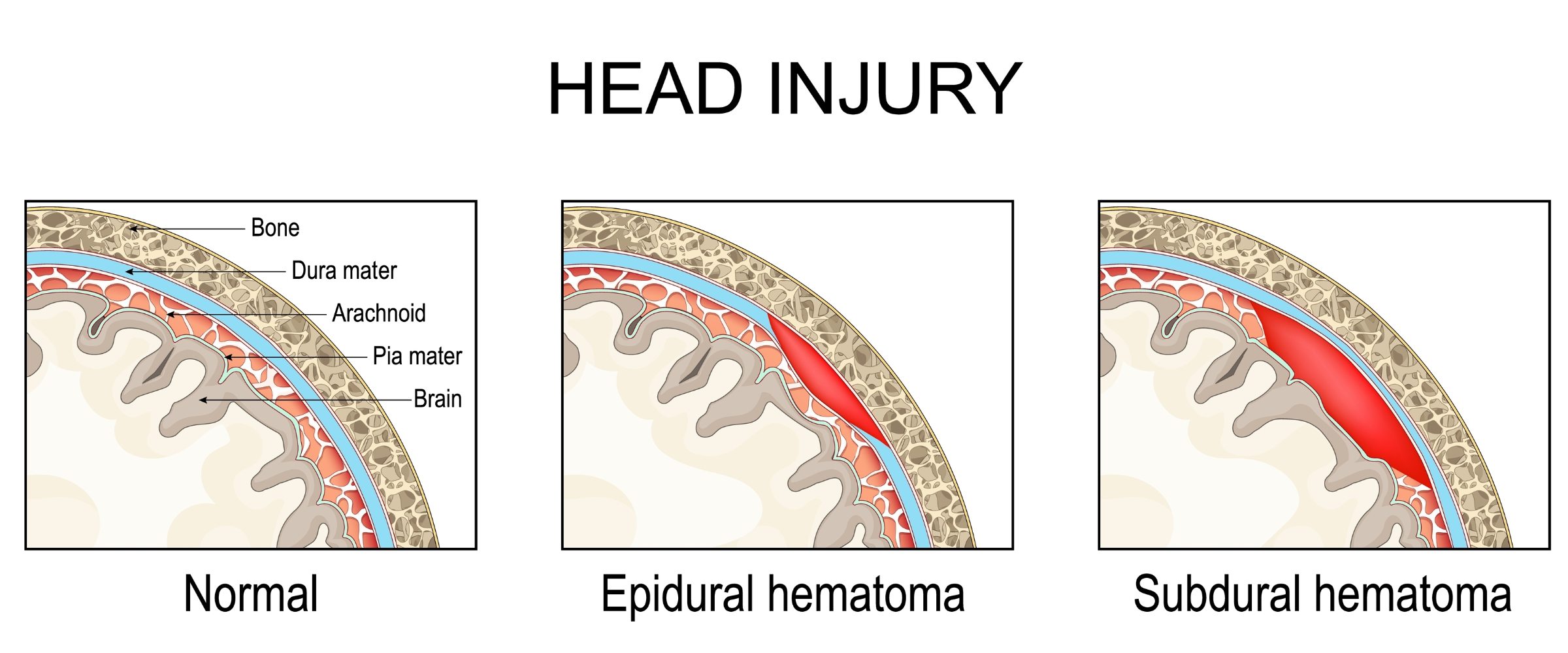
An intracranial hematoma is bleeding into or around the brain and is a common injury seen in TBI. A hematoma is TBI's most common cause of death (Ainsworth, 2024). A hematoma should be considered when there is neurological deterioration, such as worsening headache, confusion, lethargy, focal neurological signs, or loss of consciousness.
Multiple types of intracranial hematomas can occur, including subdural, epidural, and intracerebral hematomas. A subdural hematoma (SDH) occurs between the dura and arachnoid matter. It usually results from the tearing of bridging veins due to head trauma. It can be acute (symptoms appear quickly), subacute (symptoms appear over days), or chronic (symptoms develop over weeks to months).
An epidural hematoma is bleeding between the skull and the dura and is often caused by a break in the temporal bone and rupture of the middle meningeal artery. This type of hematoma can grow rapidly because the bleeding comes from a high-pressure artery and can quickly elevate the pressure in the brain. An intracerebral hematoma is bleeding into the brain.
Intracranial Hematomas
*Please click on the image above to enlarge.
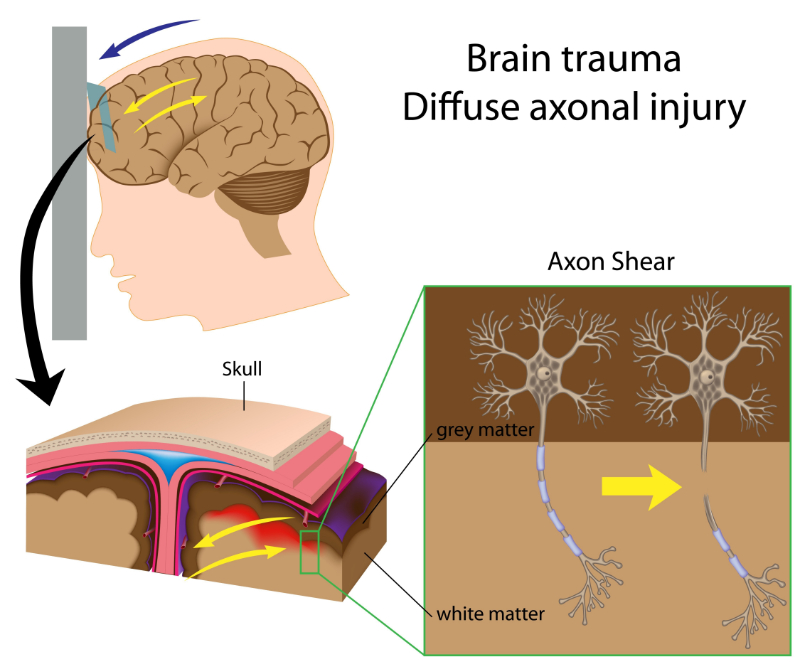
Diffuse axonal injury (DAI) is a type of traumatic brain injury (TBI) that occurs when the brain rapidly shifts inside the skull as an injury occurs, leading to widespread tearing (shearing) of axons, the long fibers that connect nerve cells (Pangilinan, 2024). This injury disrupts the brain's normal communication pathways and can cause significant neurological deficits. It results from damage on a microscopic level and, therefore, is not seen in imaging studies. An MRI is more sensitive than CT for detecting DAI, and specific sequences, like Diffusion Tensor Imaging (DTI), can reveal axonal damage.
The clinical presentation of TBI can vary widely depending on the severity of the injury, the specific areas of the brain affected, and the individual's overall health. TBI is generally classified into mild, moderate, and severe categories, each with distinct clinical features.
Mild traumatic brain injury presents with subtle symptoms that may not appear immediately. They can include headache, dizziness, nausea or vomiting, fatigue, blurred vision, sensitivity to light or noise, balance problems, confusion, memory problems, difficulty concentrating, feeling mentally "foggy," irritability, mood swings, anxiety, depression, and sleep disturbances. Mild TBI may present with a brief loss of consciousness (less than 30 minutes) or no loss of consciousness, a Glasgow Coma Scale (GCS) score of 13-15 (see Table 1), and possibly a brief period of post-traumatic amnesia (less than 24 hours).
Moderate TBI presents with symptoms that are more pronounced and persistent than in mild TBI. They may include persistent headache, repeated vomiting or nausea, convulsions or seizures, dilation of one or both pupils, clear fluids draining from the nose or ears, inability to awaken from sleep, weakness or numbness in extremities, loss of coordination, significant confusion, slurred speech, difficulty with thinking and memory, increased agitation, combativeness, or unusual behavior. In moderate TBI, loss of consciousness lasts from 30 minutes to 24 hours, with a GCS score of 9-12 and post-traumatic amnesia lasting from 24 hours to 7 days.
Severe TBI symptoms are severe and potentially life-threatening. Symptoms include prolonged unconsciousness (coma), persistent or worsening headache, repeated vomiting or nausea, seizures, dilation of one or both pupils, clear fluid draining from the nose or ears, inability to awaken from sleep, significant motor deficits (e.g., weakness or paralysis), profound confusion, significant memory loss, inability to speak coherently, profound personality changes, increased agitation or aggression, severe mood disturbances. Loss of consciousness lasts more than 24 hours, with a GCS score of 8 or below and post-traumatic amnesia lasting more than seven days.
Table 1: Glasgow Coma Scale
Assessment of the Glascow Coma Scale (GSC) is a way to measure the impact on brain function. This test is rated from one to 15. It assesses eye-opening, verbal responses, and motor responses. GCS can be used to describe the severity of the TBI.
EYE RESPONSE
4
Spontaneously opens the eyes.
3
Opens eyes with verbal commands
2
Opens eyes only in response to painful stimulus
1
Unable to open eyes
VERBAL RESPONSE
5
The patient is oriented and speaks coherently
4
Disoriented but can speak coherently
3
Inappropriate language
2
Makes incomprehensible sounds
1
No verbal response
MOTOR RESPONSE
6
Moves arms and legs in response to verbal commands
5
Able to localize pain
4
Withdrawal from painful stimulus (normal flexion)
3
Abnormal flexion (decorticate)
2
Abnormal extension (decerebrate)
1
No movement to any stimulus
The scores given to each section are added up, and the severity of the head trauma is determined based on the total score.
3-8
Severe head injury
9-12
Moderate head injury
13-15
Mild head injury
Children with head injuries may present with persistent crying, irritability, refusal to eat, abnormal sleeping patterns, tiredness, listlessness, inconsolable, changed behavior or playing patterns, reduced performance in school, regression of development, emesis, or incoordination.
Some symptoms persist long into the recovery period. Six months after mild TBI, some patients will report weakness, fatigue, memory problems, dizziness, and headache. Eighty-three percent of patients with mild TBI report at least one symptom after six months (Ainsworth, 2024).
When evaluating a head injury, it is important to evaluate for other injuries such as neck injury, spinal cord injury, facial fracture, eye injury, or skull fracture.
Post-traumatic seizures (PTS), generalized or partial, are a common complication of head trauma. Seizures are more common with moderate to severe TBIs (brain contusions, hematomas, or penetrating head injuries) than mild TBIs.
Seizures are classified as immediate, early, or late (Anwer et al., 2021). Immediate seizures occur within the first 24 hours post-injury and are often considered a direct response to the initial trauma. They are usually not predictive of the development of epilepsy.
Early seizures occur within the first week post-injury and may indicate a higher risk for developing post-traumatic epilepsy (PTE), especially if recurrent. Late seizures occur more than one week post-injury and are strongly associated with the development of PTE. Late seizures can occur months to years after the initial injury.
The risk factors for early PTS include (Evans & Schachter, 2024; Fordington & Manford, 2020; Younus et al., 2018):
GCS score of ≤ 10
Immediate seizures
Post-traumatic amnesia lasting longer than 30 min
Linear or depressed skull fracture
Penetrating head injury
Subdural, epidural, or intracerebral hematoma
Young age
Chronic alcoholism
Those with early seizures are at higher risk of developing post-traumatic epilepsy (PTE). PTE is defined as recurrent seizures >7 days following an injury. Reducing PTS should be a clinical goal to avoid PTE and decrease the associated morbidity and mortality rate. The incidence of PTE is estimated to be 1.1% in mild TBI cases, 4.8% in those with skull fractures, and up to 13.9% in cases with multiple types of hemorrhages (Fordington & Manford, 2020).
Antiepileptic medication use after traumatic brain injury (TBI) is crucial for managing and preventing post-traumatic seizures, particularly in high-risk patients. Early seizure prophylaxis is recommended for individuals with severe TBI, penetrating head injuries, or intracranial hematomas, where there is a higher incidence of early post-traumatic seizures. Prophylactic antiepileptic drugs (AEDs) are typically administered for a short duration, usually up to 7 days post-injury, to reduce the occurrence of early seizures. Commonly used AEDs include phenytoin and levetiracetam, with the latter being increasingly favored due to its favorable side effect profile and ease of administration in both oral and intravenous forms. (Younus et al., 2018)
Long-term seizure prophylaxis is not routinely recommended for all TBI patients. Instead, it is reserved for those who experience early seizures or possess specific risk factors indicating a higher likelihood of developing post-traumatic epilepsy. Regularly monitoring drug levels, patient response, and potential side effects is essential for effective management. Gradual tapering of AEDs may be necessary to avoid withdrawal seizures if long-term use is deemed unnecessary.
Brain injuries can lead to coagulopathy (a disorder of blood coagulation). TBIs may lead to a systemic release of tissue factors and brain phospholipids into the circulation, leading to abnormal intravascular coagulation and consumptive coagulopathy (Moore et al., 2021). Those with coagulopathy after a TBI have a worse prognosis.
The ventricles can dilate when CSF builds up in the brain, leading to hydrocephalus and an increased ICP. It often occurs soon after an injury but can occur after an extended time. Increased ICP may lead to cerebral edema, ischemia, hypoxia, and brain herniation.
Skull fractures are another complication. When the matter between the dura and the arachnoid membrane tears, CSF can leak out in a condition called subdural hygroma. Fluid can leak out of the nose, ears, and mouth. Any tear in the brain's protective matter increases the risk of bacteria entering these spaces, leading to meningitis.
Stroke is a complication of TBI. Hemorrhagic stroke after TBI occurs when blood vessels within the brain rupture, leading to bleeding. This can be caused by direct trauma to the blood vessels, coagulation abnormalities, or the use of anticoagulant medications. TBI can lead to ischemic strokes through mechanisms such as blood vessel injury, clot formation, or arterial dissection. The inflammation and swelling associated with TBI can also contribute to vascular damage and reduced blood flow. The clinical presentation of a stroke following TBI can include sudden weakness or numbness, particularly on one side of the body, confusion, difficulty speaking or understanding speech, visual disturbances, severe headache, dizziness, and loss of balance or coordination.
Cranial nerve (CN) injury can occur with a TBI; however, it is more common when a fracture is near the skull's base. The facial nerve (CN VII) is the most commonly injured cranial nerve, resulting in face paralysis. Cranial nerve injury may lead to an impaired sense of smell or taste. If the patients lose their sense of smell, it will likely be permanent if it lasts one year after the injury (Liu et al., 2023). Double vision may occur, and cranial nerve IV will likely be affected if it occurs. Damage to the trigeminal nerve (CN V) leads to facial pain.
Cranial Nerves
*Please click on the image above to enlarge.
Post-concussion syndrome (PCS) is a complex disorder characterized by a variety of physical, cognitive, emotional, and sleep-related symptoms that persist for weeks, months, or even longer after a concussion or TBI. While most people recover from a concussion within a few days to weeks, a significant minority develop PCS, experiencing prolonged and often debilitating symptoms. Post-concussion syndrome is characterized by dizziness, vertigo, headache, reduced concentration, apathy, depression, sleep disturbance, confusion, irritability, and anxiety. Diagnosis of PCS is made clinically based on the persistence of symptoms following a concussion. There are no definitive diagnostic tests for PCS, but neuroimaging (such as MRI or CT scans) and neuropsychological testing may be conducted to rule out other conditions and assess cognitive function.
Amnesia can also occur after a head injury. Anterograde amnesia is impaired memory of events after the injury, whereas retrograde amnesia is memory deficits of events before the injury.
Brain dysfunction can take many forms after a TBI. The following are problems that may present after a TBI:
Aphasia (inability or reduced ability to communicate, which can include impairments in expression or understanding of written or verbal language)
Dysarthria (cannot speak the proper words due to dysfunction of the muscles used to speak)
Reduced ability to carry out complex tasks
Behavior changes or onset of mental illness (depression/anxiety)
Social inappropriateness or aggression
Most of the recovery from a TBI occurs in the first six months and can be more gradual after six months.
Some problems may occur years after the head injury (Brett et al., 2022). Alzheimer's disease is the most common type of dementia and is linked to a prior history of head injury. Parkinson's disease can occur when there is a remote history of damage to the basal ganglia. As mentioned above, dementia pugilistica occurs in patients with a history of head trauma.
Agitation is commonly seen after a head injury. Other causes of agitation seen after a head injury may include pain, depression, infection, side effects of medications, sleep deprivation, or electrolyte imbalance.
A myriad of other problems may occur after a TBI, including:
Deep vein thrombosis
Spasticity
Rigidity
Gastrointestinal and genitourinary problems
Pneumonia
Decubiti
Organ failure
Chronic Traumatic Encephalopathy
Athletes who have experienced head injuries over the years may experience chronic traumatic encephalopathy (CTE), a neurodegenerative disease likely caused by repetitive brain trauma. It may result in memory problems, executive dysfunction/dementia, poor impulse control, depression, apathy, suicide, aggression, violence, substance abuse, and an increase in high-risk behaviors (e.g., increased food intake, risky sexual behavior, and gambling).
CTE is characterized by the accumulation of abnormal tau protein in specific brain regions. This pathology typically begins in the outermost layer of the frontal lobe (neocortex) and later spreads to deeper brain regions, such as the medial temporal lobe and brainstem (Wallingford & Junn, 2024). It was once thought to be only a problem in boxers but is now prevalent in football players and other sports.
CTE is not only caused by repetitive concussive blows, but may result from subconcussive trauma to the brain. CTE is difficult to diagnose because it overlaps with multiple other syndromes. CTE may start during the post-concussive syndrome. As the disease progresses, it presents similarly to other dementing illnesses such as frontotemporal dementia and Alzheimer's disease.
Different diagnostic tests are available to help determine the severity of the injury. Imaging helps determine if there is a fracture and assists in determining the prognosis.
Computed tomography (CT) scans are an often used initial test for moderate to severe head trauma.
CT scans are typically the first imaging modality used in the acute setting of TBI. They are excellent for detecting acute hemorrhages, skull fractures, and mass effects due to swelling or edema. CT scans offer the advantage of rapid acquisition, being widely available, and offering good detection of acute bleeds and fractures. Unfortunately, they offer limited sensitivity for diffuse axonal injury (DAI) and small lesions and expose patients to ionizing radiation.
Magnetic resonance imaging (MRI) is another commonly used test in the diagnostic workup of TBI. It is not the best initial test as it is more time-consuming and less readily available. The MRI is a more accurate test for detecting contusions, small hemorrhages, and diffuse axonal injury (Morales, 2023).
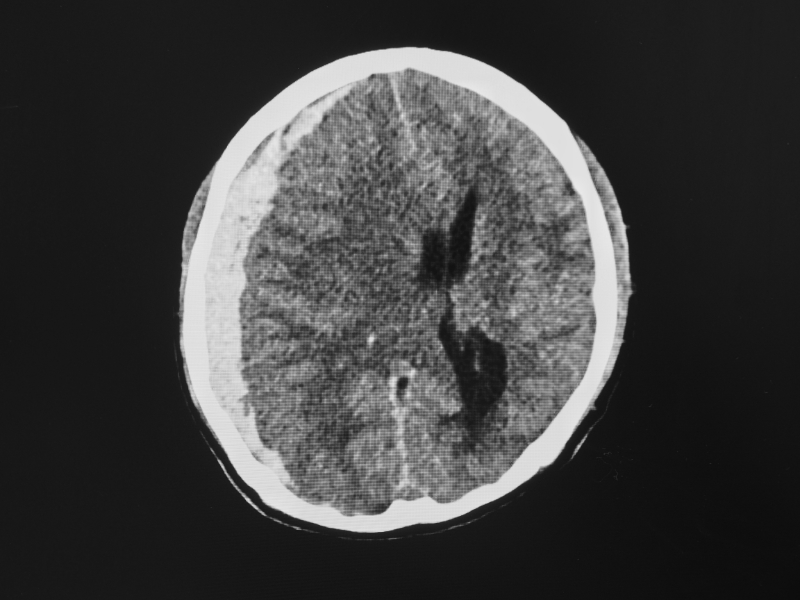
CT Showing Subdural Hematoma
Positron Emission Tomography (PET) and Single Photon Emission Computed Tomography (SPECT) are functional imaging techniques that assess brain metabolism and blood flow. They are not typically used in the acute setting but can provide valuable information in chronic TBI cases, especially for assessing brain function and recovery potential. They can detect abnormalities not visible on structural imaging but have limited availability, high cost, and exposure to radioactive tracers.
Indications for CT in TBI(Stiell et al., 2005; Kavalci et al., 2014):
Glasgow Coma Scale (GCS) score less than 15 - two hours post injury
Vomiting
Any loss of consciousness
The individual is 60-65 years old or older
Scalp lacerations to the bone of greater than 5 cm
Significant maxillofacial injuries
Persistent headache
Amnesia before the impact of 30 minutes or more
Dangerous mechanism of injury (e.g., pedestrian struck by a motor vehicle, occupant ejected from a motor vehicle, fall from ≥3 feet or ≥five stairs)
Suspected skull fracture (e.g., CSF leak [clear fluid from the nose or out of ears], raccoon eyes [bruising around eyes], Battle's sign [bruising behind ears], or hemotympanum [blood behind ear drum])
Mild TBIs often present at their primary care doctor's office, urgent care clinic, or as walk-in patients at an emergency department. More severe cases may present to the emergency department after transport by emergency medical personnel.
Those with severe injuries need to be medically stabilized as a primary priority. Pre-hospital care needs to ensure that the patient is triaged appropriately, stabilized, and assessed for any life-threatening complications, such as increased intracranial pressure and cerebral herniation.
The ABCs are of primary importance in any severe injury. Ensuring an airway is present to maintain adequate oxygen flow to the brain and the rest of the body. Intubation is often done on those with moderate or severe head injuries. Blood pressure control is necessary, as is controlling any other injuries that may accompany a head injury. Often, head injury cases are multi-trauma cases, including spinal cord injury, and patients need to be managed systemically as other injuries may be more immediately life-threatening.
Patients discharged with a mild head injury should be awakened every 2 hours and assessed neurologically. Patients and their caregivers should return to the hospital if there is any seizure, confusion, severe/worsening headache, watery discharge from the ear or nose, or persistent nausea and vomiting (Ainsworth, 2024).
Certain indications necessitate consideration for admission (Tolias, 2021). These include:
An attempted suicide
No responsible adult supervision
Epilepsy
Uncertain diagnosis
Drug or alcohol abuse
Co-morbid neurological disease
Coagulation disorder or someone on warfarin
A CT scan helps determine the degree of intracranial injury and helps predict the outcome. In those with normal CT scans, hospitalization may be avoided. CT scans help detect skull fractures, hemorrhage, midline shift, mass effect, and herniation. A repeat exam should occur in 4-8 hours for those with coagulopathies or intracranial hemorrhage. Abnormal findings on the CT scan, prolonged unconsciousness, persistent mental status changes, or an abnormal neurological exam necessitate referral to a neurosurgeon. Patients with normal CT scans after head injury will typically clinically improve within hours. Those who fail to improve should have a repeat CT scan (Rangel-Castilla, 2022).
Neurological checks should be done frequently. The patient should consume nothing orally until they are alert. Intravenous fluids will help prevent dehydration and help maintain pressure. Comfort measures should ensue with the use of mild analgesics and an antiemetic.
A Glasgow Coma Score under 8 indicates severe injury. A severe injury requires a CT scan, admission to the hospital (critical care admission), stabilization of hemodynamics, airway protection, and a neurosurgical referral. ICP should be monitored and should be lowered using a variety of measures, including:
Maintaining a systolic blood pressure above 90 mmHg
Keeping the head of the bed elevated to 30-45 degrees while keeping the neck straight
Mild sedation and pain control
External ventricular drains
Ventilate to normocapnia
Consider administering osmotic agents such as mannitol or hypertonic saline to reduce cerebral edema and lower ICP
Administer antiepileptic drugs to prevent seizures, which are common after severe TBI and can exacerbate brain injury
If medical management is not successful, surgical management may include decompressive craniectomy or evacuation of hematomas
Among those with moderate to severe head injury, fewer than 10% have an initial surgical lesion (Ainsworth, 2024). Possible indications for surgery include an open skull fracture, a depressed skull fracture, CSF leak, refractory intracranial hypertension, penetrating brain injury, and epidural, subdural, or intracerebral hematoma.
An athlete with a diagnosed sports-related concussion should not be allowed to return to play on the day of the injury(Patricios et al., 2023). If an athlete returns to play too quickly, there is a risk of recurrent concussion and cumulative brain injury. With each concussion, there is an increased risk of future concussions.
It is important to ensure that concussion symptoms are fully resolved before the athlete can return to exercise. Some student-athletes may require reduced schoolwork while recovering from a concussion. Student-athletes who are experiencing symptoms from their concussion need to rest the brain from cognitive activity so as not to worsen or lead to a re-emergence of the symptoms.
A stepwise progression is utilized to return the athlete to play gradually. There should be 24-48 hours of physical and cognitive rest before the return to sport progression begins (Bloom,G. & Caron, J., 2019). Each step should take no less than 24 hours, giving the athlete, at minimum, a one-week rehabilitation period. The athlete can proceed to the next progression if they remain asymptomatic at the current level. If post-concussion symptoms return during rehabilitation, the athlete should return to the previous step. They can try to progress again after 24 hours of rest and being symptom-free. The athlete whose symptoms persist for more than 10-14 days in adults or more than one month in children should be seen by an expert in the management of concussions.
Table 2: Graduated return-to-sport strategy (Patricios et al., 2023)
Stage
Aim
Activity
Goal of each step
1
Symptom-limited activity
Daily activities that do not provoke symptoms
Gradual reintroduction of work/school activities
2
Light aerobic exercise
Walking and stationary cycling at a slow to medium pace. No resistance training.
Increase heart rate
3
Sport-specific
Running or skating drills. No head impact activities.
Add movement
4
Non-contact training drills
Harder training drills, e.g., passing drills. May start progressive resistance training
Exercise, coordination, and increased thinking
5
Full contact practice
Following medical clearance, participate in normal training activities
Restore confidence and assess functional skills by coaching staff
Jake is a 17-year-old club soccer player who has played competitively for several years. After scoring a goal by heading the ball in a recent game, he exhibits signs of confusion when he asks the coach, “Who won the game?” Recognizing that it is only the first half, the coach decides to take Jake out of the game and requests that Emily, the athletic trainer, for an evaluation.
Upon assessment, Jake appears dazed and slightly disoriented. Emily makes note of the following subjective findings:
Jake reports feeling a bit dizzy and has a slight headache
He expresses uncertainty about recent plays and score
He has no prior history of concussion
Emily conducts several evaluations, including checking Jake’s cognitive function and symptoms. Luckily, the team had performed preseason SAC tests and Scat-6 baseline testing on all its athletes.
Glasgow Coma Scale (GCS): 15 (alert and oriented to person, place, and time).
Cervical spine assessment did not reveal pain, tenderness, or altered limb strength or sensation.
Coordination and ocular/motor screen was unremarkable.
SAC score had decreased from 19 at baseline to 16.
Given these findings, Emily decided to keep Jake out of the game, following concussion protocol guidelines. Jake was monitored on the sideline for changes in his symptoms, and a quiet space was provided for rest and recovery.
Following the game, the off-field assessment portion of the SCAT-6 was completed, and the score was mildly lower than at baseline testing.
Emily contacted Jake’s parents to inform them of the situation and recommended that he see his primary care physician for a thorough evaluation. Emily also proceeded to educate Jake and his parents on concussion symptoms, what red flag signs would warrant taking him to the emergency department, and the importance of rest, including the avoidance of screen time for the next few days. She discusses the potential risks of returning to play too soon.
The next day, Jake visits his primary care doctor, where he reports a slight headache and feelings of dizziness. He is advised to take the day off school to rest and avoid screens and strenuous activities.
Jake returns for a follow-up with his primary care doctor two days later, on day three following the concussion injury. He reports no symptoms and feels well enough to participate in light running at practice.
Over the next three days, Emily supervised Jake's return to sports and progression of physical activity. She closely monitored Jake for the return of any symptoms as he increased his physical exertion during the progression. On day one, Jake completed light running activities not with the team but independently on the sideline. The following day, he can perform technical non-contact drills with the team and continues to report no symptoms. On day 3 of his RTP progression, Jake participates in practice with more intensity, engaging in drills without discomfort. On day 4 of the practice progression, he fully participates and feels ready to return for the upcoming game. Over the week, the SAC and SCAT 6 were repeated, and it was determined that Jake's scores had returned to their baseline values.
The next Saturday, a pre-game assessment was performed, and Jake stated he woke up with a mild headache. It was decided that he would sit out the game but could participate in warm-up drills to stay engaged with the team.
The entire next week, Jake could participate in practice without limitations and reported no post-concussion symptoms. Jake was able to play in the next scheduled game without incident.
Conclusion
This case illustrates the effective management of a suspected concussion through proper assessment and adherence to a gradual return-to-play protocol. Jake was identified as potentially having a concussion and was removed from play immediately, which reduced the risk of further injury.
By following up closely and ensuring he remained symptom-free before advancing his activity levels, Jake returned to play while minimizing the risk of complications. His case emphasizes the critical role of athletic trainers in managing concussions and the importance of education regarding head injuries for athletes and their families. Emily's actions exemplify best practices in sports injury management. Immediate recognition and assessment of concussion symptoms, combined with proper communication and education, played a vital role in Jake's recovery. Future monitoring will be essential to watch for recurrent head injuries as he continues his athletic career.
Observation is recommended for at least 24 hours after a concussion because of the risk of intracranial complications. Admitting to the hospital may be considered for those with a GCS of less than 15, any seizure activity, CT scan evidence of cerebral edema or intracranial bleeding, those on anticoagulation medication, or those with a bleeding diathesis. Those with no one to monitor them at home should be admitted to the hospital for observation.
If an athlete is monitored at home, some clinicians recommend that the athlete be awakened from sleep every two hours the first night, and if the athlete cannot be awakened, immediate help should be attained. The athlete should not perform any strenuous activity for 24 hours. Other signs that should prompt the athlete to attain immediate medical help include confusion, drowsiness, vision difficulties, urinary or bowel incontinence, severe or worsening headaches, vomiting, stiff neck, fever, seizure, restlessness, and unsteadiness, or weakness/numbness of any body part. These findings suggest a potential intracranial bleed/cerebral edema secondary to a contusion. These signs warrant an evaluation, including a head CT.
Second impact syndrome is a rare complication of a mild head injury. This syndrome is diffuse cerebral swelling after a second concussion during the time the athlete is still symptomatic from the first. If the athlete returns to play too soon and develops another injury when not fully recovered from the first, swelling of the brain, herniation, or death may occur. It is not a common condition, but athletes may die within a few minutes if it does occur.
When evaluating a patient with a TBI, the priority is always airway, breathing, and circulation. It is also important to rule out any spinal cord/cervical spine injury, and if suspected, immobilization and radiography should occur. Paresthesia, reduced consciousness, posterior midline tenderness/pain, or extremity weakness may suggest spinal cord/cervical spine injury.
Preventing traumatic brain injury (TBI) is a key strategy in reducing the incidence and severity of these injuries, which can have long-lasting physical, cognitive, and emotional effects. Prevention strategies encompass various interventions, from individual protective measures to public health initiatives. Multiple steps should be implemented to prevent TBI. These include:
Wearing a seatbelt and properly securing children in the car.
Drive at or below the speed limit.
Use helmets when riding motorized vehicles or bikes.
Use proper protective gear when playing sports.
Practice gun safety.
Fall prevention methods.
Eliminate tackling from school football for those under 16 to reduce concussions.
More education should be provided to athletes, coaches, parents, school administrators, and healthcare providers regarding concussion assessment, prevention, and management.
An 85-year-old female was admitted to the hospital following an unwitnessed fall at home in the early hours of the day. The client sustained a left humeral fracture and a left hip fracture. The client underwent a total hip replacement, and a sling was applied to her left arm two days ago. The Occupational Therapist arrives to initiate AROM to the elbow, wrist, and hand and begin training with adaptive equipment for lower body dressing.
While gathering information regarding the client's home situation, prior level of function, and occupational profile, the client indicates that she does not recall the immediate events leading up to the fall (retrograde amnesia), nor does she believe that her family knows she is here in the hospital. Following ROM and strength assessment, the client begins complaining of a headache, stating, "I have had a headache since this morning. I think it is because of the lights" (photophobia). Wrapping up the OT evaluation, the OT advises the nurse of her findings related to retrograde amnesia and complaints of a headache and sensitivity to light.
This information is then relayed to the physician, who suspects a possible TBI and orders a CT, which proves negative. However, the doctor suspects the client may have a mild concussion and requests 2-hour neuro-checks and that therapy be continued.
The therapist provided ROM exercises to the client in bed with only the over-bed backlight light and short demonstrations on using the adaptive equipment, beginning with slipper socks and advancing to pants and undergarments by day 5 of admission. By day 5, the client is no longer complaining of a headache and can now demonstrate the ability to complete lower body dressing with adaptive equipment.
This case is the typical course of a client initially seen by therapy for orthopedic concerns. She was determined later to have sustained a mild TBI due to a fall. The client could participate in therapy with modifications made to the environment to reduce stimulation and graded activities until symptoms resolved. The client will need to be monitored to ensure the resolution of symptoms.
Head injuries are common, costly, and, at times, devastating. Healthcare Professionals should know how to assess, educate, and monitor patients with TBI. With recent information about mild traumatic brain injury in sports, it is becoming more important for all healthcare providers to fully understand TBI, its recognition, management, and prevention.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Ainsworth, C. R. (2024). Head Trauma. Medscape. Visit Source.
Anwer, F., Oliveri, F., Kakargias, F., Panday, P., Arcia Franchini, A. P., Iskander, B., & Hamid, P. (2021). Post-Traumatic Seizures: A Deep-Dive Into Pathogenesis. Cureus. Visit Source.
Brett, B. L., Gardner, R. C., Godbout, J., Dams-O'Connor, K., & Keene, C. D. (2022). Traumatic Brain Injury and Risk of Neurodegenerative Disorder. Biological Psychiatry, 91(5), 498–507. Visit Source.
Centers for Disease Control and Prevention (CDC). (2024). Traumatic Brain Injury & Concussion. Visit Source.
Centers for Disease Control and Prevention (CDC). (n.d.). Report to Congress on Traumatic Brain Injury in the United States: Epidemiology and Rehabilitation. Visit Source.
Fordington, S., & Manford, M. (2020). A review of seizures and epilepsy following traumatic brain injury. Journal of Neurology, 267(10), 3105–3111. Visit Source.
Kavalci, C., Aksel, G., Salt, O., Yilmaz, M. S., Demir, A., Kavalci, G., Akbuga Ozel, B., Altinbilek, E., Durdu, T., Yel, C., Durukan, P., & Isik, B. (2014). Comparison of the Canadian CT head rule and the New Orleans criteria in patients with minor head injury. World Journal of Emergency Surgery, 9(31). Visit Source.
Liu, X., Lei, Z., Gilhooly, D., He, J., Li, Y., Ritzel, R. M., Li, H., Wu, L. J., Liu, S., & Wu, J. (2023). Traumatic brain injury-induced inflammatory changes in the olfactory bulb disrupt neuronal networks leading to olfactory dysfunction. Brain, Behavior, and Immunity, 114, 22–45. Visit Source.
Moore, E. E., Moore, H. B., Kornblith, L. Z., Neal, M. D., Hoffman, M., Mutch, N. J., Schöchl, H., Hunt, B. J., & Sauaia, A. (2021). Trauma-induced coagulopathy. Nature Reviews. Disease Primers, 7(1), 30. Visit Source.
Morales, D. (2023). Brain, Contusion (Trauma). Medscape. Visit Source.
Pangilinan, P. H. (2024). Classification and Complications of Traumatic Brain Injury. Medscape. Visit Source.
Patricios, J. S., Schneider, K. J., Dvorak, J., Ahmed, O. H., Blauwet, C., Cantu, R. C., Davis, G. A., Echemendia, R. J., Makdissi, M., McNamee, M., Broglio, S., Emery, C. A., Feddermann-Demont, N., Fuller, G. W., Giza, C. C., Guskiewicz, K. M., Hainline, B., Iverson, G. L., Kutcher, J. S., Leddy, J. J., … Meeuwisse, W. (2023). Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport-Amsterdam, October 2022. British Journal of Sports Medicine, 57(11), 695–711. Visit Source.
Rangel-Castilla, L. (2022). Closed Head Trauma Workup. Medscape. Visit Source.
Stiell, I. G., Clement, C. M., Rowe, B. H., Schull, M. J., Brison, R., Cass, D., Eisenhauer, M. A., McKnight, R. D., Bandiera, G., Holroyd, B., Lee, J. S., Dreyer, J., Worthington, J. R., Reardon, M., Greenberg, G., Lesiuk, H., MacPhail, I., & Wells, G. A. (2005). Comparison of the Canadian CT Head Rule and the New Orleans Criteria in patients with minor head injury. JAMA, 294(12), 1511–1518. Visit Source.
Tolias, C. (2021). Initial Evaluation and Management of CNS Injury. Medscape. Visit Source.
Wallingford, A., & Junn, C. (2024). Chronic Traumatic Encephalopathy. Physical Medicine and Rehabilitation Clinics of North America, 35(3), 607–618. Visit Source.
Younus, S. M., Basar, S., Gauri, S. A., Khan, A. A., Imran, M., Abubakar, S., Sheikh, D., Shehbaz, N., & Ashraf, J. (2018). Comparison of Phenytoin versus Levetiracetam in Early Seizure Prophylaxis after Traumatic Brain Injury, at a Tertiary Care Hospital in Karachi, Pakistan. Asian Journal of Neurosurgery, 13(4), 1096–1100. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.