This course will be updated or discontinued on or before Wednesday, November 24, 2027
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
CEUFast, Inc. is an AOTA Provider of professional development, Course approval ID#15188. This distant learning-independent format is offered at 0.2 CEUs Intermediate, Categories: OT Foundational Knowledge
AOTA does not endorse specific course content, products, or clinical procedures. AOTA provider number 9757.
CEUFast, Inc. (BOC AP#: P10067) is approved by the Board of Certification, Inc. to provide education to Athletic Trainers (ATs).
FPTA Approval: CE25-491496, CE26-491496. Accreditation of this course does not necessarily imply the FPTA supports the views of the presenter or the sponsors.
CEUFast, Inc. is recognized by the New York State Education Department's State Board for Physical Therapy as an approved provider of physical therapy and physical therapist assistant continuing education.
Outcomes
≥ 92% of participants will know the basics of interpreting rhythms on an electrocardiogram (EKG/ECG).
Objectives
After this course, participants will be able to:
Describe normal cardiac anatomy and normal electrical conduction through the heart.
Identify and relate electrocardiogram (EKG/ECG) waveforms to the cardiac cycle.
Characterize standard lead placements and the purpose of each lead position.
Formulate a systematic process when approaching the interpretation of the EKG/ECG.
Differentiate normal and abnormal components on an EKG/ECG.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Electrocardiograms (EKGs/ECGs) are employed in ambulances, emergency departments, surgical suites, intensive care units, and other clinical settings to facilitate the diagnosis of suspected myocardial infarction, syncope, abnormal vital signs, or irregular pulses. EKG/ECG testing is routinely incorporated into health examinations for middle-aged and older adults, reflecting their increased risk of cardiovascular disease relative to younger populations. It is imperative that all healthcare professionals possess a thorough understanding of EKGs/ECGs and recognize their critical role in the prompt identification of cardiovascular system abnormalities.
EKGs/ECGs visually represent the heart's electrical activity during both contraction and relaxation phases, offering clinicians essential information regarding real-time cardiac function (Sattar & Chhabra, 2023). Accurate interpretation of EKG/ECG tracings relies on a thorough understanding of the generation and propagation of electrical impulses within the myocardium, as well as comprehensive knowledge of cardiac anatomy. This expertise enables healthcare professionals to discern normal from abnormal patterns—such as arrhythmias—thereby facilitating prompt and informed clinical decision-making.
To grasp the fundamentals of EKGs/ECGs and their interpretation, it is essential to understand the intricate relationship between the heart's structure and its function. The heart's electrical conduction system operates as the guiding force behind its rhythmic contractions, ensuring blood flow is synchronized and efficient. A comprehensive appreciation of this system not only aids in recognizing normal electrical patterns but also sharpens the ability to detect deviations that may signal underlying pathologies.
The cardiovascular system provides oxygen-rich blood to tissues, meeting their metabolic needs. The arterial system delivers oxygen, nutrients, hormones, and immune substances, while helping regulate body temperature. Venous return removes waste, directing deoxygenated blood to the lungs and organs for cleansing and excretion (Chaudhry et al., 2022).
The heart is an organ with several distinctive properties. It operates as a pump, expanding and contracting without causing stress to its structure or leading to muscle fatigue. The heart pumps four to eight liters per minute, which amounts to approximately 6,000-7,000 liters per day. It generates electrical impulses to maintain a consistent rhythm, irrespective of the contraction rate. The heart also filters out many inappropriate electrical signals, preventing overstimulation of the cardiac muscle.
As small as the heart is, it carries an impressive workload over a lifetime. It beats 60 to 100 times per minute without resting. The heart must be flexible and able to adjust to changes in the body's metabolic demands, often in a matter of seconds. Vigorous exercise can increase the metabolic requirements of muscles by as much as 20 times over their needs during rest. To meet the increased demands of the muscles, the heart accelerates its rate to increase cardiac output. Vessels must redistribute blood flow, shunting a greater proportion of blood to muscle tissues and away from internal organs.
Oh, and because it is a curious bit of data you can use to get a client's interest engaged, every minute the body's entire volume of blood circulates three times from the heart and back again! (Answers, 2024).
Now, something important. An EKG/ECG is the graphic measurement of the electrical activity within the heart. An older abbreviation stemming from the German term "elektrokardiogramm," EKG is used interchangeably with ECG (Singh, 2025b).
Why do we cling to an abbreviation with German origins? There are several rationales. However, I favor the chaos speech notion from my own work in critical care, having led off-hours code response in a community trauma center. That is, in the heat of an emergency, calling verbally for an "EKG" is better understood than calling for an "ECG," which might be misconstrued as an "EEG," or electroencephalogram, brain wave imaging. For the sake of technical accuracy, we will be using the term EKG/ECG by preference when talking about electrocardiograms.
The EKG/ECG is a valuable diagnostic tool for the healthcare provider, whether they are a doctor, nurse, emergency responder, or a rehabilitation specialist. Understanding the EKG/ECG enables the healthcare provider to respond correctly and treat dangerous and potentially deadly arrhythmias as quickly and efficiently as possible. It is important to understand the mechanisms and know just what needs to be done to provide appropriate care for clients with serious abnormal heart rhythms.
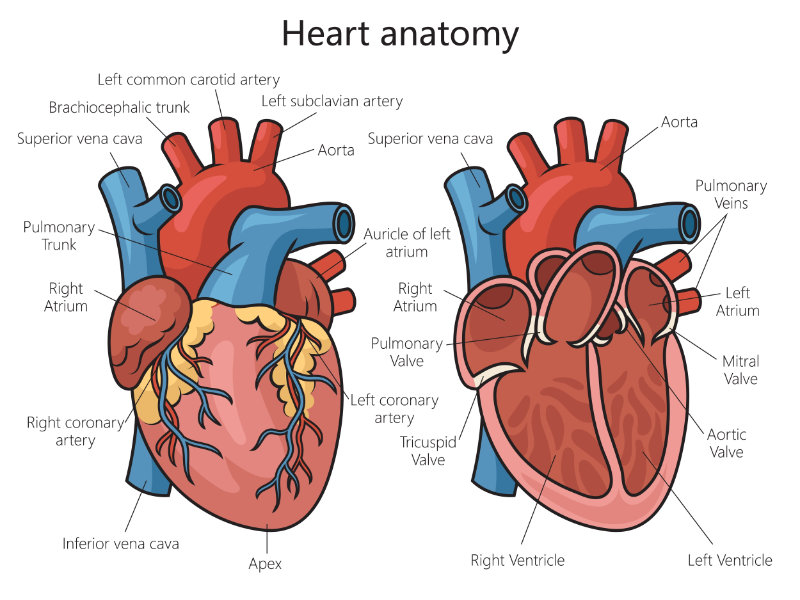
The heart is a hollow, muscular organ in the middle of the thoracic cavity, just left of the midline above the diaphragm. It is protected by the sternum, spine, and lungs, and enclosed in a fluid-filled pericardial sac that prevents infection and friction, aiding function. The heart has three layers: epicardium, myocardium, and endocardium (Helmenstine, 2025).
Activities on the right side of the heart and the left side of the heart occur simultaneously.
The heart's ability to perform its vital functions relies on its highly specialized structure and intricate coordination of impulses. This coordination begins in the sinoatrial (SA) node, often referred to as the heart's natural pacemaker, located in the upper wall of the right atrium. The SA node generates electrical signals that initiate each heartbeat. These signals travel through the atria, causing them to contract and push blood into the ventricles (Kashou et al., 2022).
From there, the impulses reach the atrioventricular (AV) node, which briefly delays the signal to ensure the ventricles are filled completely before contracting. The signals are then transmitted via the bundle of His and Purkinje fibers to the ventricular muscles, causing them to pump blood either to the lungs or throughout the body. This flawless communication between the components allows the heart to maintain a rhythm that adapts seamlessly to the body's varying demands (Heaton & Goyal, 2023).
The right side of the heart receives deoxygenated blood from the body via the vena cava into the right atrium. Blood is ejected from the right atrium into the right ventricle. Blood is pumped to the lungs from the right ventricle via the pulmonary artery. The left side of the heart receives oxygenated blood from the lungs via the pulmonary vein into the left atrium. Blood is ejected from the left atrium to the left ventricle. Blood is pumped to the body from the left ventricle via the aorta. The right side of the heart pumps blood into the lungs. The left side pumps blood into the body.
Image 2: Posterior View
The septum and valves separate the two atria and two ventricles of the heart. Blood is pumped through the chambers, aided by four heart valves. The valves open and close to let the blood flow in only one direction. The four heart valves include the following (Cleveland Clinic, 2022):
The tricuspid valve is located between the right atrium and the right ventricle.
The pulmonary (pulmonic) valve is between the right ventricle and the pulmonary artery.
The mitral valve is between the left atrium and left ventricle.
The aortic valve is between the left ventricle and the aorta.
Each valve has a set of "flaps" (also called leaflets or cusps). The mitral valve normally has two flaps; the others have three.
Our heart supplies or pushes oxygenated blood to the cells throughout the body. Given the workload, it is not surprising that the heart itself also needs oxygenated blood delivered to its busy muscle cells!
Yes, coronary arteries, the ones frequently implicated in myocardial infarctions, are the delivery arm for oxygen to myocardial cells.
Table 1: Arteries
Right Coronary Artery
Supplies:
Right atrium, anterior right
Posterior and papillary muscle wall ventricle
Posterior aspect of septum (90% of the population)
Sinus and AV nodes (80-90% of the population)
Inferior aspect of the left ventricle
Left Coronary Artery
Left anterior descending supplies:
Anterior left ventricular
Anterior interventricular septum
Septal branches supply:
Conduction system, bundle of His, and bundle branches
The human heart is a remarkable piece of engineering. The human heart beats 80,000 to 100,000 times daily and pumps approximately 2,000 gallons every day. The heart will have beaten 2-3 billion times and pumped 50-65 million gallons of blood over a 70 to 90-year lifespan. The human heart is made of specialized muscle capable of sustaining continuous beating. This muscle is different from the skeletal muscle that powers the arms and legs. Specialized areas of the myocardium exert electrical control over the cardiac cycle. These areas exhibit physiological differences from the rest of the myocardium, forming a pathway for electrical impulses that energize the heart muscle. The two types of cardiac cells are contractile and conductive. When myocardial cells are at rest, they are electrically more negative on the inside with respect to the outside of the cell. Charged particles (ions) of sodium and potassium move in and out of the cell, causing changes sensed by electrodes on the skin. The heart's electrical action will show as a tracing on the EKG/ECG.
The SA, or sinus node, initiates a self-generating impulse independent from the brain (Kunwar, 2024) and is the primary pacemaker that sets a rate of 60 to 100 beats per minute (bpm). The SA node is located at the border or junction of the superior vena cava and right atrium. Once generated, this electrical impulse sets the rhythm of contractions and travels through both atria over a specialized conduction network to the AV node. The AV node is in the floor of the right atrium and receives the contraction impulse, which it transmits to the bundle of His. The bundle of His then divides the conduction pathway into a right bundle branch and a left bundle branch. These terminate in a complex network called the Purkinje fibers, which spreads throughout the ventricles. When the impulse reaches the ventricles, stimulation of the myocardium causes depolarization of the cells, and contraction occurs. The AV node serves as a gate to delay electrical conduction and, in this way, prevents an excessive number of atrial impulses from entering the ventricles (ClinicalGate, 2025).
The SA node and AV node are supplied with sympathetic and parasympathetic fibers. These nodes enable instantaneous changes in the heart rate in response to physiological changes in oxygen demand.
Normal cardiac conduction occurs in this sequence (Bhattacharyya & Munshi, 2020):
The SA node initiates an electrical impulse, sending it through the atrium, causing an atrial kick, then to the AV node, bundle of His, right and left bundle branches, and finally to the Purkinje fibers into the ventricular muscle.
If the SA node falters, a hierarchy of backup pacemakers can take over. Atrial, AV node, and ventricular escape pacemakers can function as subsidiary pacemakers. However, they generate impulses at a much slower rate. The AV node generates rates between 40 and 60 bpm, and the Purkinje fibers at 20 to 40 bpm.
An electrical impulse does not always equal the contraction of the heart. Accessory pathways play a role in reentry tachydysrhythmias, providing a detour for unwanted electrical impulses to circle through the heart.
There are two basic cardiac cell types (Ripa et al., 2023).
Myocardial muscle cells (mechanical cells) are the myocardium or the body of the heart. These contain contractile filaments that shorten when the cells are electrically stimulated. Their primary function is contraction and relaxation. Their primary property is contractility.
Electrical cells (pacemaker cells) are electrical impulse-generating cells that are found in the electrical conduction system. They conduct impulses very rapidly, and their primary property is automaticity and conductivity.
Cardiac cells are surrounded by, and filled with, a solution that contains ions. Three key ions are sodium, potassium, and calcium. In the resting period of the cell, the inside of the cell membrane is considered negatively charged, and the outside of the cell membrane is positively charged. The movement of these ions inside and across the cell membrane constitutes a flow of electricity that generates the signal on an EKG/ECG (MacKinnon & Haque, 2025).
Cardiac cells that are resting have a negative polarization. Sodium ions are outside of the cell, and potassium ions are inside the cell. Both ions carry a positive charge; however, sodium ions have a stronger charge than potassium. Thus, the inside ion state of the cell is electrically weaker than the outside, so it is negative. The polarized state is a "ready state." When the cell is ready to accept an electrical impulse, a large amount of potassium leaks out. This leak causes a discharge of electricity, and the cell becomes positively charged. This discharge is called depolarization. The electrical wave created at this pacemaker site travels from cell to cell along the electrically sensitive conduction pathways and from there throughout the heart. Now, cell recovery begins. Sodium and potassium ions are shifted back to their original place by the sodium-potassium pump. This process is called repolarization (Grider et al., 2023).
Electrical impulses result from a brief but extremely rapid flow of positively charged ions (sodium) back and forth across the cell membrane.
The cardiac action potential illustrates the changes in the membrane potential of a cardiac cell during depolarization and repolarization.
Five electrochemical phases are recognized, starting with Phase "0". Yes, that is correct, zero through four, totaling five phases. Just go with it. The minds of clinical scientists are a mystery to the rest of us (Demyanets, 2024).
Phase 0
Rapid depolarization ends the cell's relaxation state. Thus, presumably, the "0" designation indicates coming to a readiness for the beginning of cell contraction. The electrical activity that mirrors physiological contraction is also known when considering the atrial portion of the heart as a "P" wave. Depolarization of the ventricular heart is a QRS complex (Wei et al., 2023).
This phase is also called "upstroke," "overshoot," or "spike."
Begins when a cell receives an impulse.
Sodium moves quickly into the cell through the fast sodium channels.
Potassium then leaves the cell.
Calcium moves slowly into the cell through calcium channels.
This movement produces about +20 microvolts of positive electrical power.
The cell depolarizes, and the process of cardiac contraction begins.
Phase 1
Early repolarization, e.g., "partial" repolarization of the cell membrane due to sodium ion passage, creating an electrical current (Wei et al., 2023).
The rapid flow of sodium into the cell is stopped as the fast sodium channels close.
Potassium begins to reenter the cell, and sodium begins to leave.
This movement is about zero mV and is therefore neutrally charged, neither positively nor negatively charged.
This action is the absolute refractory period.
Phase 2
Plateau phase (slow repolarization, part of the absolute refractory period). Calcium shift causes a stasis or "holding" of the electrical charge (Wei et al., 2023).
Slow repolarization continues.
Calcium continues to flow into the cell through slow calcium channels.
Phase 3
Final repolarization of the cell occurs as calcium and sodium movement is shut down. Leaving the cell at a baseline charge and eager to go (Wei et al., 2023).
Rapidly, the cell completes repolarization.
Calcium channels close.
Potassium rapidly flows out of the cell.
Active transport via the potassium-sodium pump begins restoring potassium to the inside of the cell and sodium to the outside of the cell.
The cell is now in the negative state due to the outflow of potassium.
Gradually, the cell becomes extremely sensitive to external stimuli until its original sensitivity has been restored, called the relative refractory period.
Phase 4
Return to the resting stage, at the resting potential of -89 millivolts. Do not be fooled. Holding a negative charge means the outflow or net efflux from the cell is a positive charge (Wei et al., 2023).
Corresponds to diastole.
Calcium and sodium remain outside the cell.
Potassium remains inside the cell.
During this phase, the heart is "polarized" and getting ready for discharge.
Once another stimulus occurs, the cell will reactivate.
Image 5: Cardiac Cycle
Table 2: Keys to Remember
Electrical events show as tracings on the EKG/ECG.
Depolarization and repolarization are electrical events.
The heart can initiate an electrical impulse. The heart can begin and maintain rhythmic activity without the aid of the nervous system. A heart removed from the body can beat on its own for a limited period. The highest degree of automaticity is found in the pacemaker cells of the sinus node. The atria, AV Node, bundle of His, bundle branches, Purkinje fibers, and the ventricular myocardium have less automaticity (Nora Eccles Harrison Cardiovascular Research & Training Institute, n.d.).
Excitability
The heart can respond to an electrical impulse. A cardiac cell will respond to an electrical stimulus with an abrupt change in its electrical potential. Each cardiac cell that receives an electrical impulse will change its ionic composition and its respective polarity. Once an electrical potential begins in a cardiac cell, it will continue until the entire cell is polarized (Nora Eccles Harrison Cardiovascular Research & Training Institute, n.d.).
Conductivity
The heart can conduct an electrical impulse. All areas of the heart appear to depolarize simultaneously because a cardiac cell transfers an impulse to a neighboring cell very rapidly (Nora Eccles Harrison Cardiovascular Research & Training Institute, n.d.).
Table 3: Electrical Conduction Speed
The velocity of the impulse conduction transfer varies in different cardiac tissues:
0.05 meters per second (m/s) in the SA node
1.0 m/s between the SA node and AV node
0.05 m/s in the AV node
1.5 m/s in the bundle of His
4.0 m/s in the Purkinje fibers
(Laske & Iaizzo, 2024)
Contractility is the ability of the heart to respond by contracting.
The normal cardiac impulse arises in the specialized pacemaker cells of the SA node, located about 1 millimeter (mm) beneath the right atrial epicardium at its junction with the superior vena cava. The impulse then spreads over the atrial myocardium to the left atrium via Bachmann's bundle and the AV node region via the anterior, middle, and posterior internodal tracts connecting the sinus and AV nodes. These represent the usual routes of spread but are not specialized tracts analogous to the Purkinje system. When the impulse reaches both atria, they depolarize electrically, producing a P wave on the EKG/ECG, and then contract mechanically, producing the wave of the atrial pressure pulse and propelling blood forward into the ventricles.
Conduction slows when the impulse reaches the AV node, allowing sufficient time for blood to flow from the atria into the ventricles. After the impulse emerges from the AV node, conduction resumes rapidly through the bundle of His to the right and left bundle branches. It terminates in the Purkinje fibers in the ventricular muscle.
Stimulation of the myocardium causes progressive contraction of the myocardial cells. Therefore, wave deflections correspond to the cardiac cycle's mechanical events, including contraction and relaxation of the cardiac chambers. Repolarization is only electrical, and during that, the heart is at rest.
Three major waves of electric signals appear on the EKG/ECG. Each one shows a different part of the heartbeat (Bhattacharyya & Munshi, 2020).
The first wave is called the P wave. It records the electrical activity of the atria.
The second and largest wave, the QRS wave, records the electrical activity of the ventricles.
The third wave is the T wave. It records the heart's return to the resting state.
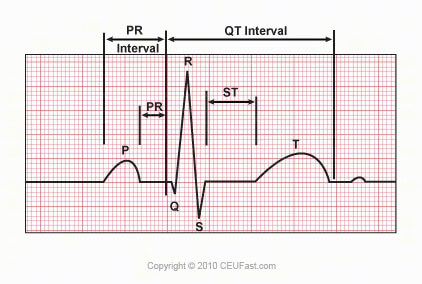
Image 6 : Cardiac Electric Cycle
The P wave represents atrial electrical activation. The PR interval is the time from the onset of atrial activation to the onset of ventricular electrical activation. The QRS complex represents the ventricular electrical activation spike. The QRS duration is the length of ventricular activation. The ST-T wave represents ventricular repolarization. The QT interval is the duration of ventricular activation and recovery. The U wave, that little bump of mystery on the electrical tracing of heart activity, represents "after depolarization" in the ventricles.
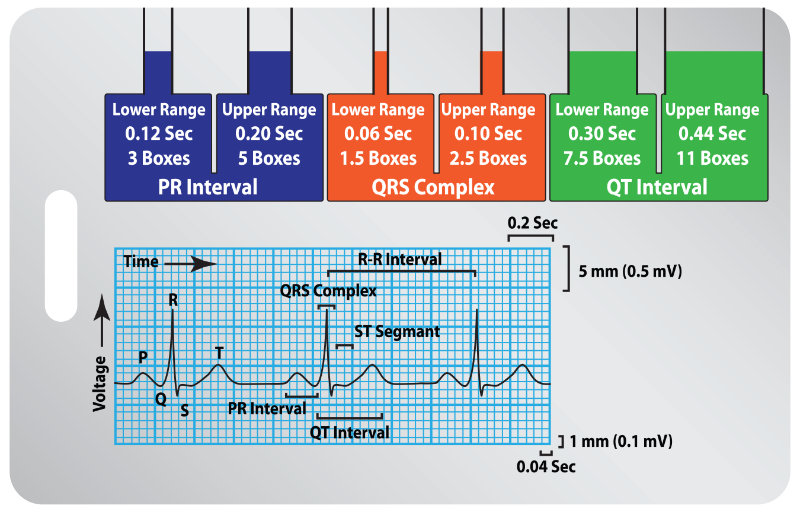
Image 7: EKG/ECG and Cardiac Cycle
An EKG/ECG is a recording of the heart's electrical output. This recording gives a visual index of the mechanical activity occurring with every life-giving beat. The background format of an EKG/ECG strip is a graphic field on what is known as electrocardiograph paper. An electrocardiograph tracing moves at a 25 mm/sec speed and is heat-inscribed onto the special paper as the horizontal X-axis. At the same time, electrical strength (voltage) is scribed onto the Y-axis (vertically). Each large square is 0.2 seconds, so five large squares make one second. Each 0.2-second square is further divided into five small squares of 0.04 seconds each.
Voltage, or the strength of the heart's electrical impulses, is represented on the vertical Y-axis. Each microvolt of positive electrical current raises the stylus 1 centimeter (cm) or one large square. The waveform baseline or bioelectric line is electrically neutral, usually without any deflections, e.g., a flat line (Sattar & Chhabra, 2023).
P Wave
A P wave on an EKG/ECG represents atrial depolarization. This wave represents one electrical activity associated with an impulse from the SA node and the electrical spread (conduction) through the atria. The SA node is, physiologically, located in the right atrium, so the right atrium begins constriction or depolarization. This depolarization represents the first half of the P wave. As depolarization spreads to the left atrium, we observe that process in the second half of the P wave (Douedi & Douedi, 2023). The total duration of the P wave should be, in general, three small squares, with 2.5 small squares of height.
In leads I and II, which we will get to soon, P waves should always be positive or above the baseline, while in lead aVR, again, looking ahead, in a normal sinus rhythm, it should be negative. And here is a teaser to whet your interest: when you see an abnormal P wave, consider strongly the presence of atrial changes such as myocardial enlargement (Biology Insights, 2025).
PR Interval
PR Interval represents the time from the start of atrial depolarization, P wave, to the beginning of the QRS, or ventricular depolarization. The normal PR interval is three to five small squares or 0.12 to 0.20 seconds. Long PR intervals might indicate a first-degree AV block presence, while short intervals accompany disorders of AV acceleration, such as Wolf-Parkinson-White (WPW) syndrome (Hacking, 2025).
QRS Complex
QRS represents ventricular depolarization (phase 0 of the action potential) until the end of ventricular depolarization (Lome, n.d.a).
This brings us to the QRS complex, a crucial portion of the EKG/ECG that illustrates ventricular depolarization—the momentous electrical event that triggers the contraction of the heart's powerful lower chambers. The QRS complex is typically much steeper and sharper than the P wave, reflecting the rapid spread of the impulse through the ventricles. Normally, its duration should measure no more than three small squares or 0.12 seconds, emphasizing the swiftness of ventricular activation. Widened QRS complexes can suggest issues like bundle branch blocks or ventricular rhythms. Each component of the complex, the Q, R, and S waves, carries unique significance.
The duration of the entire QRS is under 120 milliseconds or three small squares. An extended QRS might indicate the presence of a bundle branch block or hyperkalemia. Early ventricular contractions (premature ventricular contractions or PVCs) are frequently associated with a wide QRS length. So, remember to count boxes in the QRS when you see those annoying PVCs.
Q Wave
The Q wave is the initial, tiny, downward, or negative deflection of ventricular depolarization and contraction. To be more exact, Q represents depolarization of the intraventricular septum, the membranous and muscular partition separating the right from the left ventricles of the heart (Burns, E. & Buttner, 2024b).
The normal Q wave is small and easily missed. It is less than 25% of the R wave amplitude and does not exceed 0.04 seconds in duration, one small box. Abnormal Q waves are a strong indication of the presence of an old myocardial infarction.
R Wave
The R wave is the first upward or positive deflection after the P wave and the tallest portion of the QRS complex (ACLS Medical Training, n.d.).
S Wave
The S wave is the first downward or negative deflection after the R wave and represents the final depolarization of the Purkinje fibers (ACLS Medical Training, n.d.).
ST Segment
The ST segment is the electrical resting period after ventricular depolarization. It represents early repolarization of the left and right ventricles. This interval begins with the end of the QRS complex and ends with the onset of the T wave (Kashou et al., 2023). Its duration is two to three small squares, 80-120 milliseconds, and its isoelectric charge should lie at the same height as the PR interval. This height comparison is important. ST elevation can be an indication of acute myocardial infarction. Other heart conditions that are expressed in ST abnormalities include acute pericarditis, hyperkalemia, hypercalcemia, pulmonary embolism, ventricular aneurysm, left bundle branch block, Prinzmetal angina, blunt trauma to the heart, Brugada syndrome, and even subarachnoid hemorrhage.
T Wave
The T wave is the process of ventricular repolarization (ACLS Medical Training, n.d.). It should be less than two-thirds of the height of the R wave. T wave morphology changes are seen in conditions such as hyperkalemia, hypercalcemia, endocrine changes, myocarditis, pericarditis, cardiomyopathy, pulmonary embolism, fever, generalized infections, anemia, acid-base disorders, and more.
QT Interval
The QT interval represents the total ventricular activity from ventricular depolarization to repolarization. There is no fixed "normal" for this period of length, though 400 to 440 milliseconds has been suggested. It is measured from the beginning of the QRS complex to the end of the T wave, with slower heart rates having longer QTs (Lome, n.d.b).
Prolonged QT intervals indicate a lengthened relative refractory period, a vulnerable period for abnormal electrical mischief. Inside this vulnerable period, critical, life-threatening rhythms may attempt to establish themselves, such as Torsades de Pointe, ventricular tachycardia (VT), or ventricular fibrillation (VF).
U Wave
U waves are small positive deflections that may be seen following the T wave. There is no clear consensus on what they represent; however, delayed repolarization of the tissue known as the papillary muscle or Purkinje fibers is often present when they are seen (School of Health Sciences, n.d.).
J Wave
Osborn waves or J waves are seen mostly during hypothermia. This wave presents a small deflection at the junction, "J," of the QRS complex and the ST segment (Cadogan & Buttner, 2025).
Epsilon Wave
Congratulations if you encounter one—the epsilon wave is rare. It is a regularly occurring, small positive deflection buried at the end of the QRS complex that is most frequently associated with inherited heart disease from arrhythmogenic right ventricular cardiomyopathy. First described in 1977, this condition is responsible for 11% of sudden cardiac deaths in athletes (McKenna, 2024).
The standard heart monitor paper speed is 25 mm (five large squares)/sec. The interval between two beats (R-R) is five large squares. The heart rate is 60 bpm.
Methods for calculating the heart rate:
Rule of 300: Divide 300 by the number of the large squares between two heartbeats (R-R), or, if the interval between two beats is one large square, the HR is 300 bpm, two squares →150, three squares →100, four squares → 75, five squares → 60, six squares → 50 bpm.
The six-second method: Count the number of complete R waves within six seconds and multiply that number by ten. This count is the one-minute heart rate. This method can be used when the rhythm is "regular" or "irregular" (Singh, 2025a).
The three-second method: Count the number of complete QRS complexes in three seconds and multiply that by twenty. This count is the one-minute heart rate.
The eight-step system is a good starter system, and you will quickly learn what to look for in any suspect monitor strip.
Step One: Determine the Rate
To determine the atrial rate, measure the distance between P-P and determine the rate by one of the methods listed earlier.
To determine the ventricular rate, measure the distance between R-R.
Note: The rate of a normal sinus rhythm is 60-100 bpm.
Step Two: Determine the Rhythm
Is the rhythm regular or irregular?
To determine if the atrial rate is regular or irregular, measure the distance between two consecutive P-P intervals. Use a point from one P wave to the same point on the next P wave. Then compare this with another P-P interval. If the atrial rate is regular, the P-P interval will measure the same.
Determine if the ventricular rate is regular or irregular, and measure the distance between two consecutive R-R intervals. Use a point from one R wave to the same point on the next R wave. Then compare this with another R-R interval. If the ventricular rate is regular, the R-R interval will measure the same.
Is the rhythm regular? Irregular? Regularly irregular? Irregularly irregular?
Step Three: Evaluate P Waves
Are P waves present and uniform in appearance?
Are P waves upright (positive) in lead II?
Do P waves appear regularly before each QRS complex?
Is there more than one P wave before a QRS complex?
If irregular, is there an associated QRS?
Step Four: Evaluate the PR interval
If the PR interval is less than 0.12 or more than 0.20 seconds, conduction follows an abnormal pathway, or the electrical impulse is delayed at the AV node.
The normal PR interval is 0.12 to 0.20 seconds.
Is the PR interval consistent?
Step Five: Evaluate the QRS complex
Do the QRS complexes occur uniformly and look the same throughout the strip?
If the QRS measures .10 seconds or less, it is considered narrow and is presumed to be supraventricular in origin.
If the QRS complex is greater than .12 seconds or more, it is considered wide and presumed to be ventricular in origin until proven otherwise.
The QRS normally measures 0.04 to 0.10 seconds in duration. Determine if they are married to the P waves.
Step Six: Evaluate the T Wave
Are T waves present?
Are T waves smooth and rounded?
Do they have a normal amplitude of 0.5 millivolts or less?
Is the deflection the same as the preceding QRS?
Is there a relationship between any ectopy and the T wave?
Step Seven: Evaluate the QT Interval
Is the duration from 0.36 to 0.44 seconds?
Step Eight: Evaluate Other Components
Is the ST segment elevated? Depressed? Sloping or scooped?
The normal electrical flow through the heart originates in the SA node > AV node > bundle of His > left and right bundle branches > Purkinje fibers, with mechanical cells stimulated along the way. Therefore, the primary pacemaker is the SA node and has an inherent rate of 60-100 bpm. The SA node has the highest level of automaticity; however, escape pacemakers exist.
Escape pacemakers are cells that will initiate a heartbeat should the faster normal pace fail to descend along the standard conduction pathway. Escape cells exist in the AV junction and the ventricles (Burns & Buttner, 2024c).
The AV junction is the AV node and the non-branching portion of the bundle of His. The pacemaker cells in the AV junction are located near the non-branching portion of the bundle of His.
The AV node should only generate an impulse if the SA node does not function at its normal rate. The AV node fires electrical impulses at a slower rate of 40-60 bpm.
Table 4: Case Study One
Your colleague slaps this 12-lead down in front of you, saying, "What do you make of this? It does not look right somehow, yet our artificial intelligence that reads the EKGs/ECGs keeps spitting it out as 'abnormal, beyond system parameters'."
The client is a 68-year-old male who was brought in after collapsing on a golf course. Lab panels indicate mildly decreased sodium and potassium levels, with other results within reference ranges. Vital signs: Blood pressure 142/94 millimeters of mercury (mmHg), pulse - 48, respiratory rate - 20, O2 saturation - 97%. The client is alert and grumpy.
Image 12 : Case Study 1 EKG/ECG
Here is what you see: This is a bradycardia (heart rate of 45 bpm). It is regular. QRS complexes are narrow. No regular P waves are present, yet no flutter or fibrillating atrial waves are visible.
Disclaimer: There are two possibilities present. I prefer the first and only noticed the second while reviewing sources. Discerning between what is evidentiary and alternate actualities is why health care is considered an art, as well as a science.
Let us see what you think.
1. Sinus arrest is observed, accompanied by a junctional escape rhythm in which the retrograde P wave is concealed within the QRS complex, indicating simultaneous excitation of both the atria and ventricles.
2. There is exceptionally fine atrial fibrillation (which is usually only seen in long-lasting atrial fibrillation that has been present for many years).
Since the rhythm is regular, it could then not be a bradyarrhythmia in atrial fibrillation, but a junctional escape rhythm in atrial fibrillation and 3rd degree AV block.
Clinical decision = Allow me to be direct, in medical cardiology, as well as other branches of health provision, if the client is not actively expiring, then there is time for consults.
The client needs a consultation. If he remains stable, what is recommended is a Holter monitor at home and on the golf course; if unstable, sequential 12-leads would allow comparative views of cardiac activity with workup for a pacemaker.
The colleague was right to ask the opinion of someone else, especially if they are not sure of the rhythm or need to double-check what AI was reading. While a Holter monitor will be beneficial, the client should also be referred to cardiology, as the blood pressure was elevated and the pulse was low.
Ventricular pacemakers in the bundle branches and the Purkinje network will become the initiating pacemaker if the AV node cannot function. The inherent ventricular rate is 20-40 bpm.
This ventricular pacemaker occurs when an electrical impulse is delayed, blocked, or both in one or more portions of the conduction system. In contrast, the impulse is conducted normally through the rest of the conduction system. The results are a delayed impulse entering cardiac cells in which the normally conducted impulse has depolarized. If they have repolarized sufficiently, the delayed impulse will again depolarize the cardiac cells prematurely, thus producing unwanted ectopic beats and rhythms.
EKGs/ECGs are all about depicting the energy use of the heart. To get a standardized view of electrical flow, the "angle" from which the current flow is viewed is essential. A standardized placement pattern of EKG/ECG lead wires must be used to get consistent and usable data.
It is crucial to recognize that these underlying pacemaker sites and abnormal conduction patterns directly influence the appearance of an EKG/ECG and the interpretation of its waveforms. Any disruption along the conduction pathway—whether due to escape rhythms, premature beats, or reentry circuits—can alter the timing, morphology, and sequence of the electrical signals picked up by EKG/ECG leads. Accurate lead placement and awareness of the heart's intrinsic electrical hierarchy are therefore central to effective cardiac monitoring, diagnosis, and treatment.
Understanding EKG/ECG lead placement begins with an appreciation for the heart's complex rhythm generation and propagation. Each lead provides a unique perspective on the cardiac cycle, capturing the sum of electrical activity as it moves through the myocardium. A thorough grounding in the physiology of pacemaker cells, conduction pathways, and rhythm disturbances forms the basis for interpreting what is seen on the EKG/ECG tracing.
Let us get this clear and out of the way. The industry standard in healthcare is the 12-lead EKG/ECG. That is not what is used for monitoring a client. For ongoing client care, including pre-admission work by emergency responders, a standard three-lead configuration of foam-backed sticky electrodes is used.
Image 14: Einthoven's Triangle
We begin with three standard leads, add three augmented leads, and finish with six precordial leads for a complete 12-lead EKG/ECG. William Einthoven developed the practical EKG/ECG in 1902, earning a Nobel Prize, and his triangle, now called the Standard Limb Leads, remains central to recording heart activity in leads I, II, and III (Lee, 2025).
Lead I:
The positive electrode is placed just below the left clavicle.
The negative electrode is placed just below the right clavicle.
The neutral or grounding electrode is placed on or close to the left leg (typically placed on the left side, below the left pectoral).
Provides information about the left lateral wall of the chest.
Lead II:
The positive electrode is placed near the left leg (typically placed below the left pectoral muscle).
The negative electrode is just below the right clavicle.
The neutral or grounding electrode is just below the right clavicle.
Provides information about the inferior wall of the heart.
Common in cardiac monitoring because the position of view for this lead is close to the heart's actual conduction pathways.
Lead III:
The positive electrode is at the left pectoral muscle (instead of the traditional left leg).
The negative electrode is just below the left clavicle.
The neutral or ground electrode is placed just below the right clavicle.
Provides information about the inferior wall of the heart.
Using the same placement of three-electrode pads and a little fancy math, we can get different views of the electrical activity in the heart. Known as augmented limb leads, unipolar limb leads, or just unipolar leads, they can create an augmented theoretical null point in the center of Einthoven's triangle, allowing a view of the absolute potential in each electrode (Horoba, 2025).
Sounds a little esoteric? Well, it is all about the angle, or vector, from which you are looking at the heart. Think about standing at the end of an extremity, right arm, left arm, or the feet, lying side by side. Now squint up at the heart along that axis. Electric waves moving away from your position will have a positive amplitude on the EKG/ECG strip. The waves are moving toward you, a negative deflection. Electrical events that do neither will be minimized nor blended into the baseline (Horoba, 2025).
The augmented leads are named aVR, aVL, and aVF. "A" for "augmented," "V" for "voltage," then "Right," "Left," and "Foot." The leading "A" can be lower case or capitalized, though the lower case is correct.
Lead aVR:
The augmented unipolar right arm lead is oriented toward the cavity of the heart.
Electrical current from the heart is traveling towards the right arm.
All deflections of the EKG/ECG, P, QRS, and T should be negative in this lead.
Lead aVL:
The augmented unipolar left arm leads are oriented toward the heart, facing the anterolateral aspect of the left ventricle.
Electrical current from the heart is traveling towards the left arm.
Lead aVF:
The augmented unipolar left leg lead (feet). It is oriented toward the inferior surface of the heart.
Electrical current from the heart is traveling toward the feet.
Image 16: Augmented EKG/ECG Leads
Standard leads, plus augmented leads, make up the first six of a 12-lead EKG/ECG. Surprise! These first six share one important characteristic: they all view the heart from the frontal plane, as though the client is lying prone and their heart flat on the top of a table we are looking across. Oh, if we could only see the heart's activity from the horizontal plane, as though we were looking straight through our client!
Well, with math, we can. Welcome to the six precordial leads.
The precordial, or chest leads, view the heart's electrical conduction from a straight face-to-face view. These leads, referred to as "V" leads, are the horizontal plane, unipolar leads.
Lead V1:
It is placed in the fourth intercostal space just to the right of the sternum.
Anterior view of the right ventricle and right atrium.
Faces the heart cavity.
Provides an electrical view of the right ventricle.
QRS is mostly negative in this lead.
Lead V2:
It is placed in the fourth intercostal space just to the left of the sternum.
Anterior view.
Provides a good view of electrical activity in the right ventricle.
QRS is mostly negative.
Lead V3:
Placed exactly halfway between the positions of lead V2 and V4.
View of the heart's sternocostal surface.
Lead V4:
It is placed in the fifth intercostal space at the mid-clavicular line.
Septal view and left ventricle.
QRS is mostly positive.
Lead V5:
It is placed at the same horizontal level as V4 on the anterior axillary line.
Lateral view of the septum and left ventricle.
QRS is mostly positive.
Lead V6:
It is placed at the same horizontal level as V4 and V5 on the mid-axillary line.
Lateral view of the septum and left ventricle.
QRS is mostly positive.
Image 17: Precordial Chest Leads
There are various uncommon, used for special situations, lead patterns out there. Just so you are aware, here are the most common of the uncommon heart leads.
MCL, or modified chest leads, are different placements of electrodes used to focus on premature beats, bundle branch blocks, or supraventricular rhythms. It is sometimes difficult to discern whether a fast rhythm is supraventricular tachycardia (SVT) or ventricular tachycardia (VT); a modified lead may come into play (Francis, 2016).
MCL1:
It is a variation of V1, where the negative electrode is situated below the left clavicle, close to the left shoulder. Positive electrode in the fourth intercostal space to the right of the sternum and ground just below the right clavicle.
Useful in assessing the anterior wall of the left ventricle and conduction through the ventricles.
QRS appears mostly as negative deflections.
This lead is useful in assessing the width of the QRS complex to differentiate SVT from VT.
MCL6:
This variation is a deviation of chest lead V6.
The negative electrode is placed just below the left clavicle. The positive electrode is placed in the fifth intercostal space at the left midaxillary line (like lead V6) while the ground is placed below the right shoulder.
This lead may be used as an alternative to MCL1 for the same purposes and views of the low lateral wall of the left ventricle while monitoring ventricular conduction changes.
An EKG/ECG strip displays a single lead reading from client monitors, while a 12-lead sheet provides diagnostic information from twelve different perspectives. Abnormalities unnoticed in one lead may be visible in another.
Quick trick. However, different manufacturers of EKG/ECG machines produce various-looking EKG/ECG sheets; a standard print format is employed.
Table 5: Relative Positions of 12-Lead Results on EKG/ECG Paper
Lead I
Lead aVR
Lead V1
Lead V4
Lead II
Lead aVL
Lead V2
Lead V5
Lead III
Lead aVF
Lead V3
Lead V6
Long length focus lead, either designated by an operator or picked by a machine.
The default long lead tends to be standard limb Lead II.
Knowing this allows you always to recognize which lead you are looking at on any given EKG/ECG sheet.
Regularity is a fundamental factor for functional heart rhythms. The rate of conduction, whether it is too slow or too fast for adequate blood perfusion, is also essential for effective cardiac function. Additionally, the composition of each heartbeat is important; effective pumping ensures that blood moves forward efficiently, while ineffective efforts can reduce cardiac output. Assessment focuses on P waves, QRS complexes, and T waves to evaluate these functions quickly and effectively.
Regularity is measured using EKG/ECG graph paper. Typically, a single off-timing beat is notable but not usually concerning. Multiple irregular beats may indicate underlying issues and should prompt further evaluation. This applies to beats originating from the atria, junctional region, or ventricles.
The heart's pumping ability depends on its rate. The standard is 60–100 bpm; rates below this range can reduce cardiac output, while higher rates can compromise consistency of blood flow. The origin of any rate abnormality is significant, as the heart attempts to compensate for impaired pumping capacity.
Inadequate filling of the heart chambers can lead to a rapid decline before ventricular contraction fails, potentially resulting in congestion. Abnormal QRS complexes are indicative of incomplete contraction. What is observed electrically on the monitor corresponds to physiological outcomes that impact patient health. Early detection, investigation, and appropriate treatment are associated with improved outcomes.
This discussion will cover some of the primary arrhythmias commonly encountered when evaluating cardiac rhythms. The focus will include several frequently observed arrhythmias, particularly those originating in the upper myocardium. Subsequent parts of this series, which focused on Advanced EKG/ECGs, will address more complex examples and arrhythmia arising from other regions of the heart.
The term "aberrant" originated in the emerging field of cardiology a century ago. Over time, it has experienced varying levels of usage due to differing definitions (Well Wisp, 2025). Periodically, the term has been revived and then fallen out of favor, reflecting ongoing debate within the discipline. In this context, we adopt a broad definition: any presentation that appears abnormal or noteworthy (Sissons, 2024). While this definition may prompt discussion and divergent opinions, the fluctuating use of the declarative term "aberrancy" reflects its contested place in medical terminology.
Table 6: Definition: Aberrancy
Aberrancy on an EKG/ECG refers to the abnormal conduction of electrical impulses in the heart, resulting in irregular patterns that may be associated with various cardiac conditions. Recognizing these patterns supports accurate diagnosis and management.
Aberrancy can result from mechanisms such as bundle branch block or accessory pathways. Bundle branch block occurs when there is a delay in one branch of the bundle of His, while accessory pathways provide additional electrical connections, altering normal conduction.
Aberrancies can reflect underlying structural or functional cardiac abnormalities. Detecting aberrant conduction patterns on an EKG/ECG allows healthcare providers to evaluate cardiac function and plan appropriate interventions.
Heart patterns involve rhythm, rate, and aberrancy (Nickson, 2024). This overview examines several EKG/ECG patterns that are regarded as being visually important for medical professionals, focusing on their relationship to normal rhythm, rate, and aberrancy. More advanced heart rhythms will be discussed in a subsequent course.
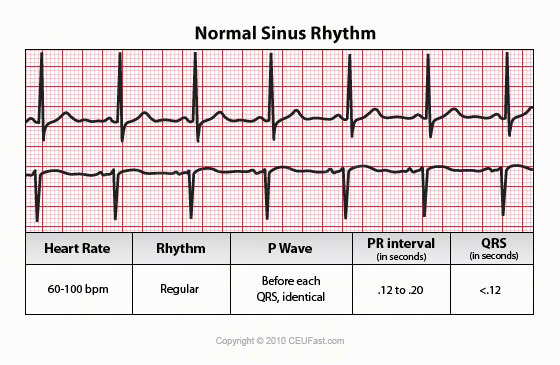
What we as health professionals always want to see is a healthy sinus rhythm. When normal heartbeats are triggered by the SA node in the upper right atrium of the heart, what is produced is a regular rhythm of 60 to 100 bpm. This normal sinus rhythm adjusts to the body's needs, increasing or decreasing with activity or rest (Goldberger et al., 2013).
Sinus bradycardia is a regular rhythm originating from the SA node that is slower than 60 bpm. In sinus bradycardia, the P vector on the EKG/ECG will be consistent with a SA node origin.
Just as a reminder, a normal SA-produced P wave will show right atrial depolarization followed rapidly by left atrial depolarization. A distinctive high-to-low, top-to-bottom, atrial polarization gives rise to the stereotypical upright P inflection in leads I, II, and aVL, with a negative P deflection in the aVR lead (Singh, 2024).
Image 19 : Sinus Bradycardia, Lead II and V1
The slower conduction of sinus bradycardia may be due to a normal response to sleep or deep breathing in a well-conditioned athlete. Abnormal drops in rate could be caused by diminished blood flow to the SA node, vagal stimulation, hypothyroidism, increased intracranial pressure, or pharmacologic agents, such as digoxin, propranolol, quinidine, or procainamide.
Consider a slow heart rate if dizziness, fatigue, or syncope occur. Sinus bradycardia may have no symptoms.
A 12-lead EKG/ECG or a wearable heart monitor is considered diagnostic of sinus bradycardia.
Too fast of a heart rate while at rest creates problems with heart filling. The large chambers of the heart, the ventricles, require a full second to fill with blood in anticipation of pushing it out on its voyage through the body. A contraction rate of greater than 100 bpm with the electrical stimulus arising from the SA node and the presence of evenly paired P with QRS waves qualifies as sinus tachycardia (Henning & Krawiec, 2023).
Image 20: Sinus Tachycardia, Lead II and V1
There are several types of tachycardia. Sinus tachycardia is a regular cardiac rhythm that meets normal sinus rhythm standards, apart from being too fast. Greater than 100 bpm in a resting adult, faster than 150 bpm in infants, up to around six years old.
Do not be misled. Too quick a heart rate, even with a normal conduction mechanism, can be problematic. Strokes, heart failure, and the risk of heart attack from increased cardiac demands can accompany sinus tachycardia.
Sinus tachycardia may result from stress, exercise, pain, fever, pump failure, hyperthyroidism, caffeine, nitrates, atropine, epinephrine, isoproterenol, nicotine, electrolyte imbalances, fatigue, blood loss, and other situations that place stress on the body.
Tachycardia means fast. Supraventricular means the origin of the impulses is from above the cardiac ventricles. These high and fast aberrant rhythms tend to be clustered together due to their shared diagnostics.
SVT is a group of regular fast rhythms characterized by narrow QRS complexes and high heart rates. Please note that while atrial fibrillation and atrial flutter share a high conduction origin point and fast rate, they are typically irregular rhythms and will be discussed later.
According to Farkas (2025), women are at least twice as likely as men to experience SVT. The symptoms of SVT are often misinterpreted as panic attacks; employing EKG/ECG patches may assist in confirming the diagnosis. Polyuria is noted as a less common symptom.
SVT may occur spontaneously or result from triggers like excessive energy drink intake, cocaine use, sepsis, dehydration, or elevated intracardiac pressures. Cardiac conditions such as heart failure, myocardial infarction, pulmonary embolus, and valve disorders can also induce SVT.
Treatments include vagal maneuvers (carotid massage, Valsalva maneuver, cold immersion) and medications that reduce AV node sensitivity, such as adenosine, verapamil, esmolol, calcium channel blockers, digoxin, amiodarone, beta-blockers, and diltiazem (Gugneja, 2024).
Table 7: Definition: Frog Sign
The "frog sign" is a clinical clue seen during atrioventricular nodal reentry tachycardia (AVNRT), where atrial contractions against a closed tricuspid valve produce strong jugular pulsations, known as "cannon waves," creating a billowing appearance in the neck.
Although not an EKG/ECG finding, cannon waves may cause deviations on a 12-lead EKG/ECG.
Cannon waves and, less often, the frog sign can also appear in VT, but a wide QRS complex usually reduces back pressure and makes the frog sign less evident.
Junctional rhythms are impulses that originate from the AV node, also referred to as the junction. These rhythms occur when the SA node, which is typically the primary pacemaker of the heart, does not function effectively. For classification purposes, rapid junctional rhythms are often grouped with SVTs. This section examines impulses that begin at the junction.
A brief overview of the cardiac conduction system: The SA node, located in the right atrium, is the main pacemaker, generating electrical impulses at a rate of 60–100 bpm. These impulses travel to both atria through the internodal pathways, causing coordinated atrial contractions that move blood into the ventricles. The signal then proceeds to the AV node, situated between the atria and ventricles, and continues down the bundle of His to the right and left ventricles. From the bundle of His, the impulse spreads to the Purkinje fibers within the ventricular myocardium, resulting in ventricular contraction and blood ejection throughout the body.
If necessary, the AV node can function as an alternative pacemaker when the SA node fails, with an inherent rate of 40–60 bpm, which is slower than the SA node. In some cases, the AV node may increase its rate above that of the SA node, resulting in junctional tachycardia, where the heart rhythm is governed by the fastest depolarization cycle.
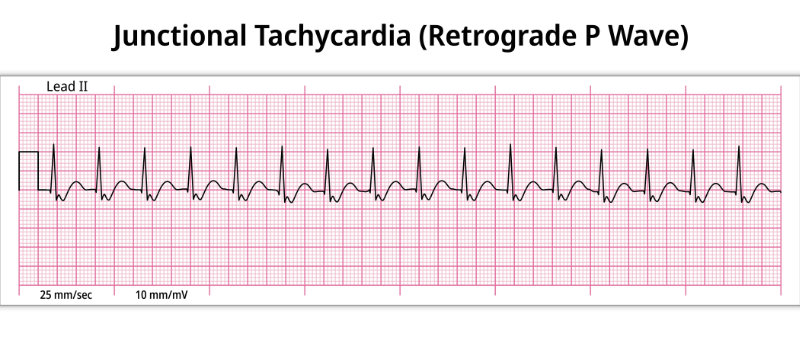
Table 8: Junctional Tachycardia
Image 21: Junctional Tachycardia
Heart Rate
Rhythm
P Wave
PR Interval
QRS
> 200
Regular
P may be immediately before, follow, or be buried in QRS. May be inverted or retrograde
Short
Narrow < 0.12
(Scanlon, 2025a)
The P wave immediately before the Q can be seen on lead II. This negative P wave inflection is common for all junctional rhythms as the depolarization pacing point originates within the AV node, as the depolarization wave must travel upwards into the atria simultaneously, or the closest thing to concurrent, as the aberrant firing wave heads to the His bundle and ventricles (Scanlon, 2025a).
Rhythms sourced from the AV node are characterized by rate (Hafeez et al., 2025).
Junctional bradycardia rate is < 40 bpm.
Junctional rhythm runs 40-60 bpm.
Accelerated junctional rhythm runs from 60-100 bpm.
Junctional tachycardia > 100 bpm.
Junctional rhythms will have a regular RR interval, and as a signature sign, one of the following P wave variations:
Absent P waves are a sign that the AV node is sending depolarization impulses simultaneously to the atria and ventricles.
Inverted P waves occur when the AV depolarization reaches the atria before the ventricles.
Post-QRS P waves are visible when the AV depolarization reaches the ventricles first.
Table 9: Case Study Two
Gimenez, a 43 y/o Sudanese African mother of seven, had family members drop her off at the clinic door, then drive away, leaving her alone. She lurched inside, complaining of dizziness, shortness of breath, and weakness that had come and gone for the last several months.
Desk staff helped her into a wheelchair and called for your assistance.
Still drying your hands from the restroom, you call for oxygen, vital signs, and an EKG while pointing towards the nearest open exam room.
Image 22: Case Study 2 EKG-ECG
Blood pressure is 98/76 mmHg, pulse is irregular, respirations are 32, O2 Saturation is 78%. The client is awake, not fully alert, and her nailbeds are cyanotic with clubbing.
So, what is that rhythm?
Clinical decision time = Based on the present EKG/ECG and clinical base, you have the oxygen continued, an IV started, and a paramedic with heart monitoring transport summoned to the emergency transport to a full-service emergency department. While this is in process, you hit the phone and speak with the receiving physician to establish continuity of care. Well done!
Starting oxygen and an IV immediately was the correct call, as the client could decompensate even more. Continuity of care should be established, and the client should be seen as soon as possible.
Atrial fibrillation (AFib or AF) is considered the most common type of treated cardiac arrhythmia, affecting 40 million people worldwide (Minneapolis Heart Institute Foundation, 2025).
Rhythmic atrial contraction contributes 20% to 30% of the heart's output (Scanlon, 2025b). Disruption of normal SA node function by irritation, inflammation, or other factors can lead to disorganized atrial depolarization, resulting in fibrillation or atrial quivering. AFib significantly compromises cardiac output, particularly in older adults or individuals with comorbidities, as effective atrial contractions are essential for optimal ventricular filling. Although many individuals with AFib remain asymptomatic, those who do experience symptoms may report sudden fatigue, dyspnea, dizziness, or chest pain, often remarking on the unexpected irregularity of their heartbeat.
Image 23: AFib
Complications of AFib can be serious.
Blood clots – Due to ineffective pumping, blood can churn and pool in the atria, allowing thrombus, embolus, or clots to travel through the blood to various parts of the body.
Stroke – Should an embolus reach the brain, a blood flow blockage or stroke may occur.
Cognitive impairment or dementias – Studies support that AFib is associated with increased rates of cognitive impairment, Alzheimer's, and vascular dementia.
Heart attack – Women and African Americans show an elevated risk of heart attack associated with AFib.
Heart failure – The fast and uneven beating of the heart raises the risk of heart failure.
Sudden cardiac death – Sudden stoppage of cardiac function and AFib sadly walk hand in hand.
So please, do not think of AFib as just a quivering nuisance.
Table 10: Atrial Fibrillation
Image 24: AFib EKG
Heart Rate
Rhythm
P Wave
PR Interval
QRS
Atrial rate usually > 400
Irregular
No identifiable P waves
None
Narrow < 0.12
(Scanlon, 2025b)
The QRS rate of AFib will be all over the scale. Fast, then slower, then well, chaotic. It is so unpredictable that there are, in some viewpoints, three diverse types of AFib.
This is when runs of fibrillation tend to last longer than one week or until delivery of a small electric cardioversion shock or medication, resetting the heart back to a normal sinus rhythm (McDermott, 2025).
In hemodynamically unstable patients, emergent electrical cardioversion to restore normal sinus rhythm is indicated. For stable patients, a careful evaluation of whether to pursue rhythm control or rate control should be conducted. Pharmacological interventions should be tailored to the individual patient's needs, and certain surgical options may also be considered. Additionally, anticoagulation therapy should be anticipated to reduce the risk of thromboembolic events.
Atrial flutter is the quintessential atrial tachyarrhythmia. Not the most common, yet it is the one a clinician tends to point out to students and state, "Now this is an atrial arrhythmia!"
The distinctive saw-tooth pattern of the atrial flutter waves is characteristic of multiple P waves successfully constricting the atria, yet only penetrating to the ventricular myocardium every second, third, or more atrial depolarizations. Pay special attention to leads II, III, aVF, and V1 to pick out the distinctive atrial flutter waves. Atrial rates will typically run 252-320 bpm. In comparison, ventricular rates will range around 120-160 bpm, with the most common ventricular rate in atrial flutter being 150 bpm, due to a phenomenon known as 2:1 AV block.
Table 11: Atrial Flutter
Image 25: Atrial Flutter
Heart Rate
Rhythm
P Wave
PR Interval
QRS
The atrial rate is usually 250-320, and the ventricular rate 120-160
Regular
Saw-tooth P waves
Varies
Narrow < 0.12
(Prutkin, 2024)
Here is a blowup of V1 from above. Note the choppy ocean waves of P in relation to the QRS complex. Most are 3:1, three P waves to each QRS. However, there is a variable ratio of P:QRS as we examine more of this lead. We would therefore call this atrial flutter with variable conduction (Prutkin, 2024).
The large muscular chambers of the lower heart push a pulsing stream of blood out into the body. When a command to contract signals fails to arrive from the primary pacemaker, the sinus node, escape cells within the ventricles step up to emit electrical depolarization waves that contract the ventricular myocardium.
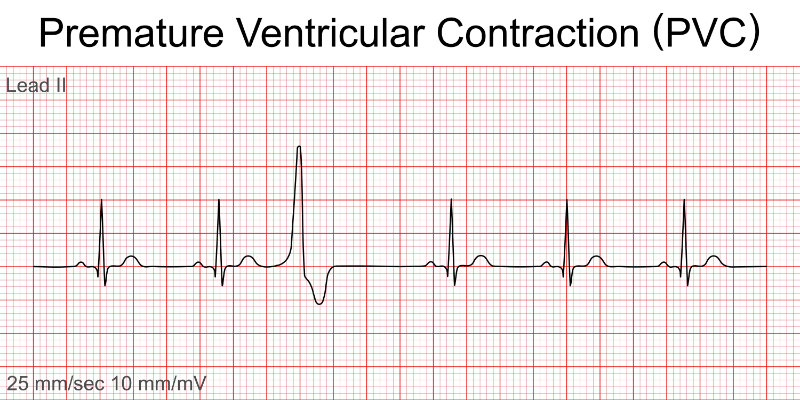
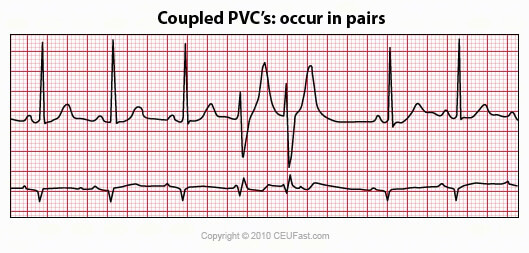
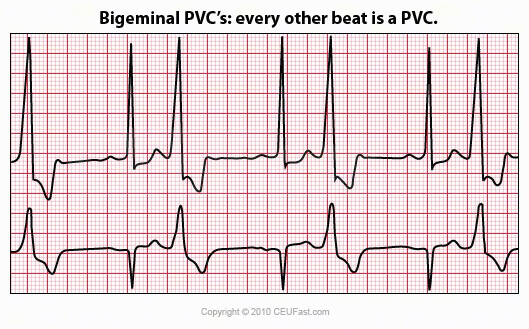
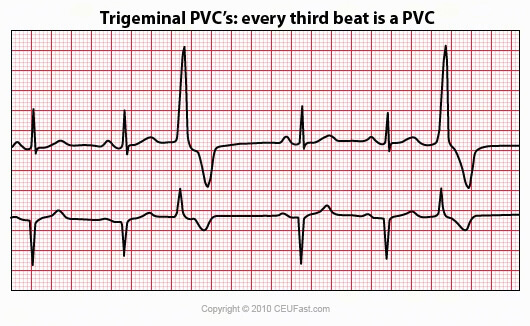
Any early, untimely cardiac contraction arising from the ventricles is a premature ventricular complex (PVC). Many, if not most, people who have the occasional PVC are completely unaware of them. Those who do perceive them tend to describe the sensation as a skipped beat or pounding heart. Both are accurate descriptions of what is brought about by the hemodynamic changes of sudden, early ventricular contractions (Sattar & Hashmi, 2025).
Table 12: Premature Ventricular Complexes
Image 27: PVCs, Lead II
Heart Rate
Rhythm
P Wave
PR Interval
QRS
60-100
Irregular
Disassociated from the abnormal QRS
None on Abnormal QRS
Wide on abnormal beat > 0.12
(Sattar & Hashmi, 2025)
Rate: Atrial and ventricular rate dependent upon the underlying rhythm.
Rhythm: Irregular due to PVC. If PVC is sandwiched between two normal beats, it is called interpolated, and the overall rhythm will be regular.
P waves: A P wave is not associated with the PVC.
PR interval: None with the PVC because the ectopic beat originates in the ventricles.
QRS: > 0.12 wide and bizarre. The T wave frequently occurs in the opposite direction of the QRS complex. If the QRS is negative, the T wave is usually upright; if the QRS is positive, the T wave is usually inverted.
PVCs may be due to stress, activity, valvular disease, coronary artery disease, heart attack, caffeine, antihistamines, or decongestants. The PVC may produce a weak pulse, and it is the client who should be treated, not the monitor.
VT, also known as V-Tach, is a regular fast heart rate originating from an area of ventricular irritation. Short bursts of rapid ventricular contractions may not endanger a person. However, the less efficient circulation of blood from prolonged bouts can be life-endangering.
Characteristic findings indicating VT are tachycardia at >100 bpm, wide QRS complexes > 0.12, and AV dissociation. VT can be monomorphic, originating from one electrical excitation, where all QRS complexes look alike, or polymorphic, where multiple spots of electric stimulation are firing within the ventricles. Polymorphic VT is seen when each QRS shows a different morphology.
Bursts of VT lasting under 30 seconds are referred to as non-sustained V-Tach, while stretches longer than 30 seconds are referred to as sustained V-Tach.
Symptoms of VT fall along the lines of reduced cardiac output and include hypotension, dizziness, syncope, cardiogenic shock, and cardiac arrest (Whitaker et al., 2023).
Table 13: Ventricular Tachycardia
Image 32: VT, 12-Lead
Heart Rate
Rhythm
P Wave
PR Interval
QRS
100-250
Regular
Absent or not related to rhythm
NA
> 0.12
(Whitaker et al., 2023)
Rate: Ventricular rate 100-250 bpm; atrial rate tends not to be discernible.
Rhythm: Atrial not discernible, ventricular regular.
P waves: May or may not be present. If present, they have no set relationship with the QRS complexes. P waves may appear between the QRS complexes at a rate different from that of the VT.
PR interval: None.
QRS Complex: Wide, > 0.12 milliseconds (or three small EKG/ECG squares). It is often difficult to differentiate between the QRS and T wave. Three or more PVCs in a row at a rate of 100 per minute are referred to as a "run" of VT. There may be a long or a short run. A client may or may not have a pulse. If it is unclear whether a regular, wide QRS tachycardia is VT or SVT, treat the rhythm as VT until proven otherwise.
Note: VT can occur in the absence of apparent heart disease.
T wave: Difficult to separate from QRS.
QT interval: Should be 390-450 milliseconds. If longer, be on alert for Torsades de Pointes.
Other Components: The presence of three or more consecutive wide QRS complexes at a rate equal to or greater than 100 per minute, accompanied by evidence of AV dissociation, confirms the diagnosis of VT. If the rapid QRS complexes are morphologically like those observed during the patient's normal sinus rhythm, SVT should be considered.
VT may arise as an early or late complication of myocardial infarction, or in association with cardiomyopathy, valvular heart disease, myocarditis, electrolyte disturbances, or post-cardiac surgical procedures (Whitaker et al., 2023).
VF, or V-fib, is regarded as the most important shockable arrhythmia during cardiac arrest (Burns & Buttner, 2024d). This is where the lower heart chambers quiver rather than constrict. Too many electrical polarization signals, arriving much too rapidly, reduce the strong rhythmic myocardial contractions to chaotic spasms. VF is a lethal arrhythmia resulting in rapid loss of consciousness, no pulse, and cardiac death in the absence of treatment.
VF is considered a medical emergency. Despite high-quality medical intervention, approximately 50% of individuals experiencing VF will not survive due to cardiac arrest or its complications (Fogoros, 2025). In the absence of prompt treatment, clinical death typically occurs within minutes when VF is present as the predominant rhythm. Even in cases where resuscitation is successful, patients may suffer from hypoxic brain injury and other neurological impairments, necessitating ongoing monitoring and potentially long-term care.
VF is often associated with structural damage to the heart. Factors that can irritate or inflame the Purkinje cells of the ventricles may contribute to the onset of multiple rapid stimuli, leading to VF. Myocardial infarction, for instance, is linked to a higher incidence of VF during the acute phase of myocardial injury (Scanlon, 2025c). Most occurrences of VF after myocardial infarction take place early when tissue ischemia is most severe.
Various conditions have been identified in association with VF, including electrolyte imbalances (such as hypokalemia, hyperkalemia, and hypomagnesemia), acidosis, hypothermia, hypoxia, cardiomyopathies, a family history of sudden cardiac death, congenital QT abnormalities, and alcohol use.
Image 33: VF, Lead II
Rate: Rapid and disorganized.
Rhythm: Irregular and chaotic.
P waves: Absent, but may be recognized among the chaos.
PR interval: Not measurable.
QRS complex: Composed of fibrillatory waves, with wide, irregular oscillations of the baseline.
T wave: Not measurable.
QT interval: Not measurable.
Other components: Coarse VF is where most waveforms are 3 mm or wider. Fine VF is where most waveforms are less than 3 mm.
Asystole or flatline is synonymous with ventricular standstill and death. Asystole is usually associated with prolonged circulatory insufficiency and cardiogenic shock. It could also be drug-related, hypothermia-related, and at times reversible.
Asystole is the disappearance of all ventricular electrical activity, meaning the absence of all physiological pumping actions. Be aware that means there may still be atrial activity. Atrial activity in the presence of ventricular standstill, e.g., P wave asystole, may respond to electrical pacing (Kryvenko, 2025).
Table 14: Fading to Asystole
Image 34: Fading to Asystole
When asystole occurs, oxygenated blood flow to all organs stops almost immediately. The brain is highly dependent on a constant supply of oxygen, making it especially sensitive to deprivation. Irreversible damage to brain cells may begin within four to six minutes without oxygen.
On an EKG/ECG monitor, this is represented by a straight, flat, or slightly undulating line, indicating the absence of the standard waveforms associated with heartbeats. This condition is distinct from other types of cardiac arrest, such as VF or pulseless VT, where electrical activity remains and may respond to defibrillation.
Our heart is an exquisitely crafted pumping machine whose myocardial muscle cells move thousands of liters of blood every single day. These wonderful engines are controlled by rhythmic electrical pulsations originating from natural pacemaker cells located in the apex of the heart itself. So well designed are our hearts that redundant backup pacemaker points exist to take over should our primary pacing points fail. Ironically, this problem is one reason we need a consistent method of examining the heart's electrical activity to see what is happening in our hearts.
Electrocardiography is the scientific method used to record and analyze the electrical activity of the heart. The sinus node's pacemaker cells initiate a process of polarization and depolarization, generating an electrical impulse that propagates through electrically sensitive tissue pathways. This depolarization triggers myocardial contraction—first in the atrial chambers, followed by the ventricular muscle—which facilitates the movement of blood throughout the body. Each phase of the electrical conduction pathway produces distinct waveforms on the isoelectric baseline of an EKG/ECG monitor strip.
The atrial depolarization from the sinus node is portrayed by the P wave. The movement of the electric pulse through the atrial tissue to the AV node and the His-Purkinje fibers causes atrial contraction. This is the PR interval. As the depolarization enters and spreads widely into the cardiac ventricles, a QRS complex is projected onto the EKG/ECG. The brief period of recovery occurring between ventricular cell depolarization and repolarization is seen as the ST segment, with the T wave signaling full repolarization. Always one for a bit of mystery, our heart can throw up a wave we call U, which follows the T and precedes the P. We have no idea why, yet life has plenty of new discoveries waiting for us, even in areas we congratulate ourselves for knowing so well.
Placement of the positive and negative cardiac monitors gives us special angles for viewing the heart's electrical activity. Twelve special lead placements compose a cardiac 12-lead EKG/ECG, the diagnostic standard. How we evaluate what is going on in the heart using an EKG/ECG strip requires a system. Some of the steps of a winning system include looking at the heart rhythm, heart rate, P waves, PR Intervals, QRS complexes, ST segment, T wave, QT duration, and then anything special, such as delta or U waves.
Using a systematic approach, we can determine where the rhythm originates from the atria, junction, or ventricles, if it is normal, fast, or slow, if there are unusual beats, if the entire rhythm is unusual and perhaps an unwanted arrhythmia, or if unusual spots of excitement, electrical blockage, chaotic electrical fibrillation, or lack of electrical activity are present.
Not only can we see and diagnose natural cardiac functions, but we can also look at the functioning of implanted cardiac pacemaker devices to determine if their function is appropriate or failing. A failing artificial pacemaker can show as under-sensing, failure to capture, or output failure.
When you want to see the heart of health issues, remember, EKG/ECG!
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
ACLS Medical Training. (n.d.). The Basics of ECG. ACLS Medical Training. Visit Source.
Answers. (2024). How many times does blood flow through the human body? Answers. Visit Source.
Bhattacharyya, S., & Munshi, N. V. (2020). Development of the Cardiac Conduction System. Cold Spring Harbor perspectives in biology, 12(12), a037408. Visit Source.
Biology Insights. (2025). P Wave on ECG: Normal and Abnormal Morphology. Biology Insights. Visit Source.
Burns, E. & Buttner, R. (2024a). Premature Ventricular Complex (PVC). Life in the Fastlane. Visit Source.
Burns, E. & Buttner, R. (2024b). Q Wave. Life In The Fastlane. Visit Source.
Burns, E. & Buttner, R. (2024c). Ventricular Escape Rhythm. Life in the Fastlane. Visit Source.
Burns, E. & Buttner, R. (2024d). Ventricular Fibrillation (VF). Life In The Fastlane. Visit Source.
Cadogan, M., & Buttner, R. (2025). Osborn Wave (J Wave). Life In The Fastlane. Visit Source.
Chaudhry, R., Miao, J. H., & Rehman, A. (2022). Physiology, Cardiovascular. In StatPearls. StatPearls Publishing. Visit Source.
Demyanets, S. (2024). The Heart: The Engine in the Center of the Vascular System. Learning Materials in Biosciences, 51–73. Visit Source.
Douedi, S., & Douedi, H. (2023). P wave. In StatPearls. StatPearls Publishing. Visit Source.
Farkas, J. (2025). Supraventricular Tachycardia (SVT). EMCrit. Visit Source.
Fogoros, R. N. (2025). Ventricular Tachycardia Causes, Symptoms, and Treatment. VeryWell Health. Visit Source.
Francis, J. (2016). ECG monitoring leads and special leads. Indian pacing and electrophysiology journal, 16(3), 92–95. Visit Source.
Goldberger, A. L., Goldberger, Z. D., & Shvilkin, A. (2013). Sinus and Escape Rhythms. Goldberger’s Clinical Electrocardiography, 114–120. Visit Source.
Grider, M. H., Jessu, R., & Kabir, R. (2023). Physiology, Action Potential. In StatPearls. StatPearls Publishing. Visit Source.
Gugneja, M. (2024). Paroxysmal Supraventricular Tachycardia Medication. Medscape. Visit Source.
Hacking, C. (2025). Wolff-Parkinson-White syndrome. Radiopaedia. Visit Source.
Hafeez, Y., Wollard, K., & Grossman, S. A. (2025). Junctional Rhythm. In StatPearls. StatPearls Publishing. Visit Source.
Heaton, J., & Goyal, A. (2023). Atrioventricular Node. In StatPearls. StatPearls Publishing. Visit Source.
Helmenstine, A. (2025). Parts of the Heart – Human Heart Anatomy and Worksheets. Science Notes. Visit Source.
Henning, A., & Krawiec, C. (2023). Sinus Tachycardia. In StatPearls. StatPearls Publishing. Visit Source.
Horoba, M. (2025). Electrocardiograms- The ECG Leads. Cardio Curious. Visit Source.
Kashou, A. H., Basit, H., & Chhabra, L. (2022). Physiology, Sinoatrial Node. In StatPearls. StatPearls Publishing. Visit Source.
Kashou, A. H., Basit, H., & Malik, A. (2023). ST Segment. In StatPearls. StatPearls Publishing. Visit Source.
Kryvenko, A. (2025). Asystole. Healthy Life. Visit Source.
Kunwar, P. (2024). 10 amazing facts about the human heart. Scientify. Visit Source.
Laske, T. G., Iaizzo, P. A. (2024). Anatomy and Physiology Overview of the Cardiac Conduction System. In: Iaizzo, P. A., Eggen, M. D., Iles, T. L. (Eds.), Cardiac Electrophysiology Methods and Models (pp. 89-117). Springer, Cham. Visit Source.
Lee, S. (2025). Mastering Einthoven's Triangle in Biomedical Engineering. Number Analytics. Visit Source.
Lome, S. (n.d.a). QRS Complex. Healio. Visit Source.
Lome, S. (n.d.b.). QT Interval. Healio. Visit Source.
MacKinnon, L. & Haque, O. (2025). Internal Balance of Potassium. Teach Me Physiology. Visit Source.
McKenna, W. (2024). Arrhythmogenic right ventricular cardiomyopathy: Anatomy, histology, and clinical manifestations. UpToDate. Visit Source.
Minneapolis Heart Institute Foundation. (2025). Understanding Atrial Fibrillation: Symptoms, Risks, and New Hope for Treatment. Minneapolis Heart Institute Foundation. Visit Source.
Mussigbrodt, A., Bethencourt, M. H., Vergier, R., Blidar, M., & Alfie, A. (2025). Leaping to diagnosis: The frog sign as a key clue in AVNRT. Clinical Case Reports, 13(3), e70248. Visit Source.
Nickson, C. (2024). ECG Rhythm Evaluation. Life In The Fastlane. Visit Source.
Nora Eccles Harrison Cardiovascular Research & Training Institute. (n.d.). Demystifying Electrophysiology: Understanding the Basics of Cardiac Rhythm Management in Heart Health. The University of Utah. Visit Source.
Prutkin, J. (2024). Control of ventricular rate in atrial flutter. UpToDate. Visit Source.
Ripa, R., George, T., Shumway, K. R., & Sattar, Y. (2023). Physiology, Cardiac Muscle. In StatPearls. StatPearls Publishing. Visit Source.
Sattar, Y., & Chhabra, L. (2023). Electrocardiogram. In StatPearls. StatPearls Publishing. Visit Source.
Sattar, Y., & Hashmi, M. F. (2025). Premature Ventricular Complex. In StatPearls. StatPearls Publishing. Visit Source.
Scanlon, A. (2025a). Do Junctional Rhythms Have P Waves? Cardiovascular Disease Hub. Visit Source.
Scanlon, A. (2025b). How Does Atrial Contraction Occur? Cardiovascular Disease Hub. Visit Source.
Scanlon, A. (2025c). How Does Myocardial Infarction Cause Ventricular Fibrillation. Cardiovascular Disease Hub. Visit Source.
School of Health Sciences. (n.d.). The U Wave. The University of Nottingham. Visit Source.
Singh, A. (2024). On An Ecg Waveform, What Does The P Wave Represent? Shanti Nursing Home. Visit Source.
Singh, A. (2025a). How To Use An Ecg To Calculate Pulse? Shanti Nursing Home. Visit Source.
Singh, A. (2025b). Why Is “Ekg” An Acronym For Electrocardiogram?. Shanti Nursing Home. Visit Source.
Sissons, B. (2024). What to know about Afib with ECG aberrancy. Medical News Today. Visit Source.
Stanley, S. (2025). The Coronary Circulation. Teach Me Anatomy. Visit Source.
Wei, X., Yohannan, S., & Richards, J. R. (2023). Physiology, Cardiac Repolarization Dispersion and Reserve. In StatPearls. StatPearls Publishing. Visit Source.
Well Wisp. (2025). What Does Aberrancy Mean On An ECG? Well Wisp. Visit Source.
Whitaker, J., Wright, M. J., & Tedrow, U. (2023). Diagnosis and management of ventricular tachycardia. Clinical medicine (London, England), 23(5), 442–448. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.