This course will be updated or discontinued on or before Thursday, December 10, 2026
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
CEUFast, Inc. is an AOTA Provider of professional development, Course approval ID#011515. This distant learning-independent format is offered at 0.20 CEUs Intermediate, Categories: Professional Issues
AOTA does not endorse specific course content, products, or clinical procedures. AOTA provider number 9757.
CEUFast, Inc. (BOC AP#: P10067) is approved by the Board of Certification, Inc. to provide education to Athletic Trainers (ATs).
CEUFast, Inc. is recognized by the New York State Education Department's State Board for Physical Therapy as an approved provider of physical therapy and physical therapist assistant continuing education.
Outcomes
≥92% of participants will know the types of medical errors, risk factors for medical errors, and strategies for prevention.
Objectives
After completing this continuing education course, the participant will be able to:
Identify the different types of medical errors.
Describe the different types of adverse events.
Identify at least three risk factors for medical errors.
Summarize at least two organizational-level medical error prevention strategies.
Evaluate at least two medical error prevention strategies at the individual level.
Summarize at least three strategies to prevent medication errors.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Medical errors account for a portion of patient deaths every year, impacting patients, families, clinicians, health facilities, and other health professionals. Unfortunately, some medical errors lead to patient harm and increase the likelihood of patient morbidity and mortality. There are several prevention measures health professionals can take to potentially prevent medical errors from occurring in their practice.
This course aims to equip learners with the different types of medical errors and the potentially harmful and nonharmful events that can result from them. It also reviews the risk factors for medical errors, reporting mechanisms, and analysis of medical errors and their potential impacts on healthcare providers. Lastly, it summarizes many prevention strategies at the individual and organizational level for specific types of medical errors.
There are various definitions of medical errors by organizations or healthcare facilities. Most follow the Institute of Medicine’s definition from its book called To Err is Human: Building a Safer Health System, which is: “the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim” (Institute of Medicine, 2020). However, over the past decades, the definition has expanded to include errors that may or may not cause patient harm (Patient Safety Network, 2019).
In the United States, it’s reported that medical errors are the third leading cause of death. Some studies have found that more than 200,000 hospitalized patient deaths are from preventable medical errors each year (Rodziewicz et al., 2024).
In 2023, The Joint Commission reports that there were 1,411 sentinel events, or adverse events causing patient harm, in the U.S. Around 18% of these events resulted in patient death, and 8% led to permanent harm or loss of function to the patient. The majority of these reported sentinel events occurred in a hospital setting. Furthermore, these sentinel events were reported voluntarily, so these figures likely only represent a small portion of adverse events (The Joint Commission, 2024a).
While medical errors can potentially harm an individual, they also increase healthcare costs. Some studies suggest that medical errors leading to adverse events and hospital-acquired infections cost an estimated $20 billion to upwards of $45 billion annually respectively (Rodziewicz et al., 2024).
Many of these medical errors can lead to adverse outcomes for the patient or others involved. Again, a medical error could have caused or potentially caused harm to a patient. According to the Patient Safety Network (2019), these adverse event categories that result in patient harm include:
Preventable: This is where a prevention strategy was not used to prevent the adverse event from occurring. An example is failing to scan a medication or confirm the patient’s identity before administering a medication.
Ameliorable:An ameliorable event is when an event is not preventable but might have been less harmful if patient care had been different. For example, if a piece of equipment fails and a patient is administered too much medication. If the nurse or healthcare personnel fail to respond appropriately to the medication overdose, then this is considered an ameliorable adverse event.
Negligence: This occurs when a healthcare professional’s care is below the standard of patient care. An example of negligence during abdominal surgery is if a surgical instrument is left inside the patient’s abdomen and is not detected until later. The healthcare team members who are responsible for the surgery and counting the instruments are considered negligent since they fall below the standard of operating room procedures.
The Agency for Healthcare Research and Quality (AHRQ) also defines events that do not cause patient harm, which are:
Near miss:An error or harmful situation occurred, but the patient was not harmed. For example, a patient was given the wrong blood pressure medication but was not harmed.
Error: Any act that can potentially harm a patient, like a human, medication, diagnostic, or surgical error (Patient Safety Network, 2019).
Sentinel Events
In addition, the Joint Commission further defines adverse severe events as sentinel events. Sentinel events are patient safety events that result in patient death or permanent or severe harm (The Joint Commission, 2024a). Some examples are patient suicide, patient falls, procedure and surgical errors, and blood transfusion incompatibilities (Rodziewicz et al., 2024).
There are many types of medical errors. Some of the most common include:
Table 1: Types of Medical Errors
Type of Error
Example
Surgical Errors: These errors have the highest likelihood of patient mortality and account for around 75% of surgeon malpractice cases (Singh et al., 2024).
The wrong surgery is performed or at the incorrect site, such as on the wrong side (right or left).
Diagnostic Errors: These errors are common in primary care settings and account for around 40,000 to 80,000 patient deaths or injuries each year (Singh et al., 2024).
Failure to discuss results within a timely manner and communicate with the patient or a misdiagnosis. Common conditions where a misdiagnosis may occur are cancers and neurological and cardiac conditions (Rodziewicz et al., 2024).
Medication Errors: Some reports also suggest medication errors occur in about 6.5 of every 100 acute hospitalizations (Tariq et al., 2024). Further details about medication errors can be found below.
The wrong medication or dosage is administered. Interestingly, these are the most common preventable medical errors (Singh et al., 2024).
Equipment Failures: Approximately 5000 types of medical devices are used worldwide, so device-related errors are inevitable (Rodziewicz et al., 2024).
A piece of equipment malfunctions or a hardware issue arises. This also involves medical devices, like pacemakers, stimulators, pumps, etc. (Rodziewicz et al., 2024).
Hospital-acquired Infections: Some reports suggest that 1 in every 20 hospitalized patients will have a hospital-acquired infection (Singh et al., 2024).
When a patient becomes infected with a pathogen within a hospital setting when receiving care for another health condition (Rodziewicz et al., 2024).
Patient Falls: Falls account for a large portion of medical errors. It’s estimated that around one-third of patients 65 years and older fall annually (Singh et al., 2024).
A patient falls when standing up to go to the bathroom.
Communication Errors: Communication errors can be caused by disruptive patient behavior, cell phones or pagers, cultural differences, personality differences, language barriers, and socioeconomic variables such as literacy and education (Rodziewicz et al., 2024).
Failure to report results, communication between healthcare staff and providers, etc. Written communication, such as using non-standard abbreviations and incorrectly ordering or labeling specimens, also falls within this category (Singh et al., 2024).
Medication errors can occur anywhere in the medication administration process, ranging from ordering and documenting to dispensing and administering. However, most medication errors occur during prescribing or ordering, which accounts for around 50% of medication errors. The second most common type of medication error that occurs is during the administration stage. There are many types of medication errors, with some including (Tariq et al., 2024):
Incorrect prescribing.
Medication is not ordered, or the patient does not receive the ordered medication.
Medication is administered at the wrong time (this is especially important for intravenous antibiotics or medications, like levothyroxine, that should be taken at a specific time to maximize absorption).
Incorrect dose, preparation, or rate (for intravenous medications or pumps).
Incorrect route.
Incorrect patient.
Failure to document a medication allergy.
Contraindications to the medication.
Using expired products.
Failure to monitor a medication’s potential effects is also a medication error. For example, oral antifungals can increase liver function values, which should be monitored before and during treatment. Failure to do so is a medication monitoring error (Tariq et al., 2024).
Human error accounts for a large portion of medical errors. This includes both active and latent errors or failures. Active errors are those that directly involve a healthcare professional causing harm during patient care (Rodziewicz et al., 2024). For example, accidentally programming an intravenous pump incorrectly or prescribing a medication to a patient who is allergic to that medication. Active errors can be further divided into errors of planning or errors in execution. Some errors in planning are mistakes in rules or knowledge. Errors in execution are slips and lapses (Sameera et al., 2021).
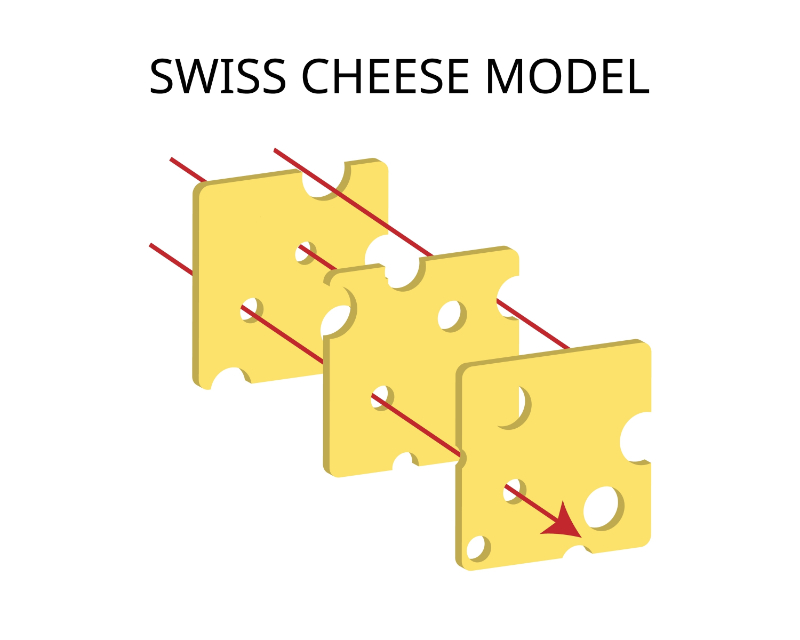
Latent errors are intrinsic or organizational problems that cause patient harm. Sometimes, these can go unnoticed for long periods of time before actually causing patient harm. An example of a latent error is using faulty equipment or a healthcare organization using different types of equipment (like multiple types of intravenous pumps or ventilators) that can cause confusion on how to operate them (Rodziewicz et al., 2024).
The “Swiss Cheese Model” helps depict how medical errors occur, specifically human errors, but may include other types of errors as well. Imagine each layer as a slice of Swiss cheese with holes. Errors or failures are the holes in the Swiss cheese. If several layers of holes line up, then this creates the opportunity for an error or adverse event to occur. It’s important to note that not every hole in the Swiss Cheese Model leads to medical error or accident (Wiegmann et al., 2022). So, a latent failure and an active failure combined represent an opportunity for a potential adverse event. For example, if an organization uses multiple types of intravenous pumps and a nurse incorrectly programs the pump, this can potentially lead to patient harm.
Many individual factors of healthcare professionals can contribute to effective healthcare delivery and patient care. One study surveying more than 700 critical care nurses found that nurses with poor mental and physical well-being reported more medical errors than those nurses who were healthy (Melnyk et al., 2021). Some individual factors that may potentially contribute to medical errors include (Wiegmann et al., 2022):
Mental state: The healthcare worker’s cognitive or emotional state, distractions, stress, or workload. For example, if a person is more stressed, they may feel pressured to hurry tasks and potentially make mistakes. In addition, professional burnout is a major contributing factor to medical errors. Several studies have linked physician burnout to an increased likelihood of significant medical errors (Li et al., 2023).
Physical state: An individual’s physical well-being can also potentially lead to medical errors. Factors like physiological stress, fatigue, and sleep disruptions can impact patient care. Furthermore, several studies have identified nurse fatigue as a major contributing factor to medication administration errors. Fatigue leads to decreased cognition and lack of attention in nurses, which reduces patient safety (Bell et al., 2023).
Patient Communication: Communication with the patient is another source of medical errors, especially medication errors. Factors like language barriers, medical jargon, and incomplete histories (confirming allergies, history, etc.) can poorly impact patient care and lead to errors (Tariq et al., 2024).
Healthcare team members must be able to communicate effectively and work as a team to provide quality patient care. There are some instances where team factors can influence patient care and possibly impact patient care, such as (Wiegmann et al., 2022):
Coordination of care:Sometimes, improper patient coordination can lead to medical errors. For example, a patient is transferred from another facility, and the patient’s home medications are not verified with the prior facility. Another example is if a patient is transferred from outpatient urgent care, where an x-ray or another diagnostic test was already performed. The test and results were not communicated to the receiving facility (like the emergency room), so the receiving facility reorders the same test.
Team Communication: Team communication is a large portion of quality patient care. If there is a communication breakdown, then this can potentially lead to medical errors. For example, if a patient becomes unresponsive and a team member starts cardiopulmonary resuscitation (CPR) and tells another team member to call for help (dialing 911 or calling a code). However, the other team member did not hear the request, so he just grabbed an oxygen tank when it was already available. This is a medical error and delays patient care since the rest of the medical team was not alerted promptly (Wiegmann et al., 2022).
Several organizational factors can affect healthcare delivery. Some of these factors include (Wiegmann et al., 2022):
Culture: Organizational culture and decision-making can affect (increase or decrease) the risk of medical errors.
Operational resources: Limited resources, like healthcare staff or equipment, can increase the risk of medical errors. Additionally, scheduling and staff assignments can impact patient care.
Operational processes: Certain operational processes, like policies and procedures, can prevent medical errors. Conversely, these policies and procedures may be altered due to a previous medical error within the policy or procedure (Wiegmann et al., 2022). Lack of standardized protocols can potentially lead to medication errors (Tariq et al., 2024).
Supervision: Lack of supervision, especially for those in training, can result in medical errors. Conversely, thorough professional guidance and engagement may reduce the likelihood of medical errors.
Many environmental factors can affect patient safety and potentially cause medical errors. Some of these include (Wiegmann et al., 2022):
Equipment: Certain types and designs of medical equipment and devices can leave opportunities for medical errors to occur.
Surrounding environment: A healthcare professional’s surroundings can also increase the likelihood of medical errors. Factors can include noise, distractions, clutter, lighting, and room layout. For example, poor lighting when drawing up a medication, like insulin, could lead to a potential underdose or overdose if the nurse cannot correctly see the number labeled on the syringe.
Other factors can also increase the likelihood of medical errors. For example, older patients are more likely to have medication errors. Moreover, patients who are 65 and older are almost twice as likely to have a medication-related hospital admission than people who are younger than 65. Polypharmacy increases risk, as patients who take five or more medications are 30% more likely to experience a medication error. Multiple prescribers (providers who prescribe a medication) also increase the risk of medication errors, as well as patients with multiple comorbidities (Tariq et al., 2024).
Reporting an incident, whether a near-miss or adverse event, is an essential component of improving quality care and patient outcomes. By reporting a medical error, healthcare organizations can investigate its possible root cause(s), which can lead to future error prevention. Investigating past medical errors can lead to organizational policy and procedure changes and improved quality of care (Sergi & Davis, 2023).
Many healthcare organizations have established incident reporting systems, which help detect, track, and manage patient safety events. An incident reporting system is an avenue where a healthcare professional can voluntarily report a patient safety event, whether near-miss or harmful. An effective and robust incident reporting system must have essential components, including reporting to the proper channels and within a timely manner, as well as a plan for reviewing reporting and next steps. Also, the majority of these systems ensure confidentiality with the identity of the incident reporter known (Patient Safety Network, 2019).
Data and information collected from incident reports may vary per healthcare organization but typically includes (Patient Safety Network, 2019):
Patient or individual affected
Date and time of incident
Location of the incident
Report of the incident (usually free text)
Witnesses of the event (if any)
Response to the incident or event
Condition of the person affected (including if any known injury or harm occurred)
Again, information collected varies per organization; some may ask for medical record numbers, treatments administered (if any), pictures, and other information. The information in these reports should be factual and objective. Examples of instances where an incident report may be submitted are:
Patient fall
Medical device or equipment malfunction
Patient complaint with the care they received
Medication administration errors
Medication reactions
Some laws and regulations at the state level require that healthcare organizations submit their incident reporting information. Many healthcare safety organizations and medical equipment companies collect information from incident reports, although the information submitted is often voluntary. For example, the Joint Commission accredits many healthcare systems, and a requirement of accreditation is mandatory incident reporting of sentinel events. It also requires that a root cause analysis be performed within 45 days of the event (The Joint Commission, 2024a).
Many healthcare organizations use the root cause analysis method to investigate and determine the underlying cause of the adverse or sentinel event. The method helps identify possible training, operational, and resource deficiencies that led to the near-miss or adverse event (Singh et al., 2024). Interestingly, many organizations use the Swiss Cheese Model to guide their root cause analysis since it identifies gaps or failures that led to the event or patient harm (Wiegmann et al., 2022). If submitted, some of the information in a root cause analysis is taken from the incident report.
Each health organization has a specific interprofessional team assigned to perform a root cause analysis on a reported event. Often, team members include individuals from risk management, quality improvement, clinical governance, clinical managers, key stakeholders, and other healthcare professionals. During a root cause analysis, the investigation attempts to discover any underlying deficiencies that caused the event. A root cause analysis often focuses on organizational or system-wide deficiencies and processes instead of the individual level. Interestingly, for organizations accredited by the Joint Commission, this organization provides a framework for healthcare systems to use when performing a root cause analysis. The framework poses questions to consider and investigates areas like communication, system processes, environmental factors, staffing, etc. After a root cause analysis, an action plan to resolve or correct the identified underlying deficiencies is discussed and performed (Singh et al., 2024).
Another method to identify medical errors is the failure mode effect analysis. This method seeks continuous quality improvement of processes to help identify and prevent medical errors. First, a process is selected, usually known as a problem or one to potentially cause problems. A team is assembled to analyze the process and identify potential or actual failures. After identifying these deficiencies, the team works on designing and implementing processes to prevent these from occurring. Last, the team evaluates the effectiveness of the implemented actions (American Society for Quality, 2024).
Unfortunately, there are instances where medical errors are not reported, especially in near-miss situations where a patient was not harmed. Several studies have been conducted to uncover some barriers to why medical errors are unreported. One study by Aljabari and Kadhim (2021) systematically reviewed 30 studies reporting barriers to medical errors by nurses, physicians, and other healthcare providers from 2000 to 2020. This study found that the most reported barrier (63%) to medical errors was fear of consequences, followed by a lack of feedback at 27% and work culture at 27% (Aljabari & Kadhim, 2021). Other studies have found that fear, lack of employee support, and staff training are potential barriers. Thus, it’s vital for healthcare team members to feel supported and have a positive workplace culture that avoids blaming staff but instead facilitates preventative measures, reporting, and further education (Asgarian et al., 2021).
Medical errors can psychologically affect nurses, physicians, and other healthcare providers. Most of these psychological effects are perceived as negative, where the healthcare member is traumatized by the event. They may experience an array of emotions, ranging from stress and guilt to depression and shame. Some healthcare providers blame themselves and further question their clinical judgment and decision-making skills, negatively impacting their self-esteem and confidence in patient care. Some healthcare professionals may develop post-traumatic stress disorder (PTSD) if they are involved in an adverse event (Zangaro et al., 2023).
Furthermore, medication errors can negatively impact healthcare providers and have serious consequences, like license suspension or revocation, lawsuits, and other legal problems (Tariq et al., 2024).
Reducing the likelihood of medical error begins with identification and prevention. There are many strategies to prevent and reduce medical errors from occurring, which are further detailed below.
As human error is a common cause of medical errors, there are some techniques to implement to help reduce these types of errors. For example, professionals in the operating room should avoid working long shifts and limit unnecessary conversations or noises that can serve as a distraction. Also, cognitive aids and tools should be used whenever possible. Examples of these include checklists, algorithms, mnemonics, and computerized prompts. Using checklists and algorithms in electronic health records can reduce human error (Sameera et al., 2021).
When considering diagnostic errors, the “rule of three” helps with human cognitive errors. The rule of three states that a healthcare provider should count to three and consider other possibilities and alternatives. This method helps the provider pause their thought and reasoning process. Another alternative to using the rule of three is to consider at least three alternatives when making a diagnosis and treatment (Sameera et al., 2021).
Healthcare organizations should have an incident reporting system to aid with recording medical errors and sentinel events. Again, this reporting system helps identify and survey medical errors. Simply having an incident reporting system can help identify possible deficiencies in healthcare systems and lead to organizational change and prevention measures.
Most healthcare organizations have a risk management department that helps with safety monitoring and reporting. This department is largely responsible for pinpointing risks early and performing ongoing risk assessments. A risk assessment helps identify possible medical errors, estimates their risk, and evaluates the potential implications of medical errors. The risk management department is also typically involved in reviewing incident reports and performing root cause analysis to determine deficiencies in patient care that lead to medical errors. A health system’s risk management is also involved in policy and procedure creation and management.
This area of expertise uses many tools to assess risk. Some of these include:
Performing a risk analysis.
Determining which risk assessment tools to implement into patient practices.
Cost-benefit analysis of risk assessment tools and implementation (Ferdosi et al., 2020).
Furthermore, risk managers use several techniques in their roles, which include:
Avoidance: Avoidance, also known as the forcing function, eliminates the potential for loss (i.e., an error). Avoidance entails designing policies, processes, or even equipment to virtually prevent an adverse event from occurring. An example is not allowing a nurse to override the withdrawal of certain medications (e.g., rocuronium—paralytic) from a medication dispensing machine. Another example is only stocking one type of supply or certain supplies in a unit.
Retention:In some cases, keeping a portion of the risk or the entire risk is more cost-effective for the health system. For example, a health organization may attempt to move to one manufacturer and a certain concentration of a life-saving medication to reduce errors. However, sometimes, the supply chain may be interrupted, and this medication may become unavailable from a single manufacturer. Instead, risk management may choose to have another supplier of this medication since it is a lifesaving medication. Thus, the health system is absorbing some risk since two medications can have different concentrations depending on the manufacturer, which potentially leaves an opportunity for a medical error to occur.
Spreading: Some risk management departments may choose to spread the risk of loss. For example, extra equipment may be stored in a separate facility to spread the risk of loss. A hospital may store extra IV pumps and oxygen tanks in a nearby outpatient facility or administration building so that if a fire were to occur inside the hospital or a mass causality event occurred, the hospital would have backup supplies readily available.
Loss Prevention and Reduction: Health systems and risk managers attempt to minimize the severity and frequency of risk. Loss prevention helps to reduce the likelihood of loss but does not reduce its severity. An example is a medication dispensing machine with a lockout mechanism for when a pain medication is withdrawn and administered to a patient; the nurse cannot withdraw the medication again until the preprogrammed amount of time has passed. This is also common with scheduled medications within the patient’s record. Some health facilities do not allow nurses to withdraw or administer medications with the electronic health record unless it is within the patient’s scheduled time window. Loss reduction entails reducing the severity of the damage. A common example is the implementation of standardized protocols and procedures, like procedural checklists.
Transfer: In many scenarios, health systems and risk managers choose to transfer or negotiate a portion of risk, usually by a contract. An example is insurance companies and contracts with healthcare providers and facilities. Health systems have large medical liability and property insurance policies to help transfer some of the risk. For instance, if there is a medical malpractice lawsuit against a health facility, the healthcare company will likely have a liability insurance policy that helps transfer a portion of its risk to the insurance company (California State University, Fullerton, 2022).
Healthcare employee training and competency is a crucial component of preventing medical errors. Many professionals might be unaware of evidence-based safety practices and strategies to reduce medical errors without education. Therefore, many healthcare accreditation organizations require health systems to provide initial and annual safety training to all their employees. Promoting system-wide skill development and ongoing competency can also minimize the risk of medical errors. Staying current with best practices through continuing medical education and reviewing recent research can reduce medical errors. Therefore, health systems should consider and offer their employees educational and professional development opportunities (Gemmete, 2024).
Furthermore, many healthcare professionals are unaware of what constitutes a medical error. Therefore, training and competency in medical error recognition are essential, as well as training regarding incident reporting (Tariq et al., 2024).
Some medical errors come in the form of billing and coding practices, which can result in further downstream consequences, like claim denials, penalties, fraudulent claims, underpayment, and overbilling. Implementing medical coders and reviewers, who are individuals trained in medical billing, can help reduce the risk of billing issues and errors. In addition, this is where proper training of these medical coders and providers plays a vital role in medical error prevention. Proper billing and coding help reduce legal and financial risk and potential penalties and fines.
Utilizing simulation-based and virtual reality training are other avenues to reduce medical errors. Some studies have found that virtual reality clinical skills training can reduce medical errors by around 40%. Virtual reality and simulation-based training are helpful ways for clinicians to practice their skills without causing direct patient harm. Learners can receive feedback about their mistakes and consider them moving forward. These types of training may also be useful for providers who have not been able to practice their skills or procedures simply due to no patient having needed the type of skill or procedure (Kennedy et al., 2023). Thus, healthcare institutions should consider adopting virtual reality and simulation training to aid with skill competency and ongoing training.
Using artificial intelligence (AI) in a healthcare setting is another way to promote patient safety and decrease the likelihood of medical errors. Some health systems’ electronic medical records have AI embedded to assist with identifying potential patient safety issues. Some AI systems can assist with patient monitoring, like minimizing unnecessary alarms, monitoring pulse and blood pressure, and analyzing false cardiac arrhythmias. While others can identify incidents, review patient feedback, and extract valuable information from safety reports. Many of these avenues are a way to prevent and reduce medical errors. However, further research is still needed on efficacy and training and its true impact on patient safety (Choudhury & Asan, 2020). Regardless, many health systems have adopted artificial intelligence into their organizational practices to identify potential medical errors and safety concerns.
Changing the workplace culture of incident reporting is key to error prevention. Health organizations should instill a safety culture and discuss incident reporting and its benefits to the health system. Instead of discussing errors at an individual level and their consequences, they should discuss how errors are a system-wide issue and can lead to changes in processes. Professionals should feel empowered by reporting possible incidents or adverse events that occur (Tariq et al., 2024).
Furthermore, health organizations should instill a culture of transparency, non-punitive measures, and accountability. Through these actions, organizations and team members can learn from their mistakes and prevent future or further harm. This, in turn, promotes a culture of safety and data-driven preventative measures (Zangaro et al., 2023). Also, many health systems are shifting from a pay-for-performance model to a value-based model to promote quality and safety practices(Sameera et al., 2021).
In addition, organizations should support a company culture of effective teamwork. They should strengthen teamwork by providing adequate resources, especially communication and staffing. Providing team-building and development opportunities can potentially reduce the rate of staff turnover, thus promoting proper staffing levels and improving patient safety (Zangaro et al., 2023).
Healthcare professional burnout is a major factor contributing to medical errors, and addressing burnout is of utmost importance. Therefore, employers should look for areas of improvement within their organization. Factors such as inadequate staffing levels and staff engagement in safety can negatively impact employees and contribute to burnout. Instead, health systems should promote staff engagement in safety concerns and resolutions and have adequate resources and staff. In turn, employees are more likely to support one another, collaborate, communicate, and gain knowledge of safety protocols (Zangaro et al., 2023). Additionally, health employers should support available mental health resources, invest in health prevention, and promote a culture of inclusion(Office of the General Surgeon, 2024).
A portion of addressing burnout also falls on the individuals themselves. Health professionals should know their physical, mental, and spiritual well-being. Moreover, they should be aware of the signs of burnout (Office of the General Surgeon, 2024), some of which include:
Depersonalization (feeling disconnected)
Emotional exhaustion
Low sense of accomplishment
Emptiness
Withdrawal
Neglecting personal needs
Depression
Anxiety
Other physical symptoms, like fatigue, headaches, irritability, and sleep problems, may develop (De Hert, 2020). Health professionals should instill self-care practices to prevent burnout, including promoting physical and mental health. They should seek mental health counseling and address any underlying mental well-being problems. Stress management and participating in small group discussions with others experiencing similar symptoms can be helpful (Razai et al., 2023).
There are several ways to reduce and prevent surgical errors from occurring. Simply adopting and completing standardized checklists before, during, and after surgery can help reduce errors. In addition, performing a surgical time-out (pause), including all team members, before any procedure helps ensure the correct patient, surgery, and surgery site. If the patient is undergoing multiple surgeries or has multiple surgeons, a time-out is performed for each. Marking the patient’s surgical site, especially for surgeries involving laterality (right or left), before surgery is also an error prevention method. Operating rooms also use measures like counting instruments before and after surgery to reduce surgical errors and foreign body retention (Rodziewicz et al., 2024).
Several strategies exist to prevent diagnostic errors. Tools like diagnostic algorithms, checklists, and differential diagnosis considerations can help reduce diagnostic errors. The provider should be encouraged to think critically about possible differential diagnoses and should foster interdisciplinary communication and collaboration. Additionally, simulation-based training and performance feedback can decrease the likelihood of diagnostic errors (Rodziewicz et al., 2024).
There are many ways to prevent medication errors from occurring. Some of these include (Sameera et al., 2021):
Barcode scanning:The patient’s armband and medication barcode must be scanned before administering a medication. The computer system displays the correct information and can alert the health provider if something is incorrect.
Standardized arrangement: Medications are arranged in a standardized fashion in certain areas, like the operating room, crash carts, or medication rooms, which helps to prevent medication errors. This is helpful during emergencies so the provider can quickly recall where a medication is typically located.
Standardized medication dosages: Having standardized medication dosages and concentrations available is helpful, especially during emergencies. In an outpatient setting, emergency medications available in autoinjectors, like epinephrine, can also prevent medication errors. Prefilled syringes and infusion bags are also helpful.
Tall man lettering:Medications that sound alike or look alike use tall man lettering and bolding to help readily identify the medication. Examples are DOPamine versus DOBUTamine, hydrALAZINE versus hydrOXYzine, and traZODone versus traMADol (Sameera et al., 2021).
Computerized Physician Order Entry (CPOE) systems: Interestingly, CPOE systems are the most effective strategy for preventing medication errors. This system allows for real-time prescribing, and many CPOEs check for allergies, medication interactions, and duplicate medications and alert the prescribing provider.
Automated Medication Dispensing Machines: Many hospitals and large health systems implement medication dispensing machines. The nurse selects the patient and medication from the patient’s list of ordered medications. The machine dispenses the medication and also has certain lockout parameters.
Medication Reconciliation: Complete medication reconciliation, especially for new patients or during transitions in care, is vital to preventing medication errors. Documenting the dosage, route, and frequency of the prescribed medications is key, as is entering any over-the-counter medications or supplements the patient is taking.
Optimize Workflow:Measures to optimize health professional workflow should also be taken. This is a strategy any individual can use to prevent error. Minimizing interruptions and having a “distraction-free zone” are helpful ways to optimize workflow, especially during the preparation and administration steps of the medication administration process.
Limit Handwritten Prescriptions: Prescribing providers should limit the use of handwritten prescriptions whenever possible. If a prescription needs to be handwritten, the prescribing provider should approach it with caution, write the exact dosage, limit the use of abbreviations, follow decimal point rules, and avoid using trailing zeros.
Limit Verbal Orders: Prescribing providers should limit the use of verbal orders whenever possible since this is where communication and transcription errors may occur. If necessary, the person receiving the orders should repeat the order to the prescriber to confirm accuracy (Tariq et al., 2024).
Clinical Decision Support Systems: This support system is a tool for error prevention. Examples are computerized alerts, reminders, and prefilled order sets within an electronic health record.
Follow the Medication Rights: When administering a medication, the nurse or other health professional should use the medication rights, such as the right patient, dose, time, route, etc.
Use Smart Infusion Pumps: When administering intravenous medications, an infusion pump should be used instead of manually hanging an IV bag. Infusion pumps provide lockouts for certain medications and rates, which can help reduce errors.
Provide Patient Education: Whenever possible, educate patients about their medications. Include information such as the medication’s name, why they are taking it, side effects, and any special administration instructions (Patient Safety Network, 2019).
Equipment malfunctions are not limited to an inpatient setting but can also occur in an outpatient setting or a patient’s home. Design flaws and user errors are common causes of medical errors. Design flaws and device/equipment malfunctions should be reported to the manufacturer, as they can gather information to change equipment design, provide better instructions, or issue a recall.
In addition, health professionals operating the equipment must receive proper training about equipment use, safety measures, and protocols. Professionals should inspect the equipment regularly, and lines should be traced back to their connection points for intravenous equipment. Patients who have medical devices at home should receive proper equipment training and check their devices' function frequently (Rodziewicz et al., 2024).
Alarm parameters and functioning should be frequently checked on medical devices and equipment. Typically, health systems have policies and protocols for how often alarms and equipment should be checked and receive scheduled maintenance (Rodziewicz et al., 2024). Furthermore, The Joint Commission’s 2024 Hospital National Patient Safety Goals provide recommendations on alarm safety as improving the safety of alarm systems is a goal. Some instances where alarm safety should be considered are if alarms are off or inaudible. Narrow or broad alarm parameters can also be a safety concern. Suggested strategies to improve alarm safety include:
Identify alarm and monitoring systems that should be managed. Health organizations should seek input from multiple sources, such as employees, stakeholders, and managers.
Discuss whether the identified alarm system should have a noise or alert. This is a valuable step to reduce alarm fatigue.
Ensure the implementation of certain policies and procedures surrounding alarm and patient monitoring systems. These policies, especially if changed, should be reviewed with managers and team members affected by these policy changes.
Ensure alarm parameters monitoring frequency and policies are communicated to all team members. For example, suppose a policy is created for cardiac rhythm alarms and parameters to be checked at the start of the shift of the healthcare professionals; this must be communicated to the team members, managers, nurses, etc. (The Joint Commission, 2024b).
Many hospital-acquired infections (HAIs) result from improper hand hygiene and failure to wear proper personal protective equipment (PPE). Thus, common HAIs include catheter-associated urinary tract infections (CAUTIs), central-line associated bloodstream infections (CLABSIs), and other infections involving aseptic or sterile techniques. To combat HAIs, health organizations should consider changing employee hand hygiene behaviors through hand hygiene campaigns and regularly auditing hygiene practices. Other prevention strategies are minimizing the duration of indwelling catheter use as much as possible, antibiotic stewardship programs, and following certain infection measures (wearing PPE, frequently assessing wounds, and using chlorhexidine to cleanse catheter sites) (Rodziewicz et al., 2024).
Many healthcare systems implement fall prevention strategies within their facilities to aid patient safety. Using assessment tools, like the Morse fall scale, can reduce the risk of patient falls through early identification of patients at increased risk (Rodziewicz et al., 2024). Hospital systems may also implement universal fall prevention measures for every patient, such as wearing non-slip socks, door signage, patient wristbands, and patient and family education. Other strategies may include setting bed and chair alarms, implementing one-on-one sitters, and intentional patient rounding. Environmental modifications can also potentially help reduce falls, like bright lighting, placing the call light within patient reach, using special rooms for patients at high risk (i.e., near the nurses’ station), and moving the bed to the lowest position. All healthcare staff members should receive training on fall prevention and remain diligent with fall prevention measures (LeLaurin & Shorr, 2019).
Patient and family education is a key component of fall prevention in an inpatient setting, and it is just as important in outpatient and home settings. Health professionals should discuss best practices in all settings to reduce the likelihood of falls. These may include using assistive devices for ambulating, reviewing home medications, and wearing the correct shoes. Reducing clutter in the home, improving lighting, and removing rugs can decrease the chances of falling at home.
There are many strategies to reduce the chances of communication errors. Some of these include:
Using checklists: Implementing the use of checklists can help improve team communication and serve as a guide.
Time out: This method is commonly used in the operating room before surgery. The team pauses before surgery and confirms the patient, procedure, and site before beginning the procedure (Sameera et al., 2021).
SBAR: SBAR (situation, background, assessment, recommendation) is a common communication tool in many healthcare settings. The situation is where the healthcare professional introduces themselves and then explains the current problem or situation to the patient. Next, a brief patient background is provided, typically including the patient’s history, symptoms, and test results. Then, an assessment is provided, which provides objective data and a description of what the communicator thinks the problem may be. Last, the communicator provides their initial recommendations and receives orders or next steps in care. They repeat back the orders to confirm accuracy (Agency for Healthcare Research and Quality, 2019).
Call-back or repeat-back: As the name implies, this method simply repeats information to ensure accuracy. For example, a nurse receives verbal orders from a provider and then repeats the orders to confirm.
Alert phrases:Alert phrases that convey the seriousness or urgency of the situation can also be used as a communication technique. Examples are “this situation is serious,” “high alert,” or “code blue” (Sameera et al., 2021).
PACE:PACE (Probe, alert, challenge, escalate/emergency) is another communication tool used to express concerns, especially when speaking to superiors. At first, the individual can probe their concern to express feelings and raise awareness about the situation. Then, if this fails, they can be alerted by repeating the concern. Next, to challenge means to confront the person. Last, the person may need to escalate their concern by interrupting the other person, saying stop, or possibly taking over the task. When using this communication tool, the receiver must acknowledge the other’s concern to be considered effective (Sameera et al., 2021).
Another way to reduce the chances of a medical error is to document information within the patient’s medical record properly. The Nurses Service Organization (2024) offers a valuable list of do’s and don’ts of documentation, which can help guide proper documentation to reduce the potential for medical errors. Some of these include:
Ensure the correct chart is open and the patient is correctly identified. To verify the patient’s chart's accuracy, ask them their name and date of birth or verify the information on their patient armband.
Make sure that documentation reflects all aspects of the nursing process. For example, if a patient is hypertensive and requires an antihypertensive medication, make sure to document their blood pressure before and after administration within the medical record.
Provide accurate and complete descriptions. When possible, provide a timeline of events and include all relevant details and objective data.
When administering medications, chart at the time the medication was administered. Real-time documentation of medication administration is the best practice. If the health facility has barcode medication scanning, always try to use this feature instead of manually entering a medication administration in the medication administration record.
Always chart patient safety precautions and the time they were implemented. For example, if a patient is on seizure precautions, document that airway supplies are at the head of the bed and the bed’s side rails are equipped with padding. Another example is when documenting about a patient being ambulated. Documentation should include what safety equipment was used (ambulating with a walker, wearing non-slip socks, with a healthcare professional assisting, and they were wearing a gait belt).
Accurately record all phone calls and conversations with physicians and other health professionals. Make sure to include the time, information provided to the person, and their response and orders (if any). For example, a unit secretary notifies a cardiologist about a cardiology consult for a newly admitted patient. The unit secretary should document the time, name of the person/provider contacted, and the information provided (patient, type of consult, etc.) and then notify the nurse.
Ensure documentation is accurate and thorough. When documenting, provide an accurate timeline of events and objective findings. For example, a patient is unresponsive and pulseless, and a code blue is called. The nurse should immediately note the time and begin compressions. During documentation, the nurse should document the time the patient was found unresponsive and the events that unfolded before and after the code (Nurses Service Organization, 2024).
Do not chart a symptom without an appropriate intervention or action. For example, if a patient complains of chest pain, make sure to document the immediate interventions. Some examples are “applied 2L nasal oxygen via nasal cannula”, “completed a STAT electrocardiogram,” “administered morphine,” or “called the physician.” Also, ensure to include the timeline of events in the documentation.
Do not falsely change a patient’s record. For example, backdating entries from the day before since information was missing or was forgotten.
Do not use unapproved medical abbreviations or shorthand. An example is inaccurately using an abbreviation, like q (every). This can be misconstrued as a typo, so document the word “every.” Another example is using shorthand for words. For instance, documenting “gave pt med and pt fm at bedside.” From this example, it is hard to determine the note. Instead, document thoroughly and spell out all words, like “Administered 5 mg of intravenous morphine to the patient and patient’s family members at the bedside.”
Do not document vague or generic descriptions. Instead, provide accurate and precise descriptions when possible. For example, do not chart “patient voided,” but instead document “patient voided 500 ml of clear yellow urine in the bedside commode.”
Avoid charting excuses in the medical record. For example, if a medication is unavailable from a pharmacy, document the request to the pharmacy and at what time. Do not chart patient refusal (this would be falsifying a medical record) or medication unavailable.
Avoid documenting subjective information in a patient’s chart unless it's pertinent. Do not document what the patient heard or what they inferred. For example, if a patient is angry, document their objective actions instead.
Never pre-document on a patient. This is considered fraud since the actions were not yet performed on the patient. Instead, document in real-time or immediately after an event or assessment occurs
Patients and their families also play a large role in preventing medical errors. Emphasizing patient involvement in their care and safety is paramount. Interestingly, patients help detect medical errors and adverse events and, thus, should be encouraged to speak up about their care. Some studies have reported that patient satisfaction surveys have detected errors in the medical care they received that were otherwise not reported or discovered within the patient’s medical record. In many health facilities, patients and their family members are encouraged to alert rapid response teams if they are deteriorating or have a change in health status. In addition, healthcare team members should instill a trusting relationship with their patients and promote effective communication practices(Patient Safety Network, 2019).
*Please note that these scenarios are not all-inclusive of potential error prevention strategies and are meant to serve as a guide.
A medical-surgical nurse is caring for a 77-year-old patient who is NPO (nothing by mouth) and hypertensive, with a blood pressure of 160/80 and a heart rate of 78. The patient has a past medical history of hypertension and has not taken any oral antihypertensive medications today. The patient is allergic to metoprolol. The nurse carefully reviews the patient’s current orders and notes that the patient has no PRN (as needed) for the antihypertensive medications ordered. Which strategies can the nurse take to prevent a potential medical error from occurring?
First, the nurse should gather the necessary information from the patient’s chart to prepare to call the healthcare provider for orders. Considering the SBAR communication tool, the nurse should gather information about the situation, background, assessment, and recommendation. This communication method can help reduce medical errors. An example of SBAR is:
Situation (statement of the problem): A 77-year-old patient is hypertensive and is NPO. Does not have any antihypertensive medications ordered.
Background (brief patient information): The patient has a history of hypertension and is allergic to metoprolol. They do not have any other medical history.
Assessment: The patient’s current blood pressure is 160/80, and heart rate is 78.
Recommendation: Since the patient is hypertensive, NPO, and allergic to metoprolol, I recommend ordering an intravenous antihypertensive medication, like hydralazine.
The nurse gives the SBAR report to the provider and receives verbal orders for hydralazine 10 mg IV push every 6 hours as needed for systolic blood pressure greater than 150. The nurse repeats back the orders to the provider and the provider confirms accuracy. Simultaneously, the nurse enters the orders into the patient’s electronic medical record (instead of handwriting them).
Next, the pharmacy reviews the patient’s medication, another step in the medication ordering process, to help identify possible errors. The pharmacy determines the orders are correct, and then the nurse prepares to administer the medication. What are some medication administration techniques they can use to prevent a medical error from occurring?
Recognize the tall man lettering on the medication
Confirm the patient’s allergies
Draw up the medication in a “distraction-free zone”
Utilize barcode scanning when available
Follow the medication rights
Provide patient education before administration
This list is not all-inclusive; these are just some methods that the nurse can use to reduce the chance of medical errors. What other medical error prevention strategies can you think of in this scenario?
A new advanced practice provider (APP), such as a physician assistant or nurse practitioner, assesses a 17-year-old patient who presents to an outpatient urgent care with severe abdominal pain and nausea. The patient’s family member is in the room as well. The APP believes the patient may have appendicitis and would like to send the patient to the emergency room but isn’t entirely confident about this diagnosis and plan. They would also like to order an antiemetic for nausea within the electronic health record. Which steps can the provider implement to reduce medical errors at this point in the patient’s care?
First, the APP should review the patient’s chart, including their history, allergies, and current medications. Recall that performing accurate medication reconciliation and verifying patient allergies is a way to reduce medical errors. To reduce the likelihood of potential diagnostic errors, the provider should pause and think critically about the possible differential diagnoses of appendicitis. At this time, the provider can use tools, like diagnostic algorithms, to aid with differentials and diagnosis of appendicitis. Also, since the provider is not confident in their diagnosis, they could consider speaking with another provider or their clinical supervisor to seek further input.
In addition, before ordering the antiemetic, the APP should review the patient’s current medications and allergies. When placing the order, they should verify the information for accuracy before submitting it to the patient’s electronic health record. Also, to reduce medical errors, they should avoid giving verbal or handwritten orders to the medical staff (medical assistants, nurses, licensed practical nurses, etc.).
The APP decides to call their supervising physician to seek a second approach and talk through possible differential diagnoses. The supervising physician agrees with the APP’s assessment and diagnoses and suggests sending the patient to the emergency room. Next, the APP goes to document in the patient’s chart. Which actions might the APP take to reduce the potential of medical errors?
*A helpful hint is to think of best documentation practices.
The APP should document when the physician was contacted and what information and results/plan were discussed.
When documenting the information, the documentation should be thorough, objective, and accurate. Other best practices to consider are that the APP should avoid incorrect medical abbreviations and personal opinions of the patient and avoid pre-charting information.
What other medical error prevention strategies might the APP use at this point in the patient’s care?
Next, the APP discusses the working diagnosis with the patient and their family member. They recommend the patient go to the emergency room for further evaluation and treatment. Which steps can the APP take to reduce medical errors at this point in the patient’s care?
Engage the patient and their family members in their care. Allow them to ask questions and provide as much education as possible.
If possible, consider calling the emergency room (ER) where the patient will be going and speaking with the ER provider. Summarize the patient’s assessment using effective communication tools and discuss the possible differential diagnoses.
Accurately document the patient transfer and telephone call with the ER provider.
Numerous strategies exist for healthcare professionals and organizations to prevent medical errors. The first step is often to understand a medical error since it does not always result in patient harm. If a near-miss event or medical error occurs, reporting it as outlined by the healthcare facility’s policies and procedures is judicious.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Agency for Healthcare Research and Quality. (2019). Tool: SBAR. Agency for Healthcare Research and Quality. Visit Source.
Aljabari, S., & Kadhim, Z. (2021). Common barriers to reporting medical errors. TheScientificWorldJournal, 2021, 6494889. Visit Source.
American Society for Quality. (2024). Failure mode and effects analysis (FMEA). American Society for Quality. Visit Source.
Asgarian, A., Mahjour, P., Heidari, H., Khademi, N., Ghassami, K., & Mohammadbeigi, A. (2021). Barriers and facilities in reporting medical errors: A systematic review study. Advances in Human Biology, 11(1): 17-25. Visit Source.
Bell, T., Sprajcer, M., Flenady, T., & Sahay, A. (2023). Fatigue in nurses and medication administration errors: A scoping review. Journal of Clinical Nursing, 32(17-18), 5445–5460. Visit Source.
California State University, Fullerton. (2022). What are the essential techniques of risk management. California State University, Fullerton. Visit Source.
Choudhury, A., & Asan, O. (2020). Role of artificial intelligence in patient safety outcomes: Systematic literature review. JMIR Medical Informatics, 8(7), e18599. Visit Source.
De Hert, S. (2020). Burnout in healthcare workers: Prevalence, impact and preventative strategies. Local and Regional Anesthesia, 13, 171–183. Visit Source.
Ferdosi, M., Rezayatmand, R., & Molavi Taleghani, Y. (2020). Risk management in executive levels of healthcare organizations: Insights from a scoping review (2018). Risk Management and Healthcare Policy, 13, 215–243. Visit Source.
Gemmete J. J. (2024). Learning from medical errors. CVIR Endovascular, 7(1), 8. Visit Source.
Institute of Medicine (US) Committee on Quality of Health Care in America, Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (Eds.). (2000). To err is human: Building a safer health system. National Academies Press (US).
Kennedy, G.A.L., Pedram, S., & Sanzone, S. (2023). Improving safety outcomes through medical error reduction via virtual reality-based clinical skills training. Safety Science., 165,106200. Visit Source.
LeLaurin, J. H., & Shorr, R. I. (2019). Preventing falls in hospitalized patients: State of the science. Clinics in Geriatric Medicine, 35(2), 273–283. Visit Source.
Li, C. J., Shah, Y. B., Harness, E. D., Goldberg, Z. N., & Nash, D. B. (2023). Physician burnout and medical errors: Exploring the relationship, cost, and solutions. American Journal of Medical Quality: The Official Journal of the American College of Medical Quality, 38(4), 196–202. Visit Source.
Melnyk, B. M., Tan, A., Hsieh, A. P., Gawlik, K., Arslanian-Engoren, C., Braun, L. T., Dunbar, S., Dunbar-Jacob, J., Lewis, L. M., Millan, A., Orsolini, L., Robbins, L. B., Russell, C. L., Tucker, S., & Wilbur, J. (2021). Critical care nurses' physical and mental health, worksite wellness support, and medical errors. American Journal of Critical Care: An Official Publication, American Association of Critical-Care Nurses, 30(3), 176–184. Visit Source.
Nurses Service Organization. (2024). Do’s and don’ts of documentation. Nurses Service Organization. Visit Source.
Office of the General Surgeon. (2024). Health worker burnout. U.S. Department of Health and Human Services. Visit Source.
Patient Safety Network. (2019). Patient safety 101: The fundamentals. Agency for Healthcare Research and Quality. Visit Source.
Razai, M. S., Kooner, P., & Majeed, A. (2023). Strategies and interventions to improve healthcare professionals' well-being and reduce burnout. Journal of Primary Care & Community Health, 14, 21501319231178641. Visit Source.
Rodziewicz, T.L., Houseman, B., Vaqar, S., & Hipskind, J.E. (2024). Medical Error Reduction and Prevention. In StatPearls. StatPearls Publishing. Visit Source.
Sameera, V., Bindra, A., & Rath, G. P. (2021). Human errors and their prevention in healthcare. Journal of Anaesthesiology, Clinical Pharmacology, 37(3), 328–335. Visit Source.
Singh, G., Patel, R.H., Vaqar, S., & Boster, J. (2024). Root Cause Analysis and Medical Error Prevention. In StatPearls. StatPearls Publishing. Visit Source.
Tariq, R. A., Vashisht, R., Sinha, A., & Scherbak, Y. (2024). Medication dispensing errors and prevention. In StatPearls. StatPearls Publishing. Visit Source.
The Joint Commission. (2024a). Sentinel event data 2023 annual review. The Joint Commission. Visit Source.
The Joint Commission. (2024b). Hospital: 2024 national patient safety goals. The Joint Commission. Visit Source.
Wiegmann, D. A., Wood, L. J., Cohen, T. N., & Shappell, S. A. (2022). Understanding the "Swiss Cheese Model" and its application to patient safety. Journal of Patient Safety, 18(2), 119–123. Visit Source.
Zangaro, G., Van, C.M., & Mossburg, S. (2023). Impact of system failures on healthcare workers. Agency for Healthcare Research and Quality. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.