This course will be updated or discontinued on or before Friday, September 11, 2026
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will know how to perform a newborn assessment.
Objectives
After completing this continuing education course, the participant will be able to:
Describe the routine management of a healthy newborn.
List the risk factors that need to be assessed for potential complications in a newborn.
Outline how to assess a newborn.
Determine when to call a provider with newborn assessment abnormalities.
Plan nursing care for the newborn.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
A newborn should have a thorough assessment completed by a provider within 24 hours of life. This assessment should include a review of the pregnancy, previous pregnancies, the mother’s history, and the mother’s prenatal screenings.
Before this complete assessment by a provider, the RN is the first to assess the baby and should be able to provide a comprehensive assessment to identify any immediate issues that need to be addressed. In addition, prior to a provider's assessment, a nurse should also perform routine assessments on all newborns.
Immediately after delivery, the RN will assess the newborn for any problems they are having transitioning to extrauterine life. The nurse may be alone with the newborn at this time or may have a provider present already if it was a high-risk delivery. This assessment is quick and may lead to the initiation of newborn resuscitation. If there is no provider present and the newborn requires intervention or resuscitation, the nurse should call for extra help.
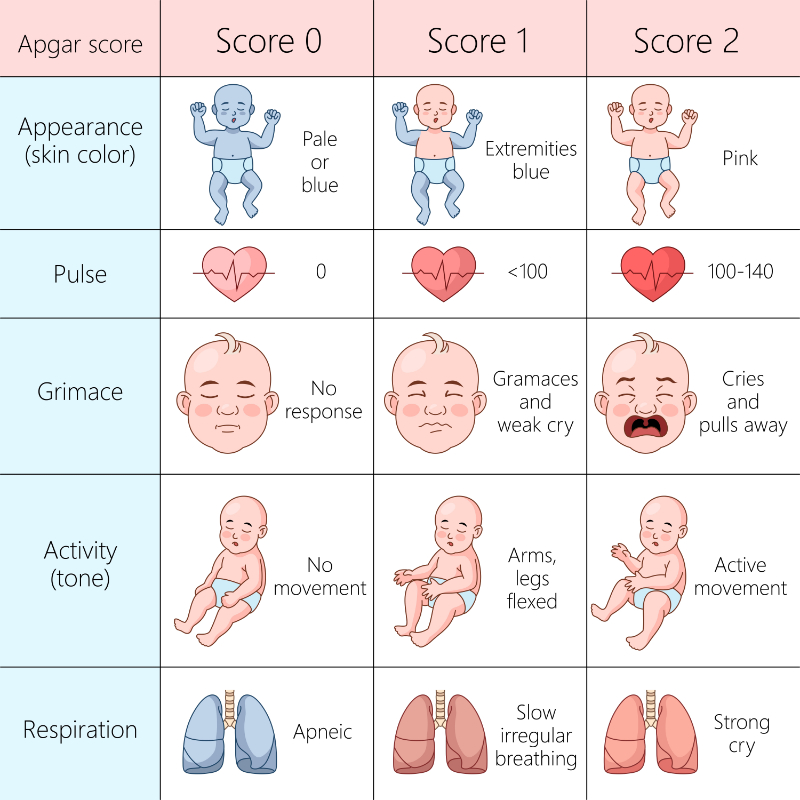
An APGAR score is a quick, evidence-based method for assessing a neonate immediately after birth and in response to any required resuscitation (Simon et al., 2023).
APGAR stands for (Simon et al., 2023):
A: Appearance
P: Pulse
G: Grimace
A: Activity
R: Respiration
While the APGAR score was originally designed back in 1952 by Dr. Virginia Apgar, this acronym of the same name is most helpful in helping to remember the components that should be assessed in the newborn (Simon et al., 2023). The APGAR scores are assigned to the newborn baby at 1 minute and at 5 minutes of life by the RN or the provider caring for the newborn (Simon et al., 2023).
The APGAR score assigns numbers based on the newborn’s heart rate, respiratory effort, muscle tone, reflex irritability, and color. These scores can range from 0 to 10 based on the assessment (Simon et al., 2023). Use the image below to help define how to assign an APGAR score based on the newborn assessment.
The transition period of the newborn is 4 to 6 hours following birth, when the newborn is transitioning from intrauterine to extrauterine life. During this period of time, the newborn should be assessed every 30 to 60 minutes to include the infant’s temperature, respiratory rate, heart rate, color, and tone (McKee-Garrett, 2023b; American Academy of Pediatrics & American College of Obstetricians and Gynecologists [AAP & ACOG], 2017).
A normal newborn heart rate is 120 to 160 beats per minute, and a normal respiratory rate is 40 to 60 breaths per minute. A temperature of ≥ 100.4°F is generally considered a fever. Infant temperature should be maintained between 36.5 to 37.5°C (97.7 to 99.5°F). When assessing the newborn’s color, it is important to watch for central cyanosis (lips, tongue, and central trunk) as these can indicate respiratory or cardiac disease (McKee-Garrett, 2023b).
Each newborn should receive the same evidence-based routine management before being discharged to go home. This routine management should include (Castro Ochoa & Mendez, 2023; Hand et al., 2022; AAP & ACOG, 2017):
As mentioned in the list briefly above, each newborn should receive prophylactic eye care (which is usually erythromycin ointment) applied to both eyes to prevent neonatal gonococcal ophthalmia.
Image 2: Neonatal Gonococcal Ophthalmia
Image Source: Centers for Disease Control and Prevention: Public Domain Image
Because newborns do not have enough Vitamin K, which is a substance in our blood that helps us to form clots, they should also receive a Vitamin K intramuscular (IM) injection to prevent Vitamin K deficient bleeding (VKDB) (Castro Ochoa & Mendez, 2023; Hand et al., 2022). Erythromycin and Vitamin K are usually given shortly after birth. Parents who refuse either or both of these prophylactic treatments should receive education about the importance of these treatments.
Newborns should also receive their first Hepatitis B vaccination. The Hepatitis B vaccine should be given within 24 hours of birth, and infants born to mothers who are Hepatitis B surface antigen (HBsAg)-positive should also receive Hepatitis B immune globulin (HBIG) shortly after birth (Chabra & Hofstetter, 2020).
Routine management of newborns following birth should also include a screening for congenital hearing loss. The universal newborn hearing screen should be performed to check for hearing loss so that early intervention can be started if there is a problem.
Blood sample screening for metabolic and genetic disorders of newborns is important as well. Metabolic and genetic screening is recommended for all newborns while in the hospital. When identified on an initial screening, newborns typically have a second screening done to confirm suspicions. When identified in the newborn stage, early intervention or treatment for these diseases can help to improve outcomes.
Image 3: Newborn Metabolic Screening
Some states also require screening for critical congenital heart disease. About 1% of babies have a congenital heart defect (CHD) (American Academy of Pediatrics [AAP], 2023). Unfortunately, not all congenital heart defects are caught prenatally or by physical examination at birth (AAP, 2023). In many cases, a baby who is identified as having a congenital heart defect could look “normal” and present completely asymptomatically (AAP, 2023). Critical congenital heart disease (CCHD) screening is a simple pulse oximetry test that can detect potential cardiac problems.
The CCHD screening should be done 24 hours of age and after, or shortly before discharge (AAP, 2023). A pulse oximeter is applied to the right hand and either right or left foot. A pulse oximeter reading of 89% Sp02 or less on any extremity is a failed test. If the infant has a pulse oximeter reading of 90% Sp02 to 94% Sp02 in any extremity OR if there is a difference of 4% or more between the right hand and either foot, the infant should be retested in 1 hour. The same result as in the first round would be a test failure. In some cases, and specifically according to unit policies and procedures, a third attempt might be done, as pictured below. Passing the CCHD is a pulse oximeter reading of 95% Sp02 or more in the right hand and either foot and a difference of 3% or less between the 2 (Oster, 2024). A failed test or a “positive screen” means that a newborn may have a CCHD that requires intervention or treatment.
It is also recommended that all infants are screened for hyperbilirubinemia during their hospital stay. This screening can be done by a blood serum level or a transcutaneous bilirubin test prior to discharge. Jaundice should be assessed by the nurse every 8 to 12 hours (McKee-Garrett, 2023b).
Weight loss of the infant should be monitored while in the hospital. It is normal for infants to lose up to 10% of their body weight, but greater than 10% weight loss requires an evaluation of feeding and support for the mother.
There are risk factors that have the potential to impact the well-being of a neonate.
These risk factors can include (McKee-Garrett, 2023a):
Maternal diabetes: This can put the newborn at risk for hypoglycemia.
Maternal substance use: This can put the newborn at risk for withdrawal/neonatal abstinence syndrome (NAS).
A positive group B strep culture: This can put the newborn at risk for sepsis.
Any infection during labor such as chorioamnionitis: This can put the newborn at risk for sepsis.
Ruptured membranes for > 18 hours: This also puts the newborn at risk for sepsis.
Inherited diseases: These can increase risk to the neonate.
Genetic disorders like Down Syndrome: These can increase risk to the neonate.
Small for gestational age (SGA) or large for gestational age (LGA) size: These infants are at risk of hypothermia, hypoglycemia, and feeding issues.
Preeclampsia, or any other condition that can affect the placenta: These can impact safe delivery and overall health of the infant.
The gestational age of an infant may also put them at risk for certain issues. Preterm infants, who are defined as infants with a gestational age (GA) below 37 weeks, and those who are born late preterm, defined as having a GA of 34 0/7 to 36 6/7 weeks, are at increased risk for morbidity and mortality compared with term infants (GA 39 to 42 weeks) (McKee-Garrett, 2023a).
Some additional screening should be done on infants who have certain risk factors. Glucose screening should be performed on infants who meet the criteria of each hospital’s policy. At the very least, infants with symptoms, including the following, should be tested (Rozance, 2024):
Jitteriness
Sweating
Irritability
Tachypnea
Hypothermia
Pallor
Poor feeding
Weak or high-pitched cry
Changes in level of consciousness
Lethargy
Seizures
Hypotonia (poor or low tone)
Infants who are asymptomatic but meet the following criteria should also be screened for potential hypoglycemia (Rozance, 2024):
Gestational age (GA) < 37 weeks
Infants who are large for gestational age (LGA)
Infants who are small for gestational age (SGA)
Infants of diabetic mothers
Additionally, consideration for glucose screening may be appropriate for infants who are (Rozance, 2024):
A full newborn nursing assessment should include measurements such as vital signs, head circumference, weight, and length. The assessment should start first by noticing the infant’s general appearance, including position, movement, color, and breathing (McKee-Garrett, 2023b). During this general visual observation, the RN should note any apparent deformities, how the baby moves, their color while resting, and their respiratory effort (nasal flaring, grunting, retractions of the chest).
The skin should be assessed for abnormalities such as areas of abnormal pigmentation, macular stains, congenital nevi, or hemangiomas. Vesicles, pustules, and bullae in the newborn may be caused by infections, congenital disorders, or other diseases. Milia are white papules that resolve within a few weeks. This is one of the most common rashes of the newborn skin and it is harmless.
Image 5: Milia
Transient neonatal pustular melanosis and erythema toxicum neonatorum also are self-limiting rashes that will resolve over a short period of time (Chadha & Jahnke, 2019).
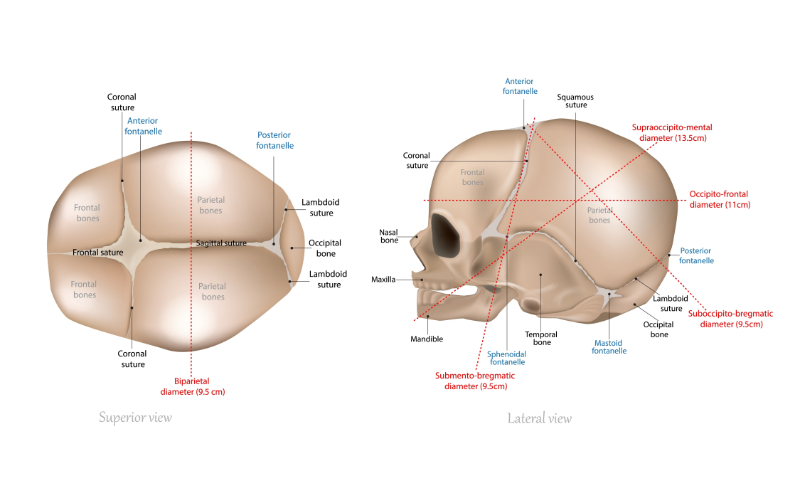
The infant’s head should be assessed next. First, it should be viewed for symmetry. The fontanelles should be soft and flat. The sutures of the skull should be felt. There may be some normal molding of the baby’s head from the birth canal, but if this lasts longer than 2 to 3 days after birth, there may be a problem.
Image 7: Fetal Skull
Caput succedaneum is an area of edema on the infant’s head. This area may be present at birth, it crosses suture lines, and it generally resolves within a few days (McKee-Garrett, 2023a).
Cephalohematomas can look like caput succedaneums from the outside, but internally they are different. Cephalohematomas are collections of blood on the head that are present in 1% to 2% of newborns (McKee-Garrett, 2023a). When palpated, they form a fluctuant mass that does not cross suture lines (McKee-Garrett, 2023a). Cephalohematomas may increase in size after birth, and usually can take weeks to months to resolve (McKee-Garrett, 2023a).
Subgaleal hemorrhages are blood collections between the aponeurosis covering the scalp and the periosteum layer (McKee-Garrett, 2023a). Subgaleal hemorrhages extend across suture lines but feel firm and fluctuant. Experiencing blood loss from these hemorrhages can be deadly and should be assessed immediately (McKee-Garrett, 2023a).
The newborn’s face should be assessed for symmetry. The eyes should also be assessed for symmetry, spacing, and movement. The ears should be assessed to ensure they are parallel to the eyes and not low set, indicating a problem. Assess for any skin tags or pits around the ears. The nose should be assessed for patency. The mouth should be examined for any cleft or abnormality. This examination includes palpation of the palette.
Image 8: Cleft Lip and Cleft Palate
A small jaw could also indicate a problem. The neck is palpated for masses, and the clavicles are palpated for crepitus, which could indicate a birth injury.
The chest should be examined for size, shape, and symmetry. A malformed chest could indicate a problem. Retractions may be observed with respiratory difficulty. Breast tissue size and location should be assessed. The lungs should be auscultated while the infant is quiet. The infant’s respirations should be observed and counted for a full minute. Heart rate should be assessed with a stethoscope while listening for murmurs. The femoral pulse should also be palpated.
The infant’s abdomen should be assessed for shape and symmetry. Any abnormal abdominal distention or discomfort on palpation should be reported to the provider, as this could indicate a problem with the infant. The umbilical cord is evaluated to ensure it is clean without any signs of infection, such as redness or discharge (McKee-Garrett, 2023a).
The genitalia should also be observed. The size and location of the labia, clitoris, meatus, and vaginal opening should be assessed in the female infant. The labia minora and clitoris are prominent in preterm infants, while the labia majora becomes larger as the infant approaches full term (McKee-Garrett, 2023a).
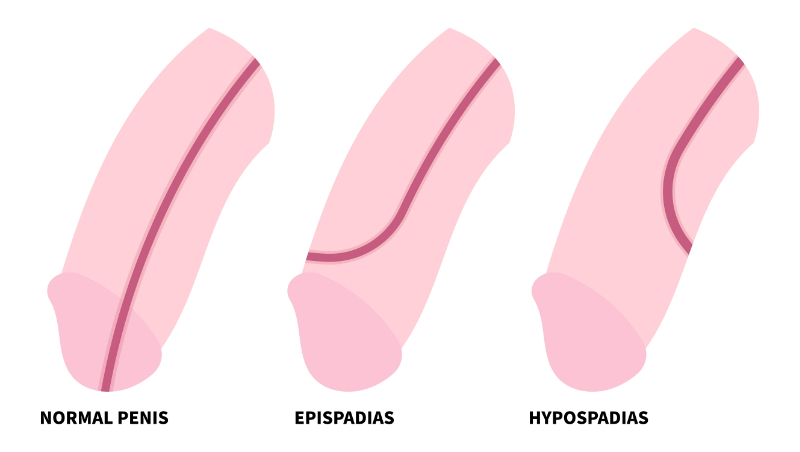
In a male infant, the presence of testes, size of the penis, appearance of the scrotum, and the position of the urethral opening should all be assessed (McKee-Garrett, 2023a). A newborn who has had a circumcision should be assessed for excessive bleeding or signs of infection. One or both undescended testicles should be reported to a provider. A male urethra with the abnormal ventral placement of the urethral opening is hypospadias.
Image 9: Hypospadias
A newborn with hypospadias should not have circumcision and should see a urologist. The tissue that is removed during circumcision, the foreskin, is what is used for the reconstruction and repair (Johns Hopkins Medicine, n.d.).
The anus is examined for patency. Imperforate anus is not always visible. A baby who has not passed meconium and has a distended abdomen needs urgent evaluation by a provider. A small sacral dimple may be normal, but a larger dimple needs evaluation.
The infant’s extremities should be assessed for proper movement and to ensure there are 5 fingers on each hand and 5 toes on each foot. The hips should be evaluated. The Ortolani and Barlow maneuvers use adduction and posterior pressure to feel for dislocation and abduction and elevation to feel for reduction (McKee-Garrett, 2023a).
Newborn pain should be assessed every time that the newborn gets vital signs taken and during a painful procedure, such as a circumcision, according to hospital policy.
Infant pain can often be indicated by (Roué, 2024):
This pain should be evaluated and documented using a validated tool. There are many options available including the Neonatal Pain Agitation and Sedation Scale (N-PASS) and the Neonatal Infant Pain Scale (NIPS) (Roué, 2024).
The newborn provider should perform a full exam on a newborn within 24 hours of birth. Any abnormal findings should be reported to the provider when they are found. It is also important to note that any change in condition (lack of passage of meconium or decreased/absent urine output, not feeding well) that is noted on a follow-up assessment should be communicated to the provider promptly (McKee-Garrett, 2023a). Some problems, as mentioned above, such as a low sugar or fever, need immediate evaluation by a pediatrician or neonatologist who is available. If the infant requires more frequent assessment and observation, they will require a higher level of care, likely in a NICU setting.
Nurses caring for newborns must know how to provide a complete, thorough assessment of the newborn. It can be easy to miss something minor, but if the nurse understands what is normal, he or she will be able to identify the abnormal.
The nurse, Cara, assesses a 20-hour-old baby girl. The infant initially breastfed well during the first 8 hours of life but has not had a good feed in the past 12 hours. The infant has been getting fussier and is now inconsolable.
When Cara takes the infant’s vital signs, her heart rate is 172, her respiratory rate is 66, and her temperature is 98.9°F. The mother states that the baby will not latch and feed, even though she did earlier. The baby has voided but has not passed any meconium.
Cara notices during her assessment that the baby’s abdomen is distended, and her skin appears shiny. The rest of the baby’s assessment is normal.
What could this be? What should the nurse do?
This case could be an infant with an imperforate anus because the baby has not passed meconium and has a distended abdomen. The infant is starting to exhibit signs of distress, with an elevated respiratory rate. This sign is an urgent scenario that a provider needs to assess immediately. This infant will need to go to the NICU and if her anus is imperforate, she will need treatment immediately.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
American Academy of Pediatrics. (AAP). (2023). Newborn screening for critical congenital heart defect (CCHD). American Academy of Pediatrics (AAP). Visit Source.
American Academy of Pediatrics (AAP) & American College of Obstetricians and Gynecologists (ACOG). (2017). Guidelines for perinatal care. (8th Ed). American Academy of Pediatrics and American College of Obstetricians and Gynecologists. Visit Source.
Castro Ochoa, K. J., & Mendez, M. D. (2023). Ophthalmia neonatorum. In StatPearls. StatPearls Publishing. Visit Source.
Chabra, S., & Hofstetter, A. M. (2020). Timely hepatitis b birth dose receipt for newborns: Within 24 hours. Hospital Pediatrics, 10(12), e18–e20. Visit Source.
Chadha, A., & Jahnke, M. (2019). Common neonatal rashes. Pediatric Annals, 48(1), e16–e22. Visit Source.
Hand, I., Noble, L., & Abrams, S. A. (2022). Vitamin k and the newborn infant. Pediatrics, 149(3), e2021056036. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.









-screening.gif)
-screening.gif&description=CEUfast.com - graphic showing flow of critical congential heart disease screening)