Heart Failure is in essence a form of structural heart pumping problem.
Since medical treatment of heart failure at best only slows the condition and/or reduces symptoms, why do not we try structural repair? Medical treatment for heart failure is always to be considered first due to the risks of invasive procedures. Of course medical treatment does not stop once an invasive approach is decided on. It continues throughout the course of the condition and is adjusted to respond to the changing needs of the client. Conventional medical heart failure treatment typically includes life style changes, ACE inhibitors, beta-blockers, digoxin, diuretics, spironolactone and perhaps blood thinners. Invasive treatments for heart failure include aid in heart pumping, devices to control rhythm disturbances, and structural repairs in tissue all the way up to the final intervention of heart replacement itself. Let’s take a look at some of these interventions.
Revascularization has been a great victory for survival. The flip side of this is that the increased survival rate translates into more patients who will inevitably develop cardiomyopathy and heart failure. When more of the actual heart tissue survives, the chance of developing heart failure is decreased. Even when heart failure is present, if areas of the heart can have their blood flow improved then the heart’s overall ability to pump also improves.
A rule of thumb is that about 40 percent of the heart tissue involved in a heart attack is likely to recover. This includes recovery of both a spontaneous nature and that achieved by surgically restoring blood flow. General heart function is expected to improve in some patients who have experienced an ischemic insult such as a heart attack after such a revascularization procedure. There is a special term for this myocardial tissue that is in a state of shock and is hovering between ischemic death and recovery, it is said to be hibernating. The potential for recovery is good enough to do surgery when less than 40 percent of the left ventricle is scarred or hibernating. If it is more than 40 percent, surgical mortality is much higher and recovering heart function is considered both unlikely and too risky.
Coronary bypass graft surgeries are now commonplace and relatively safe. The placement of stents or other expansion devices within blocked arteries during angioplasty in order to enhance vascular flow is also a common invasive treatment option. These procedures are very helpful in the slowing of heart failure progression. The more functional the heart muscle, the better its pumping capability.
One thing to consider before doing any type of invasive procedure on a heart failure client is the need for having a heart assist device ready for after the surgery. This is due to the potential for catastrophic complications that are inherent when dealing with a failing organ system such as the heart in CHF. The decision must be done before the surgery or procedure due to the time involved obtaining assistive devices. It is also important to discuss the patient and family wishes about heart transplant if the surgery fails. If the patient is unable to be taken off the heart-lung bypass machine after surgery, how can someone who is unconscious and on a ventilator tell us that he wants a transplant? He cannot. So if you have a patient who is at risk, the discussion about heart transplant options should occur before proceeding with revascularization. Allow the patient to make a decision as to whether a transplant is wanted before considering one of these high-risk procedures.
It is not just stents that are being stuffed into hearts these days in the hope of easing CHF symptoms. Muscle cells taken from the patient’s own arm muscles and even stem cells are being injected into failing hearts in an effort to establish whether cells other then heart muscle cells will be able to restructure and repair the failing heart. These treatments show promise for slowing the degradation of the heart structure in congestive heart failure, and to some small extent repairing previously damaged tissue. Studies continue and the potential for developing a usable treatment regimen is definitely there (Muscle, 2003) (Stem Cell, 2002).
If it is a structural problem that is causing failing heart function, such as aortic stenosis, fix it. An approach that combines the goals of structural repair and increasing pumping pressures is that of mitral valve repair. Some extent of mitral regurgitation is almost always seen in individuals with severe heart failure. Valve repair can be, and often is, combined with surgically restoring blood flow when coronary disease is present (as in bypass surgery). Factors that may prevent mitral valve repair in CHF patients include primary mitral valve dysfunction, aortic insufficiency, and existing mitral regurgitation that was already occurring before the patient got CHF. Initial experience with mitral valve repair in CHF patients showed reduced heart size and improved heart function. When such patients are seen 4 months after surgery, there is often improved cardiac output. This includes a decrease in CHF symptoms and increased exercise tolerance. Typically this benefit lasts for up to 2 years. In one study of 48 patients who had mitral repair, the one-year survival rate was 82 percent and the two-year survival was 71 percent. Their hospitalizations for CHF went down and their heart function class ratings improved. Unfortunately any long-term followup data is scarce on CHF post surgery patients (Glasser, 2001).
Heart reconstruction or size reduction procedures are valuable alternatives to heart transplant. Removing portions of non-functioning heart muscle may return the heart to a more normal shape and size. It is hoped that reducing heart chamber sizes will reduce heart wall stress. One of the more common procedures to accomplish this is known as the Batista Procedure after Dr. Randas Batista, a Brazilian heart surgeon who developed this technique, which could more accurately be called a partial left ventriculectomy. In this procedure a section of the left ventricular wall is removed. Then the remaining free edges are repositioned and joined together. The heart’s mitral valve is also repaired or replaced. The 30-day after-surgery death rate for the Batista Procedure runs around 22 percent. Of those who survive the immediate postoperative period a two-year survival of around 55 percent has been reported. On the positive side, CHF symptoms improved in 90 percent of the survivors; however, followup was lax and the report lacked scientific strength. Long-term followup on patients is lacking at this time. In one study, it was shown that improvement in heart function after the Batista procedure depended on how much fibrosis and heart cell enlargement was present before surgery. Despite apparent initial success, there is a high recurrence rate of CHF. About one-third of patients improve, one-third are unchanged, and one-third get worse. Late fatal arrhythmias plague this procedure, forcing use of implantable defibrillators in many of the surgery clients. It is due to the poor success rate that the Batista procedure has currently fallen out of favor with many cardiologists and surgeons (Glasser, 2001).
Cardiomyoplasty, also called dynamic cardiomyoplasty, is a surgery that wraps the big back muscle (latissimus dorsi) around the heart. The back muscle is then trained with electrical impulses to contract in time with the heart, helping it beat more strongly. Heart failure symptoms tend to improve after cardiomyoplasty. It is speculated that cardiomyoplasty may reverse remodeling of the failing heart. It may also act as an elastic girdle around the heart to help reverse heart enlargement. Study findings were seen in 261 patients from the Worldwide Cardiomyoplasty Group. Survival at one month was 88 percent, at 3 months it was 80 percent, and at 6 months it was 76 percent. Over time, surgical deaths have gone down from 31 percent to 3 percent, with heart class improving in 80 percent to 85 percent of hospital survivors. Quality of life and heart function can improve after cardiomyoplasty. However, there is not enough data as of yet to draw strong conclusions. Although 10 years of experience with cardiomyoplasty around the world suggests that there is sustained improvement in most patients, the future of this procedure for CHF patients is uncertain (Glasser, 2001).
Ventricular Assistive Devices (VADs) are any of a wide array of mechanical devices that are specifically designed to help the pumping capacity of the heart. They come in many different forms and are used to keep patients alive until a donor heart is available for transplant. For example, a left ventricular assistive device is a surgically implanted mechanical device that helps the left ventricle of the heart pump blood. If both of the heart's pumping chambers are failing, then two heart pumps may be used one for each ventricle. It has been quite exciting lately as the last few years have been a bonanza for this kind of technology, as well as a generalized increase in acceptance of mechanical organ adjuncts in this post six million dollar man market.
Several versions of temporary pumping assistance devices are on the market for use while waiting for a heart transplant or total artificial heart.
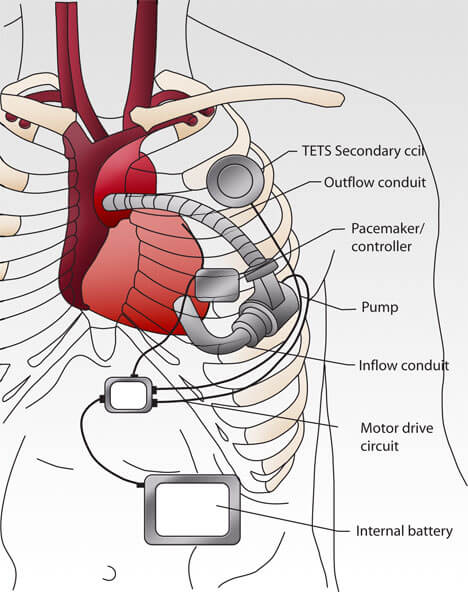
VAD (drawing compliments of NASA)
VAD – or, Ventricular Assistive Device from NASA. It can assist left or right ventricular functioning. Or with two VAD’s, both! Note the external power and control pack. – (NASA.org)
Growing acceptance of mechanical heart aids are currently paving the way for the total artificial heart. Devices like the Abiomed total artificial heart are meant to be a permanent replacement for a failing heart, and are implanted completely inside the body. The cost of the implant and the first year's followup is estimated to be about $120,000 - not much more than a transplant. As I am writing this, artificial heart trials are ongoing with no lack of volunteers. Among the medical research community, it is accepted as fact that artificial hearts will soon be available within the next ten years in ever increasing numbers (Glasser, 2001).
Heart transplant is officially the treatment of last resort. The limited availability of healthy donor hearts makes the process of receiving a heart transplant one that many candidates will not survive as no more than 2,500 clients every year are able to receive a donor heart. The main requirement of a recipient in the transplant process is terminal heart disease with an estimated chance for one-year survival less than 50 percent. Generally speaking the remaining criteria are more how a person functions rather than their age range. Life-threatening illnesses, liver, and kidney function are screened for, as well as determining the degree of pulmonary vascular resistance. This is due to the fact that when pulmonary pressure stays high long enough, it causes irreversible damage to the lungs' blood vessels. Social and psychological problems are looked at due to the stress of having a transplant. An active history of alcohol or drug abuse in the past 12 months tends to knock a person off of the waiting list and smokers must be off tobacco for at least 6 months. Many transplant centers track waiting recipients with urine tests for nicotine as some centers have found that as much as 40 percent of smokers lie about quitting. All this means that only about 12 percent of patients who are referred for transplant at some centers go on to actually getting a donor heart. Post heart transplant treatment continues as an ongoing process to aid with donor acceptance and avoid complications (Glasser, 2001) (Hunt, 2003).
A look at where the work goes into a heart transplantation (University Southern California)
Artificial hearts have gained a new name recently. They are now commonly being referred to as TAH for total artificial hearts. This separates them from LVADs and VADs, which in general are heavier in weight and more commonly used in heart failure patients. TAH’s come in several functional styles, from right at a dozen serious manufacturers. Currently Abiomed’s AbioCor TAH is the tenuous front-runner in this fast approaching technology, so we will use it as an example in this section.
The JARVAK-7 Total Artificial Heart in place, Jarvak’s made their place in history with the Barney Clark trials in the ‘80s. Artificial hearts have come a long way since then. (Compliments of Texas Heart Institute)
The JARVAK TAH, out in the light. (Compliments of the Smithsonian collection)
The TAH’s are finally coming into their own after many years of development. Other artificial assistance devices have been in use for decades, but a device designed with the exclusive purpose of being a replacement heart is just now reaching the point of serious human trials. Most of the current generation of TAH is designed to fit completely inside the body, with no wires or tubes poking through the recipient’s skin. The AbioCor device, as an example, is a quiet pulsatile device. And yes, other systems are being considered so it is important not to it take for granted that an artificial heart will produce a pulse. By pulsatile device it means that this type of TAH moves the blood in a contract/relax rhythm just like your natural heart does, creating a discernable pulse. The components of the this TAH system include:
1. an internal pumping unit,
2. an internal rechargeable battery,
3. an internal electronics system,
4. an internal power transfer coil,
5. an external power transfer coil, and
6. an external battery pack.
The pumping unit weighs about two pounds and has two ventricle chambers with valves along with a motorized hydraulic pumping system. The electronic system for the TAH is implanted into the recipient’s stomach area where it quietly monitors and controls the TAH, changing the pumping speed of the heart to handle changing activity levels.
This particular system, and most likely all of the upcoming generation of TAH’s, use energy from either an internal or external set of batteries. Since the external battery pack is small and portable, the person can go places and be fairly active. The internal battery is basically an emergency battery. It is kept charged continuously by the external batteries. That internal battery can keep the heart going for up to 30 minutes.
Power is sent from the external batteries to the internal pump through the skin (transcutaneous), using coils. One coil is implanted inside the skin and the other is external. When the individual puts the external coil over the implanted coil, power moves through their skin to the internal coil without any wires. For brief periods, a person can remove the external coil (transmitter) and be free of all external parts - the internal batteries supply the power for up to 30 minutes this way.
For those interested in materials, this TAH is made mainly of titanium and a kind of polyurethane plastic called Angioflex. The TAH does not really have many moving parts, and that is good. Moving parts wear out faster. Parts like the valves and membranes inside the ventricles that do move are made of Angioflex. In lab testing, this plastic has held up to beating 100,000 times a day for years. The smooth, seamless design is meant to reduce damage to blood cells passing through the pump.
The TAH replaces a person’s heart so that the heart muscle and surrounding tissues are almost completely removed. Once it is gone, you cannot get it back! The TAH’s currently in use can pump more than 10 liters of blood per minute. The pumping unit is about the size of a grapefruit, so it can only be used in average sized or larger adults. Other TAH devices are in development, and have been for years. It is a long, expensive road to human trials. There has been some question about other manufacturers holding back on production of their own products until TAH trials have broken the ice. Whatever the corporate psychology at play, total artificial hearts are a real thing, and an option that will not be going away.
An Akutsu-3 TAH. (Compliments of Texas Heart Institute)
As much as we would like it to be, invasive procedures and surgeries alone do not hold the answers to heart failure. Medications do a reasonable job in managing symptoms, and procedures such as revascularization and sequential pacing, are truly wonderful gifts to those who have failure. But, they do little more then slow the progression of this deadly condition.
“ACC/AHA Pocket Guidelines for Evaluation and Management of Chronic Heart Failure in the Adult.” American College of Cardiology / American Heart Association Task Force on Practice Guidelines. February 2002.
“Congestive Heart Failure.” American Heart Association (AHA) – Congestive Heart Failure Resource Site. Http://www.americanheart.org/chf. Updated November 2003.
“Congestive Heart Failure in the United States – A New Epidemic.” National Heart, Lung, and Blood Institute (NHLBI). U.S. Department of Health and Human Services. Public Health Service - National Institutes of Health. Data Fact Sheet. Http://www.nhlbi.nih.gov. Updated 2003.
“CRT Pacing Helps End-Stage CHFers.” American Journal of Cardiology. September 2002.
“Heart Failure.” The Merck Manual. 2000.
“Improving Care for Diabetes Patients through Intensive Therapy and a Team Approach Barriers to Patient Adherence Can Be Reduced.” Research in Action – Agency for Healthcare Research and Quality (AHRQ). http://www.ahcpr.gov.htm. December 2001.
Hunt et al. “Evaluation and Management of Chronic Heart Failure in the Adult.” A Report of the American College of Cardiology / American Heart Association Task Force on Practice Guidelines. February 2002.
Kinugawa, T. “Cardiovascular Disease – Neurohormonal Determinants Identified in CHF Patients.” Heart Disease Weekly. January 2004.
Schuster, et al. “Living with Advanced Congestive Heart Failure – A Guide for Family Caregivers.” The Washington Home Center for Palliative Care Studies. November, 2002.
Stewart, M. et al. “Patient-Centered Medicine: Transforming the Clinical Method.” Thousand Oaks, CA. Sage Publications, Inc. 1995.
Yee, et al. “Getting to the Heart of Atrial Fibrillation.” Nurse Management. September 2003
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.

)

)







