This course will be updated or discontinued on or before Sunday, December 6, 2026
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
CEUFast, Inc. is an AOTA Provider of professional development, Course approval ID#12170. This distant learning-independent format is offered at 0.2 CEUs Intermediate, Categories: OT Service Delivery, Foundational Knowledge.
AOTA does not endorse specific course content, products, or clinical procedures. AOTA provider number 9757.
CEUFast, Inc. is recognized by the New York State Education Department's State Board for Physical Therapy as an approved provider of physical therapy and physical therapist assistant continuing education.
Outcomes
≥ 92% of participants will know how to perform a neonatal cardiac assessment.
Objectives
After completing this continuing education course, the participant will be able to:
Describe cardiac development and fetal circulation.
Identify hereditary diseases in which congenital heart disease is a frequent finding.
Explain the components of a cardiac physical examination.
Examine the acyanotic and cyanotic cardiac defects.
Determine the methods of treatment for cyanotic cardiac defects.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Each year, approximately 1% of all babies born in the United States are diagnosed with congenital heart disease (CHD) (Centers for Disease Control and Prevention [CDC], 2024d). In fact, every fifteen minutes, another baby is born with a cardiac defect in the United States alone (CDC, 2024d). As many as 25% of these babies will be critically ill and require care by cardiologists in the first days to weeks of life (CDC, 2024d). Congenital heart defects are known as one of the leading causes of birth defect-associated infant illness and death (CDC, 2024d).
Depending on the type of heart problem, initial signs and symptoms may include tachypnea, cyanosis, or a heart murmur. With more severe forms of CHD, there may be marked cyanosis, respiratory distress, and rapid progression to advanced states of shock, and even death (Willim et al., 2020). Timely, effective care of neonates with CHD can help to improve short and long-term outcomes, reduce the risk of secondary organ damage, and reduce mortality (Willim et al., 2020).
The cardiovascular assessment of the newborn requires great skill with inspection, palpation, and auscultation techniques.
Inspection of the activity of the neonate, their breathing patterns, the presence or absence of cyanosis, and the activity of the precordium are all important to assess. Palpation of pulses, peripheral perfusion, and thrills are also imperative. Auscultation, however, is the main focus of the cardiovascular exam. While auscultating, this is when the examiner assesses the infant’s heart rate, rhythm, regularity, and heart sounds, especially the existence of any murmurs (Gonzalez et al., 2021). The dynamic properties of the newborn heart make this assessment more complicated than the cardiac assessment of an adult.
The cardiovascular exam constantly changes over the first few hours, days, and weeks of life as the neonate transitions from fetal circulation with the placental circuitry to the newborn lung circuitry. Because of changes in ductal flow, decreasing pulmonary vascular resistance, and increasing systemic vascular resistance occurs over the first few hours and days of life, cardiovascular assessments should be done shortly after birth and again at one to three days of life in addition to regular intervals after discharge. A persistent murmur after 24 hours of age could indicate a potential complication (Mckee-Garret, 2023).
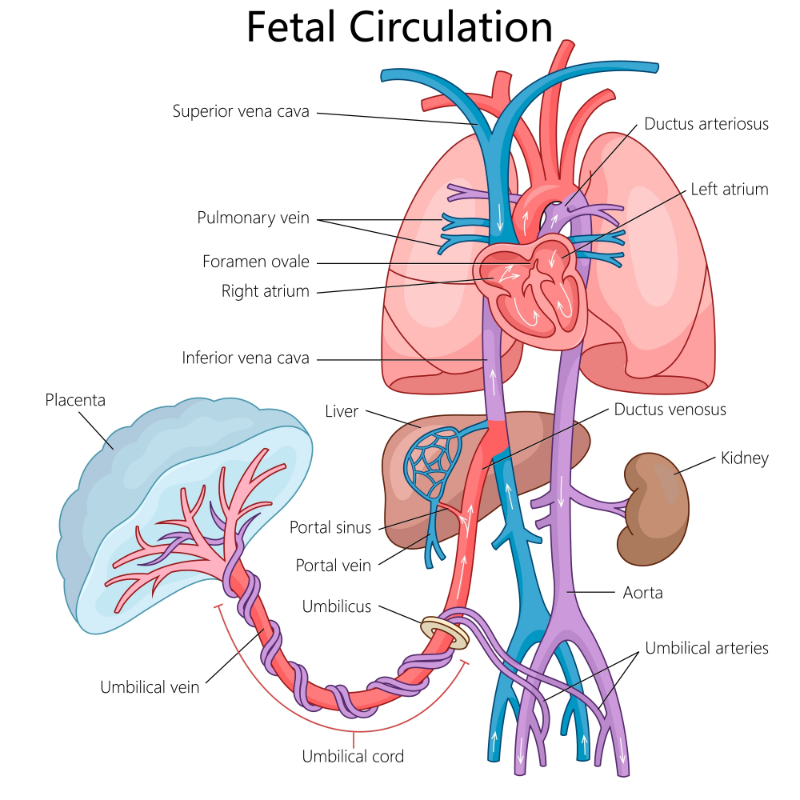
Knowledge of the normal route of fetal blood flow is essential for understanding the circulatory changes at delivery. It is important to know that fetal circulation is anatomically and physiologically unique from adult circulation in numerous significant ways. The highest oxygenated fetal blood is in the umbilical vein, which decreases when it mixes with venous return.
Image 1: Fetal Circulation
In the fetus, the oxygenation of the blood and the removal of carbon dioxide and waste occurs in the placenta, a low-resistance circulatory pathway (Fernandes, 2024). Fetal circulation involves three unique anatomic features that are not present in the adult other than the placenta and the umbilical vein and arteries (Fernandes, 2024):
Ductus venosus
Ductus arteriosus
Foramen ovale
The ductus venosus permits most blood from the placenta to bypass the liver and enter the inferior vena cava. As this blood enters the right atrium, most of it is then diverted toward the atrial septum (Fernandes, 2024). The foramen ovale is the opening between the atrial septum that permits a portion of blood to flow from the right atrium directly to the left atrium (Fernandes, 2024). This blood then goes into the left ventricle and aorta to perfuse the upper extremities and the head of the fetus (Fernandes, 2024).
From the head and upper extremities comes the venous return that passes to the heart through the superior vena cava (Fernandes, 2024). The majority of this blood flows through the right atrium into the right ventricle and then enters the pulmonary artery (Fernandes, 2024). Because pulmonary vascular resistance is high and systemic vascular resistance is low most of the blood in the main pulmonary artery flows through the ductus arteriosus and into the descending aorta to perfuse the trunk and lower extremities (Fernandes, 2024).
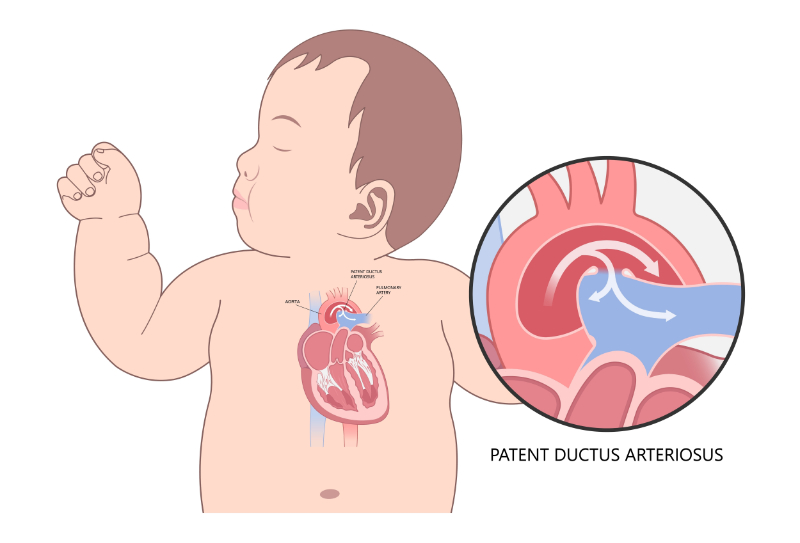
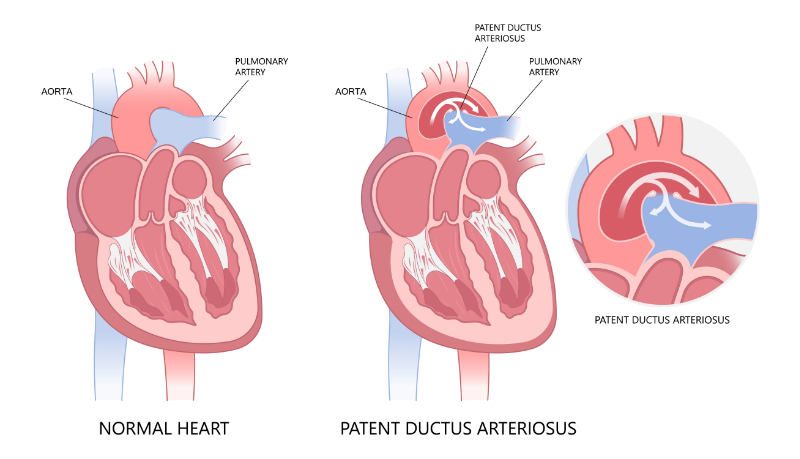
The patent ductus arteriosus (PDA) is a tubular communication between the pulmonary artery and the descending aorta that allows blood to flow between the pulmonary artery to the aorta, bypassing the fetal lungs.
Image 2: Patent Ductus Arteriosus (PDA)
Only about 10% of fetal cardiac output enters the lungs. The other 90% of blood flow is diverted through the ductus arteriosus into the descending aorta (Fernandes, 2024). It really helps to picture fetal circulation as two parallel circuits rather than the serial circuit present in extrauterine life.
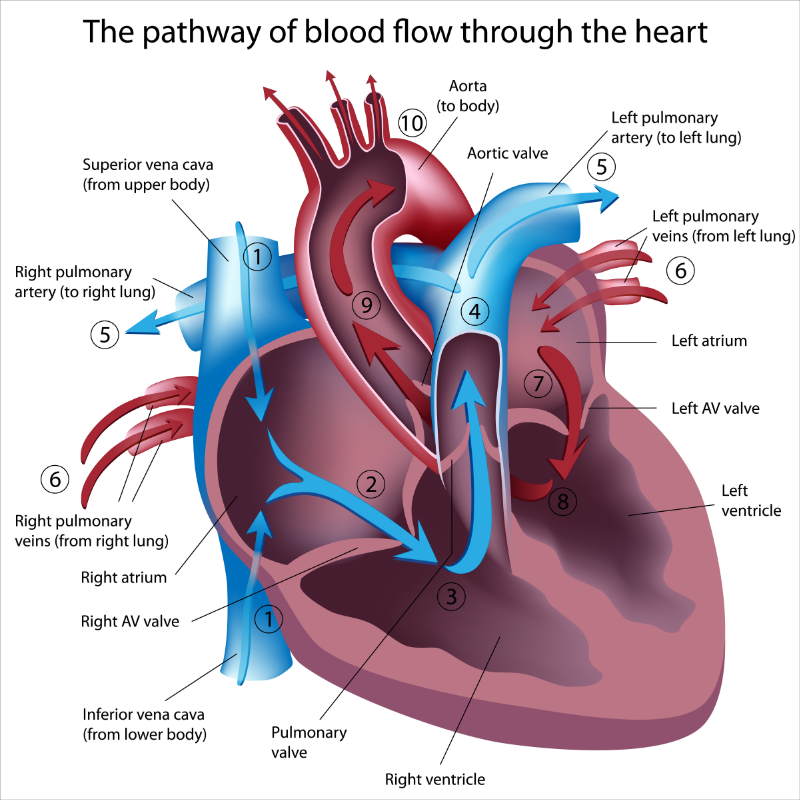
Image 3: Extrauterine Circulation
It is the action of the clamping of the umbilical cord and then the removal of the placenta that immediately initiates circulatory changes in the neonate. When the infant takes their first breath and the umbilical cord becomes occluded, the infant’s systemic resistance is elevated, which reduces blood flow through the ductus arteriosus (Vrancken et al., 2018). Cord occlusion causes a rapid rise in blood pressure and a corresponding stimulation of the aortic baroreceptors and the sympathetic nervous system (Vrancken et al., 2018). The start of respirations and lung expansion causes a decrease in the infant’s pulmonary vascular resistance secondary to the direct effect of oxygen and carbon dioxide on the blood vessels (Vrancken et al., 2018). Pulmonary resistance decreases as arterial oxygen increases and arterial carbon dioxide decreases (Vrancken et al., 2018).
The major portion of the right ventricular output flows through the lungs and increases the pulmonary venous return to the left atrium (Vrancken et al., 2018). The increased amount of blood in the lungs and heat causes increased pressure in the left atrium. The increased pressure in the left atrium, combined with the increased systemic resistance, is what functionally closes the foramen ovale (Vrancken et al., 2018). In most individuals, the foramen ovale closes and becomes sealed by fibrin and cell products deposits during the first months of life. This process is referred to as the anatomic closure of the foramen ovale.
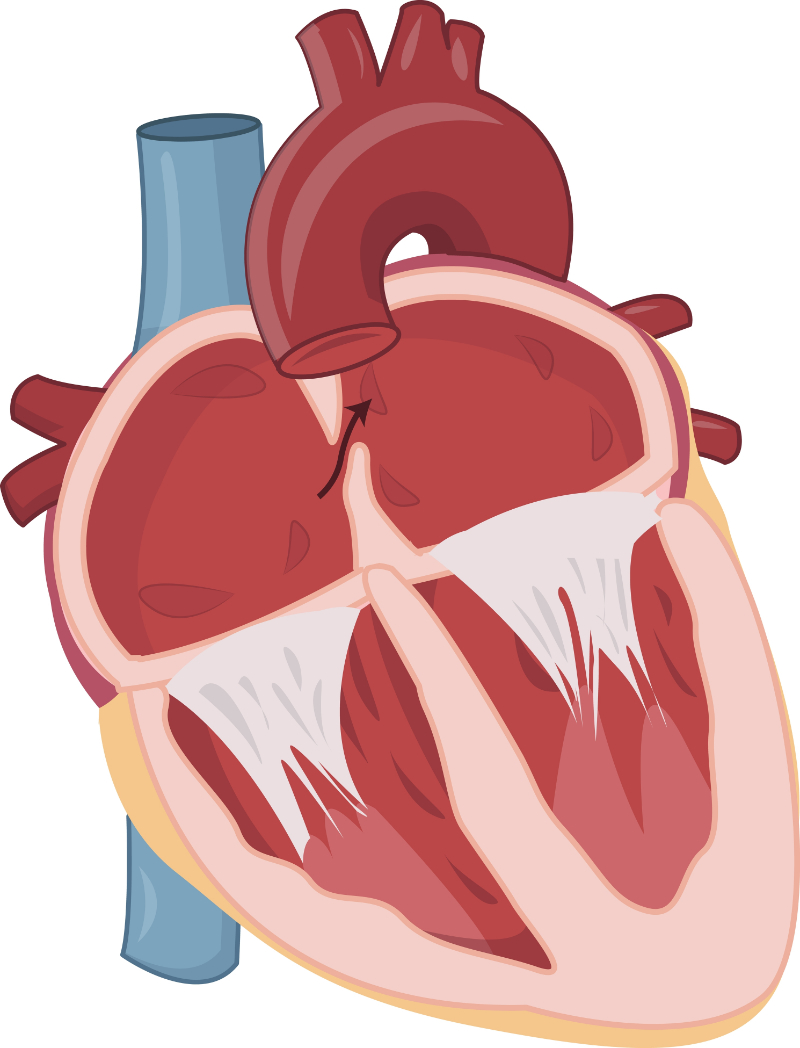
However, in approximately 25% of the population, the foramen ovale is not anatomically sealed (Mayo Clinic, 2022). Therefore, it remains partially open, or what is often called “probe-patent” beyond adolescence (Mayo Clinic, 2022). This finding means that a catheter can be passed from the right to the left atrium during cardiac catheterization or that a probe can be passed through the foramen ovale during cardiovascular surgery (Mayo Clinic, 2022).
Image 4: Patent Foramen Ovale (PFO)
Until the foramen ovale is anatomically sealed, anything that significantly increases right atrial pressure can reopen the foramen ovale, making it patent. Due to the opening structure and the pressure difference, the shunt through the patent foramen ovale (PFO) is primarily from the right to the left atrium. However, if both atria become much enlarged, the foramen ovale may become stretched open, permitting bi-directional shunting of blood or mixing at the atrial level. Most PFOs do not cause any symptoms or complications, but there is a slightly higher incidence of stroke in patients with PFO (Hampton et al., 2022).
The three major fetal shunts as we have discussed, the ductus venosus, the foramen ovale, and the patent ductus arteriosus, are typically eliminated within the first days of life (Willim et al., 2020). Following the closure of these shunts, postnatal or extrauterine circulation is then established (Willim et al., 2020).
In postnatal or extrauterine circulation, as pictured above, systemic venous blood enters the right atrium from the superior and inferior vena cava (Willim et al., 2020). This poorly oxygenated blood enters the right ventricle and then passes through the pulmonary artery and into the pulmonary circulation, where it becomes oxygenated (Willim et al., 2020). The pulmonary venous blood returns then to the left atrium through the pulmonary veins. This blood then passes through the left side of heart, through the atrium and the ventricle, and then through the aorta to supply systematic circulation of the body (Fernandes, 2024).
When the infant’s lungs expand and become filled with air, the fetal lung fluid is primarily absorbed into the pulmonary capillaries (Fernandes, 2024). Because the lungs provide a more efficient oxygenation of the blood than does the placenta, the neonate's arterial oxygen tension, in turn, rises (Fernandes, 2024). This rise is thought to be the most influential stimulus to constriction of the ductus arteriosus (Fernandes, 2024). The increase in the oxygen tension of the blood bathing the ductus may also contribute to ductal constriction. Acidosis and a fall in prostaglandin levels also help to promote ductal closure (Fernandes, 2024).
If the infant has a congenital heart defect producing increased pulmonary blood flow, such as a patent ductus arteriosus or a ventricular septal defect, pulmonary vascular resistance will not fall as it normally should immediately or shortly thereafter birth (Altman, 2024). These neonates demonstrate a delayed and less apparent drop in pulmonary vascular resistance during the first four to twelve weeks of life (Altman, 2024). It is important to note here that this pressure drop may occur over an even shorter period in the premature neonate (Altman, 2024). Because of this delay, a decrease in pulmonary vascular blood flow and decreased or absent peripheral pulses may fail to become apparent until the child is four to twelve weeks of age (Altman, 2024).
A thorough review of the maternal, fetal, and neonatal history is helpful in the full cardiac assessment and evaluation of the newborn (Geggel, 2021). There are numerous genetic syndromes that are commonly associated with a higher risk of certain congenital heart defects.
The following is a list of hereditary diseasesin which congenital heart disease (CHD) is a frequent finding (Pierpont et al., 2018; Geggel, 2021):
Hereditary
Common Cardiac Disease
Important Features
Apert’s Syndrome
Ventricular septal defect (VSD)
Irregular craniosynostosis with particular head and facial appearances
Coarse facial features, large tongue, depressed nasal bridge, kyphosis, mental retardation retarded growth, hepatomegaly, corneal opacity (not in Hunter’s)
Muscular Dystrophy
Cardiomyopathy
“Pseudohypertrophy” of the calf muscle, waddling gait
Neurofibromatosis (von Recklinghausen’s Disease)
PS, COA
Acoustic neuroma, Café au lait spots, variety of bone lesions
Noonan Syndrome
PS (dystrophic pulmonary valve)
Similar to Turner’s syndrome but may occur in phenotypic male and without a chromosomal abnormality
Osler-Weber-Rendu Syndrome
Pulmonary AV fistulas
Hepatic involvement; Telangiectasias, hemangiomas, or fibrosis
Trisomy 13
VSD
Trisomy 18
VSD, PDA, DORV
Tuberous Sclerosis
Rhabdomyoma
Adenoma sebaceum (2-5 years of age), convulsions mental defect
Turner Syndrome
COA, PS
VATER
VSD, TET
Williams Syndrome (supravalvular aortic stenosis)
Supravalvular aortic stenosis, PA stenosis
Mental retardation, peculiar “elfin” facies, hypercalcemia of infancy
In addition to a genetic review, it is important to evaluate the maternal history for what might be potential causes for a neonatal congenital heart defect. Maternal history that may be associated with congenital heart defects can include (Geggel, 2024):
Maternal infections, especially rubella and influenza, early in pregnancy
Maternal use of tobacco
Maternal use of alcohol
Maternal use of certain drugs known to cause congenital heart defects, including thalidomide, some ACE inhibitors, retinoic acid, NSAIDs, phenytoin, and lithium
Maternal age >40
Thyroid disease
Preeclampsia/Hypertension
Diabetes
Systemic connective tissue disorders
Epilepsy and mood disorders
Obesity
Multifetal pregnancy
Assisted reproductive technology
Family history of CHD
Following a genetic analysis and a maternal history review, neonatal history should be considered. Neonatal history that potentially indicates possible cardiac disease can include (Altman, 2024):
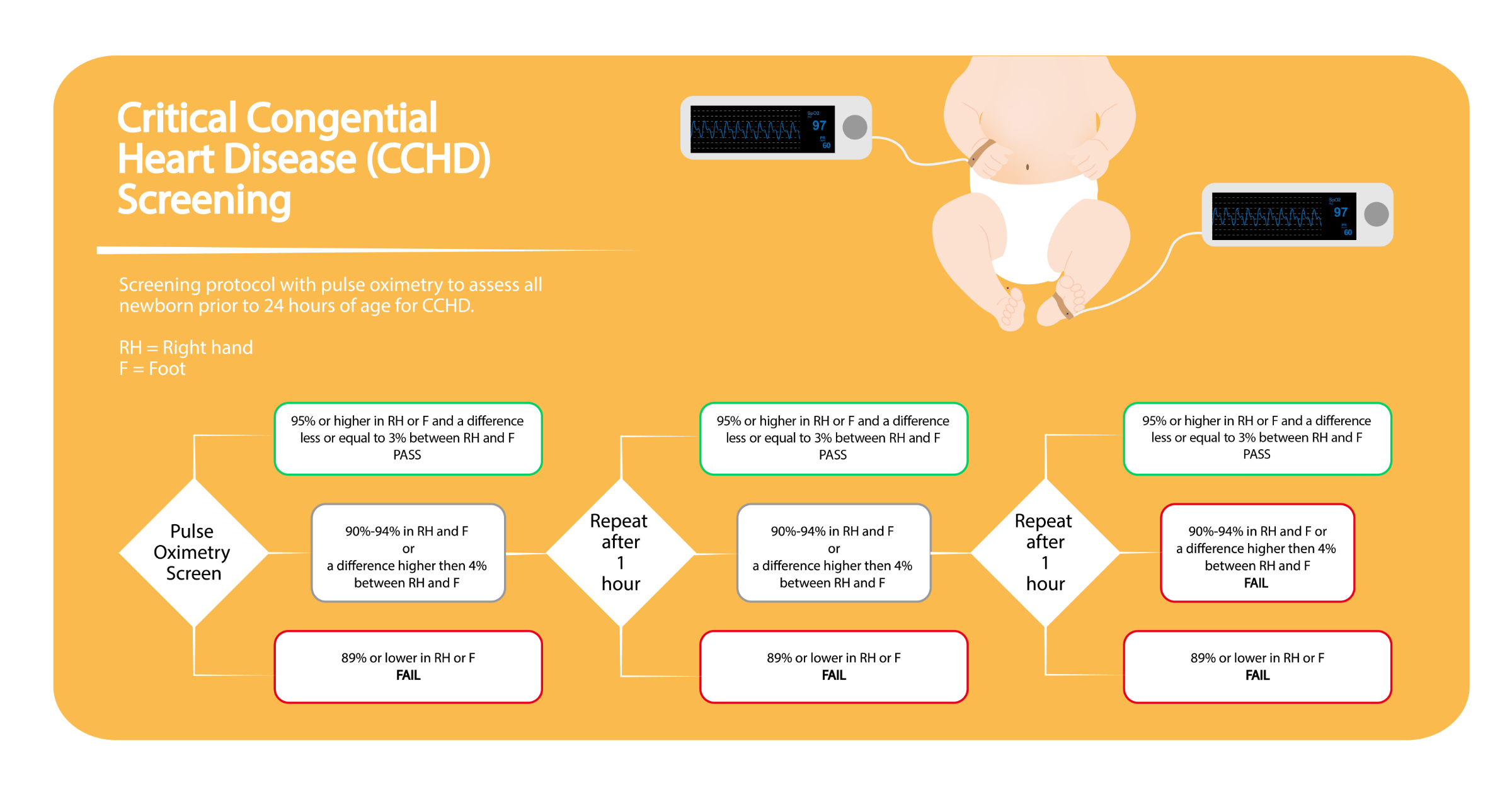
Critical Congenital Heart Disease Screening (CCHD) is a simple test that should be performed on all newborns between the age of 24 to 48 hours (American Academy of Pediatrics [AAP], 2023).
The CCHD is a simple pulse oximetry test that can help to early identify critical congenital heart defects so that a newborn can get treatment before the condition is life-threatening (AAP, 2023). Some of the conditions that the screen may detect include (AAP, 2023; Willim et al., 2020):
Coarctation of the aorta (COA)
Hypoplastic left heart syndrome (HLHS)
Pulmonary atresia (PA)
Tetralogy of Fallot (TOF)
Total anomalous pulmonary venous return (TAPVR)
D-Transposition of the great arteries (d-TGA)
Tricuspid atresia (TA)
A pulse oximetry reading should be obtained from the newborn’s right hand (pre-ductal site) and either foot (post-ductal site). As long as both readings are ≥ 95% Sp02 with a ≤ 3% Sp02 difference between the two readings, the baby passes the CCHD test (AAP, 2023). If either reading is < 90% Sp02, the infant fails. For readings between 90-94% Sp02 or a >3% Sp02 difference, the test should be repeated in one hour. If the same results occur, there should be one more repeat in an hour. The same results again would result in a failure (Willim et al., 2020). An algorithm like the one pictured is useful.
With an infant, it is important to remember that a physical assessment should be done as the child’s behavior and activity allows. Auscultation is a main focus of the cardiac assessment and should be performed at a time when the child is calm and quiet (Gonzalez et al., 2021).
As part of the physical inspection, the nurse should evaluate the newborn's activity: sleeping or awake, alert or lethargic, anxious, or relaxed. The nurse should note the nutritional status of the child, any dysmorphic features, and the activity level of the patient (Gonzalez et al., 2021).
The nurse should also check the infant’s respiratory effort, including signs of respiratory distress such as nasal flaring, expiratory grunting, stridor, retractions, or paradoxical respirations (Gonzalez et al., 2021). Next, the nurse should note the skin color in a well-lit room. For darker-skinned infants, it is essential to assess their mucous membranes (Gonzalez et al., 2021).
Acrocyanosis: Peripheral cyanosis or bluish discoloration of the infant’s hands and/or feet not involving the mucous membranes. It often resolves by 48 hours or with stabilization of the infant.
Circumoral cyanosis: Bluish discoloration around the infant’s mouth which is associated with nipple or breastfeeding and should resolve following the feeding.
Central cyanosis: Bluish discoloration of the tongue and mucous membranes caused by desaturation of arterial blood, indicating cardiac or respiratory dysfunction. Cyanosis may be visible with reduced hemoglobin (Hgb) 3 to 5 gm/dL. Infants with polycythemia (Hgb > 20 gm) may appear cyanotic even when adequately oxygenated. Infants with anemia (Hgb < 10 gm) may not appear cyanotic even when adequately hypoxemic. Pallor may indicate vasoconstriction. Physiologic jaundice may be prolonged. If cyanosis is present, one must differentiate between peripheral and central cyanosis and whether it improves with crying, does not change, or becomes worse with crying (Altman, 2024).
While performing inspection, the nurse should also check for the presence of sweating. Assess for precordial bulging or precordial activity without bulging. Check for pectus excavatum, which may cause a pulmonary systolic ejection murmur or large cardiac silhouette on an anteroposterior chest radiograph because of the decreased anteroposterior chest diameter.
Also be sure to check skin perfusion. Remember, normal capillary refill time is ≤ 3 seconds. Signs of shock can be observed with abnormal skin perfusion when the capillary refill is > 3 seconds, prolonged in the lower body compared with the upper body, and mottling associated with other symptoms (Gonzalez et al., 2021).
During palpation, the nurse should note any hyperactivity. There are two classes of heart disease in which the pericardium appears quite active. This situation can be seen in cases of volume overload present in CHD with large left-to-right shunts, such as PDA or VSD. This finding can also be seen in cases of severe valvular insufficiency, such as aortic or mitral insufficiency.
The nurse should check for a thrill. A thrill is a fine vibration felt by the hand and corresponds to the sound of a murmur (Gonzalez et al., 2021). Thrills are best detected with the palm rather than the fingertips, although the fingertips are crucial to feel a thrill over the carotid arteries or in the suprasternal notch.
The nurse should also determine the point of maximal impulse (PMI). This finding will aid in determining whether the right or left ventricle is dominant. The impulse is maximal at the lower left sternal border if the right ventricle is dominant. If the left ventricle is dominant, the impulse is at the apex.
Next, count the peripheral pulse rate, noting any irregularities or inequalities of rate or volume. Evaluate the carotid, brachial, femoral, and pedal pulses to detect differences between sides and upper and lower extremities (Gonzalez et al., 2021). If pulses are unequal, obtain four extremity blood pressures. The coarctation of the aorta may cause a marked difference. Cuff size is critical. A too narrow cuff gives falsely high readings, and too large a cuff may yield low readings. Assess for bounding pulses. Palpate the abdomen to determine the liver and spleen's size, consistency, and location.
Expert auscultation of the neonatal heart requires much practice over time. The heart of the neonate should be auscultated while the infant is quiet and inactive.
A pediatric or neonatal sized stethoscope with a diaphragm and bell is extremely helpful when auscultating. A pediatric stethoscope has a smaller chest piece than the adult ones do, and a neonatal stethoscope with an even smaller chest piece can be used for examining premature infants. The open bell conducts sound with no distortion, but it makes all sounds loud and may be difficult to maintain an airtight seal. Since low-frequency sounds are hard to hear, the bell is well suited for them. If properly sized, the diaphragm maintains its seal and is useful for high-pitched sounds. The closed diaphragm has a larger diameter than the bell. It is key to note that the bell piece functions as a diaphragm chest piece when applied too firmly to the skin. The skin acts as a diaphragm, and low-frequency sounds are not as easy to detect. The ear tubes must be inclined anteriorly to conform to the direction of the normal ear canal. Proper positioning may be difficult to achieve if the chest piece is too large, resulting in a harsh noise by intermittent contact of skin with the diaphragm. The harsh noise sounds like what could be assumed is a pericardial friction rub.
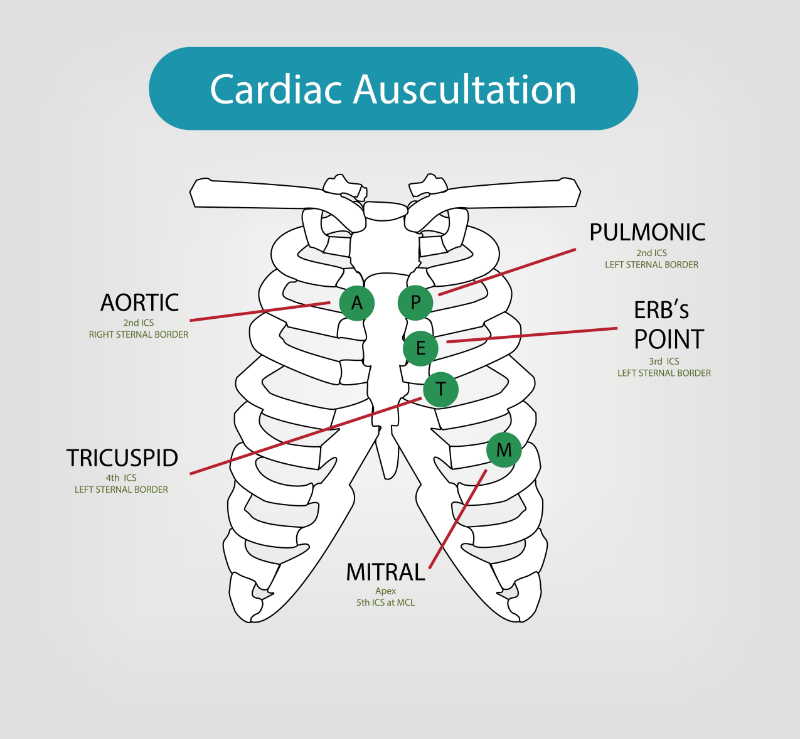
At a minimum, the five traditional auscultatory areas should be examined. These include (Gonzalez et al., 2021):
Aortic area (second intercostal space, right sternal border)
Pulmonic area (second intercostal space, left sternal border)
Erb’s Point (third intercostal space, left sternal border)
Tricuspid area (fourth intercostal space, left sternal border)
Mitral area (the apex, fifth intercostals space, left midclavicular line)
These auscultatory areas can best be remembered with the mnemonic “APE To Man” (Emfietzoglou, 2024):
In addition to the main five sites of auscultation, a more thorough examination is recommended. These additional recommended sites include the right lower border, bilateral axillae, the back, and possibly the anterior fontanelle, while listening for extra heart sounds (Gonzalez et al., 2021).
There are four individual heart sounds: S1, S2, S3, and S4.
S1 is the sound resulting from the closure of the mitral and tricuspid valves after atrial systole. It is best auscultated at the apex of the heart or lower left sternal border. S1 is the beginning of ventricular systole (Geggel, 2023). Splitting of S1 is infrequently noted in newborns.
S2 is the sound that is created by the closing of the aortic and pulmonary valves, which marks the end of systole and the beginning of ventricular diastole. It is best heard in the upper left sternal border or pulmonic area. Evaluation of the splitting of S2 is important diagnostically. The timing of the closure of the pulmonary and aortic valves is determined by the volume of blood that is ejected from the pulmonary artery and the aorta and the resistance against which the ventricles must pump.
In the immediate newborn period, there may be no appreciable splitting of S2. Because the right and left ventricles pump similar quantities of blood and the pulmonary pressure is close to the aortic pressure, these valves close almost simultaneously. Therefore, S2 is heard as a singular sound. As pulmonary resistance decreases and becomes lower than the aortic pressure, this causes a splitting of S2 as the valve leaflets on the left side of the heart (aortic valve) close before those on the right (pulmonary valve). The splitting can be heard in 80% of newborns by 48 hours of age (Altman, 2024).
The absence of a split S2 or a widely split S2 usually indicates an abnormality. A fixed, widely split S2 occurs in conditions that prolong right ventricular ejection time or shorten left ventricular ejection time (Altman, 2024). This may be heard with pulmonary valve stenosis or severe mitral regurgitation (Geggel, 2023). A narrowly split S2 occurs in conditions where there is the early closure of the pulmonary valve (pulmonary hypertension) or a delay in aortic closure (Altman, 2024). A single S2 sound is significant because it could represent the presence of only one semilunar valve (like in aortic or pulmonary atresia, or in truncus arteriosus) (Altman, 2024).
The relative intensity of the aortic and pulmonary components of S2 must be assessed. The aortic component is usually louder than the pulmonary component in the pulmonic area. Compared with the aortic component, increased intensity of the pulmonary component occurs with pulmonary hypertension. Conditions that cause decreased diastolic pressure of the pulmonary artery (critical pulmonary stenosis, tetralogy of Fallot (TOF), tricuspid atresia) may cause the decreased intensity of the pulmonary component (Geggel, 2023).
S3 and S4 are rarely auscultated in the newborn. Since S3 and S4 are rarely heard in the neonatal period, their presence denotes a pathologic process. Likewise, a gallop rhythm, the result of a loud S3 and S4 sound, and tachycardia are considered abnormal (Geggel, 2023).
After evaluating the individual heart sounds, the systolic and diastolic sounds are evaluated. The ejection sound or click occurs after S1 and may sound like a splitting of S1. The ejection click is best heard at the upper left or right sternal border or base. (Geggel, 2023).
Heart murmurs are evaluated in multiple ways. They are assessed for their location, or where they are best auscultated. They are also assessed for their transmission, or where they might be transmitting sound from or to the area where they are best heard. In addition to location and transmission, cardiac murmurs should be assessed for their:
Intensity (grades 1 to 6)
Timing (systolic or diastolic)
Quality (musical, vibratory, or blowing)
Murmurs are graded for intensity on a scale from 1 to 6 (Geggel, 2023):
Grade 1: Barely audible
Grade 2: Soft but easily audible
Grade 3: Moderately loud; No thrill
Grade 4: Loud; Thrill present
Grade 5: Loud; Audible with stethoscope barely on chest
Grade 6: Loud; Audible with stethoscope not touching the chest
A barely audible grade 1 murmur is recorded as “1/6”, and so on.
It is also important to note the quality of the murmur heard. The common descriptions used for quality include (Geggel, 2023):
Harsh
Blowing
Rumbling
Vibratory or musical
The next step in evaluating a murmur is its classification in relation to S1 and S2. The three types of murmurs are systolic, diastolic, and continuous. It is still important to appreciate that an infant who is found to have no murmur may still have significant cardiac disease (Gonzalez et al., 2021).
Most heart murmurs are systolic, arising between S1 and S2. Systolic murmurs are either ejection or regurgitation murmurs. These murmurs are a normal variation that is often identified during the routine physical exam of a healthy infant. Studies have shown that many healthy children have a benign murmur at some time during their lives.
The cardiac blood flow causes ejection murmurs through stenotic or deformed valves or increased flow through normal valves. Systolic murmurs that are described as regurgitant begin with S1, with no interval between S1 and the beginning of the murmur. Regurgitation murmurs generally continue throughout systole. Regurgitation systolic murmurs are caused by blood flow from a chamber at a higher pressure throughout the systole than in the receiving chamber. Regurgitation systolic murmurs are often associated with these conditions (Geggel, 2023):
Diastolic murmurs are classified according to their timing in relation to heart sounds as early diastolic, mid-diastolic, or pre-systolic.
Diastolic murmurs are considered pathologic and require evaluation (Gonzalez et al., 2021). They result from either:
Aortic regurgitation
Pulmonary insufficiency
With aortic regurgitation, the murmur is high-pitched and blowing. It begins with the second heart sound and is loudest in early diastole. It may be missed because it is often very soft or may even be mistaken for breath sounds because of its high pitch. Bounding pulses are present.
The murmur of pulmonary insufficiency is a distinctive diastolic murmur. It is low-pitched, early in onset, and of short duration. It ends well before the first heart sound. It occurs with postoperative TOF, pulmonary hypertension, postoperative pulmonary valvotomy for pulmonary stenosis, or other deformities of the pulmonary valve (Geggel, 2023).
Mid-diastolic murmurs result from abnormal ventricular filling. Due to stenosis, the murmur results from turbulent flow through the tricuspid or mitral valve. They are associated with mitral stenosis or large left-to-right shunt VSD or PDA, producing relative mitral stenosis secondary to increased flow across the normal-sized mitral valve. It is seen in atrial septal defect (ASD), total or partial anomalous pulmonary venous return (TAPVR, PAPVR), endocardial cushion defects, or abnormal stenosis of the tricuspid valve (Geggel, 2023).
Most continuous murmurs are not audible throughout the cardiac cycle. They begin in systole and extend into diastole. They are a pathologic finding. They can be produced in rapid blood flow, high-to-low pressure shunting, and localized arterial obstruction.
The most significant is the PDA with high-to-low shunting (Geggel, 2023). The patency of the ductus is normal in the first 24 hours of life, but a few weeks later, a patent ductus is abnormal. It is more common in girls (girl to boy ratio of 3:2), tends to affect siblings, and may be a complication of maternal rubella. It is said to be substantially more common in infants born at high altitudes and more common in premature infants. There may be a vigorous pericardial activity, a systolic thrill, and bounding pulses if the ductus is large. There may also be symptoms of congestive heart failure (CHF) or arteriovenous malformation (AVM) (Geggel, 2023).
It is important to note the location of the murmur because this can help distinguish what the cause of the murmur might be (Geggel, 2023). We talked about the main sites for cardiac auscultation above. Please refer to the image above as needed.
Left Upper Sternal Border: Murmurs heard at this location are usually associated with right ventricular outflow obstruction and can be caused by:
Pulmonary stenosis
Aortic regurgitation
Pulmonary regurgitation
PDA
Cervical venous hum
Right Upper Sternal Border: Murmurs heard here are usually associated with left ventricular outflow obstruction and can by caused by:
Aortic stenosis
Left Lower Sternal Area: Murmurs located here can be an innocent murmur or may be caused by:
VSDs
Tricuspid regurgitation
Subvalvular aortic stenosis
Hypertrophic cardiomyopathy
Semilunar valve regurgitation
Apex: May radiate to the axilla. These murmurs are usually caused by:
Mitral regurgitation
Mitral stenosis
Other locations: Coarctation of the aorta may cause a murmur heard on the back between the scapulae. Large AVMs can cause murmurs in other areas, including the cranium.
Cardiac development occurs during the first seven weeks of gestation. Causes of congenital heart defects are classified as either chromosomal, genetic, maternal, environmental, or multifactorial. The vast majority of congenital heart defects are considered to be of multifactorial origin. These defects are probably the result of an interaction effect of the other causes. Congenital heart defects affect approximately 6 to 13 per 1000 live births (Geggel, 2023).
Acyanotic heart defects are those that produce a left-to-right shunt. Typically, these defects do not produce cyanosis because sufficient oxygenated blood is in circulation. The left-to-right or right-to-left shunts increase pulmonary blood flow and workload on the heart (AHA, 2022).
Patent ductus arteriosus, or a PDA, is the failure of the ductus to close off in response to increased arterial oxygen concentrations after the initiation of respiration utilizing the lungs.
Image 7: Normal vs. PDA
The persistence of the ductus arteriosus remaining open is beyond 24 hours. A systolic murmur is heard. Bounding peripheral pulses help differentiate a PDA from a Ventricular Septal Defect (VSD). The precordium is usually active. Some infants will have widened pulse pressures. Infants weighing < 1,000 grams are likely to have reduced systolic and diastolic pressures. The volume overload of blood in the left atrium and left ventricle leads to increased pulmonary venous engorgement. In addition to the systolic murmur and bounding pulses, CHF symptoms that can also be seen include (Colombo & McCulloch, 2018):
Dyspnea
Tachypnea
Hoarse cry
Frequent lower respiratory tract infections
Coughing
Poor weight gain
The timing of PDA treatment is controversial with three broad approaches to timing:
Targeted presymptomatic treatment
Prophylactic treatment
Treating when and if the PDA becomes clinically symptomatic
None of the above treatment options has demonstrated clear, confirmatory benefits in short and long-range outcomes. It is significant to note that the prophylactic approach to PDA treatment is the only strategy that has been shown to have benefits of any sort (Colombo & McCullouch, 2018).
Medical management for PDA includes prophylactic antibiotics against bacterial endocarditis and prostaglandin inhibitors. Prostaglandins are what are given to the infant to help to prevent the ductus from closing. The definitive treatment is surgical ligation of the opening but there are risks involved. Therefore, treatment should be based case by case (Colombo & McCullouch, 2018).
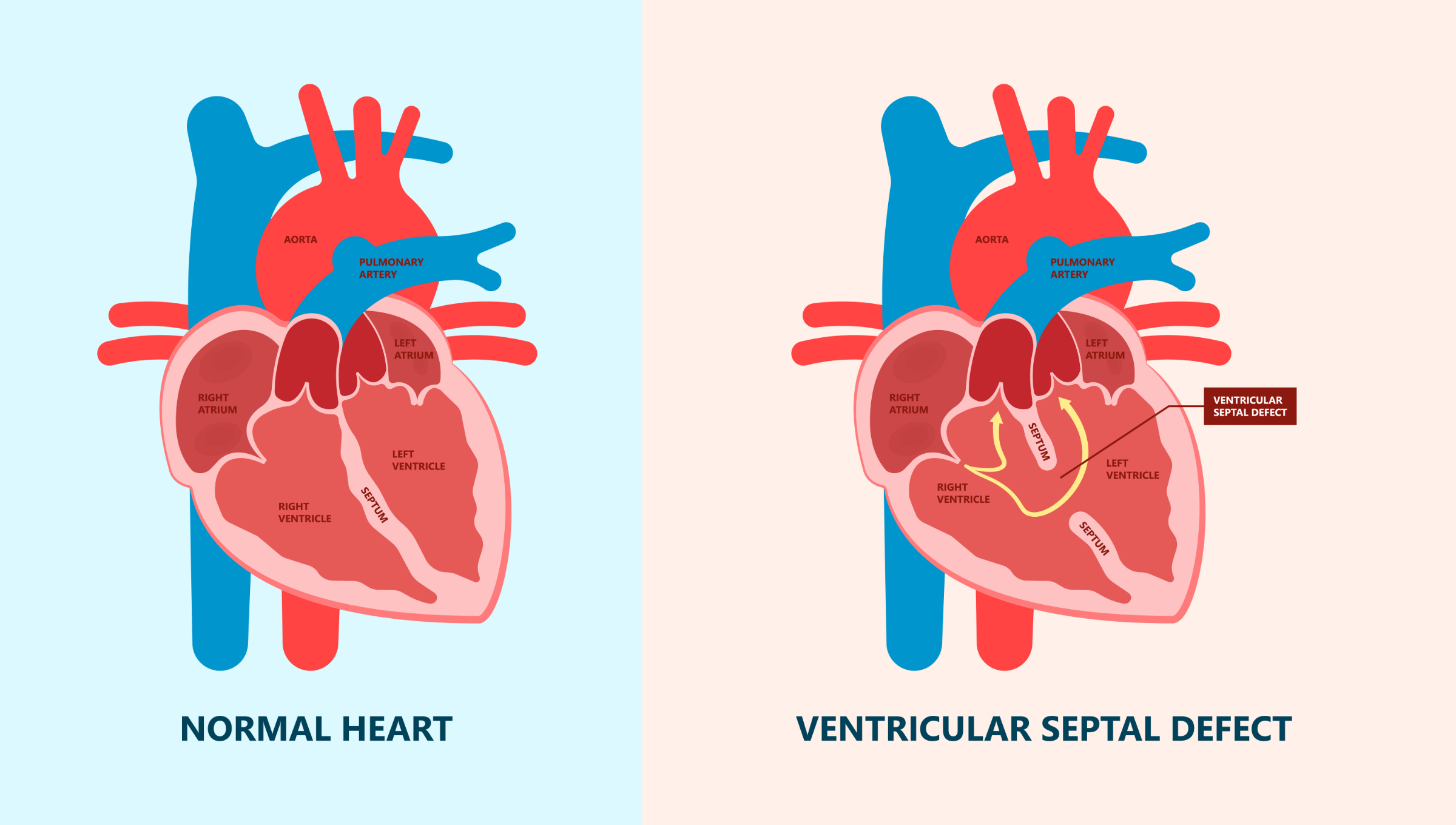
Ventricular septal defects, or VSDs, are the most common form of congenital heart disease (Colombo & McCullouch, 2018). They can occur anywhere along the ventricular septum. The size of the defect and the degree of pulmonary vascular resistance are more important to severity than location.
Image 8: Ventricular Septal Defect
(*Please click on the image above to enlarge.)
Up to 45% of VSDs will spontaneously close within the first year after birth (Colombo & McCullouch, 2018). It is typical that a chest X-ray will be normal and not show any sign of smaller VSD. With VSDs, there is usually a loud, harsh pansystolic murmur. The symptoms of a VSD will depend on the severity of the defect itself. These symptoms might range from asymptomatic completely to poor exertional tolerance, recurrent pulmonary infections, and symptoms of CHF (Colombo & McCullouch, 2018). With severe VSD, there may be pulmonary hypertension and cyanosis (Colombo & McCullouch, 2018).
Management of VSD includes monitoring for CHF and treatment with diuretics and digitalis. Unless there is pulmonary hypertension, there is no activity restriction. Prophylaxis against bacterial endocarditis may be implemented prior to surgical closure of the VSD if surgery is indicated (Colombo & McCullouch, 2018).
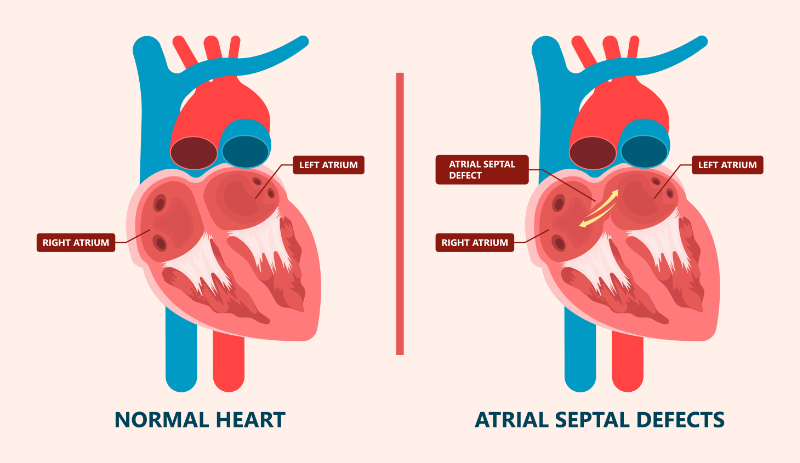
Atrial septal defects, or ASDs, are an opening or a communication between the right and left atria.
Image 9: Atrial Septal Defect
With an ASD, there is increased blood flow to the right ventricle through the pulmonary valve. It is known that 40% of cases are associated with Trisomy 21 (Colombo & McCullouch, 2018). This malformation creates the typical ejection murmur, usually grade 2 to 6. It can include the ventricles as well. The infant is usually asymptomatic unless a murmur is present. The chest X-ray may show enlargement and an increase in pulmonary vascularity (Colombo & McCullouch, 2018). Untreated ASD can lead to CHF, pulmonary hypertension, and atrial arrhythmias (Colombo & McCullouch, 2018).
A natural closure of ASDs is possible in the first five years of age in up to 40% of children (Colombo & McCullouch, 2018). The medical management of ASD includes prevention and treatment of CHF. Activity is not restricted. Surgical correction is accomplished with a patch or with direct closure (Colombo & McCullouch, 2018).
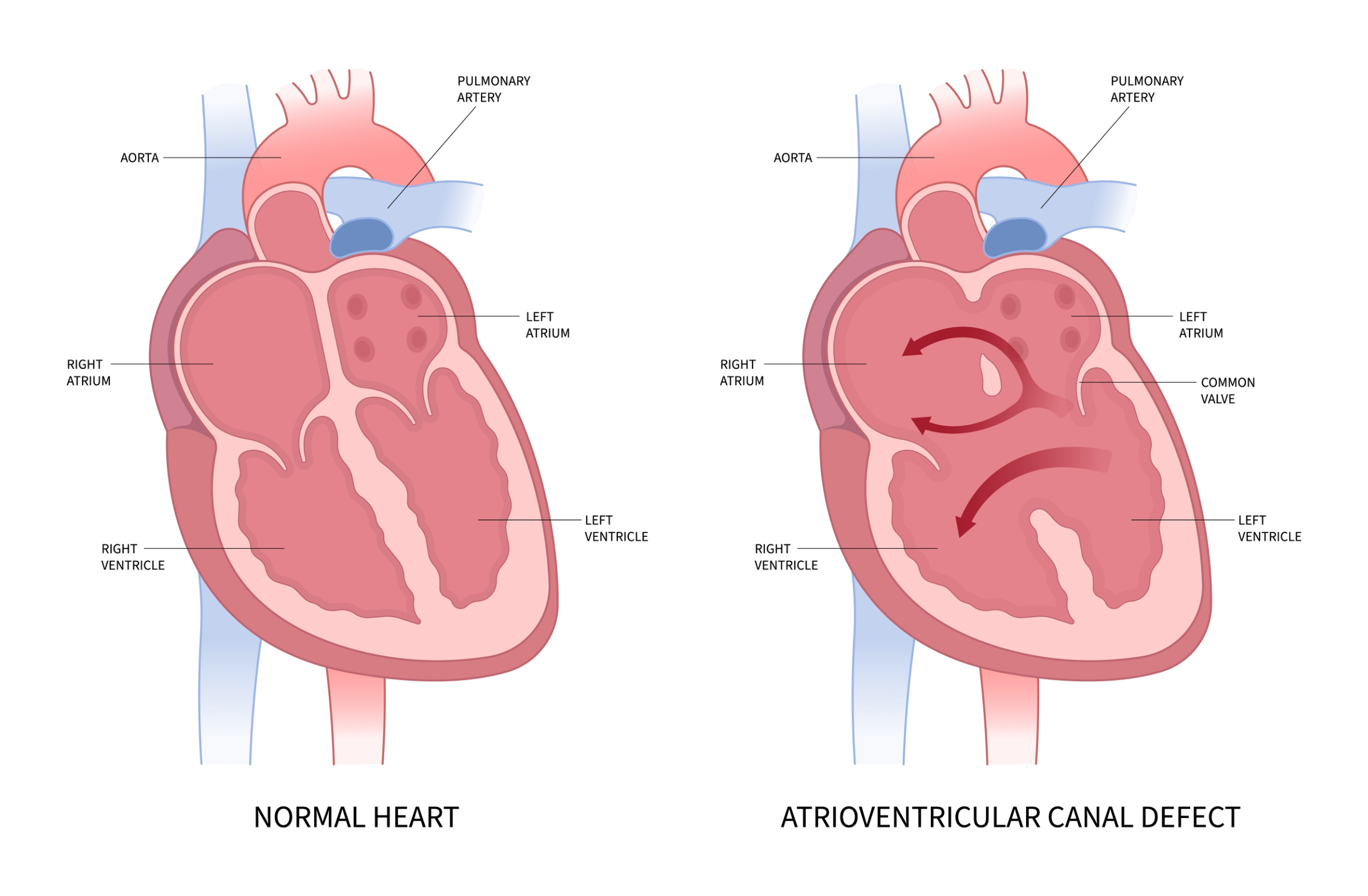
Endocardial cushion defects are also known as atrioventricular septal defects (AVSDs) or atrioventricular canal defects. In this case, these are lesions that produce abnormalities of the atrial septum, ventricular septum, and AV valves.
Image 10: Atrioventricular Canal Defect
(*Please click on the image above to enlarge.)
Symptoms of AVSDs result from increased pulmonary blood flow caused by the abnormal connection between the ventricles and the atria (Colombo & McCullouch, 2018).
An infant with an AVSD may present with respiratory distress, signs of CHF, tachycardia, and a murmur. The mitral regurgitation may generally be heard as a grade 3 holosystolic murmur transmits to the back. A chest x-ray will reveal generalized cardiomegaly and increased pulmonary vascularity (Colombo & McCullouch, 2018).
The infant will generally have recurrent respiratory infections and might even be diagnosed with failure to thrive. There is a strong association with Down syndrome (Fleishman & Tugertimur, 2022).
The management of AVSD is aimed at preventing or treating CHF and bacterial endocarditis (Colombo & McCullouch, 2018). The surgical closure of the ASD and the VSD in addition to the reconstruction of the AV valves is often required (Colombo & McCullouch, 2018). In some cases, pulmonary artery banding may be performed as a palliative procedure if there is no evidence of significant mitral regurgitation. Surgery will be indicated when CHF is unresponsive to medical therapy (Colombo & McCullouch, 2018). Surgery might also indicated if the child has recurrent pneumonia, failure to thrive, or a large shunt with the development of pulmonary hypertension and increased pulmonary vascular resistance (Colombo & McCullouch, 2018).
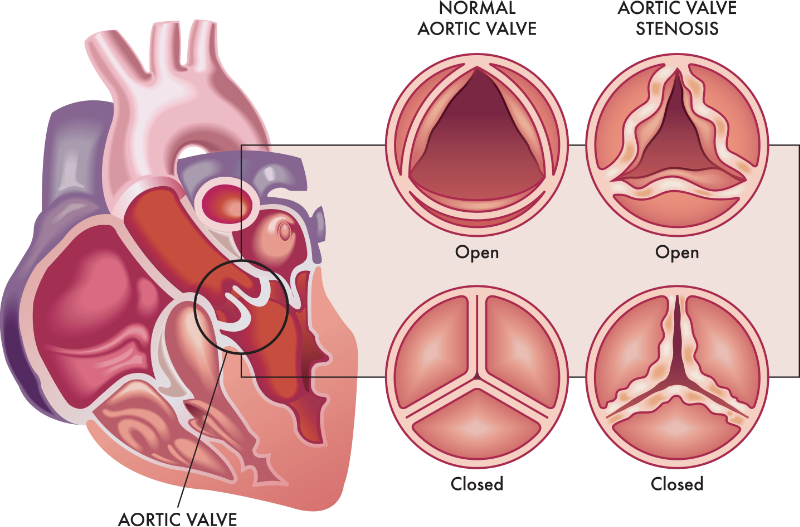
Aortic stenosis is one of a group of defects that produce obstruction to ventricular outflow (AHA, 2022). This is when there is a narrowing or thickening of the aortic valve (AHA, 2022).
Image 11: Aortic Stenosis
The symptoms of aortic stenosis depend on defect severity. Mild stenosis can be asymptomatic. More severe stenosis is associated with activity intolerance, chest pain, and CHF. There may even be an evident narrow pulse pressure and higher systolic pressure in the right arm. Cardiomegaly is present with CHF.
The management of aortic stenosis includes preventing and treating CHF with fluid restriction, diuretics, and digitalis. Some activity restrictions may be necessary to prevent increased demand on the heart in more moderate to severe cases of aortic stenosis (AHA, 2022). Balloon valvuloplasty may be performed during cardiac catheterization to improve circulation. In critical cases, maintenance of the patency of the ductus arteriosus with prostaglandin E1 to prevent hypoxia may be needed. The type and timing of surgical correction depend on the exact location and severity of the defect.
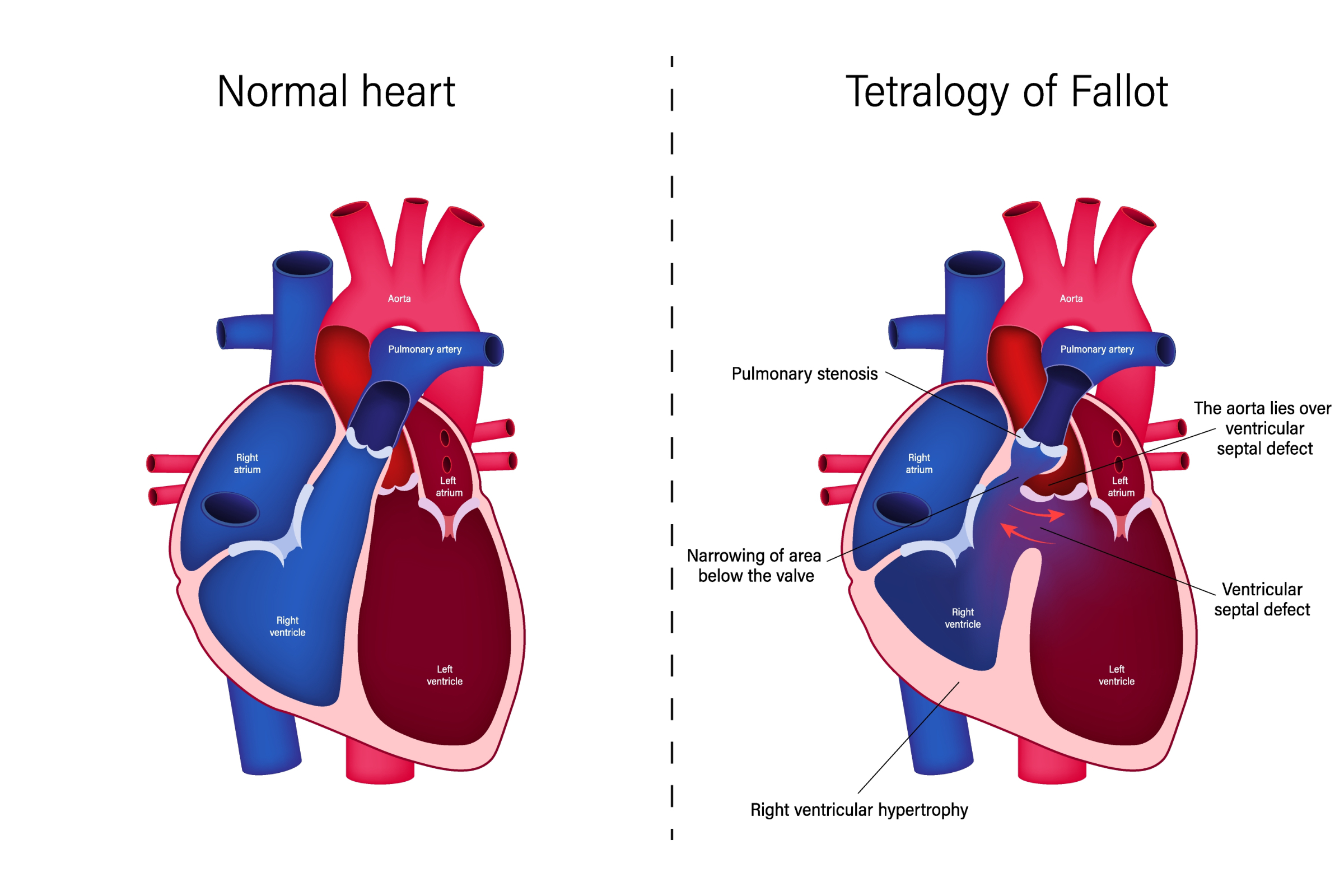
Tetralogy of Fallot, or TOF, is comprised of the four abnormalities, hence “tetra” in “tetralogy”, indicating the presence of four parts. The four defects that define TOF include (Geggel, 2021):
Ventricular septal defect (VSD)
Pulmonary stenosis (PS)
Overriding aorta
Right ventricular hypertrophy (RVH)
Image 12: Tetralogy of Fallot
(*Please click on the image above to enlarge.)
In cases of TOF, blood is shunted from right to the left through the VSD and the overriding aorta (Geggel, 2021). The murmur of TOF is loudest along the left sternal border between the third and fourth interspaces. A thrill will be present if the murmur is at least a grade 3. There is also usually a single-second heart sound. Cyanosis depends on the varying degrees of pulmonary stenosis (Geggel, 2021). The chest X-ray demonstrates an enlargement of the right ventricle, small main pulmonary artery, and a normal left atrium and left ventricle. TOF has been called a "boot-shaped" heart. The EKG would also show right ventricular hypertrophy (Geggel, 2021).
The cardinal signs of TOF include (Geggel, 2021):
Cyanosis
Hypoxia
Dyspnea
Severe decompensation or what are often called "tet spells” are common in infants or children but can also occur in neonates with untreated TOF (Geggel, 2021). In a “tet spell”, the infant or child becomes symptomatic when their oxygen levels drop quickly without warning (Cleveland Clinic, 2022a). This can happen randomly but most often during episodes of physical exertion (Cleveland Clinic, 2022a). The signs and symptoms of a “tet spell” include (Cleveland Clinic, 2022a):
Lips turning blue or gray
Skin/nails turning blue
Losing consciousness
Respiratory difficulty
Being restless
Fatigue
Limp body
These spells can last just a few short moments or as long as several hours (Cleveland Clinic, 2022a). Often out of an attempt to compensate for the experienced symptoms during a “tet spell”, children will instinctively assume a squatting position, in which their knees are pushed into their chest (Cleveland Clinic, 2022a). This position will help them to increase their systemic vascular resistance and aortic pressure, which in turn helps to decrease right-to-left blood shunting and then help to raise arterial oxygen saturation (Beerman, 2023a; Cleveland Clinic, 2022a).
Over time if TOF goes untreated, chronic arterial desaturation will stimulate erythropoiesis, causing polycythemia that may lead to increased blood viscosity, microcytic anemia, and cerebrovascular accident.
Definitive therapy for TOF is surgical repair. Medical management of TOF includes the prevention and treatment of hypoxemia, infection, polycythemia, and microcytic hypochromic anemia. It is important to avoid dehydration in these children to prevent an increased risk of cerebral infarcts because of hemoconcentration. Surgical management may be either palliative or corrective, with palliative procedures undertaken to improve pulmonary blood flow by creating a pathway between systemic and pulmonary circulation (AHA, 2022).
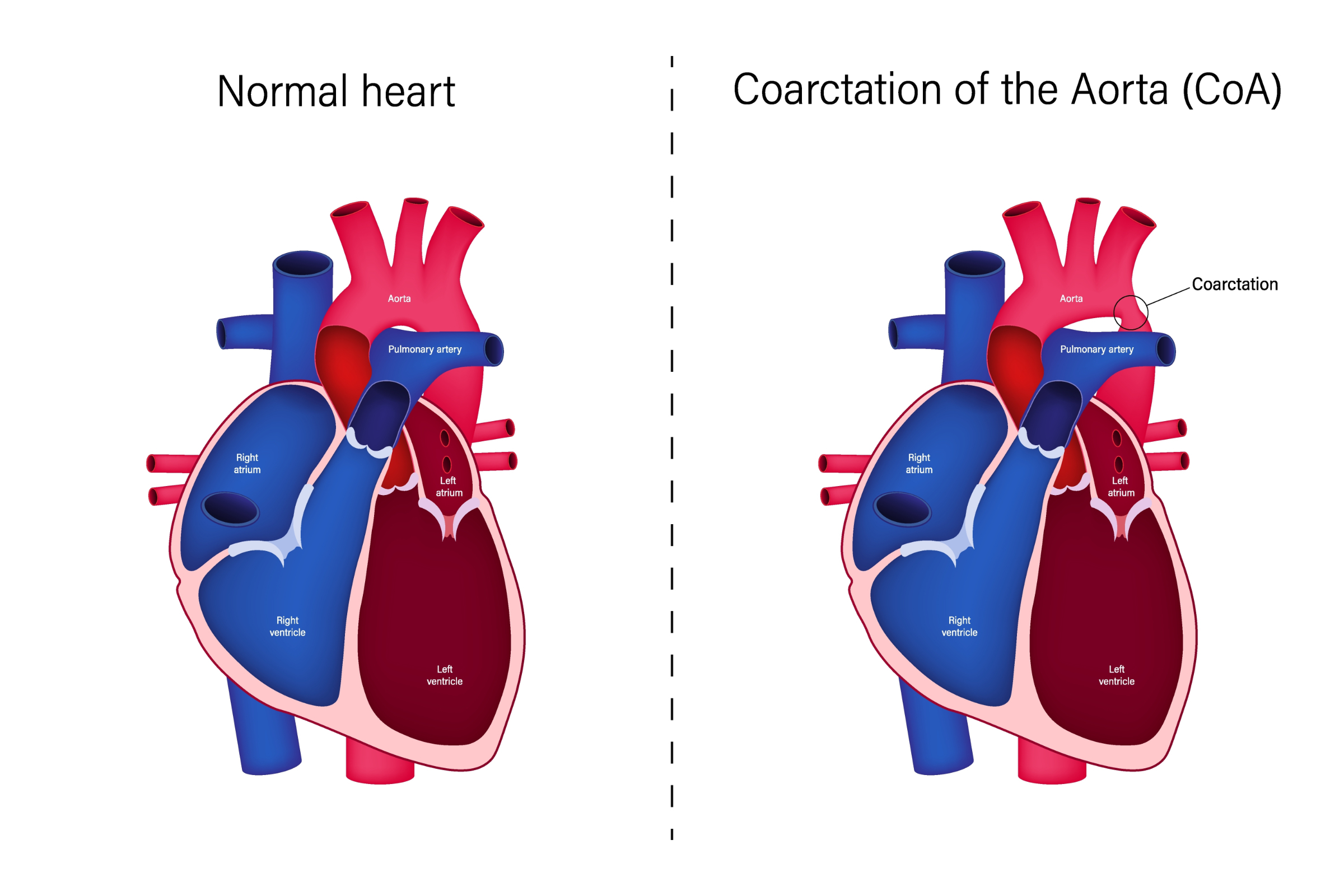
The coarctation of the aorta, or COA, obstructs the flow from the proximal portion of the aorta to its distal portion.
Image 13: Coarctation of the Aorta
(*Please click on the image above to enlarge.)
If the coarctation defect is near to the insertion of the ductus arteriosus, the lower half of the body will be supplied by the right ventricle through the ductus and would generally be cyanotic. The upper half of the body would then be supplied by the left ventricle and should be oxygenated. On chest X-ray, cardiomegaly is evident. An EKG will consistently show right ventricular hypertrophy. Hypertension in the upper extremities and lower pressure in the lower extremities can be expected. Femoral pulses will be present but will be weaker.
With COA, typically, no murmur is present. The second heart sound will be closely split. If the coarctation is distal to the insertion of the ductus arteriosus, collateral circulation will be established during fetal life to permit perfusion to the lower half of the body.
In COA, the symptoms will be dependent on the severity of the narrowing of the aorta (Mayo Clinic, 2024). In the case of smaller defects, it is possible it will be years before a diagnosis or, in some cases, COA might not ever be identified (Mayo Clinic, 2024). In the cases of more extreme narrowing, the infant may present with (CDC, 2024a; Mayo Clinic, 2024):
CHF (difficulty breathing, changes in skin color, heavy sweating)
Absent, weak, or delayed pulses in the lower extremities
Bounding pulses in the upper extremities
Higher blood pressures in the upper extremities than in the lower extremities
There may be a systolic thrill felt at the suprasternal notch. If the obstruction is mild, as alluded to above, the infant may not have any symptoms at all (AHA, 2022).
For more severe COA, surgery is necessary (CDC, 2024a; Mayo Clinic, 2024). Surgery is performed at three to five years of age if signs and symptoms can be medically controlled until that point. Surgery is required earlier if medical management fails to provide adequate oxygenation, prevent CHF, and avoid sub-acute bacterial endocarditis. Prostaglandin E1 may be administered as necessary to maintain ductal patency if the constricted segment is at the level of the ductus arteriosus, to allow for improved blood flow for the time being (Beerman, 2023b).
Pulmonary atresia is a defect in which there is an absence of a communication opening between the pulmonary artery and the right ventricle. With pulmonary atresia, the right ventricle is usually hypoplastic, with thick ventricular walls. The presence of a PDA, ASD, or PFO to allow blood mixing is crucial for survival. Cyanosis and tachypnea are typical symptoms that are present without other signs of obvious respiratory distress. A soft systolic murmur is generally heard at the upper left sternal border. Heart size may be normal or enlarged. There are decreased pulmonary vascular markings.
As far as treatment, prostaglandins are used to maintain ductal patency until balloon atrial septostomy can be done to promote the mixing of systemic and pulmonary venous blood in the atria. Surgical correction is performed by creating a systemic-pulmonary artery shunt between the left subclavian artery and the left pulmonary artery. Cardiac transplant may be necessary in infants with severe cases (Axelrod & Roth, 2023).
Pulmonary stenosis is a defect in which the pulmonary valve is narrowed. This makes it difficult for blood to flow from the heart to the lungs. Pulmonary stenosis causes the right ventricle to pump harder to get blood past the blockage.
The resulting cyanosis depends on the severity of the stenosis. Valvuloplasty may be used during cardiac catheterization in order to stretch the valve (AHA, 2022). A moderate level of pulmonary stenosis may cause easy tiring. Severe or critical pulmonary stenosis will cause CHF. A pulmonary systolic ejection “click” at the upper left sternal border and widely split S2 or systolic ejection murmur (grade 2/6 to 5/6) at the upper left sternal border and transmits across the back is commonly what is found during auscultation.
The surgical correction of pulmonary stenosis is performed in children when the right ventricular pressure measures 80 to 100 mmHg, and balloon valvuloplasty is unsuccessful. Infants with critical pulmonary stenosis and CHF require prostaglandin infusion to maintain ductal patency until surgery.
Truncus arteriosus, or TA, results from the inadequate division of the common great vessel into a separate aorta and pulmonary artery (AHA, 2022). Cyanosis may be present, depending on the amount of pulmonary blood flow. A systolic click and harsh VSD murmur may be present. On chest X-ray, the heart size is visually increased. As far as signs and symptoms of truncus arteriosus, CHF, bounding arterial pulses, and widened pulse pressures are present. If truncus arteriosus is not detected in the newborn period, the infant will feed poorly, fail to thrive, have frequent respiratory infections, and demonstrate worsening CHF.
The treatment of truncus arteriosus involves control of CHF symptoms and prophylaxis with antimicrobial agents. Pulmonary artery banding is a palliative measure in small infants with increased pulmonary blood flow and CHF that does not respond to medical management. The definitive surgical correction is performed during infancy.
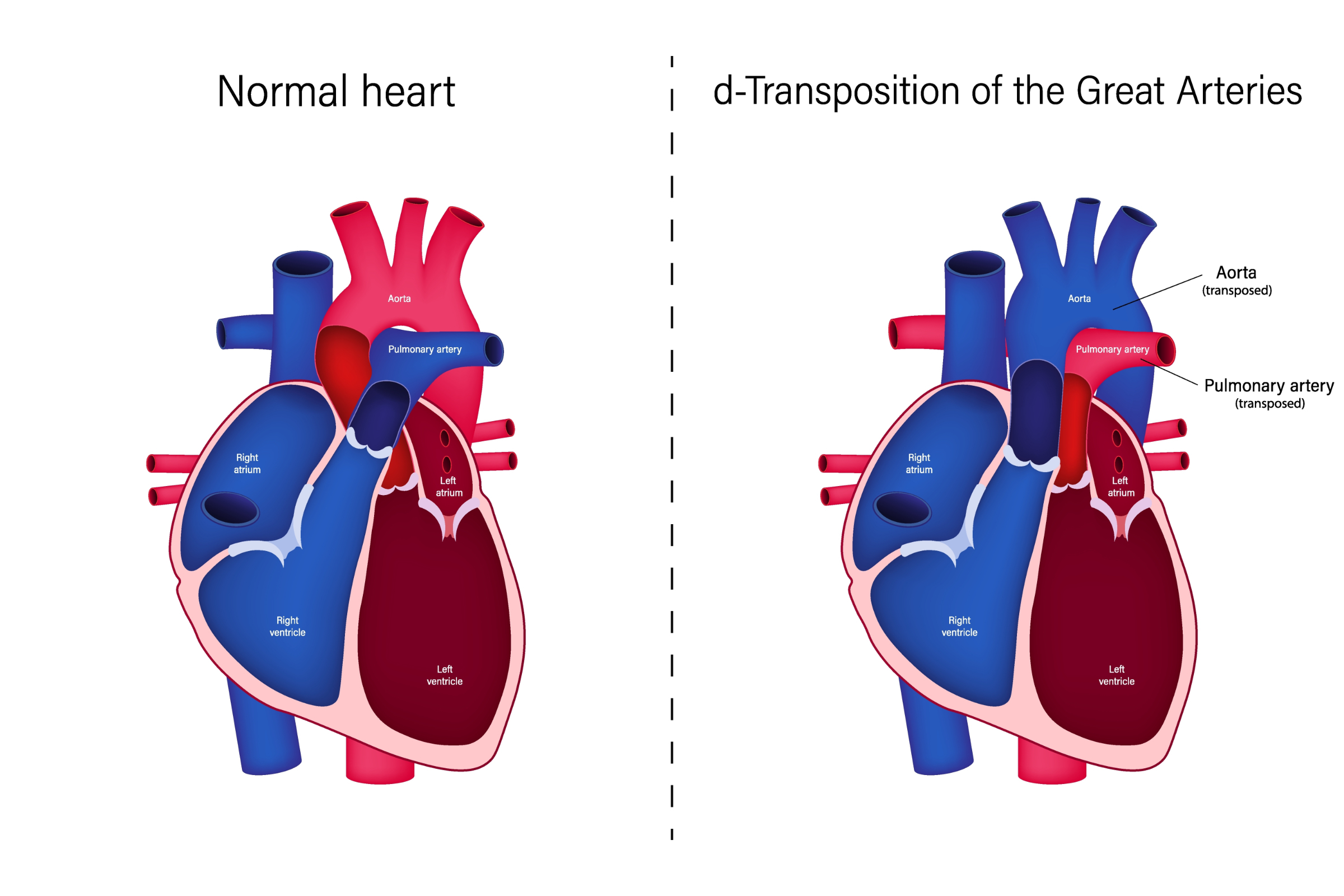
D-Transposition of the Great Arteries, or D-TGA, is a life-threatening cardiac defect in which the pulmonary artery and the aorta have switched positions in the heart, or in other words are “transposed” (CDC, 2024b).
Image 14: d-Transposition of the Great Arteries
(*Please click on the image above to enlarge.)
In d-TGA, the aorta receives unoxygenated blood and returns it to the systemic circuit. Basically, there are two separate parallel circulations going on at the same time and not allowing for mixing (Geggel, 2024). Marked cyanosis is present, as well as signs of CHF. There will be a loud, harsh systolic murmur. Hypoglycemia, hypocalcemia, and metabolic acidosis are frequently present. On chest X-ray, the heart is enlarged and has a narrow base. It is often described as being “egg-shaped”.
D-TGA is a cardiac emergency (CDC, 2024b). Immediate management includes the correction of acidosis, hypoglycemia, and hypocalcemia. Oxygen and prostaglandins are administered. Cardiac catheterization with balloon atrial septostomy is done. The prognosis for d-TGA without surgical intervention is poor. Definitive surgical correction is done by switching the right and left-sided structures at the ventricular, artery, or atrial levels (CDC, 2024b).
Tricuspid atresia, or TA, is a life-threatening congenital cardiac condition in which the tricuspid valve does not form properly if at all (CDC, 2024c). Because there is no tricuspid valve, no blood can flow from the right atrium to the right ventricle (Geggel, 2024).
Because of the fact that the right ventricle is small, survival depends on an ASD or VSD to allow for blood flow. Most poorly oxygenated blood goes from the left ventricle into the aorta and onto the body. The rest of the blood flows through the VSD to the small right ventricle to the pulmonary artery and back to the lungs. The infant will be cyanotic.
In Total Anomalous Pulmonary Venous Return, or TAPVR, the pulmonary veins drain into the right atrium (rather than the left atrium) (Karmegaraj, 2022). There is no direct connection between the pulmonary veins and the left atrium.
In TAPVR, cyanosis is present, as well as respiratory distress. Feeding is associated with increased cyanosis, the infant tires easily and has progressive growth failure. Increased cyanosis associated with feeding is secondary to the compression of the common pulmonary vein by the filled esophagus.
Upon auscultation, a grade 2/6 to 3/6 systolic ejection murmur will be heard at the left sternal border. A precordial bulge and hyperactive right ventricular impulse may also be seen. The PMI is at the xiphoid process or lower left sternal border. The pulmonic sound may be more pronounced. A quadruple or quintuple gallop rhythm is generally heard.
The chest X-ray findings include mild to moderate cardiomegaly and increased pulmonary markings. The characteristic "snowman sign" occurs because of the anatomic appearance of the left superior vena cava, the left innominate vein, and the right superior vena cava (Karmegaraj, 2022). This anatomy results in a chest X-ray shadow that resembles the shape of a snowman (Karmegaraj, 2022).
Treatment for TAPVR is focused on preventing CHF and hypoxemia. Diuretics may be administered to decrease pulmonary edema, and balloon atrial septostomy performed to enlarge the interatrial communication to promote better blood mixing. Surgery that is done in early infancy improves outcomes (AHA, 2022).
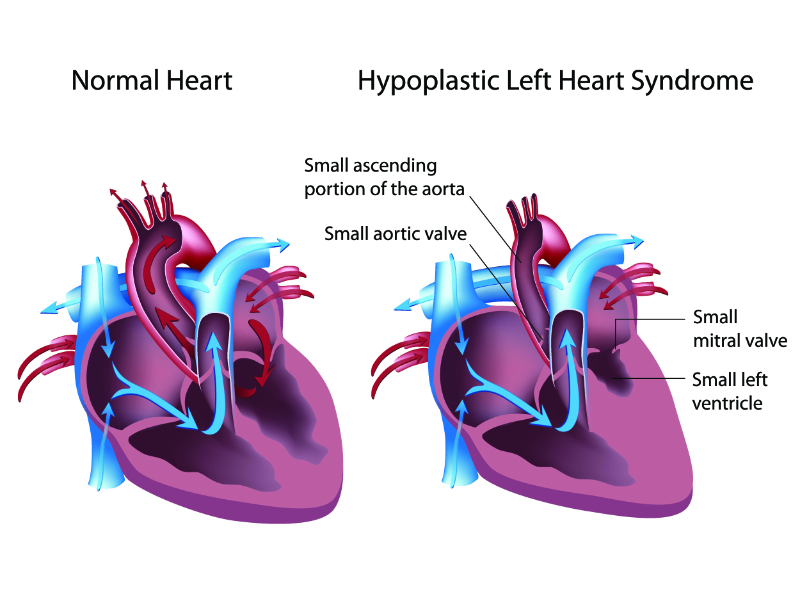
Hypoplastic Left Heart Syndrome, or HLHS, is a defect in which the left side of the heart does not form correctly during development. HLHS consists of a group of defects, including a small aorta, a smaller aortic valve, mitral valve stenosis, and a small left atrium and ventricle (Cleveland Clinic, 2022b).
Image 15: Hypoplastic Left Heart Syndrome
The infant with HLHS will often present with (Geggel, 2024; Cleveland Clinic, 2022b):
Progressive cyanosis
Pallor
Mottling
Tachycardia
Tachypnea
Dyspnea
Pulmonary rales
Upon auscultation, the second heart sound is loud and single. Poor peripheral pulses and vasoconstriction of the extremities are generally noted on the physical exam. On chest X-ray, mild to moderate heart enlargement and pulmonary venous congestion is seen.
The management of HLHS is aimed at the prevention of hypoxemia and correction of metabolic acidosis. Prostaglandins are administered to maintain ductal patency. Balloon atrial septostomy is done to decompress the left atrium. Modern medical and surgical interventions have improved the odds of living over the age of 5, but there is a high morbidity rate associated with this condition (Geggel, 2024).
Diuretics are used in the treatment of CHF to decrease fluid overload and fluid retention. The following is a list of diuretic options with their respective doses and routes of administration:
Furosemide (Lasix®) – 0.5-1.0 mg/kg/dose IV every 12 to 24 hours
Spironolactone (Aldactone®) – 1-3.0 mg/kg/day PO
Chlorothiazide (Diuril®) – 10-40 mg/kg/day PO or 5 to 10 mg/kg/day IV
Inotropic agents are used to increase myocardial performance by increasing the strength of contraction of the heart muscle. There is often a simultaneous increase in heart rate during the administration of these agents as well.
Inotropic agents are also used to increase renal perfusion and heart rate, increase venous return to the heart, and decrease pulmonary vascular resistance. They have a short half-life and must be infused continuously as drips. The major complications are tachyarrhythmias and tissue necrosis following extravasation.
The following are common inotropic agents utilized often in the neonatal and pediatric settings:
Dopamine – 2-20 μg/kg/min IV continuous infusion
Dobutamine – 2-20 μg/kg/min IV continuous infusion
Isoproterenol – 0.05-0.5 mg/kg/min IV continuous infusion
Prostaglandin is indicated to maintain patency of the ductus arteriosus to provide adequate systemic or pulmonary blood flow in infants with specific heart defects. It directly relaxes smooth muscles in arteriolar and venous walls and increases cardiac output if the decrease is secondary to myocardial dysfunction (Akkinapally et al., 2018).
Prior to initiation of therapy of prostaglandin, other causes of hypoxia should be excluded first. Prostaglandin may precipitate respiratory depression or systemic hypotension in neonates with respiratory distress syndrome (RDS), pulmonary disease, sepsis, or intracerebral hemorrhage.
Prostaglandin has a rapid onset of action. It produces vasodilation, smooth muscle relaxation of ductus arteriosus, and pulmonary and systematic circulations. There can be increased arterial saturation by 25 to up to 100%. It is important to monitor the patient’s blood pressure closely. Vasopressors may be required. Common side effects of prostaglandin can include:
Apnea
Flushing
Fever
Seizure-like activity
Decreased heart rate
Prostaglandin E1, or PGE1, is available for administration of 0.05-0.1 mg/kg/min IV as a continuous infusion.
During pregnancy, the patency of the ductus arteriosus is maintained by the production of prostaglandins. Therefore, prostaglandin synthetase inhibitors are indicated for the pharmacologic closure of a patent ductus arteriosus (PDA). They promote ductal closure by inhibition of prostaglandins in the wall of the ductus.
Failure of the ductus to close postnatally often complicates recovery from RDS in premature infants. Despite initial improvement in the RDS with a subsequent decrease in pulmonary vascular resistance, the infant's condition worsens due to a large left-to-right shunt through the ductus. This shunt often increases supplemental oxygen requirements, ventilator dependence, and CHF.
Indomethacin or ibuprofen are nonsteroidal anti-inflammatory drugs that inhibit prostaglandin production by blocking the action of cyclooxygenase on arachidonic acid (Philips & Gentle, 2024). In doing this thus accelerates ductal closure in a preterm infant (Philips & Gentle, 2024).
The following is a list of the prostaglandin synthetase inhibitors already mentioned with their respective doses and routes of administration:
Ibuprofen – 10 mg/kg given enterally or IV followed by two additional doses of 5 mg/kg given at 24-hour intervals
Indomethacin – Three doses of 0.2 mg/kg per dose given IV at 12-hour intervals
A repeat cesarean section delivered a 38-week gestation infant, Ava.
Ava had respiratory distress in the delivery room, requiring intubation.
Normal blood pressures in all four extremities were documented on admission to the NICU. Femoral pulses were normal. A pulse oximeter probe placed on her right upper limb was 95-98% with a 21-25% oxygen requirement.
Ava’s first chest X-ray demonstrated bilateral hazy lung fields. Within 24 hours, she was extubated, and a subsequent chest X-ray showed marked improvement. She was discharged home on room air with a 98-100% pulse oximeter reading in the right upper limb.
Two weeks following discharge, Ava was taken to her pediatrician's office for a routine visit, and she was noted to have absent femoral pulses. Ava was referred for a stat echocardiogram with a pediatric cardiologist.
Ava’s echocardiogram showed an interrupted aortic arch with an aberrant left subclavian artery arising from the PDA. The right common carotid artery, right subclavian, and left common carotid artery came off the proximal part of the aortic arch prior to the interruption. Ava was admitted and scheduled for surgery. She underwent corrective surgery the following day and was discharged home when she was four weeks old.
Given the fact that the pulmonary artery supplied the left upper extremity and the lower half of the body through the ductus, it is likely that SpO2 obtained from the left upper limb, or any lower limb would have demonstrated a lower SpO2 compared to the right hand. Therefore, unfortunately, a CCHD screen would likely have been negative because CCHD screening uses the right hand and not caught this congenital defect.
Meticulous attention to every aspect of care is essential to providing a positive outcome and quality of life for infants with congenital heart defects. The neonatal nurse and the pediatric nurse have a vital role in recognizing subtle signs and symptoms, providing preoperative management, and orchestrating postoperative management of the approximately 40,000 babies born annually diagnosed with congenital heart disease (CDC, 2024d). Screening for CCHD can help to identify many congenital heart cases early and can ultimately improve outcomes (CDC, 2022).
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Akkinapally, S., Hundalani, S. G., Kulkarni, M., Fernandes, C. J., Cabrera, A. G., Shivanna, B., & Pammi, M. (2018). Prostaglandin E1 for maintaining ductal patency in neonates with ductal-dependent cardiac lesions. The Cochrane Database of Systematic Reviews, 2(2), CD011417. Visit Source.
Altman, C.A. (2024). Identifying newborns with critical congenital heart disease. UpToDate. Retrieved February 13, 2024. Visit Source.
American Academy of Pediatrics. (AAP). (2023). Newborn screening for critical congenital heart defect (CCHD). American Academy of Pediatrics (AAP). Visit Source.
American Heart Association. (AHA). (2023). Fetal circulation. American Heart Association (AHA). Visit Source.
American Heart Association (AHA). (2022). Common types of heart defects. American Heart Association (AHA). Visit Source.
American Heart Association (AHA). (2018). Genetic basis for congenital heart disease: Revisited. American Heart Association (AHA). Visit Source.
Axelrod, D.M. & Roth, S.J. (2023). Pulmonary atresia with intact ventricular septum (PA/IVS). UpToDate. Retrieved February 13, 2024. Visit Source.
Beerman, L. (2023a). Tetralogy of fallot. Merck Manuals. Visit Source.
Beerman, L. (2023b). Coarctation of the aorta. Merck Manuals. Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024a). About coarctation of the aorta. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024b). About dextro-transposition of the great arteries (d-TGA). Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024c). About tricuspid atresia. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024d). Data and statistics. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2022). Screening for critical congenital defects. Centers for Disease Control and Prevention (CDC). Visit Source.
Cleveland Clinic. (2022a). Tetralogy of fallot. Cleveland Clinic. Visit Source.
Emfietzoglou, M. (2024). Heart sounds mnemonic. Osmosis from Elsevier. Visit Source.
Fernandes, C.J. (2024). Physiologic transition from intrauterine to extrauterine life. UpToDate. Retrieved February 13, 2024. Visit Source.
Fleishman, C.E. & Tugertimur, A. (2022). Clinical manifestations and diagnosis of atrioventricular (AV) canal defects. UpToDate. Retrieved February 13, 2024. Visit Source.
Geggel, R. L. (2021). Diagnosis and initial management of cyanotic heart disease in the newborn. UpToDate. Retrieved February 12, 2024. Visit Source.
Geggel, R. L. (2023). Approach to the infant or child with a cardiac murmur. UpToDate. Retrieved February 13, 2024. Visit Source.
Geggel, R. L. (2024). Cardiac causes of cyanosis in the newborn. UpToDate. Retrieved February 12, 2024. Visit Source.
Gonzalez, V. J., Kyle, W. B., & Allen, H. D. (2021). Cardiac examination and evaluation of murmurs. Pediatrics in Review, 42(7), 375–382. Visit Source.
Hampton, T., Alsaleem, M., & Murphy-Lavoie, H. M. (2022). Patent foramen ovale. In StatPearls. StatPearls Publishing. Visit Source.
Karmegaraj, B. (2022). Fetal snowman sign: Four-dimensional imaging of supracardiac total anomalous pulmonary venous connection. Ultrasound Obstetrics & Gynecology, 60(6):820-822. Visit Source.
Mayo Clinic. (2024). Coarctation of the aorta. Mayo Clinic. Visit Source.
Mayo Clinic. (2022). Patent foramen ovale. Mayo Clinic. Visit Source.
Mckee-Garret, T.M. (2023). Overview of the routine management of the healthy newborn. UpToDate. Retrieved February 12, 2024. Visit Source.
Pierpont, M. E., Brueckner, M., Chung, W. K., Garg, V., Lacro, R. V., McGuire, A. L., Mital, S., Priest, J. R., Pu, W. T., Roberts, A., Ware, S. M., Gelb, B. D., & Russell, M. W. (2018). Genetic basis for congenital heart disease: Revisited: A scientific statement from the American Heart Association. Circulation, 138(21), e653–e711. Visit Source.
Philips, J.B., & Gentle, S. (2024). Patent ductus arteriosus (PDA) in preterm infants: Management and outcome. UpToDate. Retrieved February 13, 2024. Visit Source.
Vrancken, S. L., van Heijst, A. F., & de Boode, W. P. (2018). Neonatal hemodynamics: From developmental physiology to comprehensive monitoring. Frontiers in Pediatrics, 6, 87. Visit Source.
Willim, H.A., Cristianto, & Supit, A. (2020). Critical congenital heart disease in newborn: Early detection, diagnosis, and management. Bioscientia Medicina: Journal of Biomedicine and Translational Research, 5(1), 107-116. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.