Get one year unlimited nursing CEUs $39Sign up now
This peer reviewed course is applicable for the following professions:
Advanced Practice Registered Nurse (APRN), Athletic Trainer (AT/AL), Certified Nurse Midwife, Certified Nurse Practitioner, Certified Nursing Assistant (CNA), Certified Registered Nurse Anesthetist (CRNA), Certified Registered Nurse Practitioner, Clinical Nurse Specialist (CNS), Home Health Aid (HHA), Licensed Nursing Assistant (LNA), Licensed Practical Nurse (LPN), Licensed Vocational Nurses (LVN), Medical Assistant (MA), Medical Doctor (MD), Midwife (MW), Nursing Student, Other, Registered Nurse (RN), Respiratory Therapist (RT)
This course will be updated or discontinued on or before Wednesday, September 1, 2027
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
**This course has been updated utilizing the 2025 New York State Mandated Reporter Training Syllabus. In regard to this content revision, please direct your attention to the newly added objective #2 and its’ coordinating new section “Indicators in Children with Intellectual & Developmental Disabilities” for the bulk of the curriculum update.
CEUFast, Inc. (BOC AP#: P10067) is approved by the Board of Certification, Inc. to provide education to Athletic Trainers (ATs).
Outcomes
≥ 92% of participants will know how to make an informed decision about whether a situation involves child abuse or maltreatment, what the reporting obligation is, and how to go about making such a report.
Objectives
After completing this continuing education course, the participant will be able to:
Determine if a child shows indicators of maltreatment or abuse, including in a virtual setting.
Recognize signs of intellectual and/or developmental disabilities in children and factors to consider when determining whether a child with intellectual and/or developmental disabilities shows indicators of maltreatment or abuse.
Recognize the impact of trauma and ACEs on children, families, and yourself.
Recognize the mitigating effects of the five protective factors on trauma.
Recognize the impact of bias on your decision-making.
Understand when you have a legal obligation to call the SCR.
Recognize how you may better connect individuals and families with services.
Know how to prepare to make the call to the SCR.
Know how to complete the LDSS 2221A form.
Understand your rights as a Mandated Reporter.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
This 2-hour course was developed and updated per the 2025 updates to the curriculum content for the Identification and Reporting of Child Abuse and Maltreatment/Neglect mandated workshop for the state of New York. An extensive list of additional content was required to be added after being signed into law amendments to Social Services Law § 413. This course includes all of the required content and curriculum as developed by the New York State Office of Children and Family Services (New York State [NYS], 2025).
Also, per New York, all professions are no longer required to complete both a pre-test and a post-test. These are now optional, and both included in this course, in order to demonstrate the transfer of knowledge and information about their duties and responsibilities as Mandated Reporters of child abuse and maltreatment.
This course is specifically and carefully created for New York professionals. This course will cover when you are legally required to contact the Statewide Central Register (SCR), when children and families may be more appropriately assisted through community-based services and other supports, how to reduce bias in the decision-making process of whether a call must be made to SCR, the impact of trauma as well as Adverse Childhood Experiences (ACEs) on children and families, and the protective factors and supports that you are able to refer families to in lieu of making a SCR report (NYS, 2025).
Studies have concluded that professionals who have contact with children often report only half of the incidents that may be abuse or maltreatment/neglect. The reason for this low report rate has historically been due to confusion or misunderstanding about the laws and procedures and a lack of knowledge or awareness of warning signs. This prompted the state of New York to require Mandated Reporter training several years ago.
In light of additional challenges within New York State in the past couple of years and a keen awareness of the impact of appropriate training and resources for its’ Mandated Reporters, the New York State social services laws have been amended. This training is meant to communicate these changes to further assist and equip each professional with the tools they need to identify and report suspected child abuse and maltreatment.
The SCR began in 1973 with the passing of the Child Protective Services Act. This law required the following:
Mandatory reporting of suspected child abuse or maltreatment by specific professionals. The list of those professionals can be found in the New York Social Services Law §413. This list changes as legislation is updated.
The creation of a 24-hour, 7-day-a-week central registry, known in New York as the SCR, to receive reports. The SCR is operated by the New York State Office for Children and Family Services (OCFS).
The creation of local Child Protective Services (CPS) to receive and investigate registered reports. In New York, local district CPS offices are staffed by human service professionals trained to investigate allegations of child abuse and maltreatment.
The laws that guide New York Child Protective Services today are Article 6, Title 6 of the Social Services Law (specifically Sections 411-428), and Article 10 of the Family Court Act (specifically Section 1012). To read the complete sections of these laws, visit here. Make sure to select: Laws > Laws of New York from the dropdown menu and then scroll down to “SOS” for Social Services Law or “FCT” for Family Court Law.
Social Services Law requires SCR as a single contact for reporting child abuse or maltreatment and CPS in each local department of social services (NYS, 2025). CPS requires strong partnerships within the community in order to help prevent child abuse and maltreatment (NYS, 2025). It is also vital to know that certain professionals have been designated as “Mandated Reporters” who must report child abuse or maltreatment under the law (NYS, 2025).
In 1999, the Monroe County Department of Social Services engaged the University of Rochester’s Department of Community and Preventive Medicine and the Perinatal Network of Rochester to conduct research for a campaign to increase community involvement to prevent child abuse and maltreatment and to improve reporting. Mandated Reporters were included as a group in this study.
As a result of these and other studies, we know that child abuse and maltreatment are underreported and that, conversely, some situations that are reported to the New York State Central Register (SCR) are more suitable for preventive services or other resources.
This training is designed to provide an understanding of the preventive-protective continuum of care within the Child Protective Services (CPS) system as it operates in New York State.
The OCFS, SCR, and local CPS agencies work together for a shared mission (NYS, 2025). They work together with Mandated Reporters to prioritize and promote the well-being of New York’s children, family, and communities (NYS, 2025). Mandated Reporters are so named because of their legal obligation to call the SCR. However, this only applies in certain situations. Families in crisis may, in fact, not meet the legal criteria required to call the SCR and may be better served by being connected to a range of community services in their area instead (NYS, 2025). Mandated Reporters have the opportunity to connect families to the following New York resources (NYS, 2025):
The OCFS H.E.A.R.S. stands for Help, Empower, Advocate, Reassure, and Support. This is a family line that assists families by providing necessary resources and referrals to a variety of services, including food, clothing, childcare, housing, and even parent education.
OCFS HEARS representatives are ready and available to help Monday through Friday from 8:30am to 4:30pm. If you know or come across a family that could use support, please ask them to call the OCFS HEARS family line at 888-554-3277.
In addition to the OCFS family line, the OCFS provides a list of the resources they have available as well as in-depth information regarding ACEs on their website here.
The NY Project Hope provides emotional support for New York State residents. Access to them includes the options of an Emotional Support Helpline (1-844-863-9314), online wellness support groups, and an extensive website filled with supportive resources. Their website is available here.
This office has a website that provides numerous resources for people who may be experiencing currently or who are survivors of domestic violence. This website is available here.
This organization has a prevention and parent helpline that is available for parents and caregivers that is confidential. It is available for multiple languages. It can refer or connect caregivers to community-based services.
This helpline is available Monday through Friday from 9:00am to 4:00pm. The contact number is 1-800-CHILDREN.
Parents and caregivers are also able to call 2-1-1, which is operated by the United Way, for information regarding health and human services, referrals, assessments, and crisis support to help them find the assistance they require to address the everyday challenges of living, as well as those that develop during times of disaster or other community emergencies.
2-1-1 is multi-lingual and open and accessible 24 hours a day, 7 days a week.
Per New York, for more information on what other services are available for children and parents in your community, feel free to visit here.
Youth violence is a central public health issue. The World Health Organization (WHO) estimates that nearly 176,000 people between the ages of 15 and 29 are killed every year, making it the third leading cause of death for individuals in this age group (World Health Organization [WHO], 2023). Sexual violence is also shown to affect a significant proportion of youth as well, as evidenced by about 1 in 8 young people who report being sexually abused (WHO, 2023).
It is estimated that approximately 1 in 7 children suffer from abuse or neglect every year (Centers for Disease Control and Prevention [CDC], 2022a). Even then, this is likely an underestimate because numerous cases go unreported (CDC, 2024a). In 2021 alone, more than 1,820 children died due to abuse and neglect just in the United States (CDC, 2024a). According to the U.S. Department of Health and Human Services’ National Child Abuse and Neglect Data System (NCANDS) report, there were more than 56,000 victims of child maltreatment in the state of New York just in the year 2021 (National Child Abuse and Neglect Data System [NCANDS], 2021).
There is a large gap between the true prevalence of child abuse and the number of cases that are brought forward to CPS (Baker et al., 2021). Each and every year, CPS investigates over 3 million children and their families nationally (Rizvi et al., 2023). Of this number of families, 20% produce evidence of maltreatment that is substantiated (Rizvi et al., 2023). In New York alone, there are over 150,000 referrals that are made concerning possible abuse and neglect every year (Gonzalez et al., 2023). Nearly half of these children are confirmed victims (Gonzalez et al., 2023). While males and females seem to be equally affected, the highest risk of abuse and neglect are in children who are less than 3 years of age and those who are African American and Native American (Brown et al., 2023). Of the number of abused children, 78% suffer neglect, 18% suffer physical abuse, and 9% endure sexual abuse (Brown & Yilanli, 2025).
The majority of reports of child abuse are made by Mandated Reporters. This is due to their professional experience and Mandated Reporter training (Baker et al., 2021).
Trauma is defined as an intense event that threatens a person’s life or safety in a way that is too much for the mind to handle and leaves the person powerless (NYS, 2025).
Trauma can bring about physical reactions including (NYS, 2025):
Rapid heart rate
Tense muscles
Shallow breathing
Common traumatic events could be going through or witnessing (NYS, 2025):
Family violence
Sexual abuse
Emotional abuse
Violence in the community
For many parents, having a child removed from the home and dealing with the child welfare system are traumatic events (NYS, 2025).
Adverse Childhood Experiences, or ACEs, are negative experiences or events that are potentially traumatic. These events are those that occur from birth through about 17 years of age (CDC, 2024b).
ACEs can include all the following situations as listed in the following image:
Image #1: Adverse Childhood Experiences (ACEs)
This list, however, is not fully inclusive. Additional examples of ACEs include (CDC, 2024b; Integrative Life Center, 2021):
Experiencing violence or neglect
Experiencing physical, sexual, or emotional abuse
Witnessing violence occurring in the community
Having a family member attempt or die by suicide
Having a family member who has a mental health problem
Experiencing divorce/custody battles
Child maltreatment and abuse are adverse childhood experiences (NYS, 2025).
These ACEs have been shown to impact a person’s functioning, physical and mental health, and overall well-being throughout their lives (CDC, 2024b). These effects can be seen well into adulthood. In fact, the very first ACE study was conducted by the CDC and Kaiser Permanente from 1995 to 1997 (National Conference of State Legislatures [NCSL], 2022). Of the more than 17,000 adults surveyed about childhood experiences (including emotional, physical, and sexual abuse, neglect, and household dysfunctions of separation from a parent, substance use disorder, incarceration, violence, and/or mental illness), approximately two-thirds of respondents indicated a history of at least one ACE and more than 20% noted three or more (NCSL, 2022).
Research has shown that ACEs are very common in all socioeconomic groups. It has been estimated that about 61-67% of the U.S. population has experienced at least one ACE (NYS, 2025). Children who have experienced numerous adverse experiences have higher rates of negative health outcomes including (NYS, 2025):
Depression
Obesity
Substance use
Anxiety
Heart disease
Early death
Other factors can intensify the effects of ACEs. These factors can include (NYS, 2025):
As mentioned above, exposure to ACEs has been correlated with increased risk for certain behavioral issues and health conditions. Additional research has determined that ACE exposure increases a child's risk of obesity, autoimmune diseases, depression, and substance use disorders (NCSL, 2022).
A direct correlation has been noted:
The more ACEs one is exposed to, the greater the risk for negative effects.
But why? The underlying mechanism here is associated with the "toxic stress" that ACEs are said to exert their effects on health as well as growth and development (NCSL, 2022). Although some stress is normal and even essential to proper growth and learning, sustained chronic, toxic stress is damaging to both the body and the brain (NCSL, 2022). Toxic stress occurs when a person experiences severe, prolonged adversity without adequate support. Toxic stress means that the stress response stays continuously activated in the body (NYS, 2025). This toxic stress can literally build up in the body, interfere with proper neural, hormonal, and immune development, and ultimately alter DNA expression (NCSL, 2022). This change in DNA expression can result in lifelong effects on behavior, attention, decision-making abilities, and one's response to stress (NCSL, 2022). Toxic stress impacts children developmentally and behaviorally (NYS, 2025).
ACEs can have a lasting impact on children, as we have seen, but also on PLR and Mandated Reporters.
Because ACEs can have lifelong negative implications on the health and overall well-being of a child or adolescent, it is important that we do what we can to prevent them and/or mitigate them once they have occurred.
The following strategies for prevention and mitigation have been presented by the National Conference of State Legislatures (2018) report after reviewing an extensive number of publications in the research done following the original ACE study (Bellazaire, 2018):
Achieving strong physical health: Obtaining adequate sleep, eating well, and participating in regular exercise.
Building resilience: Increasing positive parenting skills and creating safe, stable relationships in the home.
Incorporation of home visits: State-employed nurses, social workers, and teachers trained to visit family homes during pregnancy and early childhood to teach and provide support services.
Offering early childcare services: Expanding access to early childhood programs to bolster learning, social and emotional development, and the building of self-confidence.
Supporting the reduction of parental stress: Consider providing economic support, family-friendly workplaces, paid family and/or sick leave, and affordable housing.
Increasing mental health screening and treatment: Expand access to and coverage for comprehensive health and mental health services.
The CDC outlines these additional strategies for preventing ACEs altogether (CDC, 2024b):
Promoting social norms: Advertising public education campaigns, legislative approaches, and bystander approaches to teach and inform in a manner that helps to protect against violence and adversity.
Teaching vital skills: Prioritizing social-emotional learning, safe dating, healthy relationship building, family relationships, mentoring programs, and after-school programs.
Intervening early and often: Engaging children in primary care, family therapy when needed, individual therapy when needed, and family-centered treatment for households with someone suffering from a substance use disorder.
It is important to continue raising awareness of ACEs to help prevent them or work to prevent the long-term sequelae that result without adequate intervention (CDC, 2024b). The focus needs to be taken off the individual and, more so, shifted onto the community to help lessen the risk of ACEs and their effects. The more children and adolescents are able to reach their full potential, the more the communities these future adults will live in will benefit (CDC, 2024b).
Trauma-informed practice, or trauma-informed care (TIC) is a model for engaging with individuals and families that recognizes the impact and influence that trauma may have on the individuals and families you serve (NYS, 2025). The goals of a trauma-informed practice are to avoid the inadvertent re-traumatization of individuals through your own interactions with them and to understand that trauma may have an impact on a person’s behavior (NYS, 2025).
Trauma-informed practice will assist you in identifying when your own past experiences or trauma may impact the way you evaluate an incident you encounter in your professional role (NYS, 2025).
This patient-centered approach focuses on the basic understanding that the trauma the patient has endured greatly impacts their life from now on (Tracy & Macias-Konstantopoulos, 2023). This approach aims to avoid any possible reinjury, focus on survivor strengths and overarching resilience, empower healing and recovery, and promote the creation of survivorship skills (Tracy & Macias-Konstantopoulos, 2023).
Trauma-informed practice can be applied to all patients as it simply involves the healthcare personnel's practice modification to be critically aware of the general traumatic events this specific patient has lived through (Tracy & Macias-Konstantopoulos, 2023; Gaillard-Kenney et al., 2020).
The CDC’s Office of Readiness and Response (ORR), in collaboration with SAMHSA’s National Center for Trauma-Informed Care (NCTIC), developed trauma-informed practice training that included six main principles (CDC, 2020). These principles include (CDC, 2020):
Safety
Peer support
Trustworthiness & transparency
Collaboration & mutuality
Cultural, historical, & gender issues
Empowerment & choice
Based on these principles, to be trauma-informed means asking the patient permission before completing an examination, allowing them to remain clothed per their comfort level, assessing them in a place that is comfortable to them, and informing them of the steps in what you are doing so they can know what to expect each step of the way (Tracy & Macias-Konstantopoulos, 2023). The patient should also be asked what their expectations are for your time with them and how you can help them feel as comfortable as possible throughout the proceedings, which could often mean leaving the door open slightly ajar (Tracy & Macias-Konstantopoulos, 2023). It is also helpful for these patients to identify a "safe word" or a "signal" that patients can utilize if they begin to feel unsafe or distressed during the visit (Tracy & Macias-Konstantopoulos, 2023).
Engaging in trauma-informed practice is not accomplished by using a singular checklist (CDC, 2020). Instead, it requires continual attention, compassionate awareness, sensitivity, and often some level of cultural change within the organization (CDC, 2020).
Employing trauma-informed practice for these patients is extremely important. It helps the patient trust the healthcare personnel and best opens the lines for communication (Tracy & Macias-Konstantopoulos, 2021; Gaillard-Kenney et al., 2020).
Protective factors are conditions that, when present in families and communities, can help increase the health and well-being of children and families, serving as buffers to prevent worse outcomes from actualizing (Positive Childhood Alliance, 2024). Protective factors offer support, resources, and coping strategies, allowing families to care for their children and “parent” effectively, even under stressful circumstances (Positive Childhood Alliance, 2024). In fact, research has shown that protective factors can contribute to a lower incidence of child abuse and neglect (Positive Childhood Alliance, 2024).
The following are the five protective factors (Positive Childhood Alliance, 2024):
1. Parental resilience
Resilience is an inner strength and adaptability that allows one to “bounce back” when things are not going well. Resilient parents are able to cope with the stresses of everyday life as well as situational crises as they pop up.
2. Social connections
Social connection features a social network of emotionally supportive family, friends, and neighbors who can assist parents with the care of a child. Parents who have reliable people they can count on to share advice, simply listen, or provide concrete support are parents who find it easier to care for their children and themselves.
3. Parental knowledge of child development and parenting skills
Extensive research has been done taking a look at parenting skills and their effect on children. Effective parenting is strongly associated with leading to healthy child development. Children require affection, but they also require respectful communication, listening, safe opportunities to promote independence, and consistent rules and expectations.
4. Social and emotional competence of children
We also know that research has shown that babies who receive enough affection and nurturing from their parents have the best chances of healthy development. Young children who have a positive relationship with a caring, consistent adult have better grades, an increased ability to cope with stress, more positive interactions with peers, and overall healthier behavior and physical growth and development.
5. Concrete support for parents
Parents with the tools to provide basic food, clothing, housing, and transportation for their children are better equipped to provide childcare, healthcare, and mental health services. Families who have the needed tools and support are better able to ensure their children's safety and overall well-being. Sharing with parents the resources that are available in their community can be highly beneficial, especially for those who are struggling, to work to prevent child maltreatment or even neglect.
Trauma impacts much of the work Mandated Reporters do. Trauma may impact the child or family that you are working with. Your own past experiences and trauma may ultimately impact your decision-making. ACEs and trauma alone may not rise to the level of child abuse or maltreatment. It is the impact on the child that should be assessed and then used to inform us on the trauma-informed care we provide. It is important that we work to reduce the effects of ACEs on children while supporting them and their families and increasing protective factors (NYS, 2025).
Additional resources provided directly by New York State include (NYS, 2025):
As human beings, we all have our own biases (NYS, 2025). Whether implicit or explicit, these biases affect our beliefs, decisions, and actions. A bias is a personal and sometimes unreasoned judgement against a person, place, or thing. Biases, including how a person sounds, looks, and even where they live, may influence our decision-making process (NYS, 2025).
An implicit bias is a bias or prejudice that is present but not consciously held or recognized, so we are often unaware of them (NYS, 2025).
An explicit bias is a personal and unreasoned judgment that we have about a person, place, or thing on a conscious level or one that we are aware of (NYS, 2025).
Both implicit and explicit bias can show up as prejudice, discrimination, and/or oppression on individual, group, or systemic levels (NYS, 2025). Individual biases are often deeply ingrained and are born out of a long history rife with unequal treatment of different social groups, individual’s upbringing, discrimination and oppression, cultural conditioning, and stereotypical portrayals of social groups (NYS, 2025). The impact of decisions made that are rooted in biases often have significant impacts on individuals, social groups, and communities (NYS, 2025).
One of the benefits of being aware of the potential impact of your own biases is that you can choose to take a proactive role in reducing how they impact your decision-making (NYS, 2025).
National research shows, and OCFS data confirms, that disparities exist throughout the child welfare system presently and historically (NYS, 2025).
OCFS’ Disproportionate Minority Representation (DMR) data shows historical overrepresentation of children and families of color in the child welfare system (NYS, 2025). Families of color have been more likely to be involved in a report to the SCR (NYS, 2025). Children of color have been more likely to be placed in foster care and generally experience slower achievement of permanency goals (NYS, 2025).
Research shows that income status of families is a significant predictor of involvement with the child welfare system (NYS, 2025). Poverty in and of itself does not equate to child abuse or maltreatment (NYS, 2025).
Research also shows that families that have been investigated by CPS often have several poverty-related risk factors such as (NYS, 2025):
Single parenthood
Housing instability
Food insecurity
Unemployment
Lack of access to childcare
Families living below the poverty line are three times more likely to be substantiated for child maltreatment (NYS, 2025). This disparity has devastating and long-lasting impacts on both families and communities (NYS, 2025).
A Mandated Reporter’s decision whether to call the SCR can change the entire course of the life of a child and the members of a family. It is important to be aware of the tendency for implicit and explicit bias and to be intentional about making decisions based on the objective facts of a situation (NYS, 2025). Part of this process is to increase our own awareness regarding our own beliefs, including those that may be hidden or unconscious. As a professional, you must ensure that your own implicit and explicit biases do not impact your decision to call the SCR (NYS, 2025).
As an example, consider if personal characteristics such as race, ethnicity, sex assigned at birth, gender identity or expression, sexual orientation, religion, or primary spoken language would impact your decision to report. These things are important to think about and reflect on prior to making the call. You should only call the SCR as a Mandated Reporter when you have a legal obligation to do so (NYS, 2025).
Not all cases require a call. You have the ability to support a family without having to report them. It is important to keep in mind that we must approach our responsibility as Mandated Reporters with curiosity, empathy, care, and compassion (NYS, 2025). When assessing the information received about a child and their family, instead of making assumptions or jumping to immediate conclusions that a child is being maltreated or abused, we must ask ourselves the right questions (NYS, 2025): Can this family’s needs be met by providing services or other resources outside of CPS involvement?
The first step in identifying implicit bias is identifying our own lens that we see the world through. Bias can show up in many ways. Bias might look like subconscious thoughts (implicit bias), conscious thoughts (explicit bias), inaccurate judgments, or even stereotypes (NYS, 2025). However, bias can also be unlearned (NYS, 2025).
One proven strategy to reduce personal bias is to think about whether the facts of the situation would lead you to the same decision to call the SCR if the demographic information for the child or family were different (NYS, 2025). Would your decision to call the SCR regarding an individual or family with a report of suspected child maltreatment or abuse change if the following were different?(NYS, 2025):
Their race?
Their gender?
Their ethnicity?
Their gender identity or expression?
Their religion?
Their culture?
Their age?
Their sexual orientation?
Their sex assigned at birth?
Their sexual expression?
Their primary spoken language?
Their immigration status?
The neighborhood where they reside?
Their occupation?
Their socioeconomic status?
Their level of education?
Their disability?
If you answered “yes” to any of the individual bullet points, then bias may be impacting your decision to call the SCR (NYS, 2025).
Other than asking ourselves that question, the best tool we have to reduce our own bias is our ability to think critically (NYS, 2025). As Mandated Reporters, you must utilize critical thinking when deciding whether to call in a report to SCR. Critical thinking includes gathering adequate information about the current situation, analyzing that information you collect and separating facts from assumptions, determining whether you are legally required to call the SCR, and if not, determining what alternative options you have available to you (NYS, 2025). The following list are the things that must be considered prior to filing a report (NYS, 2025):
What are my specific concerns about this family’s situation?
Do I have adequate information about the current situation?
If I do not think I yet have adequate information, can I gather all I need?
What are the facts of this situation versus the assumptions that I might be making?
What is the possibility that I have some bias regarding this case?
What could be multiple explanations/hypotheses that could explain this situation rationally?
Am I legally required to call the SCR?
If I am not legally required to call the SCR, is there an alternative option, such as connecting the individual or family to appropriate services in their community?
It is important to approach each situation with humility, be open and willing to learn, recognize that we do not know everything about the situation and the family, and consider that the whole story might be different from our first impressions and assumptions that we make (NYS, 2025).
Think about situations you encounter from a different viewpoint. For example, in some cultures, beans and rice are dietary staples. One’s personal belief may not include entire meals from such a food group as nutritionally sound. Not applying one’s beliefs, values, or experiences but instead acting on the facts and from professional experience is a better measure of how to respond to suspicious incidents.
The NYS (2025) also shares another great resource for identifying our own biases. Harvard University developed the Implicit Association Test (IAT), which measures attitudes and beliefs that you may be unwilling or unable to identify and report. There are a variety of IAT tests available here(NYS, 2025).
Required Mandated Reporters may change over time as legislature is passed (NYS OCFS, n.d.-a). The most recent list of those who are Mandated Reporters can be found in the Social Services Law § 413.
The following professional persons or officials are Mandated Reporters in the state of New York in accordance with Social Services Law § 413 as of April 2024 (NYS OCFS, 2024):
Physician
Registered physician’s assistant
Surgeon
Medical examiner
Coroner
Dentist
Dental hygienist
Osteopath
Optometrist
Chiropractor
Podiatrist
Resident
Intern
Psychologist
Registered nurse
Social worker
Emergency medical technician
Licensed creative arts therapist
Licensed marriage and family therapist
Licensed mental health counselor
Licensed psychoanalyst
Certified behavioral analyst assistants
Hospital personnel engaged in the admission, examination, care, or treatment of patients
Christian Science practitioner
School officials, including (but not limited to):
School teacher
School guidance counselor
School psychologist
School social worker
School nurse
School administrator or other school personnel required to hold a teaching or administrative license or certificate
Full or part-time compensated school employee required to hold a temporary license or professional coaching certificate
Social services worker
Director of a children's overnight camp, summer day camp, or traveling camp
Employee of a publicly funded emergency shelter for families with children
Daycare center worker
School-age childcare worker
Provider of family or group family daycare
Employee or volunteer in a residential care facility for children
Any other childcare or foster care worker
Licensed behavior analysts
Mental health professional
Substance abuse counselor
Alcoholism counselor
All persons credentialed by the NYS Office of Alcoholism and Substance Abuse Services
Peace officer
Police officer
District attorney
Assistant district attorney
Investigator employed in the office of the district attorney
Any other law enforcement official
Employees of a home health or home healthcare management agency who have regular and substantial contact with children
Employees who provide home and community-based services under a Social Security Act § 1115 demonstration project, who have regular and substantial contact with children
Athletic trainer (effective 12/2025)
Whenever such a person is required to report as a member of the staff of a medical or other public or private institution, school, facility, or agency, he or she shall make the report as required by their title. No retaliatory personnel action is allowed.
Mandated Reporters are required by law to call the SCR when in their professional role, they develop a reasonable cause to suspect a child under the age of 18 is being maltreated or abused by a parent or person over the age of 18 who is legally responsible for the care of the child at the relevant time (NYS, 2025).
If the Mandated Reporter calls the local county Department of Social Services office or a law enforcement official, then that Mandated Reporter HAS NOT fulfilled their legal duty to report to the SCR.
A “reasonable cause to suspect” occurs when what you have observed or been told, combined with your professional experience or training, leads you to reasonably believe that a child has been or is being maltreated or abused (NYS, 2025). A reasonable suspicion does NOT require proof a child has been maltreated or abused (NYS, 2025). One indicator or several indicators in combination may give you a reasonable suspicion (NYS, 2025). Poverty, by itself, does not equate to maltreatment or abuse (NYS, 2025).
The term and acronym “PLR” includes the child’s custodian, guardian, and any person responsible for the child’s care at the relevant time (NYS, 2025).
The term “custodian” may include any person continually, or at regular intervals, found in the same household as the child when the conduct of such person causes or contributes to the abuse or maltreatment of the child (NYS, 2025).
As mentioned, Mandated Reporters have a legal obligation to file a report, but there is also a framework for protection and guidance to support them.
There are three components to the legal framework applicable to Mandated Reporters:
Confidentiality.
Immunity from Liability.
Penalties for Failure to Report.
No medical or other public or private institution, school, facility, or agency shall take any retaliatory personnel action against an employee who made a report to the SCR. No school, school official, childcare provider, foster care provider, residential care facility provider, hospital, medical institution provider, or mental health facility provider shall impose any conditions, including prior approval or prior notification, upon a member of their staff mandated to report suspected child abuse or maltreatment.
According to Social Services Law § 422 (4)(A), state law provides confidentiality for Mandated Reporters and all sources of child abuse and maltreatment reports (NYS, 2025). However, CPS or the SCR may be required to provide the identity of the source of the CPS report in very limited circumstances and only as described in the law (NYS, 2025).
For more information on when the identity of a source of a report to the SCR may be disclosed, please visit here(NYS, 2025).
The Health Insurance Portability and Accountability Act (commonly referred to as “HIPAA”) contains specific provisions allowing healthcare and other professionals to report information to the SCR, including personally protected health information that is otherwise confidential (NYS, 2025). Your legal obligation to report suspected child abuse and maltreatment under New York State law supersedes client-patient confidentiality provisions (NYS, 2025).
New York law gives all Mandated Reporters immunity from civil and criminal liability whenever a Mandated Reporter makes a report because they had a reasonable cause to suspect child abuse or maltreatment (NYS, 2025). The law assumes Mandated Reporters make such reports in “good faith” and, therefore, Mandated Reporters are protected, even if CPS finds no evidence of abuse or maltreatment (NYS, 2025).
A Mandated Reporter who fails to call the SCR when they have a reasonable suspicion of child abuse or maltreatment while in their professional role may be subjected to criminal and civil liability (NYS, 2025). The Mandated Reporter may also be held civilly liable for any harm suffered by a child due to their failure to call the SCR (NYS, 2025).
It is important to know that no employer or organization is permitted to require that you seek or obtain approval prior to calling the SCR (NYS, 2025). Your legal obligations as a Mandated Reporter are personal to you, and your organization may not impede you from calling the SCR (NYS, 2025). All employers and organizations are also prohibited from retaliating against you in any way for fulfilling your duties as a Mandated Reporter (NYS, 2025). The law does not require multiple reports on the same incident from the same organization (NYS, 2025).
Some Mandated Reporters face a conflict between their legal obligation to report and their legal obligation to maintain client or patient confidentiality. As we have been discussing, it is Social Services Law § 419 that provides immunity from liability for Mandated Reporters. The good faith of such a person, official, or institution required to report is presumed. This means if a person accuses you of making a false report in bad faith, they have to PROVE you acted with gross negligence or willful misconduct.
According to Social Services Law § 420, Mandated Reporters are subject to serious consequences for failure to report. A Mandated Reporter who fails to report can be found guilty of a Class A misdemeanor. A Class A misdemeanor can result in a penalty of up to a year in jail, a fine of up to $1,000.00, or both.
Additionally, failing to report may result in a lawsuit in civil court for monetary damages for any harm caused by the Mandated Reporter’s failure to make the report to the SCR, including wrongful death suits.
Professional capacity is defined as any time that a person is acting within the scope of their employment or carrying out functions as part of the duties and responsibilities of their profession.
Examples of “on duty” or “on the clock” versus “off duty”:
A doctor examining a child in her practice who has a reasonable suspicion of abuse must report her concern.
In contrast, the doctor who witnesses child abuse when riding her bike while off-duty is not mandated to report that abuse.
The Mandated Reporter's legal responsibility to report suspected child abuse or maltreatment ceases when the Mandated Reporter stops practicing his/her profession. Of course, anyone may still report any suspected abuse or maltreatment at any time and is encouraged to do so; they are just not legally obligated.
Let’s review the standards of the state of New York for the minimum degree of care that must be provided to a child.
Parents and PLRs in New York State must provide their children with the minimum degree of care (NYS, 2025). This requires adequate food, clothing, shelter, education, medical care, and supervision(NYS, 2025).
As mentioned above, a minimum degree of care must be provided to a child. In addition to adequate food, clothing, and shelter, every child is afforded an adequate education.
Parents are to ensure that the children in their care are actively enrolled in school (NYS, 2025). To be actively enrolled in school does not mean a child has to be earning high grades, participating in extracurricular activities, or have perfect attendance (NYS, 2025). The minimum degree of care regarding adequate education is measured by looking at the conduct of the parent after considering any efforts previously made by the school and/or CPS (NYS, 2025). We will get more into the definition of educational neglect in a future section.
Each child is also afforded the right to adequate medical care. This includes basic dental care, mental health services, and treatment for drug or alcohol misuse (NYS, 2025).
All children must be adequately supervised. There is no provision in New York State law or regulation that dictates how old a child must be to be left alone without adult supervision (NYS, 2025). Determining whether a child can be safely left alone must be made on a case-by-case basis, depending on many things (NYS, 2025). A child left alone in a residence or in the community must be able to demonstrate that they have the knowledge and skills necessary to properly respond to a potential emergency and to care for themselves (NYS, 2025). Also, it is important to remember that just because an individual child may be left safely alone does not mean that that child has the necessary skills to also supervise other children without an adult present (NYS, 2025).
In addition to the above components of the minimum level of care, no excessive corporal punishment is allowed to be used on children (NYS, 2025).
New York State law permits parents to utilize corporal (physical) punishment in order to discipline their children, but it is not allowed to be excessive (NYS, 2025). Excessive corporal punishment includes when (NYS, 2025):
A less severe method is available and likely to be effective
The length of punishment surpasses the child’s endurance
The punishment is inflicted due to the parent’s rage
The child receives injuries or bruises as a result
The child lacks the capacity to understand the corrective quality of the discipline
An example may help to clarify this point:
A parent slaps their twelve-year-old son once for being disrespectful. The child did not sustain any bruises. This type of discipline would not generally be considered “excessive.”
A parent slaps their twelve-year-old son for being disrespectful. As a result of this level of physical discipline, the child sustained a bruise and a slight laceration on the right side of his cheek. This type of discipline would be considered “excessive” and necessitate filing a registered report.
The “minimum degree of care” regarding adequate food, clothing, shelter, and medical care must be considered regarding whether or not the parent or PLR was financially able to provide these things or was offered other financial or reasonable means to do so (NYS, 2025).
When identifying suspected child abuse and maltreatment, begin by considering the child. Carefully review what has happened to the child that leads you to believe there is harm or risk of harm to the child.
Consider how the parent or other persons legally responsible may be culpable for this condition or circumstance.
Always start with the child and establish his or her condition, and then explore the involvement of the parent or person legally responsible for the child's care.
There are definitions you must understand that establish parameters for reporting abuse and maltreatment. Generally, maltreatment involves the quality of care a child receives. Abuse reflects the seriousness of the injury. There needs to be a connection between harm to the child or a substantial likelihood of harm and the actions or inactions of the person responsible for the child.
Deciding if a report is classified as abuse or maltreatment is the job of the SCR when the report is made or by local CPS during the investigation.
The following definitions should be used as guidelines to determine if there is reasonable cause to suspect abuse or maltreatment.
Under New York State law, a child is maltreated when (NYS, 2025):
A parent or other PLR for the child fails to provide the minimum degree of care and that failure results in impairment or imminent danger of impairment to the child’s physical, mental, or emotional condition
OR
A parent or other PLR for the child cause a non-accidental, serious physical injury to the child
It is important to note that actual impairment or harm is not required (NYS, 2025). Also, it is important to know that poverty, in and of itself, is not considered maltreatment (NYS, 2025).
Under New York State law, a child is abused when (NYS, 2025):
A parent or PLR for a child inflicts (or allows someone else to inflict) a non-accidental serious injury which causes either a serious or protracted disfigurement, a protracted loss or impairment of the function of any bodily organ, or a substantial risk of death
OR
A parent or PLR for a child creates (or allows to be created) a substantial risk of non-accidental physical injury, which would be likely to either result in a serious or protracted disfigurement, a protracted loss or impairment of the function of any bodily organ, or lead to death
OR
A parent or PLR commits (or allows someone else to commit) a sex crime against a child
Imminent danger is a term that measures the distance between a child and the harm created by a parent’s or PLR’s actions or failure to act.
Imminent danger means that the child is placed at immediate risk or substantial risk of harm.
The key factor in assessing imminent danger is to ask yourself, “How direct is the threat to the child?” In other words, the danger to the child must be immediate or nearly immediate.
The standard to be applied is reasonableness. Ask yourself, “Is it reasonable to believe an intervening factor could occur?” If the answer is yes, then there is no imminent danger. If the answer is no, then there is reasonableness to assume that harm could occur and there is imminent danger.
Let’s consider an example that may help to clarify this point:
If a parent swings an object at a child attempting to strike the child on the head but misses, we can say that the danger was imminent. The only additional factor necessary for the child to be injured was for the parent to connect rather than miss; it is reasonable to believe this could have occurred.
Risk factors for child abuse are the specific characteristics that can increase the chances of child maltreatment. For example, children younger than four years of age and those with special needs are risk factors that increase a child’s chance of being maltreated or abused (CDC, 2024b).
The following are the caregiver-related risk factors for child maltreatment and abuse (CDC, 2024c):
Use of drugs or alcohol excessively
History of mental health conditions
Previous exposure to abuse or neglect as children themselves
Low socioeconomic status (lower income, lower levels of education)
High levels of stress
Not the biological child’s parent
Caring for children with special needs that they do not understand
Self or family members in jail/prison
Violence within the family
High level of conflict within the household
Isolated from extended family, friends, and/or neighbors
Some community-related risk factors can increase the likelihood of child maltreatment and abuse. These environmental risk factors can include areas of high rates of violence and crime, limited educational and economic opportunities, high rates of unemployment, simple access to alcohol and drugs, unstable housing, quick neighbor resident turnover, and those with frequent concerns around food security (CDC, 2024b).
Protective factors are the specific characteristics that have the possibility of lowering the chances of children being neglected or abused (CDC, 2024c).
Caregivers who nurture positive relationships with children, utilize parenting skills, provide emotional support, have a college degree or higher with steady employment, and are capable of meeting a child’s basic needs of food, security, shelter, healthcare, and education are known to be those who are less likely to harm the children in their care (CDC, 2024c). Families who are active and present, enforce rules in the home, monitor their children for their safety, and have a supportive environment of friends and family who can offer guidance and assistance in caring for the children are also less at risk for engaging in child abuse and maltreatment (CDC, 2024c).
Just as communities can have a negative impact on the chances of child abuse and maltreatment, they can also have a protective effect (CDC, 2024c). The following includes the factors of communities that help to decrease the likelihood of child abuse and maltreatment (CDC, 2024c):
Access to safe housing
Access to high-quality schooling and childcare
Engaging after-school activities are available
Access to good medical care
Access to mental health services
Economic/financial help resources
Workplaces that prioritize families and their needs
Indicators of abuse warn the Mandated Reporter to pay more attention to a particular situation. Sometimes, there are no visible indicators present even though the child is being abused.
There are three types of indicators of abuse or maltreatment and abuse (SUNY, 2013):
Physical indicators
Behavioral indicators
Parent or PLR behavioral indicators
Indicators should not be viewed in isolation. They must be considered in relation to the child’s condition. Indicators should be considered in the overall context of the child’s physical appearance and behavior. Sometimes, a single indicator is self-evident or points to abuse or maltreatment/neglect. Often, several indicators must be pulled together, or clusters of indicators must be used to develop reasonable cause (SUNY, 2013).
Some Mandated Reporters see a child only once or very infrequently, whereas others see them more often. In looking for reasonable cause, you need to consider what you know about the child’s normal behavior. No two children will respond the same way to the same situation.
Now, let’s review the physical indicators of child maltreatment and abuse.
What does child maltreatment and abuse physically look like?
Physical indicators include (NYS, 2025):
Unexplained bruises:
Bruising of the torso, buttocks, and thighs
Bruising in various stages of healing
Clustered bruises forming regular patterns that might reflect the shape of the article used to inflict the injury
Bruising on several different parts of the body
Bruises regularly appear after absence, weekend, or vacation
Suspicious bruising that does not match the story that was told as to how it was obtained
Unexplained fractures:
To the nose, skull, or facial structure
In various stages of healing
Multiple or spiral fractures
Unexplained burns:
Cigar, and cigarette burns, especially on the soles of the feet, palms, back, and buttocks
Immersion burns that are often appearing sock-like, glove-like, or even doughnut-shaped on the buttocks or genitalia
Pattern-like burn in the shape of an electric burner or an iron
Rope burns on the arms, legs, neck, or torso
Unexplained welts
Unexplained lacerations:
To the mouth, lips, gums, or eyes
To external genitalia
On the back of the arms, legs, or torso
Human bite marks
Unattended physical problems, medical, or dental needs
Pain or itching in the genital area
Difficulty in walking or sitting
Pregnancy, especially in the early adolescent years
Sexually transmitted disease (especially in pre-adolescent children)
Lags in physical development or growth
Frequent injuries that are accidental or unexplained
Image #2: Handprint Injury on Child’s Face
Source: "AbuseWatch.net, n.d."
Image #3: Bruising of Torso, Buttocks, and Thighs
Source: "AbuseWatch.net, n.d."
Image #4: Spiral Fracture of the Humerus
Source: "AbuseWatch.net, n.d."
Image #5: Cigarette Burn to Finger
Source: "AbuseWatch.net, n.d."
Image #6: Glove-Like Burn of the Hands
Source: "AbuseWatch.net, n.d."
Image #7: Sock-Like Burn of the Feet
Source: "AbuseWatch.net, n.d."
Image #8: Steam Iron Burn to the Arm
Source: "AbuseWatch.net, n.d."
Image #9: Looped Cord Injury
Source: "AbuseWatch.net, n.d."
As mentioned above, injury or bruising that is most suspicious for child maltreatment or abuse is that in which (NYS, 2025):
The location of the injury may be atypical
The explanation provided regarding the injury does not match the pattern of injury
The bruise or laceration is shaped like a specific object (like a handprint, looped cord, or belt)
Let’s take a look at sites of bruising that would be considered normal for children and those that are more suspicious of possible child abuse.
Image #10: Normal vs. Suspicious Bruising
Source: "AbuseWatch.net, n.d."
In addition to the location of the bruise, the size and shape of the injury need to be considered.
Children are susceptible to injuries in relation to their developmental stage. If a plausible explanation is offered, consider the age of the child and the location of a suspicious injury when developing your thoughts about “reasonable cause to suspect.”
Accidental injuries usually involve injury to the bony prominences of the body, i.e., shins, elbows, and knees. For example:
Toddlers fall while learning to walk.
Young children “skin” elbows and knees when learning to ride a bicycle or playing on playground equipment.
Suspicious injuries usually occur in areas not susceptible to accidental, age-appropriate areas, as you have seen in the image above.
Consider the size and shape of the injury, as well as the location of the injury (SUNY, 2013). Consider the relationship of the mechanism of injury (explanation of how the injury occurred) to the child’s developmental stage. For example, we have discussed that toddlers fall when they learn to walk, and young children scrape their knees when learning to ride a bicycle.
Let’s think about a specific case example:
Think about if the story that was given as an explanation for an injury would produce the present physical indicators. For instance, a toddler falls to the floor while walking, not striking anything when he falls. That toddler has bruises on the back of his legs. One would expect that from a fall while walking, the toddler would have bruises and scrapes on his hands, knees, and shins and not bruises on the back of his legs. This would elicit some suspicion from you.
See the image below for additional information regarding physical indicators of abuse.
Image #11: Physical Indicators of Abuse
Source: "AbuseWatch.net, n.d."
As mentioned above, take a look at any bruises, welts, or burns carefully. Is it possible the injury is making a specific shape? Just like the image of the iron burn above, many tools can create visible markings that would specify what was used on the child.
The following image gives you additional ideas of what to look out for.
Image #12: Clues to the Mechanism of Injury
Source: "AbuseWatch.net, n.d."
The following image depicts a child who has been neglected. He is severely underweight and has been diagnosed with failure to thrive. The signs of his malnutrition are evident, even in this picture.
Now, let’s review the behavioral indicators of child maltreatment and abuse.
The behavioral signs that might be suspicious of child maltreatment and abuse include (NYS, 2025):
Child is not acting like they normally do
Child is acting oddly shy or attention-seeking
Child has a sudden drop in grades or lack of interest in their everyday activities
Child is engaging in self-destructive behaviors
Child begins isolating from their peers
Child is begging for or stealing food
Child has consistent fatigue or falls asleep often in class
Child begins lingering around the school, reluctant to go home
Child is using drugs or alcohol
Child has infrequent school attendance
Child is demonstrating sudden new sexual behavior or knowledge that is inconsistent with their age, development, circumstances, experiences, or past behaviors
It is important to remember NOT to view indicators in isolation (NYS, 2025). Each indicator must be considered in relation to the child’s current age and circumstances and in the context of their physical condition or behavior (NYS, 2025). You may need to assess if there is an explanation for the presenting concern and whether the explanation is consistent with the observed physical and behavioral indicators (NYS, 2025).
Abuse or maltreatment should never be assumed (NYS, 2025). Carefully consider your prior experiences with this child and whether there is a difference in what you are currently observing (NYS, 2025). It is important to make an objective assessment that is free from any implicit or explicit bias (NYS, 2025).
As briefly mentioned above, there might be physical indicators and behavioral indicators that a child is being sexually abused (NYS, 2025). But this is not always the case. Sexual abuse is the act of sexual activities with dependent, developmentally immature children to which they are unable to provide consent (Zeanah & Humphreys, 2018). Because many individuals who sexually abuse children are family members or friends, it makes disclosure of the abuse very difficult. Often, child victims feel shame and guilt and are afraid to disclose because of what might result.
Sexual abuse or maltreatment occurs when a parent, caregiver, or PLR of a child under the age of 18 commits or allows to be committed any of the following (Zeanah & Humphreys, 2018):
Physical touching of the child’s genitals, buttocks, breasts, mouth, or other private parts for the sexual gratification of the other individual
Engaging in intercourse or sodomy
Forcing children to engage in sexual intercourse
Exposing children to sexual activity for the sexual gratification of the other individual
Utilizing a child in a sexual performance within a video, photograph, play, or dance
The physical indicators that might point to sexual abuse include (SUNY, 2013):
Difficulty walking or sitting down
Torn, stained, or bloody underclothing
Painful or itchy genitalia
Pregnancy
Sexually transmitted diseases
Behavioral indicators that a child might be a victim of sexual abuse can include (SUNY, 2013):
Child is not willing to change to participate in physical education (PE) class at school
Self-injurious behavior, suicide attempts
Poor peer relationships
Withdrawn
Fantasy behavior
Regressive, infantile behavior
Aggressiveness
Delinquency, running away, school truancy
Reports of sexual assault by caretakers
Exaggerated fear of closeness or physical contact
But what about their caregivers? There are certainly signs that a parent or PLR might demonstrate that would point to possible sexual abuse. These caregiver behavioral signs can include (SUNY, 2013):
Protective or jealous of the child
Misuses alcohol or drugs
Has low self-esteem
Encourages the child to engage in things not appropriate for age
Is geographically isolated or lacking in social and emotional contacts outside of the family
Next, let’s review what would be defined as educational neglect.
Poor school attendance does not automatically equate to a reasonable cause to suspect maltreatment (NYS, 2025). A report of suspected educational neglect should be called in to the SCR as a remedy for excessive absences only as a last resort (NYS, 2025). School personnel should first try working with the child, family, and community agencies to identify needs and the resources available to meet those needs (NYS, 2025).
The following elements are those that must be present to warrant a call to the SCR specifically for educational neglect. These include (NYS, 2025):
The child must be excessively absent without a valid reason or excuse
The child’s education must be impaired due to the excessive absenteeism (or the child has an Individualized Education Plan (IEP) and has missed the necessary services due to excessive absenteeism)
The school officials have made efforts to engage the child and parent or PLR
The parent or PLR has been made aware of the excessive absenteeism and impairment by means beyond simply sending a note home or leaving a voicemail message
No parent or PLR has taken any action to rectify the situation
The child must be of compulsory school age and currently living in New York State
New York State’s Abandoned Infant Protection Act (AIPA) was developed to save the lives of newborns by protecting a person who does not want that infant and chooses to surrender them safely from criminal liability (NYS OCFS, 2016).
The AIPA first went into effect in 2000 and was last amended in 2010 (NYS OCFS, 2016). The most recent adjustments were removing the liability from the person surrendering the infant (NYS OCFS, 2016). Criminal liability is avoided under the following conditions (NYS OCFS, 2016):
The abandoned infant is no more than 30 days of age
The person who abandoned the infant intends that the infant will be safe from physical injury and cared for appropriately
The person who leaves the infant leaves them with an appropriate person or in a suitable, safe location and immediately notifies someone of the infant’s location
The person who surrenders the infant must intend to relinquish their responsibility and their rights of the care and custody of the infant
What would a “suitable” drop-off location be?
New York law does not specifically spell out what a suitable location would be but does consider hospitals, fire stations, and police stations as trusted suitable locations (NYS OCFS, 2016). It is important to note that these locations must be staffed in order to be considered “suitable” (NYS OCFS, 2016).
It is also important to note that this law does not affect your responsibilities as a Mandated Reporter. Any abandonment of an infant is reportable as possible child abuse or maltreatment (NYS OCFS, 2016). You would be fulfilling your duties as a Mandated Reporter if you reported this. A person who does abandon an infant in a manner that complies with the AITA law is not required to provide their name (NYS OCFS, 2016). Even if you do not have the name of the person who abandoned the infant, you must make this report to the SCR (NYS OCFS, 2016).
Children who have intellectual and developmental disabilities may present differently when they are experiencing abuse or neglect. Children who have intellectual and developmental disabilities are, in fact, also at an increased risk of maltreatment, abuse, and neglect due to their unique vulnerabilities (Scurich, 2025; McDonnell et al., 2018).
Intellectual and developmental disabilities (IDDs) are differences that usually present at birth and uniquely affect a person’s physical, emotional, and intellectual development (National Institute of Health [NIH], 2021). Several of these conditions impact multiple body systems (NIH, 2021).
The following are body systems and the IDDs that can be present (NIH, 2021):
Metabolic:
Metabolic disorders alter how the body breaks down food and utilizes it for energy.
Sensory disorders are what affect how the brain interprets information that comes from the senses of hearing, touch, taste, smell, and sight.
Ex. Autism Spectrum Disorder (ASD).
Nervous system:
Nervous system disorders can impact the brain, spinal cord, and nerves throughout the body, being associated with speech or language issues, seizures, movement problems, or even behavioral disorders, which can ultimately impact overall intelligence and learning ability.
Additional examples of IDDs that also can impact multiple systems can include Down syndrome and Prader-Willi syndrome (PWS).
In addition to the indicators listed above that can be seen physically and behaviorally in children experiencing maltreatment or neglect, make sure to consider the following indicators as well for children with IDDs. The following are physical indicators of child maltreatment and abuse in children with IDDs (NYS, 2025):
Poor hygiene
Malnutrition
Dehydration
Unexplained injuries
Medical neglect
Physical restraint marks
Because children with IDDs have unique ways in which they communicate, socialize, and understand the world in general, especially those who are unable to or struggle to verbalize what is wrong, less typical behavioral indicators are especially important to consider. Behavioral indicators of child maltreatment and abuse in children with IDDs can include (NYS, 2025):
Self-harming
Changes in sleeping patterns
Sudden or gradual changes in typical behavior
Signs of agitation, anxiety, or stress about a particular caregiver
Regression in previously acquired skills
Inappropriate sexual behavior
Because, as we said, communication can look very different with children with IDDs already, we have to take note and be aware of any non-verbal cues, potential changes in vocalization, and new difficulty in the child’s ability to communicate (NYS, 2025).
But what about different signs that can be observed from their caregivers when maltreatment or neglect might be occurring? Behavioral indicators of caregivers who care for children with IDDs can include (NYS, 2025):
Dismissive attitude
Isolation from support networks
Inconsistent explanations
Excessive anger or frustration
Children with IDDs can require extra effort, time, and patience (Tathgur & Kang, 2021). Whether it be due to a lack of support or resources, financial issues to pay for special treatment or care, problems with communication, social isolation, lack of family support, and/or difficulties with behavioral management, caregivers of children with IDDs can struggle with this and can, at times, experience high levels of stress and anxiety and sometimes even depression and burnout (Tathgur & Kang, 2021). Because of this, children with IDDs can be particularly vulnerable to exploitation as well as maltreatment and neglect (Scurich, 2025; McDonnell et al., 2018). Families of children with IDDs do best when they are supported with early intervention, adequate education, effective parenting strategies, emotional support, and community resources.
New York State Mandated Reporters may have interactions with children that occur in a virtual setting (NYS, 2025). For example, children may attend school remotely, see doctors utilizing telemedicine, and participate in mental health therapy sessions on virtual platforms (NYS, 2025). It is important to remember that if you are interacting with children in your professional role, your responsibilities as a Mandated Reporter are the same in a virtual environment (NYS, 2025).
When assessing for a child’s safety virtually, please consider all of the following (NYS, 2022; University of South Carolina, 2020):
Does the child’s demeanor or behavior seem different when someone else enters the room?
Does the child appear anxious or depressed?
Are there any indications that a child is trying to communicate something to you without someone else in the room noticing?
Has the child made any concerning statements to you, siblings, or their peers?
While trying to observe the child’s body, even if you can only see the child’s face, neck, shoulders, and chest, is there anything that seems suspicious? (bruises, welts, burns?)
If you hear or observe an altercation between children or adults, even if it does not rise to a level of making a report, is there still an opportunity for a conversation about safety or managing stress that could help?
There are several things that are important to be sure to do when working with children through a virtual setting (NYS, 2025). Always use reliable technology with adequate lighting and sound (NYS, 2025). Make sure that the child is present for at least part of the visit (NYS, 2025). Also be sure to have everyone in the room with the child introduce themselves, even those who enter the room after the visit begins (NYS, 2025).
Make sure to ask if there is enough privacy to discuss sensitive matters in the location in which the child and/or parent is virtually meeting you (NYS, 2025). This may mean asking nonparticipating household members to move to a different room. Confirm with the family their physical location in the event that you need to contact emergency services and will need to know when to send them (NYS, 2025).
Next, take note of the environment (NYS, 2025): Are there any noticeable unsafe conditions? Is there appropriate supervision of the child? Are young children watching even younger siblings?
Watch carefully during the course of your virtual interaction. Verbalize what you think you are seeing and ask if the family agrees with your observations (NYS, 2025). Pay attention to non-verbal cues (NYS, 2025). Make note if the child’s demeanor or behavior is different when someone else enters the room (NYS, 2025). Notice if a child turns off or attempts to turn off the webcam or is even hesitant to use one in the first place (NYS, 2025).
At the close of your interaction, make sure to provide clear channels for the child to reach out to you (NYS, 2025). This can be done by email, phone, chat, text, or online tool (NYS, 2025).
When dealing with child abuse or maltreatment, you are not to investigate or interrogate. Your responsibility is to assess for reasonable cause to suspect and make the necessary report.
Occasionally, you learn of possible abuse or maltreatment not by what you see but by what a child says to you.
When a child discloses, consider the following suggestions of what to do when talking with children.
It is important to (SUNY, 2013):
Find a private place
Remain calm
Be honest, open, up-front, supportive
Be an advocate
Listen to the child
Report the situation immediately
When talking with a child, stress that the situation and the behaviors are not his or her fault.
What about what not to do? It is important not to overreact. It is natural, at the moment, for us as human beings to potentially act immediately when something like this is disclosed to us. It is important that we listen and remain mindful not to react. We must also not make any quick judgments. We should also never make any promises to the child. And as mentioned above, it is not our duty to interrogate and investigate. Make sure not to do this.
You are NOT legally required to inform parents or other persons legally responsible for a child’s care that you are making a report to the SCR. Do NOT assume a parent will support the child. If you have questions or concerns about whether to inform the parents, contact your local CPS. Informing the parent or other person legally responsible may place a child at further risk of harm.
There are specific guidelines that apply to cases of suspected sexual abuse. Once a child reveals information that makes you suspect sexual abuse, avoid talking in detail with the child about the incident. Often CPS and law enforcement work together to interview a child at the same time. These professionals have been specially trained to interview children. This is a traumatic experience for a child to relive. In your role as a Mandated Reporter, try to minimize how much you talk to a child about an incident involving suspected sexual abuse.
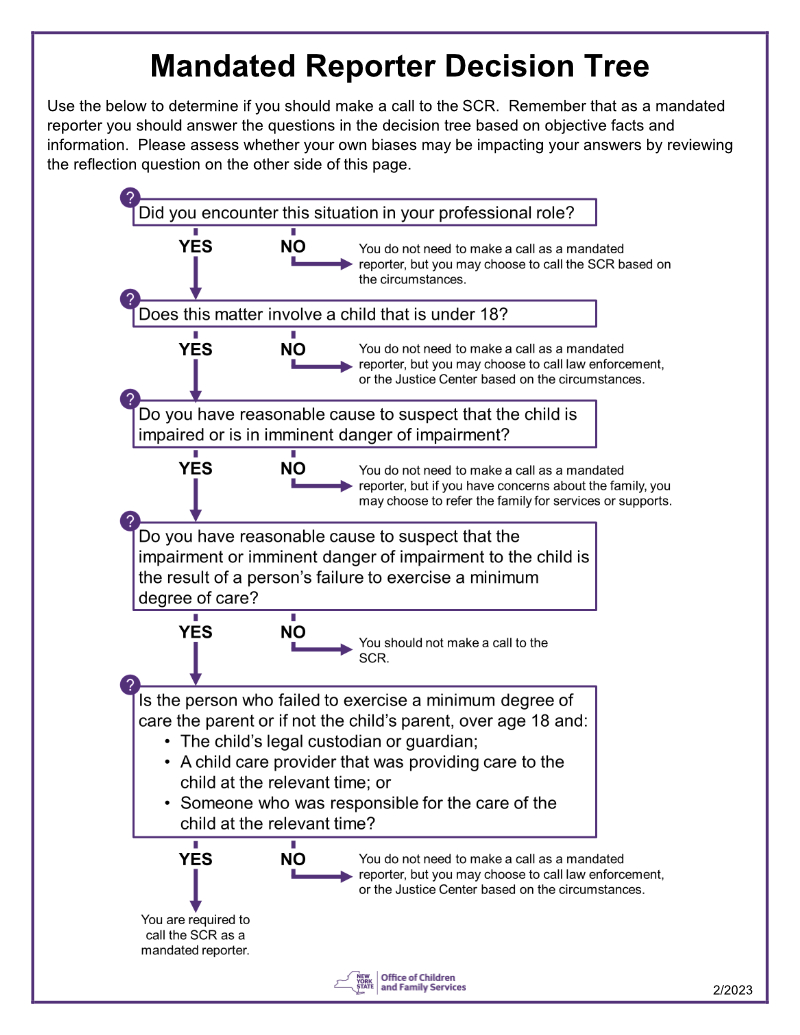
As a New York State professional, you can use the following flow chart to assist you in making the final decision of whether or not the situation that you are a witness to necessitates an SCR report. The following decision tree was developed and shared by the New York State Office of Children and Family Services in 2023:
If while in your professional role you have developed a reasonable suspicion that a child is being abused or maltreated, you are required to call the SCR immediately at the Mandated Reporter line (NYS, 2025): 1-800-635-1522.
It is important to remember that if you are in an emergency situation, it is not the time to call and report to SCR (NYS, 2025). In an emergency situation, please default to contacting 911.
As a Mandated Reporter, you need to be prepared to articulate your concerns in a clear and concise manner. It is important for you to prepare before you make the call so you will have information readily available when the CPS specialist asks you to provide it.
It is also important to note here not to have the child in the room or put the child on the phone with CPS unless extremely necessary. This can be too distressing for the child. You, as the trusted adult, can speak for the child and seek clarification if needed.
During your phone call, provide your direct contact information as well as an alternate contact number at the beginning of the call in case you become disconnected. Explain to the CPS specialist what your suspicions or concerns are relative to the child who has come to your attention. Explain whether the child has been subjected to harm and why you think this.
Some Mandated Reporters have consistent and close contact with a child or parent because of the nature of their profession. This may give the Mandated Reporter an advantage in being able to assess the overall condition of the child.
Some identifying information is required. The local CPS agency will need some way to be able to locate the child.
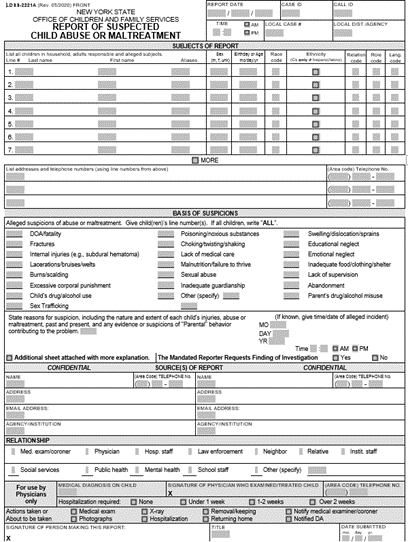
A useful tool you can use to organize your information is the LDSS-2221A Form. You will also be completing this form in addition to your phone call.
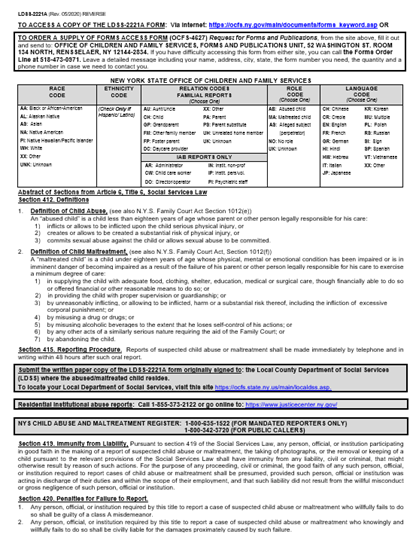
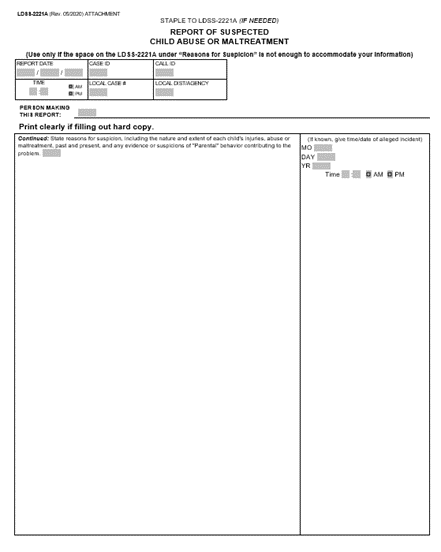
As a Mandated Reporter for child abuse and maltreatment, you are required to fill out and submit a specific form following your phone call report to SCR (NYS, 2025). This form is the LDSS 2221A Form.
The LDSS 2221A Form must be completed and submitted to the local department of social services within 48 hours of your call to SCR (NYS, 2025).
(New York State Office of Children and Family Services [NYS OCFS], n.d.-a)
The image above is the first page of the three pages of the LDSS 2221A form. For your access and ease of use, it is available online at OCFS’ website here.
At this link, you are also able to access and download the LDSS 2221A in several additional languages, including Spanish, Italian, Chinese, and Russian.
For a direct link to a Microsoft Word version of the form, visit here.
Upon completion of this form, send it to your local Department of Social Services. There is a link included on the form to assist with finding where to bring it.
To fully complete the LDSS 2221A Form, you will need to have the following (NYS, 2025):
Your full name as the Mandated Reporter
The name of your agency or organization
Your contact information, including your phone number and email address
The full name of the parent or PLR for the child
The parent's or PLR’s dates of birth, if available
The full name of the child or children you suspect are being abused or maltreated
The child or children’s dates of birth, if available
The specific information which led to you having a reasonable suspicion of abuse or maltreatment
The addresses or locating information for the parent or PLR as well as the child or children
The name of any other Mandated Reporter you believe personally observed or was provided with relevant information about the child
Image 16: LDSS 2221A Form Page 2
(New York State Office of Children and Family Services [NYS OCFS], n.d.-a)
This second page reviews explanations of the codes you will input on the first page.
Image 17: LDSS 2221A Form Page 3
(New York State Office of Children and Family Services [NYS OCFS], n.d.-a)
This third and final page provides additional space for you to provide a detailed explanation of your reasons for suspicion and any other relevant information you choose to include.
*It is important to note that one of the most crucial components needed for reporting is the address or locating information for the child and their parent or PLR (NYS, 2025). This is essential to have when you call the SCR. The SCR will not be able to accept the report if you do not have this information (NYS, 2025).
Let’s discuss what criteria are required for the SCR to accept a report made by Mandated Reporters. The SCR is bound by legal criteria which decide whether they can accept a report (NYS, 2025). For the SCR to accept a report, the following criteria must be met (NYS, 2025):
The child must be born and under 18 years of age
The alleged perpetrator must be the child’s parent or another person over the age of 18 who is the PLR for the child
The conduct described must meet the legal definition of maltreatment or abuse
The SCR is not legally required to accept the report just because you are calling as a Mandated Reporter (NYS, 2025). The staff at SCR will conduct their own interview in order to determine if the information you provide them with during the call rises to the legal level of suspected child abuse or maltreatment (NYS, 2025). In the event that it does not rise to this level, based on the information you provided, the SCR cannot and will not accept the report (NYS, 2025).
As long as you call the SCR and provide all the information you have, you have fulfilled your legal obligation by making the call, even if the SCR declines to accept the report (NYS, 2025).
If the SCR cannot register the report you are trying to make, the reason for their decision should be clearly explained to you, and you should be offered an opportunity to speak to a supervisor.
If you are not satisfied with the outcome of your interview with the CPS specialist, be sure to ask to speak with a supervisor. Supervisors are on duty at the SCR around the clock and can be very helpful in clarifying issues and reviewing decisions whenever necessary.
After you complete your call to the SCR, immediately notify the person in charge of the institution, school, facility, or agency, or the designated agent of the person in charge, and provide the information reported to the SCR, including the names of other persons identified as having direct knowledge or the alleged abuse or maltreatment and other Mandated Reporters identified as having reasonable cause to suspect.
Once notified that a report has been made to the SCR, the person in charge or designated agent becomes responsible for all subsequent administration concerning the report, including preparation and submission of the form LDSS-2221A.
As suggested earlier, if time permits, it may be helpful to fill out the form before placing your call to the SCR. This enables you to organize whatever demographic and identifying information you might have, as well as your allegations and concerns.
REMEMBER: The safety of the child must come before the completion of the form.
Once the SCR has officially accepted a report, the SCR forwards it to the local Department of Social Services for further investigation (NYS, 2025). The SCR then follows up with the local Department of Social Services that the report was sent to in order to receive a confirmation that the report has been received (NYS, 2025). Once the local Department of Social Services has the report, they must begin their investigation within 24 hours of receiving the report (NYS, 2025).
During their investigation, the CPS caseworker assigned to the case must comply with numerous regulations and policies to ensure that they conduct a thorough investigation and safety assessment (NYS, 2025). CPS is required to contact the parent or PLR and the children involved (NYS, 2025). CPS will also contact the source of the report and may ask for additional information or clarification (NYS, 2025). The assigned CPS caseworker might also request copies of reports or records from you which you are required by law to provide (NYS, 2025).
Within 60 days of filing the report, the CPS agency must determine whether the cited allegations are substantiated (meaning that there is evidence that the allegations that were made were true) or unsubstantiated (meaning that the was not enough evidence that the allegations made were true) (NYS, 2025). CPS caseworkers are also obligated to offer the parents or PLR services for them, or the children or children involved, which may be helpful (NYS, 2025).
Please view the following image to get an idea of what the CPS system process is from the initial report phone call.
Image #18: CPS System Flowchart
(Adapted from New York State Office of Children and Family Services)
CPS intervention in a family’s life can be positive. It can provide stability and a structure for change. The CPS system works to support families through crisis and stress in their lives. Working with a family to improve their lives and break the cycle of abuse and maltreatment is the purpose of the intervention.
Instead of thinking of your report to the SCR as punitive, remember that sometimes intervention can provide exactly the kind of help a family needs to prevent the abuse or maltreatment from causing irreversible harm.
Whether or not you believe the child's parent(s) or legally responsible adult(s) will be open to intervention, you are still obligated to make the report to the SCR. In some cases, a report is the “wake-up call” a parent needs or a means of gaining assistance in areas of their lives that have become unmanageable.
The most common outcome of a CPS investigation is that the caseworker will spend time and work with the family to help them obtain necessary services or aid to alleviate problems and promote safety (NYS, 2025). It is important to keep in mind that CPS intervention is not required in order for parents, PLRs, children, or families to obtain and utilize services (NYS, 2025). We are all able to support a family without having to report a family (NYS, 2025).
The following are some of the questions and answers found in the frequently asked questions section of the New York State Office of Children and Family Services CPS page (NYS OCFS, n.d.-b).
Where can I find the laws pertaining to Child Protective Services and Social Services?
There are two bodies of law in New York State that deal with child abuse and maltreatment, specifically in a familial context (NYS OCFS, n.d.-b):
Social Services Law (SSL), Title Six Article Six, sections 411-428
Family Court Act (FCA), Article 10 section 1012
It is important to also know that some acts of child abuse and maltreatment are also crimes. For more information on the crimes associated with child abuse and maltreatment, you should contact your local police or district attorney's office or refer to the Penal Law (NYS OCFS, n.d.-b).
What happens after I make a report?
The Child Protective Service (CPS) unit of the local department of social services is required to begin an investigation of each report within 24 hours (NYS OCFS, n.d.-b). CPS may take a child into protective custody if it is essential for the protection from further abuse or maltreatment. Based upon an assessment of the circumstances, CPS may offer the family appropriate services. The CPS caseworker has the responsibility to petition the Family Court to mandate services when they are necessary for the care and protection of a child. CPS then has 60 days after receiving the report to determine whether the report is "indicated" or "unfounded” (NYS OCFS, n.d.-b).
Who decides what information pertaining to the report is "essential for a full investigation" and, therefore, must be provided to CPS: the Mandated Reporter or CPS?
In the first instance, the Mandated Reporter to whom the request is directed makes the
determination of what information is essential. If CPS believes that the Mandated Reporter has additional essential information pertaining to the report, CPS should ask the Mandated Reporter for the additional records and attempt to come to agreement regarding any additional records. If CPS and the Mandated Reporter cannot come to agreement and CPS disagrees with the Mandated Reporter's rationale for why the records are not relevant to the report, CPS may seek a court order pursuant to Civil Practice Law and Rules (CPLR) Article 31 and SSL §415 directing the Mandated Reporter to produce the essential information (NYS OCFS, n.d.-b).
What can I do if someone has filed a false child abuse or maltreatment report against me with the Statewide Central Register?
The New York State OCFS takes any false report extremely seriously, as the taking of the false report and the following investigation are a misuse of valuable time and resources. According to section 240.50 of the New York State Penal Law, falsely reporting a case is a Class A misdemeanor (NYS OCFS, n.d.-b). If you are a victim of a false report, contact your local police department to discuss your options.
At what age is it okay to leave children home alone in New York State?
There is no straightforward answer to this question, and there is no state-mandated law. All children develop at their own rate and have their own unique special needs and abilities. Some children are responsible enough to be left alone at 12 or 13, whereas some are not mature enough at that age to be left alone, much less watching another child.
Questions that can be considered prior to leaving a child alone or allowing a child to babysit include (NYS OCFS, n.d.-b):
How mature is the child?
How comfortable is the child with being alone?
What has the child done to demonstrate responsibility?
Does the child know how to contact emergency help if needed?
Is the child capable of preparing food for themselves?
Are there dangerous hazards in the child’s environment (knives, ovens)?
The following important child abuse-related terms are found within the 2023 New York State Child Protective Services Manual (NYS OCFS, 2023a). For the complete list of definitions, please refer to the glossary of terms.
Abused Child: A child under the age of 18 whose parent or other person legally responsible for his/her care inflicts upon the child serious physical injury, creates a substantial risk of serious physical injury, or commits a sex offense against the child (NYS OCFS, 2023a).
Indicated Report: Upon conclusion of the investigation, the local investigative agency determined there was some credible evidence to support the allegations in the report (NYS OCFS, 2023a).
Maltreated Child: A child under the age of 18 whose parent(s) or other person legally responsible for the care of a child harms a child or places a child in imminent danger of harm by failing to exercise the minimum degree of care in providing the child with any of the following when financially able to do so (NYS OCFS, 2023a):
Food
Clothing
Shelter
Education
Medical care
Maltreatment can also result from abandonment of a child or from not providing adequate supervision for the child. Furthermore, a child may be maltreated if a parent engages in excessive use of drugs or alcohol such that it interferes with their ability to adequately supervise the child (NYS OCFS, 2023a).
Neglected Child: A child under the age of 18 whose mental, emotional, or physical health has been impaired or in imminent danger of becoming impaired because of failure of the minimum degree of care requirement of their parent or person legally responsible (NYS OCFS, 2023a).
Person Legally Responsible: This individual includes the child's custodian, guardian, and any other person responsible for the child's care at the relevant time. A custodian may include any person continually or at regular intervals found in the same household as the child when the conduct of such person causes or contributes to the abuse or neglect of the child (NYS OCFS, 2023a).
Preliminary Assessment of Safety: This is when an initial evaluation of the safety factors decides if the child or children named within the report may be in imminent danger or serious harm. If the child or children is/are assessed to not be safe, immediate action is taken to protect the child or children (NYS OCFS, 2023a).
Protective Custody: The action of law enforcement or a designated employee of the state taking and holding a child or children from a place, home, or circumstance in the case where the child or children is believed to be in imminent danger (NYS OCFS, 2023a).
Reasonable Cause to Suspect: A logical basis for your concern (NYS OCFS, 2023a). It does not mean you have to be certain or have proof.
Subject of a Report: Any parent of, guardian of, custodian of, or other person eighteen years of age or older legally responsible for a child reported to the central register of child abuse and maltreatment who is allegedly responsible for causing injury, abuse, or maltreatment to such child (NYS OCFS, 2023a).
Unfounded Report: Upon conclusion of the investigation, the local investigative agency determined there was no credible evidence to support the allegations in the report (NYS OCFS, 2023a).
Emma, a 13-year-old female, has come into the emergency room with a rash in her vaginal area. She shares with you that she has been engaging in sexual intercourse with her mother’s 42-year-old boyfriend for the past four months. Emma’s mom’s boyfriend has resided in the house with the child and her mother for the past three years and is responsible for her care when the mother is working as a bartender.
What indicators are present?
Is there a reasonable cost to suspect abuse or maltreatment?
Is there a parent or other person responsible for the suspected abuse or maltreatment?
Tommy, a five-year-old male, came into his pediatrician’s office for a sports physical so he can play soccer at school. You notice that he has a bruise on the left side of his face with scrapes along his left arm and hand. Tommy claimed he fell off the monkey bars at school. He lives with his mother, who is a single parent. Tommy’s mother says that he is a very active child and, at times, can misbehave at school.
What indicators are present?
Is there a reasonable cost to suspect abuse or maltreatment?
Is there a parent or other person responsible for the suspected abuse or maltreatment?
Pamela, a 32-year-old female, is admitted to the obstetric unit at your hospital. She delivers her child, Sarah. After 36 hours of birth, the nurse notices that Sarah has tremors and increased muscle tone. Sarah is soon diagnosed with neonatal abstinence syndrome (NAS) by the neonatologist, as she is showing signs of drug withdrawal from when Pamela was pregnant with her. When talking to Pamela, you learned she has not prepared at all for her baby to come home.
What indicators are present?
Is there a reasonable cost to suspect abuse or maltreatment?
Is there a parent or other person responsible for the suspected abuse or maltreatment?
Seven-year-old Nick comes to the emergency room with an injured arm. His mother says he fell off the trampoline when he was jumping around and playing with his friend. An X-ray is ordered to assess for any breaks. When Nick’s arm is X-rayed, a spiral fracture of his humerus is identified.
What indicators are present?
Is there a reasonable cost to suspect abuse or maltreatment?
Is there a parent or other person responsible for the suspected abuse or maltreatment?
Three-year-old Emily comes into the pediatric primary care clinic for her yearly well-child examination. You notice ligature marks and bruising around both of her wrists. You ask Mom what these are from. Mom indicates that she knows her child is good but is sometimes possessed by evil spirits that make her do bad things. She tells you that in her culture, it is common practice to tie the child to their bed and restrict food in order to eliminate the evil spirit.
What indicators are present?
Is there a reasonable cost to suspect abuse or maltreatment?
Is there a parent or other person responsible for the suspected abuse or maltreatment?
Four-month-old Sabrina is brought into the emergency room for being unresponsive. Mom accompanies Sabrina. Mom indicates that Sabrina was fine until they got back home from running errands. Mom says that her boyfriend, Rick, was watching her while she took a shower. She said that she heard Sabrina crying. When the crying had been continuous for ten minutes and then abruptly stopped, she heard Rick yell that he was going to pick up some cigarettes from the gas station and then slam the door. Mom finished getting dressed and went back to Sabrina’s room to check on her. Mom initially thought she was asleep in her crib, but on closer examination, she was not breathing. Mom notes that Rick does have a temper and that he is frustrated easily with Sabrina.
What indicators are present?
Is there a reasonable cost to suspect abuse or maltreatment?
Is there a parent or other person responsible for the suspected abuse or maltreatment?
Benjamin is a 17-year-old who attends the school you teach at. Benjamin is in your English class but has not come to school in a few weeks. You reach out to his mother, who tells you he is absolutely refusing to go to school, and there is nothing she can do to get him to go. She said that he has a job at the local convenience store and spends all of his time there.
What indicators are present?
Is there a reasonable cost to suspect abuse or maltreatment?
Is there a parent or other person responsible for the suspected abuse or maltreatment?
You are discussing with the mother of a two-year-old about how much stress she is currently dealing with. She admits that she leaves her son, Elijah, at home alone at least once a week so that she can run to the corner store to buy groceries. She says that he’s just fine and that she tells her neighbors that she’ll be back in 15 to 20 minutes and just to listen out for him.
What indicators are present?
Is there a reasonable cost to suspect abuse or maltreatment?
Is there a parent or other person responsible for the suspected abuse or maltreatment?
You are back in the Young family’s house for another welfare check. The single mother, Tina, has two children, Christian, who is 10-year-old male, and Sarah, who is an eight-year-old female with ASD. Today’s visit was unannounced, so mom did not know you were coming. She says she’s been overwhelmed lately and has had to call out of work for the last two days. Christian appears calm, quiet, and pleasant as he did on your last visit, just doing his homework at the kitchen table. However, Sarah is alone in her bedroom in the dark. Tina explains that she is in time-out for being bad at school today. When you go in to see her, you notice that her hair is messy and seemingly unkempt, she’s dressed in pajamas that are heavily stained with what looks like dirt, and she looks to maybe have lost weight since you last saw her. You also notice what looks like bilateral restraint marks on both of her wrists when you gently adjust her nightgown sleeves. She has a large bandage on her right thigh that mom says is a self-inflicted wound that she was planning on having the pediatrician look at in the next few days. You ask mom to remove the bandage so you can take a look. Tina rolls her eyes at you initially, saying “she’s fine,” but then lifts the bandage to reveal several 3-4-inch-long cuts that have greenish-yellow pus oozing from them.
What indicators are present?
Is there a reasonable cost to suspect abuse or maltreatment?
Is there a parent or other person responsible for the suspected abuse or maltreatment?
What indicators are present? Sexual abuse and verbal disclosure
Is there reasonable cause to suspect abuse or maltreatment? Yes
Is there a parent or other person responsible for the suspected abuse or maltreatment? The 42-year-old boyfriend is an adult living in the home, acting as a caregiver when the mother is away at work.
What are your next steps? Call SCR.
Case Study 2
What indicators are present? Bruises, scrapes
Is there reasonable cause to suspect abuse or maltreatment? No, the story is consistent with a playground injury. Injuries sustained in an accidental fall would be along one side of the child’s body.
Is there a parent or other person responsible for the suspected abuse or maltreatment? No
What are your next steps? Prioritize the treatment of the child’s injury. You do not need to report this to SCR.
Case Study 3
What indicators are present? Neonatal drug withdrawal and no plan for when the baby comes home from the hospital
Is there reasonable cause to suspect abuse or maltreatment? Yes
Is there a parent or other person responsible for the suspected abuse or maltreatment? Mother
What are your next steps? Call SCR.
Case Study 4
What indicators are present? Spiral fracture, the explanation for the injury is not plausible.
Is there reasonable cause to suspect abuse or maltreatment? Yes
Is there a parent or other person responsible for the suspected abuse or maltreatment? Mother
What are your next steps? Call SCR.
Case Study 5
What indicators are present? Ligature marks around the risks, mom’s admission that she ties the child up to her bed and denies her food
Is there reasonable cause to suspect abuse or maltreatment? Yes
Is there a parent or other person responsible for the suspected abuse or maltreatment? Mother
What are your next steps? Although this appears to be a cultural practice, it is illegal to use these means to deal with the misbehavior of a child. Call SCR.
Case Study 6
What indicators are present? Mom’s boyfriend was taking care of the baby, Sabrina was fine one minute and then not breathing the next, reported to the ER for unconsciousness, boyfriend has a temper, boyfriend left suspiciously for cigarettes.
Is there reasonable cause to suspect abuse or maltreatment? Yes
Is there a parent or other person responsible for the suspected abuse or maltreatment? Mother’s boyfriend, Rick
What are your next steps? This case is suspicious of shaken baby syndrome and should be worked up as such in the ER. Call SCR.
Case Study 7
What indicators are present? Benjamin is not going to school anymore.
Is there reasonable cause to suspect abuse or maltreatment? No, it seems Mom has tried. Additional attention can be given specifically to Benjamin to confirm Mom’s story.
Is there a parent or other person responsible for the suspected abuse or maltreatment? No
What are your next steps? According to the compulsory attendance law in New York, children between the ages of six and sixteen are required to attend school regularly. It also says that children over the age of 17 have the right to determine whether or not they go to school (New York State Education [NYSED], 2022). You do not need to report.
Case Study 8
What indicators are present? Mom is under a lot of stress; she also admits to leaving two-year-old Elijah home alone while she runs to the store.
Is there reasonable cause to suspect abuse or maltreatment? Yes
Is there a parent or other person responsible for the suspected abuse or maltreatment? Mother
What are your next steps? This is considered inadequate supervision. Mom should never do this. Someone must be physically present with Elijah while she is out in case of an emergency. Call SCR to report.
Case Study 9
What indicators are present? Mom is under a lot of stress being a single mom, trying to provide for two children, one of which has an IDD; Sarah is alone in a dark room, unkempt, has lost weight, and has restraint marks on her wrists; Tina was reluctant and had a dismissive attitude about the bandage that ultimately revealed an infected, supposedly self-inflicted wound.
Is there reasonable cause to suspect abuse or maltreatment? Yes
Is there a parent or other person responsible for the suspected abuse or maltreatment? Mother
What are your next steps? This child with IDD is showing behavioral and physical signs of abuse. Call SCR.
Child abuse and maltreatment are, unfortunately, quite common. With an improved understanding of what to look out for, what situations warrant additional resources or referrals, and the New York State reporting process, Mandated Reporters have the unique position, due to their positions in their work roles, to file a report when they suspect a child or children is being mistreated or abused. We all have the ability to identify a child in need and speak up on their behalf to protect them!
New York State is divided into 58 local social services districts. The five boroughs of New York City comprise one district. Outside of New York City, each district corresponds to one of the fifty-seven counties that make up the remainder of the state.
County Departments of Social Services (DSS) provide or administer the full range of publicly funded social services and cash assistance programs. Families whose income meets state guidelines and who meet other criteria may be able to receive a subsidy to offset some of their childcare costs.
Listed below is an alphabetical list of the 58 DSS Offices available throughout New York State.
The Administration for Children and Families (ACF) is a federal agency funding state, territory, local, and tribal organizations to provide family assistance (welfare), child support, childcare, Head Start, child welfare, and other programs relating to children and families.
The Children's Bureau Express is designed for professionals concerned with child abuse and neglect, child welfare, and adoption. The Children's Bureau Express is supported by the Children's Bureau, Administration for Children and Families, U.S. Department of Health and Human Services and published by the National Clearinghouse on Child Abuse and Neglect Information and the National Adoption Information Clearinghouse.
Since 1948, the Annie E. Casey Foundation (AECF) has worked to build better futures for disadvantaged children and their families in the United States. The primary mission of the Foundation is to foster public policies, human service reforms, and community support that more effectively meet the needs of today's vulnerable children and families.
The Child Welfare League of America is the nation's oldest and largest membership-based child welfare organization. It is committed to engaging people everywhere in promoting the well-being of children, youth, and their families, and protecting every child from harm.
The National Children's Alliance is a group of 53 national organizations with an interest in the well-being of children and youth.
National Data Archive on Child Abuse & Neglect — Website
A resource since 1988, NDACAN promotes scholarly exchange among researchers in the child maltreatment field. NDACAN acquires microdata from leading researchers and national data collection efforts and makes these datasets available to the research community for secondary analysis.
New York State Office for Children and Family Services — Website
A variety of resource information related to child abuse and maltreatment/neglect specific to New York State.
U.S. Department of Health and Human Services — Website
A wide variety of resources is available on the home page of this federal agency.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
AbuseWatch.net. (n.d.). Prevention resources for the community and professionals. AbuseWatch.net. Visit Source.
Baker, A. J., LeBlanc, S., Adebayo, T., & Mathews, B. (2021). Training for mandated reporters of child abuse and neglect: Content analysis of state-sponsored curricula. Child Abuse & Neglect, 113, 104932. Visit Source.
Bellazaire, A. (2018). Health report: Preventing and mitigating the effects of adverse childhood experiences. National Conference of State Legislatures. Visit Source.
Brown, C. L., & Yilanli, M. (2025). Child physical abuse and neglect. StatPearls Publishing. Visit Source.
Brown, C.L., Yilanli, M., Rabbitt, A.L. (2023). Child physical abuse and neglect. StatPearls Publishing. PMID: 29262061. Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024a). About child abuse & neglect. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024b). About adverse childhood experiences. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024c). Risk and protective factors. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2020). Infographic: 6 guiding principles to a trauma-informed approach. Centers for Disease Control and Prevention (CDC). Retrieved April 15, 2024. Visit Source.
Gaillard-Kenney, S. F., Kent, B., Lewis, J., & Williams, C. (2020). Effects of trauma-informed care training on healthcare providers caring for victims of human trafficking. Internet Journal of Allied Health Sciences & Practice, 18(3), 1–8. Visit Source.
Gonzalez, D., Bethencourt Mirabal, A., & McCall, J.D. (2023). Child abuse and neglect. StatPearls Publishing. PMID: 29083602. Visit Source.
Integrative Life Center. (2021). What are the 10 adverse childhood experiences? Integrative Life Center. Visit Source.
McDonnell, C. G., Boan, A. D., Bradley, C. C., Seay, K. D., Charles, J. M., & Carpenter, L. A. (2018). Child maltreatment in autism spectrum disorder and intellectual disability: Results from a population-based sample. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 60(5), 576. Visit Source.
National Child Abuse and Neglect Data System. (NCANDS). (2021). New York child maltreatment data. U.S. Department of Health and Human Services. Visit Source.
National Conference of State Legislatures. (NCSL). (2021). Adverse childhood experiences. National Conference of State Legislatures (NCSL). Visit Source.
National Institute of Health (NIH). (2021). About intellectual and developmental disabilities (IDDs). National Institute of Health. (NIH). Visit Source.
New York State. (NYS). (2025). 2025 NYS mandated reporter training syllabus. New York State. Visit Source.
New York State Education. (NYSED). (2022). Religious and independent schools: State requirements and programs. New York State Education (NYSED). Visit Source.
New York State Office of Children and Family Services. (NYS OCFS). (n.d.-a). Child protective services. New York State Office of Children and Family Services. Visit Source.
New York State Office of Children and Family Services. (NYS OCFS). (n.d.-b). Child protective services FAQ. New York State Office of Children and Family Services. Visit Source.
New York State Office of Children and Family Services. (NYS OCFS). (2024a). Summary guide for mandated reporters in New York State. New York State Office of Children and Family Services (NYS OCFS). Visit Source.
New York State Office of Children and Family Services. (NYS OCFS). (2024b). Abandoned infant protection act. New York State Office of Children and Family Services (NYS OCFS). Visit Source.
New York State Office of Children and Family Services. (NYS OCFS). (2023a). Child protective services manual. New York State Office of Children and Family Services. Visit Source.
New York State Office of Children and Family Services. (NYS OCFS). (2023b). Mandated reporter decision tree. New York State Office of Children and Family Services. Visit Source.
Rizvi, M.B., Conners, G.P., & Rabiner, J. (2023). New York State Child Abuse, Maltreatment, and Neglect. StatPearls Publishing. Visit Source.
Scurich, N. (2025). Maltreatment of children with disabilities in the United States. Journal of Public Child Welfare, 1–16. Visit Source.
State University of New York. (SUNY). (2013). Mandated reporter training: Identifying and reporting child abuse and maltreatment/neglect (CARR workshop). SUNY Buffalo State College. Visit Source.
Tathgur, M. K., & Kang, H. K. (2021). Challenges of the caregivers in managing a child with autism spectrum disorder— A qualitative analysis. Indian Journal of Psychological Medicine, 43(5), 416. Visit Source.
Tracy, E. & Macias-Konstantopoulos, W. (2023). Human trafficking: Identification and evaluation in the healthcare setting. UpToDate. Retrieved April 15th, 2024. Visit Source.
University of South Carolina. (2020). Virtual settings: Recognizing and reporting child abuse & neglect. Visit Source.
World Health Organization. (WHO). (2023). Youth violence. World Health Organization (WHO). Visit Source.
Zeanah, C.H., & Humphreys, K.L. (2018). Child abuse and neglect. Journal of the American Academy of Child & Adolescent Psychiatry, 57(9), 637-644. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.





_800px.jpg)
_800px.jpg&description=CEUfast.com - graphic showing adverse childhood experiences)