This course will be updated or discontinued on or before Saturday, October 24, 2026
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will know how to care for patients with placental complications.
Objectives
After completing this continuing education course, the participant will be able to:
Define the role of the placenta.
List the risk factors for an abnormal placenta.
Describe the potential placental complications that can occur.
Identify the risks to the mother and fetus that can occur as a result of placental complications.
Plan the nursing care for women with placental complications.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
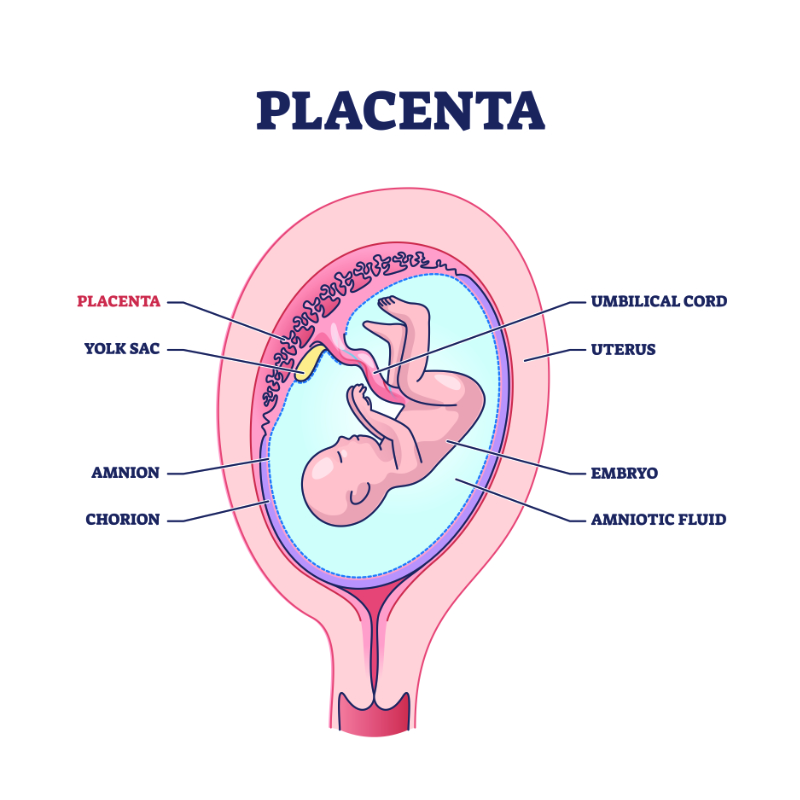
The placenta is a vital organ needed for endocrine, immune, and physiological functions as the fetus develops (Herrick & Bordoni, 2023). The placenta develops along with the fetus at the time of fertilization.
Image 1: Placenta
The placenta is the organ that transports oxygen and nutrients to the fetus from the mother while removing waste from the fetus as well. There is normally no mixing of maternal and fetal blood (Herrick & Bordoni, 2023). The placenta is usually attached to the top, side, front or back of the uterus but can also attach lower in the uterus near the cervix, which may lead to complications. Any abnormal development of the placenta can cause complications for the mother and the fetus (Herrick & Bordoni, 2023).
Certain factors can place the placenta at risk for complications. Some issues that can impact placental function and can lead to placental complications can include (Mayo Clinic Staff, 2022a):
High blood pressure
Maternal age > 40
Premature rupture of membranes (PROM)
Blood clotting disorders
A twin or multiple pregnancies
Previous uterine surgery or previous placental complications
Substance use, including tobacco and drugs, especially cocaine use
Abdominal trauma such as a fall or motor vehicle accident
Abnormal development is the first set of complications with the placenta. Preeclampsia and intrauterine fetal growth restriction (IUGR) may be caused by abnormal development of the placenta.
During a normal pregnancy, trophoblasts are some of the first cells that contribute to the formation of the placenta (Meakin et al., 2022). These trophoblasts differentiate into many different subtypes with individual functions (Meakin et al., 2022). Further development and differentiation of these trophoblasts leads to the process of maternal wall invasion (Meakin et al., 2022). This is what helps to form the connection that will allow for proper nutrient exchange during pregnancy (Meakin et al., 2022). When defects in endovascular extravillous trophoblast (EVT) invasion occur, some spiral arteries are not invaded at all, and some are invaded superficially. This problem can lead to reduced blood flow in the intervillous space and hypoxia (Roberts & Myatt, 2023).
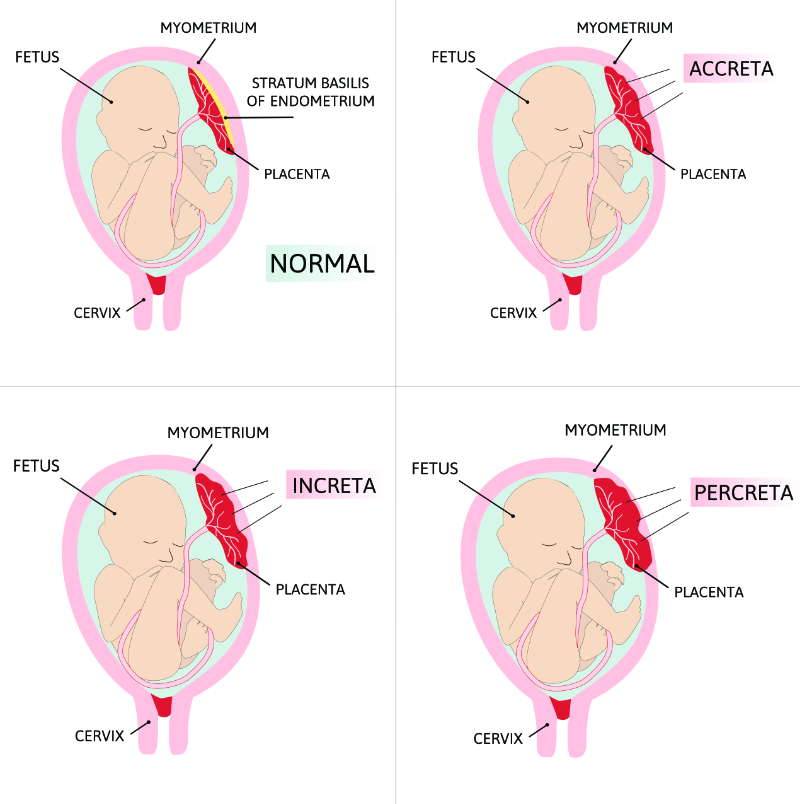
A placenta accreta spectrum is a group of placental abnormalities based on adherence to the placenta, including placenta accreta, increta, and percreta (American College of Obstetricians and Gynecologists [ACOG], 2018).
Image 2: Types of Placenta Accreta
Placenta accreta is an abnormal invasion of trophoblasts into part of a portion of the myometrium, which is the middle and thickest layer of uterine wall (ACOG, 2018). Placenta accreta occurs when the placental villi attach to the myometrium (Silver, 2024). In placenta increta, the placental villi actually penetrate the myometrium (Silver, 2024). In placenta percreta, the placental villi fully penetrate through the myometrium layer and into the uterine serosa and/or other internal organs (Silver, 2024). The chief risk factors for the placenta accreta spectrum are (ACOG, 2018):
Previous cesarean sections
Previous placenta previa
Previous uterine surgery
The placenta accreta spectrum is often diagnosed with ultrasound (Rathburn & Hildebrand, 2022). An ultrasound may suggest placenta accreta in the first trimester but is more often found in the second and third trimester. An ultrasound that does not show placenta accreta does not mean that there is not one. It is important to also consider risk factors (ACOG, 2018). An MRI may be used to evaluate the placenta further, but MRI has not been proven to improve the accuracy of diagnosis.
Women with the placenta accreta spectrum should deliver in an experienced, high-level maternity care center with a multi-disciplinary team (ACOG, 2018). This team should minimally include experienced obstetricians, maternal-fetal medicine specialists, neonatologists, pelvic surgeons, urologists, anesthesiologists, critical care experts, interventional radiologists, and general surgeons (ACOG, 2018).
Women with placenta accreta spectrum should usually deliver between 34 0/7 to 35 6/7 weeks gestation. Earlier delivery may be recommended. Before the woman delivers, she should have pre-operative consultations with appropriate providers and have her hemoglobin maximized. All team members should be aware of this condition at the time of the scheduled cesarean section. A surgical suite may be more appropriate with extra surgeons to assist. This may include obstetricians, anesthesiologists, pelvic surgeons, gynecologic oncologists, general surgeons, trauma surgeons, neonatologists, and critical care experts. A cell saver, a device that collects and then returns a patient’s blood back to them, may be used during surgery, and blood products should be available, with the blood bank being aware of the patient. Postoperative care may require intensive care (ACOG, 2018).
These women are at high risk for hemorrhage. A hysterectomy may be necessary to stop hemorrhage during delivery. A massive transfusion may be initiated, and tranexamic acid may be given prophylactically (ACOG, 2018). These women may also have an injury to other organs and require extensive surgery. The fetus is at risk for complications due to preterm delivery.
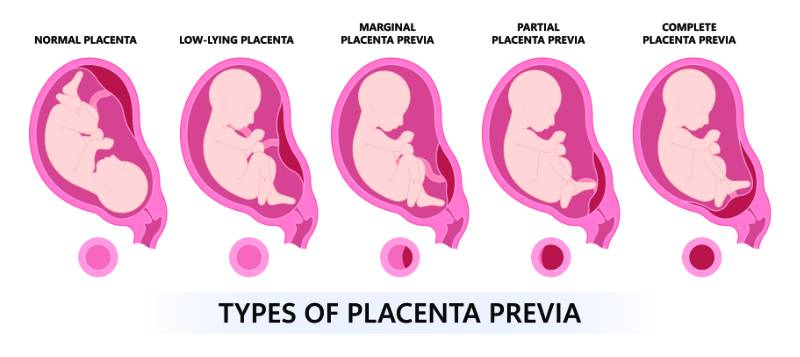
Placenta previa is when the placenta extends over the cervical os. The previa may be partial or complete. The main risk factors for placenta previa are (Anderson-Bagga & Sze, 2023):
Previous placenta previa
Previous cesarean section(s)
Multiple pregnancies
Smoking
Cocaine use
Prior dilation and curettage
Assisted reproductive technology
Image 3: Types of Placenta Previa
Placenta previa is diagnosed by ultrasound. A partial placenta previa may resolve as the pregnancy advances. The woman may present with vaginal bleeding. A vaginal exam should not be performed on a pregnant woman who is bleeding. An ultrasound should be performed and should also look for placenta accreta spectrum (Lockwood & Russo-Stieglitz, 2024).
Placenta previa puts a woman at high risk of antepartum and postpartum hemorrhage. Women with previa are advised not to have sexual intercourse or perform heavy lifting or exercise, as this may increase their risk of bleeding. Actively bleeding placenta previa is an obstetric emergency. These women should be stabilized if possible and may need a blood transfusion. If she stabilizes, a woman may not have to deliver at the first sign of bleeding. Women with uncomplicated placenta previa should have a cesarean section at 36 0/7 to 37 6/7 weeks. If the previa is found at 36 weeks or greater, delivery by cesarean is recommended at that time. If the bleeding is severe and persistent, the delivery may be indicated at any gestational age. The patient with a placenta previa is at risk for postpartum hemorrhage, which can require blood transfusions, hysterectomy, and intensive care after delivery. The fetus is at risk for complications from preterm delivery, such as low birth weight, lower APGAR scores, and respiratory distress syndrome (RDS) (Anderson-Bagga & Sze, 2023).
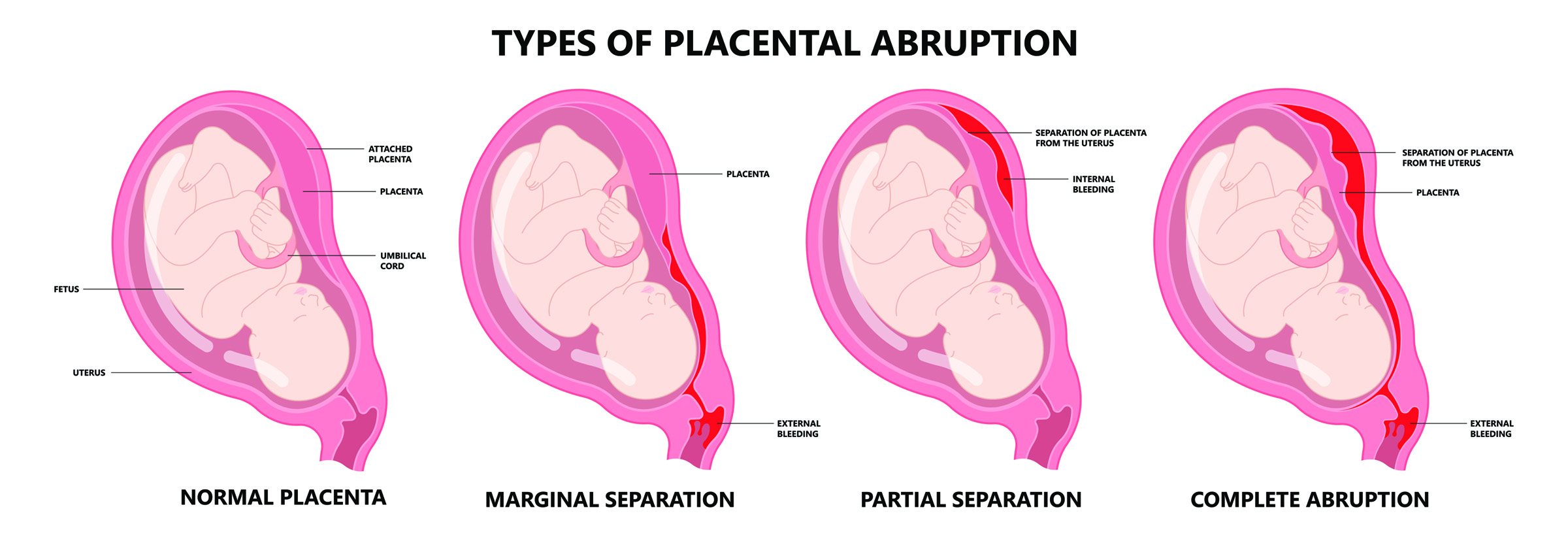
Placental abruption is complete or partial detachment of the placenta after 20 weeks gestation but before delivery of the fetus.
Image 4: Types of Placental Abruption
(*Please click on the image above to enlarge.)
The main findings of placental abruption are (Ananth & Kinzler, 2024):
Bleeding
Abdominal pain
Hypertonic uterine contractions
Uterine tenderness and abnormal fetal heart tracing are also usually seen with placental abruption (Ananth & Kinzler, 2024).
A concealed abruption occurs when blood accumulates behind the placenta (Schmidt et al., 2022). It may not cause obvious bleeding, but the maternal vital signs, including hypotension and/or tachycardia, as well as abnormal lab work may indicate a concealed abruption (Schmidt et al., 2022).
A rupture of maternal vessels tearing away from the placenta is the usual cause of abruption, although rarely the bleeding starts with fetal vessels. Blood accumulates between the uterine wall and placenta. Low pressure hemorrhage generally occurs at the periphery of the placenta, is often called marginal abruption, and can be self-limiting and stabilize. Lighter vaginal bleeding is seen with this type of abruption. A chronic abruption is a light, intermittent bleeding that can lead to fetal growth restriction or oligohydramnios. High pressure hemorrhage generally causes complete or nearly complete separation of the placenta, which can be life-threatening to the mother and fetus (Ananth & Kinzler, 2024).
The risk factors for a placental abruption include(Schmidt et al., 2022):
Previous abruption not caused by trauma
Hypertension
Cocaine use during pregnancy
Smoking
Polyhydramnios
Multiple gestation pregnancy
Preeclampsia
Sudden uterine decompression
Age > 35
Trauma (ex. abdominal trauma)
Placental abruption can cause maternal hemorrhage, disseminated intravascular coagulation (DIC), shock, and death for the mother. The fetus is at risk of preterm delivery, fetal growth restriction, low birth weight, and hypoxemia and asphyxia, which can lead to death (Mayo Clinic Staff, 2022b). A stable woman with a reassuring fetal status may wait for delivery until after 36 weeks and may deliver vaginally. Unstable women need to deliver emergently by c-section, unless a vaginal birth occurs rapidly, which is possible because of excessive contraction (Schmidt et al., 2022). As with the above conditions, this patient is at risk for postpartum hemorrhage. Maternal death and fetal demise can occur, as well as coagulopathy and hysterectomy (Schmidt et al., 2022).
All placental complications can be dangerous for the mother or fetus. The nurse must understand the risks and treatments for each problem. All of these women require close monitoring of maternal and fetal status.
If a nurse is caring for a woman with placenta accreta spectrum, the nurse should be part of any interdisciplinary care planning that takes place concerning this patient. This nurse needs to know that hemorrhage is a serious possibility. Labor and delivery nurses may provide long-term care for a woman with a previa who is hospitalized for antepartum bleeding. Any nurse caring for a severe abruption must be ready for an emergent cesarean section and the possibility of a massive hemorrhage.
It is also important that the nurse remembers the emotional component of caring for these women. Often, the care given may be emergent and focused on saving the mother and fetus. This experience can be overwhelming to the woman and her family. Explaining what is happening to the woman and her family is imperative. Patients with a fetal death or baby in the neonatal intensive care unit (NICU) will need emotional support. A woman with a hysterectomy may suffer additional loss because of her inability to have more children. The experience can be traumatic to everyone involved. Patients who experience traumatic births are at increased risk for postpartum depression.
Natalie is a 22-year-old woman who has had 3 babies, all delivered by cesarean section. She does not have custody of these children because of her history of drug use.
Natalie is currently 32 weeks pregnant. She has had limited prenatal care. She smokes and admits to using cocaine earlier in pregnancy and several times over the last month, including earlier today.
Natalie arrives at your labor and delivery complaining of active, severe, bright red vaginal bleeding and abdominal pain that she rates as a 10/10.
Natalie’s Vitals:
Blood pressure (BP): 100/60
Heart rate (HR): 135
Temperature: 98.6°F
Respiratory rate (RR): 20
Oxygen saturation (SpO2): 95%
Her cervix is 2cm dilated and 20% effaced.
When you put Natalie on the monitor, the fetal heart tracing shows a category 3 tracing with absent variability and recurrent, late decelerations.
What do you think is happening? What are the priorities for Natalie?
Natalie is likely experiencing a placental abruption, given her symptoms and history of drug use. This woman needs an immediate cesarean section to save her life and the life of the fetus. The team caring for the mother needs to be prepared to provide fluids and blood products to replace what has been lost. The team caring for the baby needs to be prepared for a baby that needs full resuscitation. Additionally, this woman and her baby may have drug withdrawal symptoms after delivery that will need to be monitored.
Fortunately, placental complications are relatively rare. With the technology of ultrasound, most serious placental abnormalities are able to be detected before delivery (Rathburn & Hildebrand, 2022). It is essential to consider all of the above potential complications in pregnant women, especially those who exhibit the aforementioned risk factors. With the possibility of hemorrhage being one of the most severe complications, protocols featuring preparedness and a team approach are vital to ensure the safety of both the woman and her child (Rathburn & Hildebrand, 2022).
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
American College of Obstetricians and Gynecologists (ACOG). (2018). Obstetric care consensus no. 7: Placenta accreta spectrum. Obstetrics and Gynecology, 132(6), e259–e275. Visit Source.
Ananth, C.V., & Kinzler, W. L. (2024). Acute placental abruption: Pathophysiology, clinical features, diagnosis, and consequences. UpToDate. Retrieved February 10, 2024. Visit Source.
Anderson-Bagga, F. M., & Sze, A. (2023). Placenta previa. In StatPearls. StatPearls Publishing. Visit Source.
Herrick, E. J., & Bordoni, B. (2023). Embryology, placenta. In StatPearls. StatPearls Publishing. Visit Source.
Lockwood, C. J., & Russo-Stieglitz, K. (2024). Placenta previa: Epidemiology, clinical features, diagnosis, morbidity and mortality. UpToDate. Retrieved February 10, 2024. Visit Source.
Mayo Clinic Staff. (2022a). Placenta: How it works, what is normal. Mayo Clinic. Visit Source.
Mayo Clinic Staff. (2022b) Placental abruption. Mayo Clinic. Visit Source.
Meakin, C., Barrett, E. S., & Aleksunes, L. M. (2022). Extravillous trophoblast migration and invasion: Impact of environmental chemicals and pharmaceuticals. Reproductive Toxicology (Elmsford, N.Y.), 107, 60. Visit Source.
Rathburn, K.M., & Hildebrand, J.P. (2022). Placenta abnormalities. In StatPearls. StatPearls Publishing. Retrieved October 1st, 2024. Visit Source.
Roberts, V., & Myatt, L. (2023). Placental development and physiology. UpToDate. Retrieved February 10, 2024. Visit Source.
Schmidt, P., Skelly, C. L., & Raines, D. A. (2022). Placental abruption. In StatPearls. StatPearls Publishing. Retrieved February 10, 2024. Visit Source.
Silver, R. (2024). Placenta accreta spectrum: Clinical features, diagnosis, and potential consequences. UpToDate. Retrieved February 10, 2024. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.