This course will be updated or discontinued on or before Wednesday, February 23, 2028
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
CEUFast, Inc. is an AOTA Provider of professional development, Course approval ID#9758. This distant learning-independent format is offered at 0.2 CEUs Intermediate, Categories: OT Foundational Knowledge
AOTA does not endorse specific course content, products, or clinical procedures. AOTA provider number 9757.
CEUFast, Inc. (BOC AP#: P10067) is approved by the Board of Certification, Inc. to provide education to Athletic Trainers (ATs).
FPTA Approval: CE25-1175500, CE26-1175500 Accreditation of this course does not necessarily imply the FPTA supports the views of the presenter or the sponsors.
CEUFast, Inc. is recognized by the New York State Education Department's State Board for Physical Therapy as an approved provider of physical therapy and physical therapist assistant continuing education.
Outcomes
≥ 92% of participants will know the seriousness of the disease’s processes, etiology, and how to implement patient care.
Objectives
Following the completion of this continuing education activity, the participant will be able to:
Differentiate between the types and locations of urinary tract infections (UTIs).
Discriminate between uncomplicated and complicated UTIs.
Outline manifestations of a UTI in at-risk populations.
Demonstrate knowledge of ways to prevent UTIs.
Describe testing methods for a UTI.
Recall the most common uropathogenic species.
Assimilate and support the concepts of antimicrobial stewardship into practice.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
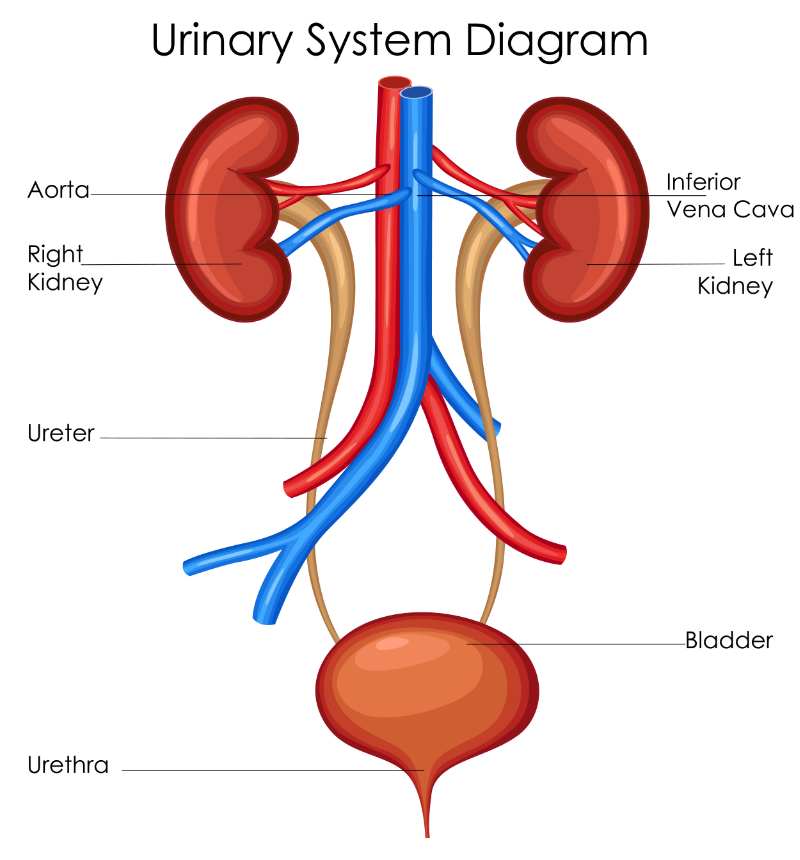
Urinary tract infections (UTIs) are infections that may be located anywhere in the kidneys, ureters, bladder, and/or urethra. The most common uropathogens are Escherichia coli (E. coli), Klebsiella, Staphylococcus saprophyticus (S. saprophyticus), and Proteus mirabilis (P. mirabilis) bacterium. Rarely, UTIs are caused by fungal or viral pathogens. Many of our patients are at risk. Both male and female children are at risk before one year of age, with boys less at risk after this age. Patients with diabetes have UTIs at a greater frequency than non-diabetics. Patients who are recently post-surgery are UTI candidates due to invasive catheterization of the bladder. Universally, women are at the greatest risk for UTI at any age due to normal female anatomy and vaginal sexual intercourse. However, this risk increases after age 40. Men's chances of UTI increase with age as well due to complications connected with the aging prostate. The longer urethra is protective in the younger male, as prostatic involvement is less likely.
Bladder infection or lower UTI is also often referred to as cystitis. Acute pyelonephritis (APN) is the common name for a kidney infection or upper UTI. UTIs can be mild, uncomplicated infections that are easily treated or may be severely complicated and even cause death.
"In the United States, the CDC estimates that UTIs are responsible for nearly 13,000 deaths every year"(Graham et al., 2021, p. 12).
Prevalence worldwide varies; the United States has a lifetime UTI occurrence rate of 12.9%, Europe has a rate of 19.6%, and developing countries have a rate of 24% of the population.
The urinary tract is complex and encompasses the kidneys, ureters, bladder, and urethra. The tract is identical in males and females, except at the urethra, which passes through the prostate in males and is about 14 cm longer. Recurrent or chronic UTIs are possibly preventable, but scientists do not agree on what prevents them. In 2023, how to treat and prevent recurrent UTIs and even the reasons for recurrent UTIs are still controversial due to different populations, medical coverage, empiric antibiotic dosing, and antibiotic resistance.
Adipsia/hypodipsia: A condition whereby a person has no or reduced sensation of thirst.
Antibiotic stewardship: The global effort to keep antimicrobials effective by reasonable practices in prescribing and thoughtful patient education.
Asymptomatic bacteriuria (ASB): A condition where the patient has greater than 100,000 colony-forming units (> 108 colony-forming units [CFU]/L) in a urine sample without signs or symptoms of a UTI.
Clean catch urine sample: A sample of urine taken mid-stream, after handwashing and using antiseptic wipes to clean the areas around the urethra to decrease possible contamination of the sample.
Colony-forming units: The number of microbial cells seen under a microscope in a sample (such as urine) that can multiply into a colony (group) of cells (REVIVE, n.d.).
Colovesical fistula: A pouch formed between the colon and the bladder, allowing leakage of the contents and bacteria of the colon into the bladder (Pollock, 2023).
Commensal: An organism that benefits from living in or on another organism while causing no harm to the host. The organism may cause harm to the host if located in or on the body outside its customary place (Singh & Christina, 2021).
Dyspareunia: Difficult or painful sexual intercourse (Cleveland Clinic, 2024).
Gram-negative: Uropathogens may be E. coli, Proteus species, Pseudomonas aeruginosa (P. aeruginosa), Acinetobacter species, Klebsiella species, Enterobacter species, and Citrobacter species.
Gram-positive: Uropathogens may be S. saprophyticus, Enterococcus species, and coagulase-negative Staphylococci (CoNS). Fungal uropathogens would be Candida albicans (C. albicans). Parasitic and viral causes are rarely seen.
High-powered field (HPF): Generally, the microscopic examination of a pathogen in a sample represents the greatest magnification of 400 times the actual size.
Extended-spectrum beta-lactamases (ESBLs): Organisms that produce enzymes that make them resistant to beta-lactam antibiotics, such as penicillin and cephalosporins.
Sodium-glucose cotransporter-2 (SGLT2) inhibitors: Antidiabetic medications empagliflozin (Jardiance®) and dapagliflozin (Farxiga®) work by causing the kidneys to pull glucose out of the blood and eliminate it in the urine. These drugs also have the effect of increasing urination, lowering blood pressure, and causing UTIs as possible side effects. Serious adverse events such as dehydration, severe UTI, kidney damage, and even gangrenous infection in the genital area (Fournier's gangrene) can be seen.
Urinalysis with reflexive culture and sensitivity (C&S): Following urinalysis, this test is commonly used to evaluate the microbes cultured in agar dishes (or other growth medium) with small discs of antibiotics added. The reason for this test is to determine if the uropathogens(s) will grow close to the discs (resistant) or be repelled by them (sensitive). This test is typically triggered by positive nitrites on a dipstick and protein in the urine.
Urinalysis with reflexive microscopy: Microscopic examination of the sample under HPF to count the CFUs. This is triggered by positive nitrites and white blood cells (WBCs) in the urine.
Uropathogens: Bacteria commonly seen in urinary infections have built-in (genetic) features that can specifically attack the urinary system (Merriam-Webster, n.d.).
Vesicoureteral reflux (VUR): A congenital condition where urine can back up into the ureters and kidneys.
Urinary System Diagram
Table 1. Upper vs. Lower UTI
Feature
Lower UTI
Upper UTI
Location
Bladder and urethra
Kidneys and ureters
Symptoms
Dyspareunia, color, clarity, and odor changes, hematuria, pain with urination, frequent urination, urgency, pain in the lower abdomen or back, and delirium in older adults may be seen.
Fever, chills, nausea and vomiting, color, clarity, and odor changes, hematuria, pain in the lower back and flank
Treatment
Short course of antibiotics, longer in the older adult population, increased fluid intake, and bladder antispasmodics.
May require hospitalization for IV antibiotics if severe. Sepsis possible with delayed treatment.
Women: Due to the shorter urethra of the woman, she is at greater risk globally for an uncomplicated UTI. If pregnant, she is at risk of a complicated UTI. Women who have had select hysterectomies are at greater risk of UTI due to retained urine because of the new prolapsed shape of the bladder.
Men: Due to the longer urethra and the prostatic involvement of the urethra, when a man gets a UTI, it is automatically called a complicated UTI.
Children: A Polish study by Daniel et al. in 2023 showed that children have UTIs at a rate of 9.5% by age seven and about 11% by age 10. Over three years of study and almost a thousand children, fever was often the only noted symptom of a UTI in non-toilet-trained children, and they are harder to diagnose without lab testing. There are many risk factors for UTIs in children (Renko et al., 2022). Fortunately, many children grow out of these problems. One cause of UTI in children is that as many as 3% of infants are born with incompetent vesicoureteral valves, allowing urine to "back up" into the kidneys, causing hydronephrosis and UTIs in up to 20% of these babies and small children (Mattoo et al., 2021). Normally, the pressure of urine in the bladder against these valves prevents urine reflux. Once children are toilet trained, more classic signs of UTI are noted; see Table 1.
"Virtually all authors, including the American Academy of Pediatrics (AAP) and the UK National Institute for Health and Clinical Excellence (NICE), emphasize the importance of rapid antibiotic treatment (of UTI) in the very young to reduce sequelae" (Coulthard, 2019).
E. coli is still the most common infective agent, and girls are more at risk than boys after the first year (due to the protected anatomy of the male). Children two years and under who are born with a congenital anatomical uropathy are more at risk for acute pyelonephritis. UTIs peak at two to three years old, related to potty training. Lower UTIs (cystitis) with E. Coli are the most common uropathogen, causative in 80% of all UTIs in children. E. coli easily proliferates in female bladders. It creates a biofilm around itself and a polysaccharide outer capsule, making the human immune system's workforce less effective at defeating it. In addition, E. coli's biofilm allows it to embed itself into the interstitial cells of the walls of the bladder; this adherence and embedding cause E. coli to be the most effective uropathic microbe among all uropathogens at any age or gender. "It (UTI) is estimated to be the third most common cause of fever in children after gastrointestinal infections and respiratory diseases" (Obeagu, 2023, p. 44).
People with diabetes mellitus: In a retrospective study performed in Thailand, it was shown that patients with type 2 diabetes with an average glycated hemoglobin (HbA1c) result of 8.6 taking the SGLT2 inhibitors empagliflozin (Jardiance®) and dapagliflozin (Farxiga®) were 3.7% more likely to develop a UTI than diabetic patients who did not use these drugs (Uitrakul et al., 2022). The study shows that when a large amount of glucose is present in the urine, UTIs are more likely to occur; this can be seen in people with diabetes with chronically high HbA1c levels because glucose will "spill" into the urine, feeding the bacteria that may be present around the urethra. Based on 15 studies with a sample size of over 800,000 participants in a meta-analysis, the overall prevalence of UTIs in patients with type 2 diabetes was 11.5% (Salari et al., 2022, p.1). Interestingly, the 2022 study by Salari et al. also reports that due to a host of problems such as neuropathy and increased body mass index (BMI), a diabetic patient is 66% more likely to develop asymptomatic urinary tract infection (AUTI) than someone without diabetes.
Incontinence: Wearing disposable incontinence protection can also be linked to increased UTIs. If not changed at once upon urinating, the fluid makes it easier for bacteria to travel by multiplication from the anus to the area of the urethra.
Men over 40 years old: Prostatic involvement causes men to have greater problems as they age. Nagakura et al. (2022) showed that as men get older, problematic testicular hormonal changes occur. It is well-accepted that benign prostatic hypertrophy (BPH) is the cause of retained urine and urinary infections, mostly in men over forty. Smoking, lack of daily exercise, and even weather (likely because of changes in exercise levels) have been reported as related to developing or increasing BPH (Nakagura et al., 2022).
According to Sabih and Leslie (2023), an uncomplicated UTI can be managed on an outpatient basis with oral antibiotics, achieving a normally excellent patient response. Langner et al. (2021) report that UTIs are traditionally treated with fluoroquinolones, which are no longer recommended as first-line treatment and have black box warnings due to the high side effects and adverse effects. However, primary care providers still prescribe fluoroquinolones despite the warnings and antibiotic resistance patterns. ESBLs that are considered responsible for UTIs are exhibiting resistance at an increasing rate (Graham et al., 2021). Fluoroquinolones have not been used as much in the last ten years, though they are still predominant in patients older than 40 years old. This is concerning as the FDA released updated black box warnings for fluoroquinolones that say that older people should not be prescribed them unless they have a serious intractable infection for which all other appropriate antibiotics do not work. Since the Infectious Disease Society of America Clinical Guidelines in 2016-2019 recommended nitrofurantoin, trimethoprim-sulfamethoxazole, and fosfomycin as the first-line treatments for UTI, fluoroquinolone prescribing for UTIs has decreased.
In 2021, it was shown that uncomplicated UTIs appear more often in the summer months when the temperature is 77-86 degrees Fahrenheit or 25-30 degrees Celsius. A well-thought-out study by Simmering et al. (2021) shows a clear increase in UTIs (20-30%) experienced by women in the summer months, with a plateau at temperatures above 86 degrees Fahrenheit or 30 degrees Celsius; this holds true all over the United States. Unfortunately, it was impossible to determine whether the women drank more water and stayed indoors at higher temperatures. In other studies, noted by Simmering et al. (2021), it has been shown that other infections (chlamydia, C. difficile, Legionnaires' disease) are known to increase during specific weather periods, showing that this is not a far-fetched concept. Unsurprisingly, the most popular day to get treatment for a UTI seems to be Monday (Simmering et al., 2021). It's impossible to know the exact day these women's bacteria multiplied to the point of infection status or why this happened. Likely, the UTI becomes noticeable on or before the weekend, and patients are unable to get an appointment until Monday or Tuesday! The authors of this study used fourteen days of weather reports to decide that the UTIs increased when a week of hotter weather followed a substantially lower week of temperatures (Simmering et al., 2021).
Complicated UTIs are those where a patient may incur life-threatening complications such as sepsis, require longer antibiotic courses, and often require additional diagnostic workups. Recurrent UTIs that recur despite adequate antibiotic treatment are considered complicated.
Sabih and Leslie (2023) report that a complex or complicated UTI is labeled as such when the following are factors:
The patient is male.
A broad spectrum of pathogens (including atypical) is involved.
In pregnant females.
Because of kidney stones.
With a colovesical fistula.
In immunocompromised patients.
In older adult patients.
In post-surgical patients with catheters (especially urinary tract surgeries).
In patients with renal transplants.
Table 2: Uncomplicated UTI vs. Complicated UTI Features
Uncomplicated UTI
Complicated UTI
Highest risk in non-pregnant females
Males, pregnant females, age less than 18 or older than 70
In Saudi Arabia, Ahmed et al. (2019) report that antibiotic susceptibility and resistance are changing targets and are not the same in all the studied countries. For instance, Ahmed et al. (2019) state that Europe's numbers are not the same as Saudi Arabia's or the United States' and, in some cases, are diametric opposites. Physicians and prescribing providers must be alert to which microbes are resistant to which antimicrobials in their distinct regions. They must only prescribe the required amount, and waiting for at least the preliminary cultures before prescribing might be more efficacious.
"…inappropriate and non-judicious usage of antibiotics has resulted in the development of worldwide antibiotic resistance in bacteria, leading to the emergence of multi-resistant strains of bacterial pathogens(Ahmed et al., 2019, p. 65)".
In children, where there is an even greater need for speedy microbe identification and efficacy of antimicrobials, Esposito et al. (2022) write,
"However, to limit the emergence of resistance, every effort to reduce and rationalize antibiotic consumption must be made. An increased use of antibiotic stewardship can be greatly effective in this regard" (p.504).
An extensive study by Autore et al. (2023) noted that continuous antibiotic prophylaxis was instituted in the past to prevent recurrent UTIs in children. However, it is now only recommended for a short term until significant urinary blockage can be corrected by surgery. These conclusions are supportive of antibiotic stewardship. Empiric prescribing of antibiotics is a large part of the multidrug resistance found in uropathogens (Goodman et al.,2023). Originally, this method was an attempt to prevent renal scarring and other long-term effects from recurrent UTIs in children, which can be serious. Providers must ask themselves, "Do the benefits of empirical prescribing for UTIs outweigh the risks"?
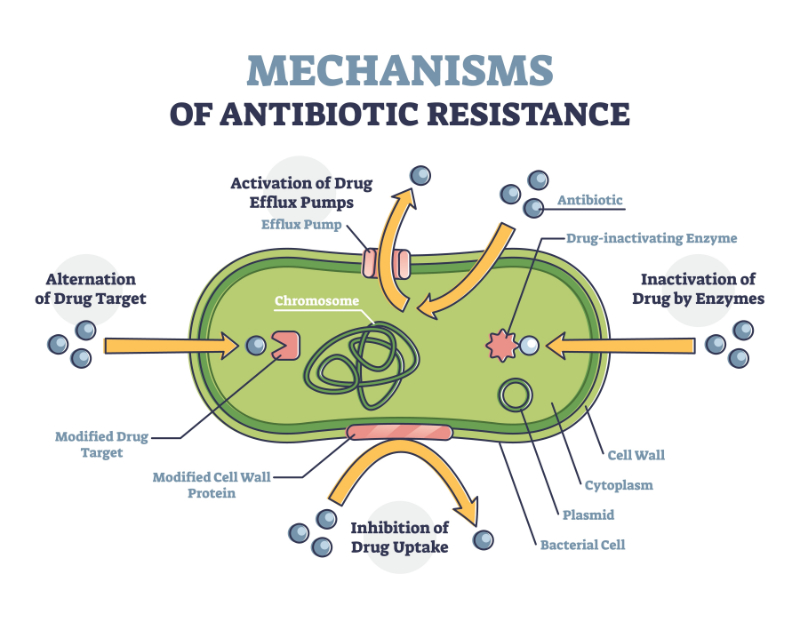
In 1885, when pediatrician Dr. Theodor Escherich was looking for the cause of dysentery in children, he cultured E. coli out of the stool of sick children in Austria. Today, we know of over 700 strains of E. coli due to location and mutation. There are "good" or commensal strains of E. coli in the guts of warm-blooded mammals, including humans and poultry (Wickham Ltd., n.d.). According to Wickham Laboratories (2022) fact sheet, it can live and thrive with or without oxygen and is shed into the environment via stool. Also, E. coli can be contracted by contact, ingestion, and externally. It can defend itself and has developed genetic tools through mutation that can make it antibiotic-resistant. Through mutation, E. coli has developed the power to modify, redirect, and even change antibiotics' targets (Rozwadowski & Gawel, 2022); this is not good for humans, though it is not generally a problem for the carrier animals.
Antibiotic Resistance
"…ampicillin was the least active antimicrobial agent against E. coli, with resistance rates ranging between 50 and 75%… that is why ampicillin is no longer recommended for E. coli infections (Daoud et al., 2020, p.202).
Bioengineers can use E. coli in many beneficial ways; however, we need to know how to control it so that it cannot mutate, nullifying our best antibiotics without killing the "good" E. coli. Through gene editing, scientists are attempting to "create" a strain of E. coli that cannot protect itself and will not interfere with normal human gut biome operations (Wickham Laboratories, n.d.).
Isolating the bacteria and culturing them to find the sensitivity has been occurring since Fleming discovered penicillin in 1928 (Lajiness & Lajiness, 2019). Following urinalysis, C&S is commonly used to test the microbes cultured in agar dishes (or other growth media) with small discs of antibiotics added. Each disc is part of the set of antibiotics currently used in a particular region at each laboratory.
It is not easy to get a good urine sample from children for urinalysis, specifically for C&S. For infants up to potty-trained age, the method to obtain a "clean" sample is to perform suprapubic aspiration (Diviney & Jaswon, 2021; Kaufman et al., 2019). Squeezing a diaper pad or holding a "cleaned" baby over an open cup until it urinates is an ineffective way to get a clean, uncontaminated sample. After potty training, a midstream "clean catch" urine sample is possible.
In most cases, 100,000 CFUs per milliliter signal a UTI. Pyuria thresholds of 3 WBCs per HPF at low urine concentrations, while 8 WBCs per HPF at high urine concentrations in children have the best predictive value for UTI (Coulthard, 2019; Kim et al., 2020; Nadeem et al., 2021).
Positive leukoesterase is a strong predictor of UTI regardless of urine concentration.
This test determines if the uropathogen will grow close to the antibiotic discs (resistant) or be repelled by them (sensitive). A C&S test is typically triggered by a positive automatic dipstick (chemical) urinalysis, positive nitrite, leukoesterase, and WBCs, with subjective positive physical signs and symptoms. More than 3-4 cultured microbes likely indicate contamination or normal urobiome flora. In the absence of signs and symptoms, when an incidental urinalysis is performed and is positive for 100,000 CFU, the patient has ASB. ASB should be screened and treated only in the following people: pregnant women, kidney transplant patients during the first 30 days, and patients currently in endourological procedures such as lithotripsy or implantation of urologic devices such as ureteral stents (Nicolle et al., 2019).
Regarding the chemical testing of a urine specimen, Chambliss et al. (2020) found that, statistically, chemical testing (dipstick) was a good predictor of the need for further urine testing, with only a 6.3% error rate. Claeys et al. (2022) clarified standardized guidelines with a panel of 15 urologists and infectious disease and epidemiological experts. They reported a set of guidelines with changes, such as not automatically getting a urine sample at the medical facility door. They also confirmed the reflexive susceptibility culturing if greater than 10 WBCs are seen on the HPF microscopic examination of the specimen. Homogeneous testing standards support antimicrobial stewardship.
Pregnant women are at an increased risk of UTIs due to normal hormonal increases that occur during pregnancy. Progesterone dilates the uterus, and the progression of the pregnancy causes compression of the ureters by the then heavier uterus. Further, this ureteral compression leads to retained (static) urine, which is then vesicoureteral reflux with ascending bacterial growth. The cascade of expected changes leads to UTIs in roughly 8% of all pregnancies in the United States (Committee on Clinical Consensus—Obstetrics, 2023). As in most other populations, E. coli represents about 85% of all UTI infections; this increased risk is serious enough that there are published guidelines for screening, treating, and re-treating, whether prophylactically or not. The possible serious complications to mother and baby of an untreated or incorrectly treated UTI, upper or lower, are too great to ignore.
While many countries or regions choose different first-line antibiotic therapies, most published guidelines direct five to seven days of treatment for ASB and cystitis. If the infection is pyelonephritis, targeted treatment is to be increased to 14 days; post-treatment screening and prophylaxis are still decided on a case-by-case basis, as there is no unequivocal evidence to make guidelines for this currently. In general, antibiotic choices in the United States for cystitis or ASB are nitrofurantoin and fosfomycin, as resistance to amoxicillin is high here. In Australia, sulfamethoxazole and trimethoprim oral is the first-line treatment for cystitis, and ASB for pyelonephritis or upper UTI treatment is intravenous (IV) gentamicin or gentamicin plus ampicillin. In China and the United Kingdom, oral amoxicillin combined with clavulanate or cephalexin is used first-line. In the United States, fosfomycin is not used for upper UTIs because of the difficulty that the medication has reaching the deeper cells of the kidneys.
Pediatric patients' treatment for mild and uncomplicated cystitis is amoxicillin combined with clavulanate or two to three doses of one of several antibiotics from the second generation of cephalosporins. In targeted cultures, only ciprofloxacin or trimethoprim-sulfamethoxazole may be used. With serious, complicated, febrile UTIs, inpatient IV treatment with the same medications plus added choices of amikacin, gentamicin, and ampicillin combined with ceftazidime for three to four doses is needed. Infants up to three months of age can be empirically treated with three to four doses of IV ampicillin combined with sulbactam and gentamicin. Vancomycin combined with gentamicin can be used for hospital-acquired UTIs in newborns. If there is a further neurologic complication, cefotaxime may be added in three doses (Ramsay et al., 2022).
It should be noted that confusion in older adults can be indicative of a UTI, though not always. Testing for a UTI in a patient who is confused may be difficult. It is not always recommended to test for a UTI if confusion is the only symptom, as it can lead to unnecessary treatment with antibiotics and increased hospitalization and mortality (Pinnell et al., 2021).
It's Friday morning, and you're seeing Sharon Jones. She's a 31-year-old nurse who's been pregnant twice and has two living children. She's had no abortions, no stillbirths, and her last menstrual period was two weeks ago. Today, she is complaining about a three-day bout of frequent burning during urination and strong-smelling urine. She is afebrile, and her heart rate, respiratory rate, and blood pressure are all within normal limits. On examination, she does have tenderness over her lower abdomen centrally. Her abdomen is non-distended, and her bladder is not distended but tender on palpation. She has no costovertebral tenderness to palpation.
As she is being examined, you check her current social history for evidence of multiple sexual partners or even recent sexual activity. She denies these. You can rule out a sexually transmitted infection or an irritated urethra from sexual activity. You know that sometimes if a woman forgets to empty her bladder after vaginal sexual intercourse, uropathic bacteria that have been forced into the end of the urethra will not be flushed out. However, that's not applicable here. You also know that it has been proven that female nurses have higher rates of UTIs compared to other professions (Nerbass et al., 2021); this is due to extended periods of "holding in" their urine and insufficient water during long shifts.
Her clean catch urine sample looks tawny and cloudy. The automatic dipstick urinalysis shows positive results for nitrites and leukoesterase. Because leukoesterase is an enzyme present in WBCs, you know there's an infection under attack in Sharon's body. Plus, nitrates are normal in urine. However, if it's positive for nitrites, gram-negative uropathogens have broken the nitrates down into nitrites. The positive protein of acidic pH and increased urine specific gravity, along with the physical symptoms, show that Sharon has a UTI, probably uncomplicated. You note that Sharon has no drug allergies, and she's not pregnant or breastfeeding. The only medications Sharon takes are lisinopril and a multivitamin daily. The first line of treatment is nitrofurantoin extended release of 100 milligrams orally every 12 hours for five days. You recommend that she take it with food. You also advised her to take her two 15-minute breaks and half-hour lunch breaks to drink water to keep hydrated and take bathroom breaks, flushing out her urinary system.
Although she's a nurse, you still want to provide complete education for prevention and antimicrobial stewardship. You remind her to take all her medicine so she doesn't grow antimicrobial-resistant uropathogens. Recurrent UTIs can be damaging to the kidneys in all populations. You tell Sharon to come back if her symptoms persist and if any new symptoms, such as fever or flank pain, develop. If her uncomplicated UTI becomes a complicated one or continues to persist or recur, a C&S test will be ordered on a new urine sample after the antibiotic is completed. A C&S test will help to target her more resistant uropathogens. You know that antimicrobial resistance has been increasing, and depending on the resistance profile in your area, you might order a C&S anyway.
Sharon reports she will make a more determined effort to drink water at work and to use her break time for herself. Instead of soldiering against all the warnings she knows and has taught others, she will consider her own needs. You electronically send the script for her nitrofurantoin to her pharmacy. You chart the automated urinalysis values, signs and symptoms she is experiencing, vital signs, education performed, and prescriptions. In your note, you added your specific instructions to Sharon to take this medicine with food and to return to the office in the future if needed. You scanned through her problem list and diagnosis codes to see how many urinary infections Sharon has had in the last couple of years, noting that it's been over a year since the last one; you chart this as well. Sharon's uncomplicated lower UTI responds to treatment, and further investigation with diagnostic lab tests is unnecessary.
Preventative antibiotics are not the best plan. Prophylaxis is not used except in select cases, such as patients with long-term indwelling catheters, certain physical manifestations caused by spinal or neurological injuries or illnesses, select pregnant women, and some children.
Humans, in general, must keep fluid hydration constant in the system. Fluid levels are lowered by vomiting, diarrhea, trauma (burns, wounds hemorrhage), adipsia, hypodipsia, mineral imbalance such as hypo/hypernatremia, and finally, hyperglycemia. This is where our excellent teaching skills come into the picture. It has been shown that UTIs are less common when women drink more water regularly. Optimal fluid intake is a controversial subject, and the public has been subjected to mistaken information by well-meaning and sometimes sensationalist medical journalists. Based on a 2018 randomized controlled trial study of 140 premenopausal women by Hooten et al. 2018, it is advised that premenopausal women who increased their fluid intake by 1-1.5 liters per day were less likely to get a UTI. As evidence-based practice regarding hydration is taught in nursing schools, water intake parameters will have to be refined regarding special populations.
Cranberry has been used in America for the last 20 years to prevent UTIs, but does it work? Williams et al. (2023) reported in a 25-year update of the many scientific studies since the original article in 1998 that cranberry juice does not appear to prevent UTIs. As far as treating UTIs, there is no information showing treatment of UTIs with cranberry. Another interesting point is that cranberry supplements of powdered extract are inconsistent in concentration, overall contents, and purity, and cannot be used in medical studies under these circumstances. Guaranteed pure medical-grade cranberry extract powder would not be available to the public, even if made for the studies. Cranberry (Vaccinium macrocarpon) is high in oxalates, antioxidants, and Vitamin C. It has proanthocyanidin (PAC), which is known to cause uropathogens such as E. coli, P. aeruginosa, and P. mirabilis to be unable to attach to the bladder wall (Williams et al., 2023). Cranberry has little to no side effects unless taken in high doses. According to the FDA, as a dietary supplement, it is considered safe (Madden et al., 2021; Valente et al., 2022).
Saw palmetto (Serenoa repens) is used to reduce the volume of the prostate to decrease urine retention and, therefore, UTIs. Two studies showed that the quality and purity of the liposterolic content of the saw palmetto berry extract make the product work to decrease the prostate's volume. However, finding a quality product with the expected therapeutic amount of lipidosterolic 80% or more is the problem. However, the saw palmetto is generally well tolerated and may be taken prophylactically for many years without issue (Nickel et al., 2022; Chughtai et al., 2023).
D-mannose is increasingly being studied in the prevention and treatment of UTIs. Some studies show that it inhibits E. coli’s ability to adhere to the wall of the bladder. Researchers are also finding that treatment efficacy is comparable to the use of antibiotics (Wagenlehner et al., 2022). More research is necessary to determine the true efficacy, as the results of the use of this supplement are mixed.
Men should urinate following all penetrating intercourse. Men older than 40 should exercise daily, avoid excessive alcohol intake, and not smoke, as these are associated with increased prostate volume, which leads to urinary retention and ultimately to increased numbers of UTIs. Men should try to empty the bladder when urinating completely.
Following penetrative vaginal intercourse, all women should urinate. Women should urinate as often as once every two hours while awake. After going to the bathroom, women should wipe from front to back. Wearing loose-fitting lower-body clothing and cotton underwear are all accepted preventative practices, although not always followed (Mangai et al., 2019). Men should try to empty their bladder completely when urinating.
For infants, change diapers as soon as they get wet to prevent microbes from traveling from the anus to the urethra. Potty-trained children should be encouraged to drink water regularly. They should be taught to wipe correctly after going to the bathroom or assist if needed to prevent contamination of the urethra.
Those who are incontinent should not remain in wet disposable briefs. Dementia patients who can ambulate should be on a bathroom schedule and, if needed, helped with wiping. Patients who are paralyzed, bedfast, or otherwise unable to use the toilet safely and cleanly should be aided on a schedule to stay clean and dry.
It has been found that the application of low-dose estrogen cream vaginally significantly reduces the occurrence of UTIs in postmenopausal women. It has been shown to moderate the inflammatory profile, leading to a decrease in symptoms (Meister et al., 2021). More research is necessary to determine if more prophylactic therapies are applicable.
Speed is the thing. The old methods are cheap but much too slow to prevent blind, empiric prescribing. Interestingly, in 2022, Webber et al. showed that the antibiotic discs could be put onto the Petri dishes at the start of the culture process. It costs no more and provides accurate susceptibility results 18 hours sooner than waiting until after the culture has matured. The results can be quantified as early as six hours after the antibiotic discs are applied. This method can also be read by automation; this would lead to specific antibiotic prescriptions within six hours. The plan supports antibiotic stewardship and the patient's need for the right antibiotics. However, many levels of acceptance and change are required for the world to switch to a new "old" method after more than 50 years. Modern alternatives to C&S are on the way. Polymerase chain reactions can now evaluate which specific microbes are in the urine much faster than culture on agar-coated Petri dishes. Fast, automated microfluid testing combined with special optical and biomarker science is available and is in further development (Salam et al., 2023). Eventually, scientists can quickly check a specific microbe's DNA for surface antigens and peculiarities that infer resistance to antimicrobials. Between cost, speed, size, regulatory hurdles, and habits, global acceptance and use of faster methods is the dream—a medical diagnostic kumbaya, so to speak.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Ahmed, S. S., Shariq, A., Alsalloom, A. A., Babikir, I. H., & Alhomoud, B. N. (2019). Uropathogens and their antimicrobial resistance patterns: Relationship with urinary tract infections. International Journal of Health Sciences, 13(2), 48. Visit Source.
Autore, G., Bernardi, L., Ghidini, F., La Scola, C., Berardi, A., Biasucci, G., Marchetti, F., Pasini, A., Capra, M. E., Castellini, C., Cioni, V., Cantatore, S., Cella, A., Cusenza, F., De Fanti, A., Della Casa Muttini, E., Di Costanzo, M., Dozza, A., Gatti, C., Malaventura, C., … The Uti-Ped-Er Study Group (2023). Antibiotic Prophylaxis for the Prevention of Urinary Tract Infections in Children: Guideline and Recommendations from the Emilia-Romagna Pediatric Urinary Tract Infections (UTI-Ped-ER) Study Group. Antibiotics (Basel, Switzerland), 12(6), 1040. Visit Source.
Bono, M. J., Leslie, S. W., & Reygaert, W. C. (2023). Uncomplicated Urinary Tract Infections. In: StatPearls [Internet]. StatPearls Publishing. Visit Source.
Chambliss, A. B., Mason, H. M., & Van, T. T. (2020). Correlation of Chemical Urinalysis to Microscopic Urinalysis and Urine Culture: Implications for Reflex Urinalysis Workflows. The journal of applied laboratory medicine, 5(4), 724–731. Visit Source.
Chughtai, B., Bhojani, N., Zorn, K. C., & Elterman, D. (2023). Variability of Commercial Saw Palmetto–Based Supplements for the Management of Benign Prostatic Hyperplasia/Lower Urinary Tract Symptoms. JU Open Plus, 1(8), e00037. Visit Source.
Claeys, K. C., Trautner, B. W., Leekha, S., Coffey, K. C., Crnich, C. J., Diekema, D. J., Fakih, M. G., Goetz, M. B., Gupta, K., Jones, M. M., Leykum, L., Liang, S. Y., Pineles, L., Pleiss, A., Spivak, E. S., Suda, K. J., Taylor, J. M., Rhee, C., & Morgan, D. J. (2022). Optimal Urine Culture Diagnostic Stewardship Practice-Results from an Expert Modified-Delphi Procedure. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 75(3), 382–389. Visit Source.
Committee on Clinical Consensus—Obstetrics. (2023). Urinary Tract Infections in Pregnant Individuals. The American College of Obstetricians and Gynecologists. Visit Source.
Coulthard, M. G. (2019). Defining urinary tract infection by bacterial colony counts: a case for 100,000 colonies/ml as the best threshold. Pediatric nephrology (Berlin, Germany), 34(10), 1639–1649. Visit Source.
Daniel, M., Szymanik-Grzelak, H., Sierdziński, J., Podsiadły, E., Kowalewska-Młot, M., & Pańczyk-Tomaszewska, M. (2023). Epidemiology and Risk Factors of UTIs in Children-A Single-Center Observation. Journal of personalized medicine, 13(1), 138. Visit Source.
Daoud, N., Hamdoun, M., Hannachi, H., Gharsallah, C., Mallekh, W., & Bahri, O. (2020). Antimicrobial Susceptibility Patterns of Escherichia coli among Tunisian Outpatients with Community-Acquired Urinary Tract Infection (2012-2018). Current urology, 14(4), 200–205. Visit Source.
Diviney, J., & Jaswon, M. S. (2021). Urine collection methods and dipstick testing in non-toilet-trained children. Pediatric nephrology (Berlin, Germany), 36(7), 1697–1708. Visit Source.
Esposito, S., Biasucci, G., Pasini, A., Predieri, B., Vergine, G., Crisafi, A., Malaventura, C., Casadio, L., Sella, M., Pierantoni, L., Gatti, C., Paglialonga, L., Sodini, C., La Scola, C., Bernardi, L., Autore, G., Canto, G. D., Argentiero, A., Cantatore, S., Ceccoli, M., … Iughetti, L. (2022). Antibiotic Resistance in Paediatric Febrile Urinary Tract Infections. Journal of global antimicrobial resistance, 29, 499–506. Visit Source.
Goodman, K. E., Baghdadi, J. D., Magder, L. S., Heil, E. L., Sutherland, M., Dillon, R., Puzniak, L., Tamma, P. D., & Harris, A. D. (2023). Patterns, Predictors, and Intercenter Variability in Empiric Gram-Negative Antibiotic Use Across 928 United States Hospitals. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 76(3), e1224–e1235. Visit Source.
Graham, J. P., Amato, H. K., Mendizabal-Cabrera, R., Alvarez, D., & Ramay, B. M. (2021). Waterborne Urinary Tract Infections: Have We Overlooked an Important Source of Exposure?. The American journal of tropical medicine and hygiene, 105(1), 12–17. Visit Source.
Kaufman, J., Temple-Smith, M., & Sanci, L. (2019). Urinary tract infections in children: an overview of diagnosis and management. BMJ paediatrics open, 3(1), e000487. Visit Source.
Kim, D., Pantanowitz, L., Schüffler, P., Yarlagadda, D. V. K., Ardon, O., Reuter, V. E., Hameed, M., Klimstra, D. S., & Hanna, M. G. (2020). (Re) Defining the High-Power Field for Digital Pathology. Journal of pathology informatics, 11, 33. Visit Source.
Lajiness, R., & Lajiness, M. J. (2019). 50 Years of Urinary Tract Infections and Treatments - Has Much Changed? Urologic Nursing, 39(5), 235. Visit Source.
Langner, J. L., Chiang, K. F., & Stafford, R. S. (2021). Current prescribing practices and guideline concordance for the treatment of uncomplicated urinary tract infections in women. American journal of obstetrics and gynecology, 225(3), 272.e1–272.e11. Visit Source.
Madden, E., McLachlan, C., Oketch-Rabah, H., & Calderón, A. I. (2021). Safety of Cranberry: Evaluation of Evidence of Kidney Stone Formation and Botanical Drug-Interactions. Planta medica, 87(10-11), 803–817. Visit Source.
Mangai, J. M., Bongji, G., Kopdima, G., Udeh, P., Patienceringkat, K., Nadyen, S., Jidauna, D., & Salome, D. (2019). Assessment of knowledge and prevention practices of urinary tract infection (UTI) among female students residence in university of Jos. International Research Journal of Public and Environmental Health, 6(5), 89-96. Visit Source.
Mattoo, T. K., Shaikh, N., & Nelson, C. P. (2021). Contemporary Management of Urinary Tract Infection in Children. Pediatrics, 147(2), e2020012138. Visit Source.
Meister, M. R., Wang, C., Lowder, J. L., & Mysorekar, I. U. (2021). Vaginal Estrogen Therapy Is Associated With Decreased Inflammatory Response in Postmenopausal Women With Recurrent Urinary Tract Infections. Female pelvic medicine & reconstructive surgery, 27(1), e39–e44. Visit Source.
Merriam-Webster. (n.d.). Uropathogenic. In Merriam-Webster.com medical dictionary. Visit Source.
Nadeem, S., Badawy, M., Oke, O. K., Filkins, L. M., Park, J. Y., & Hennes, H. M. (2021). Pyuria and Urine Concentration for Identifying Urinary Tract Infection in Young Children. Pediatrics, 147(2), e2020014068. Visit Source.
Nagakura, Y., Hayashi, M., & Kajioka, S. (2022). Lifestyle habits to prevent the development of benign prostatic hyperplasia: Analysis of Japanese nationwide datasets. Prostate international, 10(4), 200–206. Visit Source.
Nerbass, F. B., Santo, C. E., Fialek, E. V., Calice-Silva, V., & Vieira, M. A. (2021). Female nurses have a higher prevalence of urinary tract symptoms and infection than other occupations in dialysis units. Jornal brasileiro de nefrologia, 43(4), 495–501. Visit Source.
Nickel, J. C., Chughtai, B., De Nunzio, C., Brahmbhatt, J., Shore, N., Te, A. E., & Djavan, B. (2022). Rethinking the Role of Saw Palmetto Extract for Men with Lower Urinary Tract Symptoms in North America. Uro, 2(3), 137–150. Visit Source.
Nicolle, L. E., Gupta, K., Bradley, S. F., Colgan, R., DeMuri, G. P., Drekonja, D., Eckert, L. O., Geerlings, S. E., Köves, B., Hooton, T. M., Juthani-Mehta, M., Knight, S. L., Saint, S., Schaeffer, A. J., Trautner, B., Wullt, B., & Siemieniuk, R. (2019). Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria: 2019 Update by the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 68(10), e83–e110. Visit Source.
Obeagu, E. I. (2023). An update on urinary tract infection in Children less than Five Years. Newport International Journal of Research in Medical sciences, 3(2), 44-46. Visit Source.
Pinnell, R. A. M., Ramsay, T., Wang, H., & Joo, P. (2021). Urinary Tract Infection Investigation and Treatment in Older Adults Presenting to the Emergency Department with Confusion: a Health Record Review of Local Practice Patterns. Canadian geriatrics journal : CGJ, 24(4), 341–350. Visit Source.
Pollock, D. M. (2023). What to know about colovesical fistula. Medical News Today. Visit Source.
Ramsay, J. A., Mascaro, S., Campbell, A. J., Foley, D. A., Mace, A. O., Ingram, P., Borland, M. L., Blyth, C. C., Larkins, N. G., Robertson, T., Williams, P. C. M., Snelling, T. L., & Wu, Y. (2022). Urinary tract infections in children: building a causal model-based decision support tool for diagnosis with domain knowledge and prospective data. BMC medical research methodology, 22(1), 218. Visit Source.
Renko, M., Salo, J., Ekstrand, M., Pokka, T., Pieviläinen, O., Uhari, M., & Tapiainen, T. (2022). Meta-analysis of the Risk Factors for Urinary Tract Infection in Children. The Pediatric infectious disease journal, 41(10), 787–792. Visit Source.
REVIVE. (n.d.). Colony-forming unit (CFU). Global Antibiotic Research and Development Partnership. Visit Source.
Rozwadowski, M., & Gawel, D. (2022). Molecular Factors and Mechanisms Driving Multidrug Resistance in Uropathogenic Escherichia coli-An Update. Genes, 13(8), 1397. Visit Source.
Sabih, A., & Leslie, S. W. (2023). Complicated Urinary Tract Infections. In: StatPearls [Internet]. StatPearls Publishing. Visit Source.
Salam, M. A., Al-Amin, M. Y., Pawar, J. S., Akhter, N., & Lucy, I. B. (2023). Conventional methods and future trends in antimicrobial susceptibility testing. Saudi journal of biological sciences, 30(3), 103582. Visit Source.
Salari, N., Karami, M. M., Bokaee, S., Chaleshgar, M., Shohaimi, S., Akbari, H., & Mohammadi, M. (2022). The prevalence of urinary tract infections in type 2 diabetic patients: a systematic review and meta-analysis. European journal of medical research, 27(1), 20. Visit Source.
Simmering, J. E., Polgreen, L. A., Cavanaugh, J. E., Erickson, B. A., Suneja, M., & Polgreen, P. M. (2021). Warmer Weather and the Risk of Urinary Tract Infections in Women. The Journal of urology, 205(2), 500–506. Visit Source.
Singh, B., & Christina, E. (2021). Bacterial metabolites: an unexplored quarry. Volatiles and Metabolites of Microbes, 205–234. Visit Source.
Uitrakul, S., Aksonnam, K., Srivichai, P., Wicheannarat, S., & Incomenoy, S. (2022). The Incidence and Risk Factors of Urinary Tract Infection in Patients with Type 2 Diabetes Mellitus Using SGLT2 Inhibitors: A Real-World Observational Study. Medicines (Basel, Switzerland), 9(12), 59. Visit Source.
Valente, J., Pendry, B. A., & Galante, E. (2022). Cranberry (Vaccinium macrocarpon) as a prophylaxis for urinary tract infections in women: A systematic review with meta-analysis. Journal of Herbal Medicine, 36, 100602. Visit Source.
Wagenlehner, F., Lorenz, H., Ewald, O., & Gerke, P. (2022). Why d-Mannose May Be as Efficient as Antibiotics in the Treatment of Acute Uncomplicated Lower Urinary Tract Infections-Preliminary Considerations and Conclusions from a Non-Interventional Study. Antibiotics (Basel, Switzerland), 11(3), 314. Visit Source.
Webber, D. M., Wallace, M. A., & Burnham, C. D. (2022). Stop Waiting for Tomorrow: Disk Diffusion Performed on Early Growth Is an Accurate Method for Antimicrobial Susceptibility Testing with Reduced Turnaround Time. Journal of clinical microbiology, 60(5), e0300720. Visit Source.
Williams, G., Hahn, D., Stephens, J. H., Craig, J. C., & Hodson, E. M. (2023). Cranberries for preventing urinary tract infections. The Cochrane database of systematic reviews, 4(4), CD001321. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.