This course will be updated or discontinued on or before Sunday, March 26, 2028
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥92% of participants will know the stages of pressure injuries, risk factors, and interventions to prevent pressure injuries in the perioperative setting.
Objectives
After completing this continuing education course, the participant will be able to:
Categorize the different stages of pressure injuries.
Outline items that are necessary when performing a wound assessment.
Identify at least two pressure injury risk assessment screening tools used in a perioperative setting.
Examine at least three interventions regarding pressure injury prevention.
Identify at least two complications of pressure injuries.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
According to the Agency for Healthcare Research and Quality, more than 2.5 million Americans develop pressure injuries annually (Agency for Healthcare Research and Quality [AHRQ], 2024). In certain healthcare settings, pressure injuries are more common due to prolonged periods of immobility, such as in long-term care facilities or hospital intensive care units (Mervis & Phillips, 2019). However, they can also occur in the perioperative setting due to prolonged immobility and the patient’s inability to reposition themselves from being sedated or under anesthesia.
There are several measures that healthcare providers can take to prevent pressure injuries from occurring in a perioperative setting. Healthcare providers must understand the implications of pressure ulcers, risk factors, and interventions to prevent pressure injuries from occurring. In this course, you will learn about the different stages of pressure injuries and individual risk factors (both intrinsic and extrinsic) that can contribute to their development. This course will also review perioperative pressure ulcer screening tools, preventative interventions, and potential complications of pressure injuries.
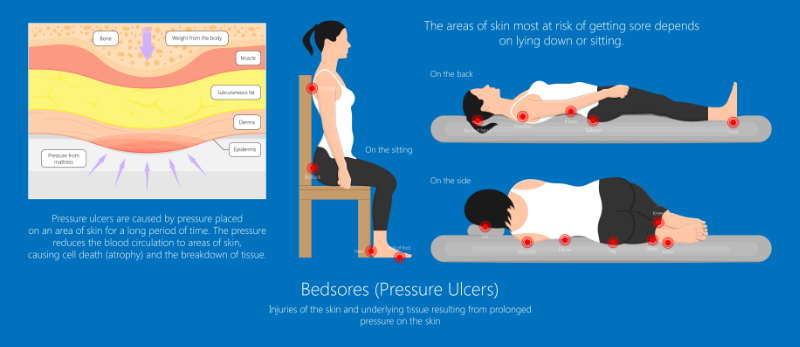
Pressure injuries, also called pressure ulcers, occur when there is prolonged pressure on an area of the body, causing localized damage to the skin and underlying soft tissue. This is usually due to an individual’s body weight causing pressure on an area, but it can also occur from medical devices and equipment (Mondragon & Zito, 2022). Pressure injuries typically develop over a bony prominence, such as the sacrum, heels, or greater trochanter (Al Aboud & Manna, 2023). Pressure injuries are sometimes called bedsores, pressure sores, or decubitus ulcers.
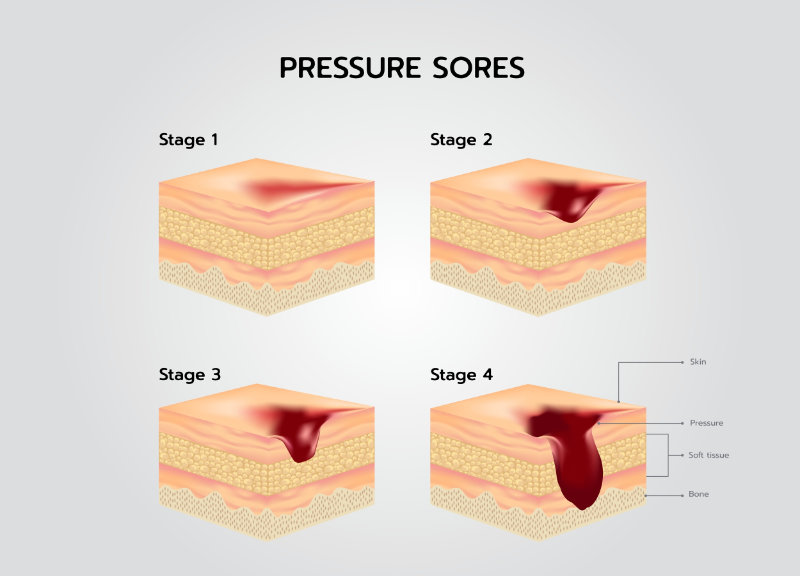
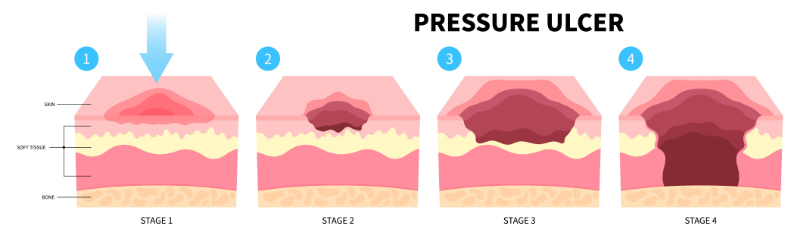
Pressure ulcers are typically classified or staged based on the depth of the skin injury, ranging from stages 1 to 4. In addition to the four stages, some pressure injuries are considered unstageable or deep tissue injuries. The 4th edition of the International Pressure Ulcer/Injury Guidelines is still being developed, therefore, the 2019 edition is still the currently utilized Clinical Practice Guideline. This CPG was developed by a consortium of the National Pressure Injury Advisory Panel (NPIAP), the European Pressure Ulcer Advisory Panel (EPUAP), and the Pan Pacific Pressure Injury Alliance (PPPIA). (EPUAP et al., 2019). This most recent version includes an updated review of the research literature and recommendations that reflect the latest evidence. It provides a detailed analysis and discussion of available research, recommendations for clinical practice, good-practice statements, implementation considerations, a description of the methodology used to develop the guidelines, and acknowledgements of the many experts who were formally involved in the development process. The following details are the staging system for pressure-related injuries from the International Guidelines (EPUAP et al., 2019).
Stage 1 pressure injuries are a non-blanchable area of erythema where the skin is intact. A non-blanchable area is where the skin is pressed, usually with a fingertip, and does not turn white (EPUAP et al., 2019). Furthermore, the area should remain red for more than one hour after pressure is relieved to be considered a stage 1 pressure injury(Mondragon & Zito, 2022).
Stage 2 pressure injuries are considered partial thickness. The skin is not intact, the dermis is exposed, and there is an open wound bed. The wound bed can appear pink to red and moist, without visible fat or deeper tissues. Some stage 2 pressure injuries will initially have a blister without an open wound bed(EPUAP et al., 2019).
Stage 3 pressure injuries are full-thickness skin loss. Fat tissue, also called adipose tissue, and granulation tissue will be visible. Sometimes, slough, which appears like a yellowish stringy material over the wound bed, may be present. Undermining or tunneling may be present. Some stage 3 pressure injuries may also have an eschar, which is dry, dead tissue that is usually black and firm. However, if an eschar or slough is present, the healthcare provider should still be able to see portions of the underlying wound bed for it to be considered a stage 3 pressure injury. Many stage 3 pressure ulcers will tunnel or undermine. Another key feature is no exposed ligaments, muscles, tendons, or bones (EPUAP et al., 2019).
Stage 4 pressure injuries are full-thickness skin loss and tissue loss. A distinguishing feature of a stage 4 pressure ulcer is that there will be visible, exposed muscle, fascia, tendons, ligaments, bone, or cartilage. Again, wound undermining is common, and slough or eschar may be present, but the underlying wound bed will still be visible (EPUAP et al., 2019).
It's considered unstageable when slough or eschar completely covers the wound bed. The pressure injury can be appropriately staged once the slough or eschar is removed(EPUAP et al., 2019).
Deep tissue injuries (DTIs) are where the skin is non-blanchable but will be purple or maroon in color. A key difference between a stage 1 and deep tissue injury is that a stage 1 pressure ulcer has red or erythematous skin, while a DTI does not(Mondragon & Zito, 2022).
A skin inspection should be a high priority whenever there is a change in the level of care or the staff caring for the patient. Many healthcare organizations require a documented skin assessment at every shift change or change in care. Furthermore, the perioperative healthcare professional should collaborate and perform a skin assessment before, during, and after any procedure completed in the operating room. The perioperative care team includes preoperative (Pre-Op), post-anesthesia care unit (PACU), operating room, and circulating nurses.
The nurse should inspect the skin for erythema and pay particular attention to areas of bony prominence and where medical devices and equipment overly the skin. If any prophylactic dressings are present, they should be inspected underneath. Additionally, the nurse should assess the patient for pain, even if the patient is non-verbal, sedated, or altered. The nurse can utilize the pain scale that correctly corresponds to the patient’s level of consciousness. Examples may include the Behavioral Pain Scale (BPS), Critical Care Pain Observation Tool (CPOT), Numerical Rating Scale (NRS), and Visual Analog Scale (VAS). Healthcare organizations often provide guidance on which pain scale to use in each setting and required documentation parameters (EPUAP et al., 2019).
If a pressure injury is suspected or present, the nurse should complete a thorough assessment and documentation of the area. When there is an erythema area, the nurse should inspect if the skin is blanchable. The nurse may use the finger pressure method, where they press their finger to the area of erythema for three seconds and then release, or the transparent disk method, where a transparent disk is applied over the area, and blanching is observed through the disk. A pressure injury is confirmed if the erythematous area is non-blanchable (EPUAP et al., 2019).
The nurse should also assess and document the pressure injury location, length, width, and depth. Wound measurements are typically taken in centimeters (cm), but this depends on the healthcare organization’s policies. The nurse should also document if there is any undermining, tunneling, or necrosis. Undermining of the skin is when a pocket of dead tissue or space is under the healthy skin tissue. Additionally, the nurse should assess the wound for signs of infection, such as erythema, warmth, odor, drainage, and tenderness or pain with palpation (Mondragon & Zito, 2022).
The nurse should inspect the area for any moisture, edema, or change in tissue consistency to the affected and surrounding areas. When performing a skin assessment, the patient’s skin tone should also be considered, as it’s sometimes more challenging to detect pressure injuries on people with darkly pigmented skin or areas. Using adjunct assessment strategies, like assessing skin temperature, moisture, and a color chart, is beneficial (EPUAP et al., 2019).
Other portions of proper wound assessment and documentation use risk assessment tools and review major risk factors (EPUAP et al., 2019). Common risk assessment tools utilized in a perioperative setting and risk factors are detailed below. Nurses need to understand that all areas of skin breakdown are not pressure injuries. Furthermore, if a pressure injury is suspected or identified, the nurse should immediately notify the healthcare provider and follow the facility’s protocols and procedures. This often involves wound care and infectious disease consultation. These specialized healthcare professionals can help determine if the area of skin breakdown is a pressure-related injury or from another cause, like a skin tear or venous ulcer (Association of Perioperative Registered Nurses [AORN], 2023).
Nurses should strive to use pressure injury risk assessment tools and screenings for every patient that enters the perioperative setting, which includes the preoperative, intraoperative, and postoperative periods. These tools aid with a structured approach to assessing a patient’s likelihood of developing a pressure ulcer. Risk assessment tools do not replace a comprehensive skin assessment and should be used with clinical judgment (AORN, 2023). Furthermore, selecting which assessment tool to utilize usually depends on the healthcare setting and the facility’s policies. The Braden, Norton, and Waterlow scales are common pressure injury risk assessment tools used throughout healthcare facilities, regardless of the unit or setting (EPUAP et al., 2019). However, the Association of Perioperative Registered Nurses (AORN) does not recommend using these risk assessment tools since they do not specifically address surgical patients (AORN, 2023).
Risk assessment tools specific to the perioperative room setting include the Munro Pressure Ulcer Risk Assessment Scale for Perioperative Patients, Risk Assessment Scale for the Development of Injuries due to Surgical Positioning (ELPO), Perioperative Risk Assessment Measure for Skin (PRAMS), and Scott Triggers Tool (AORN, 2023).
Although the Braden scale is not widely used during the perioperative period, its total score is used as a component in other assessment tools, like the PRAMS. Additionally, some healthcare organizations require routinely documented Braden scores regardless of the unit. The Braden scale screens for six factors: moisture, sensory perception, activity, mobility, nutritional status, and friction and shear. Patient scores range from 6 to 23; the lower the score, the higher the risk of developing a pressure injury (Al Aboud & Manna, 2023).
The Munro Scale predicts the risk of pressure injuries developing in patients under general anesthesia. It’s one of the only screening tools that can be used throughout the perioperative period and is further broken down by the perioperative period. The preoperative period evaluates six factors: mobility, body mass index (BMI), age, length of nothing by mouth (NPO), weight loss in the last 30 to 180 days, and certain comorbidities. Points are assigned for each category, and patients with a score of 6 or lower are considered at low risk of developing a pressure injury. Patients with a total score between 7 and 14 are at moderate risk, and those with a score of 15 or higher are at high risk (Lei et al., 2022).
Intraoperative nurses use the Munro scale to evaluate seven factors, which include the American Society of Anesthesiologists (ASA) Physical Status Classification, type of anesthesia, body temperature, hypotension, moisture, patient position, and surface and motion. The ASA classification score is obtained from the anesthesiologist. Nurses add the preoperative to the intraoperative Munro score for a cumulative total. Patients with scores of 13 or less are low risk, between 14 and 24 are moderate risk, and 25 or greater are high risk (Lei et al., 2022).
Lastly, PACU nurses will evaluate two risk factors: blood loss and length of the perioperative duration. The length of the perioperative duration is when the patient arrives in the preoperative unit to the departure from the postoperative unit. The nurse totals the preoperative, intraoperative, and postoperative scores for a final total score. Patient scores of 15 or less are low risk, from 16 to 28 are moderate, and 29 or greater are high risk (Lei et al., 2022).
The ELPO scale evaluates the risk of developing a pressure injury. It is based on components such as surgical position, surgery duration, type of anesthesia, support surface, limb positioning, patient comorbidities, and age. Total scores range from 7 to 35, and risk increases with higher scores (Peixoto et al., 2019).
The PRAMS scale evaluates the potential risk of developing a pressure injury using factors such as whether the patient has diabetes, patient age, prior surgeries during the current hospital admission, Braden score, preexisting pressure ulcers, and scheduled length of surgery (Spruce, 2023).
The Scott Triggers Tool evaluates a patient’s risk by accounting for factors such as age, serum albumin, estimated length of surgery, and the ASA Physical Status Classification. Surgical patients are considered high risk for scores of two or more, and nurses should implement pressure injury precautions (Spruce, 2023).
There are several risk factors for developing pressure injuries during the perioperative setting, including intrinsic and extrinsic factors. Perioperative nurses should evaluate intrinsic and extrinsic factors when assessing a patient’s pressure injury risk (AORN, 2022a).
Intrinsic factors are factors involving the patient’s characteristics and health status. Some intrinsic factors include:
Presence of infection
High lactate levels
High C-reactive protein levels
Low albumin levels
Low hemoglobin levels
Low hematocrit levels
Diastolic blood pressure less than 60 mmHg
Hypotensive episodes
High ASA physical status classification
Poor skin turgor (AORN, 2022a; EPUAP et al., 2019)
Additionally, patients with an underweight or overweight BMI may develop injuries due to friction, shear, and pressure over bony prominences. Weight loss of 10% or more within the 30 to 180 days before surgery significantly increases risk (Lei et al., 2022). Other independent, significant risk factors are patients who are biologically female sex and above the age of 60 (Peixoto et al., 2019). The patient’s nutritional status is important as those with malnutrition are at increased risk for pressure injuries. Insufficient calories, fluids, protein, and vitamin C can lead to potential pressure injuries, as these are required for tissue metabolism (Al Aboud & Manna, 2023). Patients with urinary and fecal incontinence are also at increased risk due to skin moisture issues(Sengul & Gul, 2022a).
Pressure injury risk also increases with certain medical conditions or comorbidities, which include peripheral vascular disease, diabetes mellitus, cancer, and cardiovascular disease. Patients who are former or current smokers, who have a history of postoperative urinary tract infections, and who have a current or previous pressure injury are at increased risk (Sengul & Gul, 2022; AORN, 2022a). Hypertension, prehypertension, and respiratory diseases like asthma increase the likelihood (Lei et al., 2022). Additional risk factors are patients with spinal cord injuries, chronic neurological conditions, prolonged immobility, or problems with sensory perception (EPUAP et al., 2019).
Extrinsic factors are those outside of the patient but still affect the body. Some extrinsic factors include:
Blood loss during the procedure
Vasopressor use
Hypothermia
Hypotension
Cardiopulmonary bypass use
Temperature of the operating room
General anesthesia use (AORN, 2022a; EPUAP et al., 2019)
Additionally, prolonged procedure time (expected and unexpected) greater than 2 hours in the operating room increases the risk of pressure injuries. Factors such as pressure, moisture, heat, friction, and shear forces also affect the likelihood of pressure injury. Using devices for positioning and the type of table mattress can affect the development of pressure injuries. The type of surgery can increase the chances of developing a pressure injury. Surgeries involving the spine, abdominal, and heart increase a patient’s risk. As many neurological and cardiac surgeries last for several hours and affect tissue perfusion, this may also be a factor for increased pressure injury risk (AORN, 2022a; EPUAP et al., 2019). Vascular operations, such as major amputations and lower extremity bypasses, may also increase risk (Ahmad et al., 2023).
Patient positioning during the procedure is important in pressure injury prevention. Depending on the position the patient is placed in during surgery, certain areas are at increased risk. Additional information about specific pressure points for surgical positions is discussed in more detail later in this course (AORN, 2022a; EPUAP et al., 2019). The prone and Trendelenburg positions have also increased the risk of postoperative vision loss due to pressure on the orbital area during surgery (AORN, 2022b).
In addition to identifying patient risk factors, performing a comprehensive skin assessment, and utilizing pressure injury risk screening tools, perioperative nurses should also complete several interventions to protect against pressure injuries. The following discusses interventions perioperative nurses can take to prevent pressure injuries from occurring.
As discussed, positioning during a surgical procedure can increase a patient’s risk of developing a pressure injury. While the type of surgical procedure determines the patient's position, nurses should still be aware of the common pressure areas.
Increased pressure points for patients in the supine position are the shoulder blades, back of the head, elbows, heels, buttocks, sacrum, and coccyx. The same pressure points are applicable for patients placed in Trendelenburg, with the addition of the shoulders. Conversely, the reverse Trendelenburg position has the same pressure points as the supine position plus the soles of the feet. The sitting or modified sitting position has the same pressure points as supine patients but with added pressure to areas like the ischium, sacrum, and back of heels. The Lithotomy position increases pressure on areas like the sacrum, coccyx, and backs of the knees (EPUAP et al., 2019).
Alternatively, the prone position puts pressure on the anterior portion of the body. So, areas like the patient’s forehead, chin, anterior shoulders, chest, patella, and dorsal surfaces of the feet. Also, consider the anterior pelvic bones, genitalia, nose, cheek, and elbows as pressure points. The freestyle or swimmer’s position has the same pressure points as the prone position but adds the lateral face and ear. The knee-to-chest position, also called the kneeling position, puts added pressure on areas like the anterior tibia, anterior ankle, face, and chest. Lastly, the lateral position’s pressure points are the lateral face, ear, shoulder, axilla, ribs, and trochanter of the hip. The patient’s medial and lateral malleoli, knees, and bent lower leg are also affected (EPUAP et al., 2019).
Pressure Points in Different Positions
Nurses should add extra padding and pillows around the pressure point areas for certain positions. For example, patients in the prone position should have additional padding around the face and chest regions, or those in supine positioning should have their knees slightly flexed and their heels elevated off the bed. Rolled towels, sheets, and blankets can also be used as extra padding. The nurse should check for the placement of medical devices and lines overlying and under the patient, as these can lead to injury. While repositioning patients in the operating room is not always an option, nurses can still reposition medical equipment and devices overlying the patient. Furthermore, the OR team should plan patient repositioning ahead of time. Nurses and the OR team must also consider “micro” turns, or small changes in a patient’s position, whenever possible. This could be as simple as turning a patient’s head to a different side while prone or shifting an elbow slightly. Also, preoperative and postoperative nurses should strive to place patients in a position different from the one required during the surgical procedure to reduce risk. For inpatients undergoing operations, a thorough skin assessment should be completed before the procedure, and again, nurses should position the patient differently from the surgical procedure (EPUAP et al., 2019).
The Association of Perioperative Registered Nurses no longer recommends using shoulder braces to secure patients. This device was causing compression over the acromion and injury to the brachial plexus. Instead, it recommends alternatives like convoluted foam or viscoelastic gel overlays (AORN, 2022b).
Before a procedure, the nurse and operating room team must consider proper supportive surfaces and mattresses for the patient. Selecting a correct supportive surface can reduce friction, moisture, and shear. The operating room team can choose from non-powered mattresses made from materials like foam, gel, or viscoelastic polymers. Other selections are powered mattresses that have continuous low-pressure or alternating-pressure support.
Alternating pressure support mattresses provide rotating air fluctuations in the mattress by inflating and deflating, thus reducing the risk of pressure injuries (Gefen et al., 2020). These types of mattresses are often preferred for high-risk patients (AORN, 2022a). However, available mattress selection greatly depends on the operation type and other equipment surrounding the patient. For example, hip replacement surgeries often require an intraoperative X-ray to be completed. A thinner mattress may be needed for this procedure so the X-ray can penetrate the mattress. Also, patients must remain stable and not be moved during certain surgeries, like neurological and cardiovascular. Thus, an alternative pressure support mattress is inappropriate for these patients (Gefen et al., 2020).
Some beds offer pressure mapping, which offers visual guidance on patient repositioning. While sometimes this is not conducive to the intraoperative environment, preoperative and postoperative nurses can still utilize this option. This would be especially helpful for postoperative nurses caring for inpatients (EPUAP et al., 2019). Some dynamic OR mattresses also offer humidity and temperature control, which can benefit patients with excessive moisture (Spruce, 2023).
Before any surgery, the nurse should perform required skin care procedures and apply prophylactic dressings to prevent pressure injuries from occurring, especially over bony prominences. Specific barrier creams can also be applied to the patient to decrease friction (Mervis & Phillips, 2019). However, this is typically determined by hospital protocols, type of procedure, and availability of certain creams.
Nurses should apply prophylactic dressings to the specific pressure points during surgery. For example, if the patient will be placed in a supine position, then sacral, scapular, and heel dressings are appropriate. For patients in Trendelenburg, some pressure areas include the occipital region, sacrum, shoulders, and others. Dressings can also be used to protect against shear and friction while moving the patient. Dressings made of soft silicone foam are preferred for prevention. However, other types may be used if these are unavailable, such as hydrocolloids or films.It should be replaced if the dressing becomes loose, soiled, or dislodged (EPUAP et al., 2019).
Careful consideration must also be taken when transferring patients within the perioperative environment. First, if the patients can transfer themselves to the operating room table, the perioperative team should allow them to do so whenever possible. However, this depends on the type of procedure and anesthesia. When transferring patients to and from the operating room table, the OR team should avoid dragging them to reduce friction and shear. Lift and transfer equipment should be used whenever possible. For example, a transfer board can be placed under the patient’s sheets and pulled by the OR team members to move a patient. Any lift or transfer equipment used should not be left under the patient as this can increase the potential of a pressure injury. However, some lifting equipment is specifically designed to be left under the patient. The perioperative nurses should know the available equipment (EPUAP et al., 2019).
Additionally, the AORN recommends that at least two to three healthcare personnel be present when completing patient transfers. This includes when lift equipment is being utilized. Having several perioperative team members present helps to avoid patient and team member injury (AORN, 2022a).
Nurses and other operating team members should be aware of medical devices that can cause pressure injuries. They must evaluate external equipment like catheters, drains, lift equipment, and prosthetic devices. Also, implanted pacemakers, medication pumps, and ports can cause added pressure to areas where they are present and will need extra padding (Spruce, 2023). Nurses must consider devices that can help to control patient moisture or continence during the procedure. For more extended operations, inserting an indwelling urinary catheter or fecal management system may be necessary for moisture control and infection prevention (EPUAP et al., 2019).
Nurses must consider personal items that may be present on the patient as potential causes of pressure injury. Some examples include hair ties, clips, braids, extensions, and body piercings or jewelry (Spruce, 2023). Items with metal can also increase the chance of burn injury during a procedure. Therefore, all personal items should be removed before surgery, labeled with the patient’s information, and placed in a designated, secure location (EPUAP et al., 2019).
The patient’s nutritional status can significantly influence perioperative pressure injury development. Malnutrition and nutritional deficiencies promote skin breakdown and can increase a patient’s healing time after surgery. Patient hydration and fluid balance are also vital. The patient’s lab values, including pre-albumin and albumin levels, should be reviewed before the procedure. (Al Aboud & Manna, 2023). The healthcare provider may order albumin before the operation to maintain fluid balance. Nurses should assess the patient’s nutritional status before surgery and utilize screening tools as previously discussed. For admitted patients, perioperative nurses can coordinate with the inpatient nurse regarding the patient’s nutritional status. A nutritional consultation with a dietician or nutritionist is also an alternative, and dietary recommendations can be made.
If a patient is scheduled for surgery, the healthcare provider should consider nutritional supplementation before and after the procedure. A high-protein and high-calorie diet can support patients with malnutrition. For patients with known pressure injuries, the required protein intake is calculated and is typically higher than for those without pressure injuries. Other supplements may include arginine, zinc, vitamin C, and antioxidants (EPUAP et al., 2019). For patients who cannot take anything by mouth, inserting a feeding tube or parenteral nutrition may be needed (Al Aboud & Manna, 2023). If the nurse finds that nutritional requirements have not been addressed, they can advocate for patient dietary supplementation to the patient’s healthcare providers.
Early mobilization and repositioning are pivotal in pressure injury prevention, especially during the postoperative setting (i.e., PACU or Phase II Recovery). Nurses should individualize early mobilization options for every patient since factors such as the patient’s cognitive and physical condition can affect decision-making. In the PACU setting, nurses must encourage patients to reposition themselves in the bed when able, assist with off-loading bony prominences, and document accordingly. Nurses in Phase II recovery, preparing patients for hospital discharge, should also discuss the importance of early mobilization after surgery. While mobilization is usually a requirement for discharge, nurses should provide education about the additional benefits of early mobilization, including preventing complications (EPUAP et al., 2019).
In addition, there are several factors nurses must consider before and during patient mobilization. First, the nurse should assess the patient’s physical and cognitive level. They would identify appropriate techniques to prevent shear forces and mobility aids, like a walker, cane, or non-slip socks, when applicable. Early mobilization doesn’t always promote the patient's walking but can include simply sitting on the edge of the bed for several minutes. Furthermore, healthcare personnel should always adequately supervise patients during early mobilization (EPUAP et al., 2019).
Documentation promotes communication between nurses and other members of the healthcare team. Nurses should always adequately document patient activities and assessment findings in the patient’s electronic health record. They should strive to complete this documentation at the bedside and in real-time. Some items to include when documenting are pressure injury risk assessments, vital signs, repositioning, and pressure injuries. Not all patients who enter a perioperative environment are inpatients. Therefore, perioperative nurses must perform a complete head-to-toe skin assessment on the patient before surgery. Preoperative nurses can sometimes coordinate complete skin assessments with emergency room, intraoperative, or other available nurses. Any skin findings, including normal and abnormal, should be documented thoroughly in the patient’s medical record. Preoperative nurses should also complete the appropriate pressure injury risk assessment tools outlined by their healthcare organization and document the patient’s risk factors and position (EPUAP et al., 2019).
Next, the intraoperative nurse receives a report from the preoperative nurse regarding the patient’s condition. The risk assessment screening tool is also reviewed before surgery. The nurse must document the patient’s starting position, pressure injury risk assessment, and any repositioning changes during surgery. Again, the nurse screens the patient for risk factors regarding pressure injury development, which may also require coordination with the anesthesia team (EPUAP et al., 2019).
During the postoperative phase, the nurse receives a detailed report regarding the patient’s condition and risk factors from the intraoperative nurse. Again, the nurse completes and documents the risk screening tool. They should document all skin assessment findings, patient repositioning, and early ambulation techniques (EPUAP et al., 2019).
Staff and patient engagement are other important factors for pressure injury prevention. Healthcare organizations should include key stakeholders in supporting prevention measures, policies, and protocols. Steering committees can promote management engagement, unit-specific projects, and measurement tracking. Often, the healthcare organization can provide specific tracking, such as which units are most likely for patients to develop pressure injuries or which injuries are facility or outpatient-acquired. Collaboration among management and staff members can help identify and address unit-specific barriers and promote team decision-making (EPUAP et al., 2019).
Another way to promote staff engagement is to have wound and pressure injury champions. Wound champions can be staff volunteers or those who’ve been elected to provide some leadership, coaching, and potential training on pressure injury prevention and wound care practices (EPUAP et al., 2019). Assignment of pressure injury prevention duties to specific perioperative team members can also promote staff engagement (Perrenoud et al., 2023). Healthcare organizations can also encourage participation in pressure injury prevention quality improvement projects by offering recognition and rewards. Reminders, such as automatic ones through the intranet or verbal reminders during staff meetings, can also promote best practices (EPUAP et al., 2019).
Nurses and other healthcare professionals should promote patient engagement. This can be done by providing written educational materials, group training sessions, and instruction. Patients and family members should be involved in this aspect of care, especially if the patient is on strict bedrest before or after surgery for a prolonged period (EPUAP et al., 2019).
All healthcare professionals within the perioperative environment should receive pressure injury education and training. Training can include didactic, computer-based, written, and bedside teaching. Some healthcare institutions also have “train the trainer” teaching and group discussions. Most high-level pressure injury prevention training starts at the organizational level, where education may include policies and standardized protocols. Unit-specific training typically involves hands-on and bedside training from fellow nurses. Unit-specific training may include hand-off tools, specific forms, and pressure injury prevention devices, like mattresses or foam (EPUAP et al., 2019).
Education should include documentation requirements, required risk assessment tools, pressure injury risk factors, classification, repositing, and wound care practices. It should also detail the skin assessment requirements and timeframe after admission for required skin assessment documentation. Lastly, education should discuss implementing best practices about a specific unit or setting within the perioperative environment. The importance of assessment tools, communication, and interprofessional approach should also be reviewed (EPUAP et al., 2019).
Initial and ongoing education and training about pressure injury prevention should also be required. Not everyone has the same learning style or experience; thus, healthcare facilities should tailor education as much as possible. One study found that direct support in each surgery specialty and assessment of responsibilities within a multidisciplinary team lead to improved prevention practices within the intraoperative setting at a Swiss University Hospital (Perrenoud et al., 2023).
Pressure injuries can lead to many potential complications, and thus, nurses must identify and understand these. First, infections are the most common complication of a pressure injury, especially if the injury is located in the sacral region. While frequently the infection is localized, an abscess can form. Postoperative wound sepsis is also another potential severe complication. Moreover, chronic injuries can cause anemia and amyloidosis, which is secondary to bleeding and water loss through the wound(Zaidi & Sharma, 2024). Other complications are osteomyelitis, leukocytosis, and bacteremia (Mondragon & Zito, 2022).
*Please note that this scenario is not all-inclusive of potential pressure injury prevention strategies and is meant to serve as a guide.
A 66-year-old male patient was admitted to the hospital’s cardiac unit earlier this morning for an elective coronary artery bypass graft (CABG) surgery. The patient’s spouse is also present. The patient was ambulatory and frequently walked before surgery; his BMI is 27.45, and he requires no assistance with transfers. After surgery, the patient will be admitted to the cardiac ICU for continuous monitoring for at least several days. What pressure injury prevention strategies would the preoperative, intraoperative, and postoperative nurses take?
First, the preoperative nurse should perform a full skin assessment alongside the cardiac unit or another perioperative nurse. They should document findings and complete the appropriate risk assessment screening tools, like the Braden and Munro scales, as their healthcare organization outlines. During this time, the preoperative nurse can also screen for patient risk factors that increase the likelihood of a pressure injury, such as increased BMI, length of NPO status, comorbidities, lab results, etc. Depending on the patient’s lab results, the nurse may need to administer albumin, blood products, or other medications. The perioperative nurse can begin education about postoperative pressure injury prevention and should include the patient and their spouse.
Next, the perioperative nurse will give the intraoperative nurse and team a detailed report. Risk factors, screening tools, and proper communication hand-off should be discussed, and documentation should be completed. Again, the intraoperative nurse will review patient risk factors, anticipated length of surgery, and other various factors that may contribute to pressure injury development. If a mattress and other repositioning devices haven’t been selected, this would be the time to do so. However, since it’s a scheduled elective surgery, this likely occurred several days before. The intraoperative nurse can also coordinate with other operating room team members for assigned injury prevention and repositioning tasks. The team should discuss planned times for patient repositioning, safety measures, the patient’s risk, and assistive device use. The intraoperative team should also document the patient’s condition during surgery, including vital signs, estimated blood loss, position changes, and length of surgery.
Last, the postoperative nurse receives a thorough report from the intraoperative nurse and anesthesia. Proper patient transfer techniques (i.e., transfer boards, lifts, etc.) should be used when moving the patient from the operating room bed to the inpatient bed. Postoperative should assess the patient’s skin alongside the intraoperative nurse, paying close attention to areas of bony prominence, where medical devices were placed, and higher-risk regions due to the patient’s position during surgery. Again, the postoperative nurse should complete the risk assessment tool and total the score. Once the patient is ready to be transferred to the cardiac ICU, the postoperative nurse will employ effective communication strategies regarding pressure injury prevention and discuss the patient’s risk. They should also report and document the patient’s risk factors, skin assessment findings, length of procedure, and estimated blood loss. After the patient is transferred to the cardiac ICU, the ICU nurse can begin promoting repositioning, early mobilization, and adequate nutrition as ordered by the surgeon.
There are numerous strategies perioperative nurses and team members can take to prevent pressure injuries. Prevention begins with a thorough skin assessment and health history; risk assessment screening tools aid it. Healthcare organizations must require initial and ongoing education regarding pressure injury prevention.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Agency for Healthcare Research and Quality. (AHRQ). (2024). Pressure ulcers. Agency for Healthcare Research and Quality. Visit Source.
Ahmad, B., Rubio-Sefati, M., & Yacob, M. M. (2023). Incidence and risk factors for pressure injuries in patients who have undergone vascular operations: a scoping review. European Journal of Medical Research, 28(1), 77. Visit Source.
Al Aboud, A. M., & Manna, B. (2023). Wound Pressure Injury Management. In StatPearls. StatPearls Publishing. Visit Source.
Association of Perioperative Registered Nurses. (AORN). (Revised 2022a, March). AORN position statement on prevention of perioperative pressure injury. Association of Perioperative Registered Nurses. Visit Source.
Association of Perioperative Registered Nurses. (AORN). (2022b, October 10). 10 new practices to protect patients from positioning injuries. Association of Perioperative Registered Nurses. Visit Source.
Association of Perioperative Registered Nurses. (AORN). (2023, May 24). Key takeaways: Prevention of pressure injury guideline updates for 2023. Association of Perioperative Registered Nurses. Visit Source.
European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance (EPUAP et al.). (2019). Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline (E. Haesler, Ed.). Visit Source.
Gefen, A., Creehan, S., & Black, J. (2020). Critical biomechanical and clinical insights concerning tissue protection when positioning patients in the operating room: A scoping review. International Wound Journal, 17(5), 1405–1423. Visit Source.
Lei, L., Zhou, T., Xu, X., & Wang, L. (2022). Munro pressure ulcer risk assessment scale in adult patients undergoing general anesthesia in the operating room. Journal of Healthcare Engineering, 2022, 4157803. Visit Source.
Mervis, J. S., & Phillips, T. J. (2019). Pressure ulcers: Pathophysiology, epidemiology, risk factors, and presentation. Journal of the American Academy of Dermatology, 81(4), 881–890. Visit Source.
Mondragon, N., & Zito, P. M. (2022). Pressure Injury. In StatPearls. StatPearls Publishing. Visit Source.
Peixoto, C. A., Ferreira, M. B. G., Felix, M. M. D. S., Pires, P. D. S., Barichello, E., & Barbosa, M. H. (2019). Risk assessment for perioperative pressure injuries. Revista Latino-americana de Enfermagem, 27, e3117. Visit Source.
Perrenoud, B., Maravic, P., & Delpy, P. (2023). Pressure injury prevention in the operating unit of a Swiss university hospital: a best practice implementation project. JBI evidence Implementation, 21(1), 46–57. Visit Source.
Sengul, T., & Gul, A. (2022). Pressure injury in the perioperative period during COVID-19 pandemic: Incidence and patient-related risk factors in a hospital in Turkey. Journal of Tissue Viability, 31(4), 714–717. Visit Source.
Spruce L. (2023). Prevention of Perioperative Pressure Injury. AORN Journal, 117(5), 317–323. Visit Source.
Zaidi, S. R. H., & Sharma, S. (2024). Pressure Ulcer. In StatPearls. StatPearls Publishing. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.