Urinary tract infections (UTIs) include cystitis (infection of the bladder/lower urinary tract) and pyelonephritis (infection of the kidney/upper urinary tract). The pathogenesis of UTI begins with colonization of the vaginal introitus or urethral meatus by uropathogens from the fecal flora, followed by ascension via the urethra into the bladder. Pyelonephritis develops when pathogens ascend to the kidneys via the ureters. Pyelonephritis can also be caused by seeding of the kidneys from bacteremia. It is possible that some cases of pyelonephritis are associated with seeding of the kidneys from bacteria in the lymphatics.
Acute complicated UTI in adults is defined as a UTI that has possibly extended beyond the bladder (i.e., UTI with fever or other systemic symptoms, suspected or documented pyelonephritis, and UTI with sepsis or bacteremia). When there are symptoms of cystitis without fever, flank pain, costovertebral angle (CVA) tenderness, and other signs of systemic illness, this is considered acute simple cystitis. This approach to categorizing UTI differs from other conventions as will be discussed in detail below.
The urinary system can simply be described as the body’s drainage system for filtering and eliminating wastes from the body, as well as, maintaining the homeostasis of water, ions, pH, blood pressure, calcium and red blood cells.
The organs of the urinary system are the (Figure 1):
Kidneys which secrete the urine
Ureters or tubes that convey the urine to the bladder where it is temporarily stored
Urethra, through which the urine is discharged from the body.
Figure 1 Organs of the Urinary System
The kidneys are paired organs lying along the posterior wall of the abdominal cavity on either side of the vertebral column and behind the peritoneum. They are often described as bean-shaped each about the size of a fist. The left kidney is located slightly higher than the right kidney because it is displaced upwards by the liver. The kidneys, unlike the other organs of the abdominal cavity, are located posterior to the peritoneum and touch the muscles of the back. The kidneys are surrounded by a layer of adipose tissue that holds them in place and protects them from physical damage.
The kidneys are responsible for regulating the acid-base balance in the blood and hence in the body as a whole, maintaining the water balance in the body and excreting the waste products of metabolism from the blood. Their excretory activities conserve the proper concentration of essential organic and inorganic substances in the blood. Essentially the kidneys role of excretion keeps the body’s internal environment within physiological limits. The kidneys filter about 3 ounces of blood every minute. The waste products of metabolism along with extra water make up approximately the 1 to 2 quarts of urine a person produces each day.
The ureters are a pair of tubes that carry urine from the kidneys to the urinary bladder. Each is about 10 to 12 inches long and run along the left and right sides of the body parallel to the vertebral column. They descend beneath the peritoneum on the posterior abdominal wall and cross the pelvic floor to reach the bladder. Gravity and peristalsis of smooth muscle tissue in the walls of the ureters move urine toward the urinary bladder. The ends of the ureters extend slightly into the urinary bladder and are sealed at the point of entry to the bladder by the ureterovesical valves. These valves prevent urine from flowing back upwards to the kidneys.
The urinary bladder is pear-shaped, becoming more oval as it fills with urine. This muscular sac lays midline at the inferior end of the pelvis behind the symphysis pubis, in front of the rectum in the male and in front of the vagina and uterus in the female. When empty, the bladder inside is arranged in folds (called rugae), which disappear as the bladder expands with urine. Urine entering the urinary bladder from the ureters fills the hollow space of the bladder slowly and stretches its elastic walls. The walls of the bladder allow it to stretch to hold anywhere from 500 to 800 milliliters of urine. After emptying, the bladder may still retain about 50 cc residual volume. At about 150 cc of volume, stretch receptors in the detrusor muscle begin signaling the central nervous system via afferent nerves; at 400 cc we are "seeking" an appropriate toilet.
Thus, the bladder serves as a reservoir in which the urine is stored until it is eliminated from the body. There are three openings on the floor of the bladder: one in front for the urethra and two at the sides for the ureters (called urethral openings).
At the base of the bladder is the bladder neck, which opens into the urethra, through which urine is expelled to the external environment. The bladder neck and the proximal urethra (nearest part) are supported by pubourethral ligaments and the levator ani muscles of the pelvic floor. The anatomy of the male urethra and female urethra vary considerably in both length and structure. The female urethra is around 2 inches long and ends inferior to the clitoris and superior to the vaginal opening. In males, the urethra is about 8 to 10 inches long and ends at the tip of the penis. The urethra is also an organ of the male reproductive system as it propels sperm out of the body through the penis. The first 3 - 4 cm of the male urethra passes through the prostate gland, which lies below the bladder and is attached to its base.
The flow of urine through the urethra is controlled by the internal and external urethral sphincter muscles. The internal urethral sphincter is made of smooth muscle and opens involuntarily when the bladder reaches a certain set level of distention. The opening of the internal sphincter results in the sensation of needing to urinate. The external urethral sphincter is made of skeletal muscle and may be opened to allow urine to pass through the urethra or may be held closed to delay urination.
Micturition is the process by which urine is expelled from the bladder. It can be broken down into 5 basic steps:
Urine is made in the kidneys
Urine is stored in the bladder
The urethral sphincter muscles relax
The bladder muscle (detrusor muscle) contracts
The bladder is emptied through
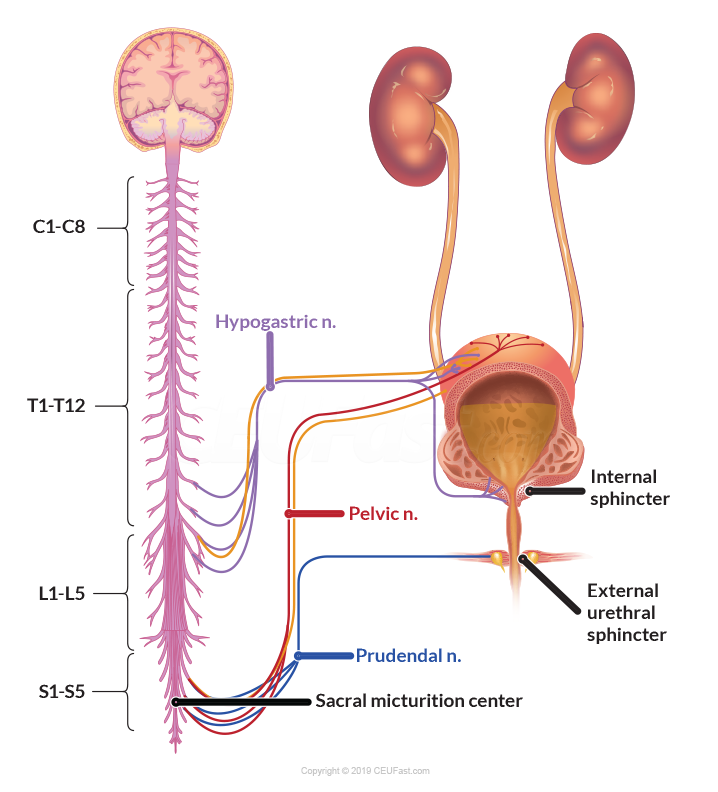
Beyond those 5 steps, there are elaborate layers of neurologic control which illustrate the micturition process (Figure 2).
Figure 2 Neurologic Innervation of Urinary System
The bladder is composed of bands of interlaced smooth muscle called the detrusor muscle. The innervation of the body of the bladder is different from that of the bladder neck. The body of the bladder is rich in beta-adrenergic receptors which are stimulated by the sympathetic component of the autonomic nervous system (ANS). Beta stimulation, via fibers of the hypogastric nerve, suppress contraction of the detrusor muscle, i.e., allows the detrusor muscle to relax (the bladder fills with urine). Conversely, parasympathetic stimulation, by fibers in the pelvic nerve causes the detrusor muscle to contract (the bladder empties). Sympathetic stimulation is predominant during bladder filling, and the parasympathetic causes emptying.
The ureters pass between the layers of the detrusor muscle and enter the bladder through the trigone. The ureters propel urine into the bladder. The bladder passively expands to accept urine. As the bladder expands and intravesicular pressure increases, the ureters are compressed between the layers of muscle, creating a valve mechanism. This valve mechanism limits the backflow of urine up towards the kidneys.
Two sphincters control the bladder outlet:
The internal sphincter is composed of smooth muscle like the detrusor muscle and extends into the bladder neck. Like the detrusor muscle, the internal sphincter is controlled by the ANS and is normally closed. The primary receptors in the bladder neck are alpha-adrenergic. Sympathetic stimulation of these alpha receptors, via fibers in the hypogastric nerve, contributes to urinary continence.
The external sphincter is striated muscle. Like skeletal muscle, it is under voluntary control. It receives its innervation from the pudendal nerve, arising from the ventral horns of the sacral cord. During micturition, supraspinal centers block stimulation by the hypogastric and pudendal nerves. This relaxes the internal and external sphincters and removes the sympathetic inhibition of the parasympathetic receptors. The result is the unobstructed passage of urine when the detrusor muscle contracts.
Under normal circumstances, we are able to control where and when we urinate. This is largely because the cerebrum is able to suppress the sacral micturition reflex. If the sacral reflex is unrestrained, parasympathetic stimulation via the pelvic nerve causes detrusor muscle contraction. Detrusor muscle contraction is suppressed by alpha and beta sympathetic stimulation via the hypogastric nerve. In response to afferent stimulation, the cerebrum becomes aware of the need to void. If it is appropriate, the cerebrum relaxes the external sphincter, blocks sympathetic inhibition, the bladder contracts, and urine is expelled.
Infection does not always occur when microorganisms are introduced into the bladder. A number of defense systems protect the urinary tract against infection-causing microorganisms:
Urine functions as an antiseptic, washing potentially harmful microorganisms out of the body during normal urination. Urine is normally sterile, that is, free of bacteria, viruses, and fungi.
The ureters join into the bladder in a manner designed to prevent urine from backing up into the kidney when the bladder squeezes urine out through the urethra.
The prostate gland in men secretes infection-fighting substances.
The immune systems defenses and antibacterial substances in the mucous lining of the bladder eliminate many organisms.
In healthy women, the vagina is colonized by lactobacilli, beneficial microorganisms that maintain a highly acidic environment (low pH) that is hostile to other microorganisms. Lactobacilli produce hydrogen peroxide, which helps eliminate microorganisms and reduces the ability of Escherichia coli (E. coli) to adhere to vaginal cells. (E. coli is the major bacterial culprit in UTIs.)
UTIs are some of the most common bacterial infections, affecting 150 million individuals each year worldwide.1 In 2007, in the United States alone, there were an estimated 10.5 million office visits for UTI symptoms (constituting 0.9% of all ambulatory visits) and 2 - 3 million emergency department visits.2-4 Currently, the societal costs of these infections, including health care costs and time missed from work, are approximately US $3.5 billion/year in the United States alone. UTIs are a significant cause of morbidity in infant boys, older men and females of all ages. Serious sequelae include frequent recurrences, pyelonephritis with sepsis, renal damage in young children, pre-term birth and complications caused by frequent antimicrobial use, such as high-level antibiotic resistance and Clostridium difficile colitis.
UTIs are caused by both Gram-negative and Gram-positive bacteria, as well as, by certain fungi. The most common causative agent for both uncomplicated and complicated UTIs is uropathogenic Escherichia coli (UPEC).
Causative agents involved in uncomplicated UTIs are3,5-7:
UPEC (75% incidence)
Klebsiella pneumoniae (6% incidence)
Staphylococcus saprophyticus (6% incidence)
Enterococcus faecalis (5% incidence)
group B Streptococcus (GBS) (3% incidence)
Proteus mirabilis (2% incidence)
Pseudomonas aeruginosa (1% incidence)
Staphylococcus aureus (1% incidence)
Candida spp. (1% incidence)
Causative agents involved in complicated UTIs are8,9-11:
UPEC (65% incidence)
Escherichia coli is the most common organism isolated but is isolated more frequently in women than in men.12-14
Enterococcus spp. (11% incidence)
Klebsiella pneumoniae (8% incidence)
Candida spp. (7% incidence)
Staphylococcus aureus (3% incidence)
Staphylococci (methicillin-sensitive Staphylococcus aureus [MSSA] and methicillin-resistant S. aureus [MRSA])
Proteus mirabilis (2% incidence)
Pseudomonas aeruginosa (2% incidence)
group B Streptococcus (GBS) (2% incidence)
The prevalence of particular pathogens depends partially on the host. For examples:
Pseudomonas is more common in patients with health care exposures or instrumentation.
Staphylococcus saprophyticus is an occasional cause of pyelonephritis in young, otherwise healthy women.
UTI due to Candida spp will be presented in another learning module.
Patients suffering from a symptomatic UTI are commonly treated with antibiotics, but these treatments can result in long-term alteration of the normal microbiota of the vagina and gastrointestinal tract and in the development of multidrug-resistant microorganisms.15 The availability of niches that are no longer filled by the altered microbiota can increase the risk of colonization with multidrug-resistant uropathogens.
UTIs are becoming increasingly difficult to treat owing to the widespread emergence of an array of antibiotic resistance mechanisms.3,4,10,16-19 Of particular concern are members of the family Enterobacteriaceae, including E. coli and K. pneumoniae, which have both acquired plasmids encoding extended-spectrum β-lactamases (ESBLs). These plasmids rapidly spread resistance to third-generation cephalosporins, as well as, other antibiotics.10,16-20 Other Enterobacteriaceae family members produce the class C β-lactamases (AmpC enzymes) that are active against cephamycin in addition to third-generation cephalosporins and are also resistant to β-lactamase inhibitors.16-19 The expression of AmpC enzymes is also associated with carbapenem resistance in K. pneumoniae strains lacking a 42 kDa outer-membrane protein.10,16-19
Importantly, the ‘golden era’ of antibiotics is waning. As such, the need for rationally designed and alternative treatments is therefore increasing. Recent studies have used RNA sequencing to directly analyze uropathogens from the urine of women experiencing symptomatic UTIs. These studies, together with basic science and improved animal models, have been crucial in enabling us to understand the molecular details of how uropathogens adhere, colonize and adapt to the nutritionally limited bladder environment, evade immune surveillance, and persist and disseminate in the urinary tract. These studies have therefore revealed key virulence factors that can be targeted to prevent and counteract the pathogenic mechanisms that are important in UTIs.15,21,22
Step 1: Contamination of the periurethral area with a uropathogen from the gut
Step 2: Colonization of the urethra and migration to the bladder
Step 3: Colonization and invasion of the bladder mediated by pili and adhesins
Step 4: Host inflammatory responses, including neutrophil infiltration, begin to clear extracellular bacteria.
Steps 5 and 6: Some bacteria evade the immune system, either through host cell invasion or through morphological changes that result in resistance to neutrophils, and these bacteria undergo multiplication (step 5) and biofilm formation (step 6).
Steps 7 and 8: These bacteria produce toxins and proteases that induce host cell damage (step 7), releasing essential nutrients that promote bacterial survival and ascension to the kidneys (step 8).
Steps 9 and 10: Kidney colonization (step 9) results in bacterial toxin production and host tissue damage (step 10).
Step 11: If left untreated, UTIs can ultimately progress to bacteremia if the pathogen crosses the tubular epithelial barrier in the kidneys.
Complicated UTIs (Figure 3B)
Uropathogens that cause complicated UTIs follow the same initial steps as those described for uncomplicated infections, including:
Step 1: Periurethral colonization
Step 2: Progression to the urethra and migration to the bladder
However, in order for the pathogens to cause infection, the bladder must be compromised. The most common cause of a compromised bladder is catheterization.
Step 3: Owing to the robust immune response induced by catheterization fibrinogen accumulates on the catheter, providing an ideal environment for the attachment of uropathogens that express fibrinogen-binding proteins.
Step 4: Infection induces neutrophil infiltration but after their initial attachment to the fibrinogen-coated catheters
Step 5: Bacteria multiply
Step 6: Formation of biofilms
Step 7: Bacterial toxins and proteases promote epithelial damage
Steps 8 and 9: ascension to the kidneys (step 8) resulting in colonization of the kidneys (step 9)
Step 10: where toxin production induces tissue damage
Step 11: If left untreated, uropathogens that cause complicated UTIs can also progress to bacteremia by crossing the tubular epithelial cell barrier.
UTIs can be clinically categorized as either acute uncomplicated UTIs or acute complicated UTI based on the extent and severity of the infection. This categorization directs the management of care and differs somewhat from other conventions. Specifically:
Uncomplicated UTIs typically affect women, children and elderly individuals who are otherwise healthy and have no structural or neurological urinary tract abnormalities.5,23
An acute uncomplicated UTI is presumed to be confined to the bladder (cystitis) with no signs or symptoms that suggest an upper tract or systemic infection.
Risk factors associated with cystitis include3-5,21,23:
Diabetes
Female gender
Genetic susceptibility
Obesity
Prior history of a UTI
Sexual activity
Vaginal infection
Cystitis or pyelonephritis in a nonpregnant premenopausal woman without underlying urologic abnormalities has traditionally been termed acute uncomplicated UTI.
Complicated UTI has been defined, for the purposes of treatment trials, as UTIs associated with factors that compromise the urinary tract or host defense.
Risk factors associated with complicated UTIs include8,24:
Exposure to antibiotics
Immunosuppression
Pregnancy
Presence of foreign bodies such as calculi, indwelling catheters or other drainage devices
Renal failure
Renal transplantation
Urinary obstruction
Urinary retention caused by neurological disease
In the United States, 70 - 80% of complicated UTIs are attributable to indwelling catheters,25 accounting for 1 million cases/year.4
Catheter-associated UTIs (CAUTIs) are associated with increased morbidity and mortality and are collectively the most common cause of secondary bloodstream infections.
Risk factors for developing a CAUTI include26:
Diabetes
Female gender
Older age
Prolonged catheterization
Acute complicated UTI refers to an acute UTI with any of the following features, which suggest that the infection extends beyond the bladder.
Fever (>99.9°F/37.7°C)
This temperature threshold is not well defined and should be individualized, taking into account baseline temperature, other potential contributors to an elevated temperature, and the risk of poor outcomes should empiric antimicrobial therapy be inappropriate
Costovertebral angle tenderness
Flank pain
Other signs or symptoms of systemic illness including:
Chills or rigors
Significant fatigue or malaise beyond the baseline
Pelvic or perineal pain in men, which can suggest accompanying prostatitis.
As defined, pyelonephritis is a complicated UTI, regardless of patient characteristics. In the absence of any of these symptoms, patients with a UTI are considered to have acute simple cystitis, and consequently, the patient will be managed differently.
Patients with underlying urologic abnormalities (such as nephrolithiasis, strictures, stents, or urinary diversions), immunocompromising conditions (such as neutropenia or advanced HIV infection), or poorly controlled diabetes mellitus are not considered to have a complicated UTI if they have no concerning symptoms for upper tract or systemic infection. These patients, however, can be at a higher risk for more serious infection and have not traditionally been included in studies evaluating the antibiotic regimens typically used for acute simple cystitis. These patients are followed more closely and/or have a lower threshold to manage them as a complicated UTI (e.g., if they have subtle signs or symptoms that could be suggestive of more extensive infection). Many patients with significant urologic abnormalities come to clinical attention for UTI because of signs or symptoms consistent with complicated UTI as defined here (rather than features of simple cystitis alone).
Men are not automatically considered to have acute complicated UTI in the absence of concerning symptoms for upper tract or systemic infection. However, the possibility of prostatic involvement should always be considered in men, and this is incorporated into the approach with men with apparent simple cystitis.
Special populations with unique management considerations such as pregnant women and renal transplant recipients will not be considered in this learning module.
Individuals who do not fit into either category have often been treated as having a complicated UTI by default.
The approach to treatment should be based on the extent of infection and severity of illness. Since complicated UTI, as defined here, is a more serious infection than simple cystitis, the efficacy of an antimicrobial agent is of greater importance, and certain agents used for simple cystitis should not be used for complicated UTI because they do not achieve adequate levels in tissue, which may be important for a cure. The risk of infection with drug-resistant organisms is a consideration in antibiotic selection for both simple cystitis and acute complicated UTI.
A wide variety of genitourinary abnormalities may be associated with complicated UTI27 (Table 1). The most common determinant of infection is interference with normal voiding, leading to impaired flushing of bacteria from the genitourinary tract. Mechanisms of infection include28:
Increased introduction of organisms into the genitourinary tract through instrumentation
Obstruction with incomplete urinary drainage
Persistence of bacteria in biofilm on stones or indwelling devices
The risk of infection varies with different abnormalities. For instance, a chronic indwelling catheter is uniformly associated with bacteriuria,29 while infection complicating a single obstructing ureteric stone may be transient, especially with stone removal.
Table 1: Structural and Functional Abnormalities in teh Genitourinary Tract Associated with Complicated UTI
Obstruction
Congenital abnormalities Diverticulae Pelvicalyceal obstruction Prostatic hypertrophy Renal cysts Tumors of the urinary tract Ureteric or urethral strictures Urolithiasis
Complicated UTI occurs in both women and men, and in any age group.
Because uncomplicated UTI is rare in men, any male urinary infection is usually considered complicated.30
Recurrent UTI in postmenopausal women is associated with genetic and behavioral risk factors similar to those in younger women with acute uncomplicated UTI, including a greater likelihood of being a nonsecretor and history of prior urinary infection.31
Postmenopausal women with recurrent UTI are also more likely to have increased residual urine volume, cystoceles and prior genitourinary surgery than are women without infection, and these associations are consistent with complicated infection. Thus, as a population, postmenopausal women with recurrent UTI encompass elements consistent with both uncomplicated and complicated UTI.
Risk factors for multidrug-resistant gram-negative UTIs in patients with a history of any of the following in the past three months include32-36:
A multidrug-resistant gram-negative urinary isolate
Inpatient stay at a health care facility (e.g., hospital, nursing home, long-term acute care facility)
Use of a fluoroquinolone, trimethoprim-sulfamethoxazole (TMP-SMX), or a broad-spectrum beta-lactam (e.g., third or later generation cephalosporin)
This includes a single antibiotic dose given for prophylaxis prior to prostate procedures.
Travel to parts of the world with high rates of multidrug-resistant organisms
Multidrug resistance refers to nonsusceptibility to at least one agent in three or more antibiotic classes. This includes isolates that produce an extended-spectrum beta-lactamase (ESBL).
The prevalence of multidrug resistance is not well documented in all parts of the world. Some countries where the prevalence is particularly high include India, Israel, Spain, and Mexico.
Increasing rates of resistance in uropathogens have been reported globally.
As an example, in the United States, one study documented a threefold increase in the prevalence of ESBL-producing Enterobacteriaceae among hospitalized patients with UTIs from 2000 to 2009.37
In another study of patients with pyelonephritis presenting to emergency departments across the United States, approximately 6% of the 453 E. coli isolates produced ESBL, although rates varied by region and complicating features.38
In particular, a specific strain of E. coli, sequence type 131 (ST131), has emerged globally as a major cause of fluoroquinolone-resistant and ESBL-producing E. coli UTIs.39 In one study of E. coli clinical isolates from extraintestinal sites, predominantly urine, collected at Veterans Affairs (VA) laboratories across the United States, the ST131 clone accounted for the majority of fluoroquinolone-resistant and ESBL isolates and was calculated to account for 28% of all VA E. coli isolates nationwide.40 Carbapenem resistance among Enterobacteriaceae has also increased.
Other comorbidities which increase the risk factors for UTIs include:
Blockages in the urinary tract such as kidney stones or an enlarged prostate which can trap urine in the bladder.
Catheter use including individuals who are hospitalized, individuals with neurological problems that make it difficult to control their ability to urinate and individuals who are paralyzed.
Recent urinary procedure, i.e., urinary surgery or an examination of an individual’s urinary tract that involves medical instruments.
Suppressed immune system such as diabetes mellitus, HIV/AIDS.
Urinary tract abnormalities
Babies born with urinary tract abnormalities that do not allow urine to leave the body normally or cause urine to back up in the urethra.
The clinical spectrum of acute complicated UTI encompasses both cystitis with complicating features and pyelonephritis:
Signs and symptoms of cystitis include:
Dysuria
Urinary frequency and urgency
Suprapubic pain
Hematuria
Signs and symptoms of acute complicated UTI which suggest that infection has extended beyond the bladder include:
Fever
Other features of systemic illness such as:
Chills
Marked fatigue or malaise beyond baseline
Rigors
Signs and symptoms of pyelonephritis classically include41:
Fever/chills
Flank pain
Costovertebral angle tenderness
Nausea/vomiting
Symptoms of cystitis are often but not always present
Atypical symptoms may occur including:
Pain in the epigastrium
Pain in lower abdomen
Not all patients with acute complicated UTI present with clear symptoms localized to the urinary tract. For examples:
Patients with spinal cord injury and neurogenic bladder can present with autonomic dysreflexia and increased spasticity.
Elderly or debilitated patients may present with more generalized signs or symptoms of infection (e.g., fever and chills) without clear symptoms localizing to the urinary tract.
Pyuria is present in almost all patients with UTI.
Patients with acute complicated UTI may be associated with severe morbidity, such as septic shock or even death. But patients may also present with:
Acute renal failure
Renal failure was previously a common cause of death in spinal cord injury patients with recurrent urosepsis.
Current management strategies that maintain a low bladder pressure prevent reflux and progression to renal failure, despite a continued high incidence of urinary infection experienced by these patients.42
When renal failure occurs in patients with complicated UTI, deterioration in renal function is usually attributable to the underlying urological defect rather than infection.
Bacteremia
Multiple organ system dysfunctions
Shock
Acute or chronic infection is occasionally associated with suppurative complications, such as:
Metastatic infection including bone and joint infection or endocarditis
Paraurethral abscesses
Renal abscesses
Perirenal abscess
Risk factors for these complications are relatively uncommon and are more likely to occur in patients with comorbidities such as43,44:
Diabetes mellitus
Those with chronic urological devices
Recent urinary tract instrumentation
Urinary tract abnormalities
Urinary tract obstruction
Acute pyelonephritis can also be complicated by:
Emphysematous pyelonephritis
Papillary necrosis
Perinephric abscess
Progression of the upper urinary tract infection to renal corticomedullary abscess
Xanthogranulomatous pyelonephritis is a rare variant of pyelonephritis in which there is massive destruction of the kidney by granulomatous tissue.
Most cases occur in the setting of obstruction due to infected renal stones.
Affected patients can present with weeks to months of insidious and nonspecific signs and symptoms, such as malaise, fatigue, nausea, or abdominal pain.
Acute complicated UTI should be suspected in patients with complaints of acute lower tract irritative symptoms which include:
Dysuria
New or increased incontinence
Suprapubic discomfort/pain
Those who otherwise appear clinically ill
Urinary frequency or urgency
Acute pyelonephritis, specifically, should be suspected in patients (even in the absence of typical symptoms of cystitis) presenting with complaints of:
Costovertebral angle pain or tenderness
Fever, chills, rigor
Flank pain
Pelvic or perineal pain (in men)
Variable lower tract symptoms
Some patients with neurological illnesses may be more difficult to assess because of atypical presentations.42,45,46
Patients with spinal cord injuries may present with symptoms such as increased bladder and leg spasms42 or autonomic dysreflexia.45
Patients with multiple sclerosis may experience increased fatigue and deterioration in neurological function.46
The individual patient often experiences consistent symptoms in each episode and will frequently attribute specific complaints to urinary infection.
Cloudy or foul-smelling urine is often interpreted by patients and caregivers as urinary infection.
While these findings may accompany bacteriuria, they are not diagnostic of symptomatic infection.47
The identification of symptomatic infection in patients with chronic symptoms or impaired communication, such as long-term care facility patients, is more problematic.
Clinical deterioration without genitourinary-localizing symptoms is seldom due to UTI in residents without a chronic indwelling catheter.48
Fever without localizing findings is, however, a common presentation of UTI in patients with chronic indwelling catheters.
Acute complicated UTI should also be suspected in patients with nonlocalizing fever or sepsis.
Acute complicated UTI should be suspected in elderly or debilitated patients who have nonspecific signs or symptoms, such as falls, change in functional status, and change in mental status. However, growing evidence indicates that these are not reliable predictors of bacteriuria or UTI.49-52 When these nonspecific signs or symptoms are accompanied by signs or symptoms of systemic infection or pyelonephritis, evaluation for acute complicated UTI with urine studies, in addition to a general infectious workup, is appropriate.
A complete physical examination should specifically include:
Assessment for fever
Costovertebral angle tenderness
Abdominal tenderness
Suprapubic tenderness
Among sexually active young women, a pelvic examination should be performed, particularly if symptoms are not convincing for a UTI, to evaluate for cervical motion or uterine tenderness, which would be suggestive of pelvic inflammatory disease (PID).
A digital rectal examination should be performed on men who present with symptoms of pelvic or perineal pain to evaluate for a tender or edematous prostate that would suggest acute prostatitis.
Urinalysis (either by microscopy or by dipstick) for evaluation of pyuria
Symptomatic UTI is usually accompanied by pyuria (i.e., urine containing white blood cells or pus) identified by urinalysis or a positive leukocyte esterase dipstick test. However, pyuria is also present in most patients with asymptomatic bacteriuria.12,53,54
Noninfectious causes of urinary tract inflammation in patients at risk for complicated UTI are also characterized by pyuria.
As a result, pyuria is consistent with, but not diagnostic of, UTI and pyuria in the bacteriuric patient does not identify symptomatic infection.
There is, however, a high negative predictive value for pyuria, and a urinalysis without pyuria may reliably exclude symptomatic urinary infection.55,56
White blood cell casts are found on urinalysis in some subjects with renal infection. They are, however, nonspecific, and present in interstitial nephritis and other tubulointerstitial disorders with inflammation, in addition to infection.
Pyuria is present in almost all patients with UTI, therefore, its absence suggests an alternative diagnosis, particularly in patients who present with nonspecific symptoms.
White cell casts, in particular, suggest a renal origin for pyuria. However, pyuria and bacteriuria (i.e., presence of bacteria in the urine) may occasionally be absent if the infection does not communicate with the collecting system or if the collecting system is obstructed.
The ideal voided urine sample for evaluation of UTI is one that accurately represents the bladder bacterial count with minimized contamination by bacteria colonizing the distal urethra and genital mucosa.
In theory, this would be a clean-catch, midstream sample of the first micturition of the day.
In fact, there is no clinical evidence that this ideal specimen yields more accurate results.
Collection of a midstream urine, with or without cleaning of the urethral meatus, at the time of clinical evaluation likely produces a reasonable specimen for analysis.57
The likelihood of detecting a bladder bacteriuria by voided urine culture is highest if urine is collected upon awakening in the morning.
This sample is likely to be most concentrated, and bacteria in the bladder will have had time to multiply overnight.
However, this ideal sample is not practical since most cultures are obtained at the time the patient is seeing the clinician.
With samples collected later in the day, the combination of more dilute urine and partial bacterial washout due to multiple voids may lower the colony count below the accepted definition for bacteriuria diagnostic of a UTI.
An optimal clean-catch, midstream urine is collected through the following steps in attempts to minimize the degree of contamination with bacteria from the urethra:
Local disinfection of the meatus and adjacent mucosa should be performed with a non-foaming antiseptic solution, such as Dakin’s solution (diluted sodium hypochlorite solution 0.5%). The region should then be dried with a sterile swab to avoid mixture of the antiseptic with urine.
Contact of the urinary stream with the mucosa should be minimized by spreading the labia in females and by pulling back the foreskin in uncircumcised males.
The initial stream of the voided specimen should be discarded since the initial urine flushes urethral contaminants. It is the subsequent midstream sample that should be sent to the laboratory.
However, clinical studies do not demonstrate that cleaning the meatus is associated with lower rates of contamination.57-60 Thus, for patients in whom the cleaning step may be impractical or difficult, a midstream urine collected (with the labia spread, for women) is likely to be an appropriate sample.
For men with suspected chronic bacterial prostatitis, evaluation of the last few drops of urine after prostatic massage is indicated. Firm prostatic massage per rectum, from lateral to midline on each side, causes the contents of the prostatic ducts to be expressed. Vertical strokes in the midline will then project the secretions into the urethra and permit counting of leukocytes. Of note, this maneuver should be avoided when acute bacterial prostatitis is suspected because of the risk of bacteremia.
The urine sample should be sent immediately to the bacteriology laboratory since bacteria will continue to proliferate in the warm medium of freshly voided urine, leading to increased bacterial counts.
If such immediate transport is not possible, the container should be transported in iced water and then stored in a refrigerator at 4ºC. Cooling stops bacterial growth, but the following day the bacteria can still grow on culture medium. However, urinary leukocytes may be altered by refrigeration, possibly affecting the interpretation of the urinalysis.
Urinalysis by Dipstick
Indications and Use
Dipsticks to evaluate for urine leukocyte esterase and nitrite can be used as a screening tool for the diagnosis of UTI. Dipsticks are generally performed whenever a UTI is suspected.
However, we do not routinely collect urine for dipstick in young nonpregnant women with a history clearly suggestive of a UTI (i.e., typical symptoms without vaginal discharge or irritation), as the dipstick generally does not provide additional useful information.61-63
A positive dipstick can support the diagnosis of UTI in a patient with suggestive symptoms, and a negative test can refute the diagnosis if clinical suspicion is low.
A negative nitrite and leukocyte esterase on the dipstick may represent false negative results in a truly infected patient, and a urine culture should generally be performed if clinical suspicion is high.64
In general, dipsticks to evaluate for leukocyte esterase and nitrite should not be performed in patients without any symptoms consistent with a UTI, as a positive dipstick, which would denote the presence of pyuria and/or bacteriuria, does not indicate a UTI in an asymptomatic patient.
Accuracy of Dipsticks
Dipsticks detect the presence of leukocyte esterase and nitrite in the urine. Leukocyte esterase corresponds to pyuria and nitrite reflects the presence of Enterobacteriaceae, which convert urinary nitrate to nitrite.65,66 Leukocyte esterase may be used to detect >10 leukocytes per high power field (sensitivity of 75 to 96%, specificity of 94 to 98%).67 A positive nitrite test is a reliable index of significant bacteriuria, although a negative test does not exclude bacteriuria.
The dipstick nitrite test depends on the presence of nitrate (from dietary metabolites) in the urine that is then converted to nitrite by bacteria also present in the urine.
Normally no detectable nitrite is present.
When bacteriuria is significant, the test is positive in about 80% of cases in which the urine has incubated for at least four hours in the bladder.68
False positive nitrite tests can occur with substances that turn the urine red, such as the bladder analgesic phenazopyridine or the ingestion of beets.
Reasons for a negative nitrite test despite the presence of bladder bacteriuria include:
Inability of some organisms to convert nitrate to nitrite (such as Enterococcus faecalis)
Insufficient bladder incubation time for conversion of nitrate to nitrite
Low urinary excretion of nitrate
Decreased urine pH (due to cranberry juice or other dietary supplements)
Most studies have supported the diagnostic value of the nitrite and leukocyte esterase results, particularly when they are concordant.69,70
A meta-analysis including 70 publications concluded that the urine dipstick test alone is useful when both nitrite and leukocyte esterase tests are positive (sensitivity 68 to 88%).69
The diagnostic value of dipstick testing has been evaluated in both primary care and emergency settings.
In a review of six studies that included women aged 17 to 70 with suspected UTI in primary care settings, positive dipstick findings (nitrite or leukocyte esterase and blood) had sensitivity and specificity of 75 and 66%, respectively.71
In a systematic review of four studies that evaluated the utility of dipstick results in addition to history and physical examination findings in diagnosing uncomplicated UTI in women presenting to the emergency room, a negative dipstick urinalysis accurately ruled out the diagnosis of UTI (as confirmed by urine culture) when the pretest probability was low.72
Across the studies, which included 948 women, the prevalence of UTI ranged from 40 to 60% and only a positive nitrite reaction was useful to rule in a UTI and only a negative leukocyte esterase or blood reaction were accurate in ruling out a UTI.
However, other studies have suggested that dipstick results are of lower clinical utility.
In one study, 434 adult females with suspected lower UTI in a primary care setting were assessed. Sixty-six patients had confirmed UTI. The presence of nitrite, leukocyte esterase, and blood on the dipstick, as well as, clinical criteria (urine cloudiness, dysuria, and nocturia) were evaluated for diagnostic value. The negative predictive value was 67% for the absence of all features, and the positive value was 82% for the presence of three features. The authors concluded that dipstick results can modestly improve diagnosis, but cannot adequately rule out infection.73
Similarly, in a study of 2,252 women with overactive bladder, dipstick test was not sufficient to identify patients with UTI (sensitivity and specificity 44 and 86% respectively).74
Urine Culture with Susceptibility Testing
A urine specimen for culture obtained before the initiation of antimicrobial therapy confirms the diagnosis of UTI and identifies the infecting organism and susceptibilities. The wide variety of potential infecting organisms and increased likelihood of more resistant organisms makes the urine culture essential for optimal antimicrobial management. Urine Gram stain can also be helpful to narrow down the list of potential causative organisms and inform empiric antimicrobial selection.
A positive urine culture confirms but is not diagnostic of symptomatic UTI.
In populations with a high prevalence of asymptomatic bacteriuria, a positive urine culture has a low positive predictive value for symptomatic infection.13,75,76
For instance, in noncatheterized bacteriuric elderly institutionalized patients with fever and no localizing signs or symptoms, bacteriuria has only a 10% positive predictive value for a urinary source of fever.48
A negative urine culture, however, has a high negative predictive value, and is useful to exclude UTI.
Indications for urine culture
The role of pretreatment urine culture in the evaluation of suspected UTI is to confirm the presence of bacteriuria and to identify and provide antibiotic susceptibility information on the causative organism (often retrospectively, if treatment is empirically given).
The culture of a clean-catch voided urine specimen is warranted for these purposes among most patients with suspected UTI, except for healthy non-pregnant young women with typical symptoms of non-febrile cystitis, that is, of an uncomplicated UTI.61,62,77
Among such women, the constellation of symptoms is sufficiently diagnostic.63,78
The causative organism is typically Escherichia coli,79 and an empiric short course of antimicrobial therapy is typically effective.80,81
The choice of antibiotic is generally determined by the local susceptibility patterns of E. coli and a patient history of antibiotic allergy, especially to sulfonamides.
In certain cases, however, pretreatment urine culture is indicated in young women with:
Atypical symptoms
Failure to respond to initial therapy, raising the possibility of a resistant organism
Presentation suggestive of pyelonephritis
Recurrent symptoms less than one month after treatment of a previous UTI for which no culture was performed
Suspicion of a complicated infection
Definition of a positive culture
In asymptomatic patients, the standard threshold for bacterial growth on a midstream voided urine that is reflective of bladder bacteriuria as opposed to contamination is ≥105 colony forming units (CFU)/mL.
In symptomatic women with pyuria, however, lower midstream urine counts (i.e., ≥102CFU/mL) have been associated with the presence of bladder bacteriuria. In such instances, the findings of a colony count <105 but ≥102CFU/mL may still be indicative of a UTI. Lower bacterial counts still representative of infection are also seen in men, in patients already on antimicrobials, and with organisms other than E. coli and Proteus species.
A quantitative count of at least 108 CFU/mL in a voided specimen is consistent with infection in the noncatheterized patient.82 When a urine specimen is obtained by in and out catheterization, any quantitative count of a potential uropathogen is considered consistent with infection. A quantitative count of at least 105 CFU/mL is sufficient for a microbiological diagnosis in urine specimens obtained by intermittent catheterization,54 or in patients with short-term83or long-term84 indwelling catheters.
Typically, normal values in a noninfected midstream, clean-catch sample are <105 CFU/mL, with bacterial growth primarily due to E. coli from fecal contamination.85-89 In early studies, >95% of patients with bacterial counts ≥105 CFU/mL in voided urine, but only a minority of those with lower counts had concomitant bacteriuria on a catheterized specimen.85
Subsequent studies have identified a substantial number of women with symptoms and pyuria consistent with a UTI but colony counts <105 CFU/mL in voided urine.90-96 This was demonstrated in a study of 202 premenopausal, nonpregnant women who presented with at least two symptoms of acute cystitis, collected a midstream, clean-catch urine, and subsequently underwent urethral catheterization to collect a bladder urine specimen. Of the 121 women who had E. coli grow in a catheterized specimen, 49 (40%) had counts of <105 CFU/mL in their voided urine.97 A threshold of ≥102 CFU/mL in voided specimens had a 93% positive predictive value for bladder bacteriuria with E. coli. Another study estimated that 88% of women with symptoms and a CFU count ≥102/mL on voided urine have a UTI.93
It is not well understood why some infected women have low colony counts. One possibility is that low counts reflect insufficient sensitivity of conventional urine cultures.
In a study that included 220 women with symptoms of acute cystitis and 86 asymptomatic women, urine was tested with both standard culture and quantitative polymerase chain reaction (qPCR) for E. coli, S. saprophyticus, and sexually transmitted pathogens.98 Among symptomatic women, 81% of urine cultures were positive for any uropathogen while 95% of samples were qPCR positive for E. coli (19 were positive for S. saprophyticus qPCR, 1 for Mycoplasma genitalium, and 1 for Trichomonas vaginalis). In contrast, urine culture and qPCR were positive for E. coli in only 11 and 12%, respectively. These findings suggest that almost all women with typical urinary complaints and a negative culture still have an infection with E. coli.
There are also several other settings in which a colony count of ≤105CFU/mL often represents true infection rather than contamination:
Among patients already being treated with antimicrobials.
Among men, in whom contamination is a much lesser problem.
When organisms other than E. coli and Proteus are present, included in this group are Pseudomonas, Klebsiella, Enterobacter, Serratia, and Moraxella species, particularly in symptomatic patients with an indwelling bladder catheter.
Pregnancy testing is appropriate in women of childbearing potential when the possibility of pregnancy cannot be reasonably excluded by history alone.
Blood tests, such as general chemistry and complete blood counts, are not generally necessary unless the patient is hospitalized.
Blood cultures are warranted for those who present with sepsis or severe illness.
Imaging Studies
Most patients with acute complicated UTI do not warrant imaging studies for diagnosis or management.
Imaging is generally reserved for those patients who22:
Are severely ill
Have persistent clinical symptoms despite 48 to 72 hours of appropriate antimicrobial therapy
Have suspected urinary tract obstruction (e.g., if the renal function has declined below baseline or if there is a precipitous decline in the urinary output).
Have recurrent symptoms within a few weeks of treatment
Recurrent infection may be prevented if the genitourinary abnormality that promotes infection can be corrected. The abnormality may be apparent such as:
A spinal cord injury patient managed with intermittent catheterization
A patient with an ileal conduit or nephrostomy tube
Where complicated urinary infection is suspected but abnormalities have not been defined, a diagnostic investigation to characterize the potential underlying abnormality is indicated.
The diagnostic approach will be determined by the patient history, clinical presentation and access to testing.
Diagnostic imaging may include:
Renal and pelvic ultrasound
Intravenous pyelography
Computed tomography (CT)
Magnetic resonance imaging
Urological assessment may include:
Cystoscopy
Retrograde pyelography
Urodynamic studies (UDS)
Patients presenting with severe clinical presentations such as sepsis, or those who fail to respond to initial therapy, may require urgent evaluation to exclude an obstructed urinary tract or abscess, which may require drainage.
Men who present with a first urinary infection without prior genitourinary instrumentation frequently have an abnormality identified following investigations.30
For healthy young women with recurrent cystitis or acute pyelonephritis, however, investigations have a low diagnostic yield and are not routinely recommended.99
Postmenopausal women with a new onset or increased frequency of recurrent infection should be assessed to characterize abnormalities, such as bladder diverticula or cystoceles.31
Recurrent infection following a bladder suspension or other gynecological surgery may suggest bladder outlet obstruction, and urodynamic studies may be appropriate.
Patients with a previously characterized abnormality and increased frequency or severity of symptomatic episodes may require repeat evaluation to exclude new or progressive abnormalities.
The main objective of imaging is to evaluate for a process that may delay response to therapy or warrant intervention, such as a calculus or obstruction, or to diagnose a complication of infection, such as a renal or perinephric abscess.100
Imaging should be obtained urgently in patients with sepsis or septic shock to identify any evidence of obstruction or abscess that requires urgent source control.
Computed tomography (CT) scanning of the abdomen and pelvis (with and without contrast) is generally the study of choice to detect anatomic or physiologic factors associated with acute complicated UTI. CT is more sensitive than excretory urography or renal ultrasound for detecting renal abnormalities predisposing to or caused by infection and in delineating the extent of the disease.101,102
CT without contrast has become the standard radiographic study for demonstrating102:
Abscesses
Calculi
Gas-forming infections
Hemorrhage
Obstruction
Contrast is needed to demonstrate alterations in renal perfusion.
CT findings of pyelonephritis include:
Localized hypodense lesions due to ischemia induced by marked neutrophilic infiltration and edema.101-103
The CT can be normal in patients with mild infection.104
Renal ultrasound is appropriate in patients for whom exposure to contrast or radiation is contraindicated.105
Magnetic resonance imaging (MRI) is not advantageous over CT except when avoidance of contrast dye or ionizing radiation is warranted.106
Resolution of radiographic hypodensities may lag behind clinical improvement by up to three months.101,103,107
The diagnosis of acute complicated UTI is made in the following clinical scenarios:
Symptoms of cystitis (dysuria, urinary urgency, and/or urinary frequency) along with fever (>99.9ºF/37.7ºC) or other signs or symptoms of systemic illness, such as chills, rigors, or acute mental status changes. In such cases, pyuria and bacteriuria support the diagnosis.
Flank pain and/or costovertebral angle tenderness in the setting of pyuria and bacteriuria. This is suggestive of pyelonephritis.
Fever and typical symptoms of cystitis are usually present, but their absence does not rule out the diagnosis.
CT findings that support the diagnosis include low attenuation extending to the renal capsule on contrast enhancement with or without swelling and complications such as renal abscesses. However, a normal CT does not rule out the possibility of mild pyelonephritis.
Fever or sepsis without localizing symptoms in the setting of pyuria and bacteriuria may be attributed to UTI if other causes have been ruled out. Careful clinical assessment is necessary. The diagnosis of acute complicated UTI is unlikely if pyuria is absent.
The presence of bacteriuria (≥105 CFU/mL of a uropathogen) with or without pyuria in the absence of any symptom that could be attributable to a UTI is called asymptomatic bacteriuria and generally does not warrant treatment in nonpregnant patients who are not undergoing urologic surgery.
Empiric antimicrobial therapy should be initiated promptly, taking into account risk factors for drug resistance, including previous antimicrobial use and results of recent urine cultures, with subsequent adjustment guided by antimicrobial susceptibility data. Urology should be consulted to address anatomic abnormalities if these are suspected or identified on imaging.
The decision to admit patients with acute complicated UTI should be individualized. The decision to admit is usually clear when patients are septic or otherwise critically ill. Otherwise, general indications for inpatient management include:
Outpatient management is acceptable for patients with acute complicated UTI of mild to moderate severity which can be stabilized, if necessary, with rehydration and antimicrobials in an outpatient facility or the emergency department and discharged on oral antimicrobials with close follow-up.
Many patients can be managed in the outpatient setting. As an example, in a study of 44 patients with pyelonephritis but no major comorbidities, a 12-hour observation period with parenteral antimicrobial therapy in the emergency department followed by completion of outpatient oral antimicrobials was effective management for 97% of patients.108
The approach to empiric therapy of acute complicated UTI depends on the severity of illness, the risk factors for resistant pathogens, and specific host factors.109 The choice among the options presented for each population depends on:
Drug toxicity, interactions, availability, and cost
Local community resistance prevalence of Enterobacteriaceae (if known)
Patient circumstances (such as allergy or expected tolerability and history of prior antimicrobial use)
Susceptibility of prior urinary isolates
Urine culture and susceptibility testing should be performed in all patients, and the initial empiric regimen should be tailored appropriately to the susceptibility profile of the infecting pathogen, once known.109
Data evaluating the efficacy of various regimens for acute complicated UTI are limited, and only a small number of different regimens have been formally evaluated.110,111 The recommendations in this section are based instead on the expected microbial spectrum of antimicrobial agents that achieve adequate urinary tract and systemic levels.
Table 2: Review of Therapeutic Agents Used to Treat Acute Complicated UTIs
Aminoglycoside Antibiotics
Mechanism of Action: Aminoglycosides have concentration-dependent bactericidal activity. They bind to the 30S ribosome, thereby inhibiting bacterial protein synthesis.
Agents: Gentamicin Tobramycin
Indication for usage include:
Aerobic, Gram-negative bacteria, such as:
Pseudomonas
Acinetobacter
Enterobacter
Some Mycobacteria
β-lactam Antibiotics
Mechanism of Action: β-lactam antibiotics (beta-lactam antibiotics) are a class of broad-spectrum antibiotics, consisting of all antibiotic agents that contain a beta-lactam ring in their molecular structures. Most β-lactam antibiotics work by inhibiting cell wall biosynthesis in the bacterial organism and are the most widely used group of antibiotics. Bacteria often develop resistance to β-lactam antibiotics by synthesizing a β-lactamase, an enzyme that attacks the β-lactam ring. To overcome this resistance, β-lactam antibiotics are often given with β-lactamase inhibitors such as clavulanic acid.
Class: Carbapenems
Agents: Doripenem Ertapenem Imipenem Meropenem
Indications for usage include:
Haemophilus influenzae
Anaerobes
Most Enterobacteriaceae (including those that produce ampC β-lactamase and extended-spectrum β-lactamase [ESBL], although P. mirabilis tends to have higher imipenem minimum inhibitory concentration [MICs).
Methicillin-sensitive staphylococci and streptococci, including S. pneumoniae (except possibly strains with reduced penicillin sensitivity).
Most Enterococcus faecalis and many P. aeruginosa strains, including those resistant to broad-spectrum penicillins and cephalosporins, are susceptible to imipenem, meropenem, and doripenem but are resistant to ertapenem. However, meropenem and doripenem are less active against E. faecalis than imipenem.
Carbapenems are active synergistically with aminoglycosides against P. aeruginosa. E. faecium, Stenotrophomonas maltophilia, and methicillin-resistant staphylococci are resistant.
Class: Cephalosporins
Agents:
Cefadroxil
Cefdinir
Cefepime
Cefodoxime
Ceftazidime
Ceftriaxone
Indications for usage include:
Gram-positive bacteria
Gram-negative bacteria
Class: Penicillin
Agent: Amoxicillin
Indications for usage include:
Enterococci: gram positive bacteria such as E. faecalis and E. faecium
Certain gram-negative bacilli, such as non-β-lactamase–producing H. influenzae, E. coli, and Proteus mirabilis; Salmonella spp; and Shigella spp
Mechanism of Action: Timethoprim and Sulfamethoxazole have a greater effect when given together than when given separately because they inhibit successive steps in the folate syntheses pathway. They are given in a one-to-five ratio in their tablet formulations so that when they enter the body their concentration in the blood and tissues is roughly on-to-twenty - the exact ratio required for peak synergistic effect between the two
Agent: Trimethoprim/Sulfamethoxazole (TMP-SMX)
Indications for usage include:
Gram-positive bacteria (including some methicillin-resistant Staphylococcus aureus)
A broad spectrum of gram-negative bacteria
Protozoans Cystoisospora and Cyclospora spp
The fungus Pneumocystis jirovecii.
Fluoroquinolone Antibiotics
Mechanism of Action: Fluoroquinolone, which contain a fluorine atom in their chemical structure, are effective against both Gram-negative and Gram-postive bacteria.
Mechanism of Action:Glycopeptide antibiotics are large, rigid molecules that inhibit a late stage in bacterial cell wall peptidoglycan synthesis
Agent: Vancomycin
Indications for usage include:
Most gram-positive cocci and bacilli, including almost all Staphylococcus aureus and coagulase-negative staphylococcal strains that are resistant to penicillins and cephalosporins
Many strains of enterococci (via a bacteriostatic mechanism) (However, many strains of enterococci and some strains of S. aureus are vancomycin-resistant)
Certain β-lactam – and multidrug-resistant Streptococcus pneumoniae
β-Hemolytic streptococci (when β-lactams cannot be used because of drug allergy or resistance)
Corynebacterium group JK
Viridans streptococci (when β-lactams cannot be used because of drug allergy or resistance)
Enterococci (when β-lactams cannot be used because of drug allergy or resistance)
Lipopeptide Antibiotic
Mechanism of Action: Daptomycin is a cyclic lipopeptide antibiotic that has a unique mechanism of action. It binds to the bacterial cell membranes, causing rapid depolarization of the membrane due to K efflux and associated disruption of DNA, RNA, and protein synthesis. The result is rapid concentration-dependent bacterial death.
Agent: Daptomycin
Indications for usage include:
Gram-positive bacteria (broad-spectrum activity)
Multidrug-resistant gram-positive bacteria (because cross-resistance with other classes of antibiotics does not occur)
Vancomycin-resistant Staphylococcus aureus
Vancomycin-resistant enterococci
Pneumococci with reduced penicillin sensitivity
Oxazolidinone Antibiotics
Mechanism of Action:Linezolid can be considered as teh first member of the class of oxazolidinone antibiotics. The compound is a synthetic antibiotic and inhibits bacterial protein synthesis through binding to rRNA. It also inhibits the creation of the initiation complex during protein synthesis which can reduce the length of the developed peptide chains, and decrease the rate of reaction of translation elongation.
Agent: Linezolid
Indications for usage include:
Streptococci
Enterococci (Enterococcus faecalis and E. faecium)
Staphylococci, including strains resistant to other classes of antibiotics
A broad-spectrum antimicrobial regimen is mandatory for empiric therapy of patients with acute complicated UTI who are:
Critically ill (i.e., with sepsis or otherwise warranting intensive care unit admission)
Getting worse on current therapy
Suspected to have a urinary tract obstruction (e.g., if the renal function has declined below baseline or if there is a decline in urine output).
In such patients, an antipseudomonal carbapenem to cover extended-spectrum beta-lactamase (ESBL)-producing organisms and Pseudomonas aeruginosa, is advocated. Select ONE of the following.?
*Doses listed are for patients with normal renal function and may require adjustment in the setting of renal impairment.
Imipenem 500 mg intravenously (IV) every six hours
Meropenem 1 gram IV every eight hours
Doripenem 500 mg IV every eight hours
PLUS Vancomycin 15 mg/kg IV every 12 hours to cover MRSA.
Alternatives to Vancomycin are:
Daptomycin 6 mg/kg IV every 24 hours OR
Linezolid 600 mg IV every 12 hours
Other therapeutic agents which also have activity against some ESBL-producing and multidrug-resistant P. aeruginosa isolates and are effective for acute complicated UTI are112-114:
Advanced cephalosporin or carbapenem combinations with beta-lactamase inhibitors such as:
Ceftazidime-avibactam
Ceftolozane-tazobactam
Meropenem-vaborbactam
Because of cost and antimicrobial stewardship concerns, these therapeutic agents should only be used in select cases of highly resistant infections.
If carbapenem resistance is suspected based on prior susceptibility testing results, an infectious diseases consult should be obtained.
The rationale for such broad coverage is that these critically ill patients who are at high risk of adverse outcomes should the empiric antimicrobial therapy be insufficient and the increasing prevalence of multidrug-resistant organisms, even in the general population. Patients who have a UTI in the setting of urinary tract obstruction are at a particularly high risk of clinical decompensation. Such patients also warrant imaging to evaluate for obstruction or other complications that may warrant intervention.
Results of urine culture and susceptibility testing should be followed to ensure that the chosen empiric antimicrobial regimen is appropriate and to guide selection of definitive therapy.
For patients who are hospitalized for acute complicated UTI but are not critically ill and do not have suspected urinary tract obstruction, the recommended approach to empiric antimicrobial regimen selection depends on the risk for infection with multidrug-resistant (MDR) gram-negative organisms. (Table 3)
Suspect MDR Gram-negative UTI in Patients with a History of the following in the past 3 Months:
A MDR gram-negative urinary isolate
Inpatient stay in a health care facility (e.g., hospital, nursing home, long-term acute care facility)
Use of fluoroquinolone, TMP-SMX, or broad-spectrum beta-lactam (e.g., third or later generation cephlalosporin)**
Travel to parts of the world with high rates of multidrug-resistant organisms (e.g., India, Israel, Spain, Mexico)
*Multidrug resistance refers to nonsusceptibility to at least one agent in three or more antibiotic classes. This includes isolates that produce an extended-spectrum beta-lactamase (ESBL)
** This includes a single antibiotic dose given for prophylaxis prior to prostate procedures.
No risk factors for infection with a MDR gram-negative organism:
Ceftriaxone (1 gram IV once daily) OR
Piperacillin-tazobactam (3.375 grams IV every 6 hours) for parenteral treatment because of their safety profile and narrow spectrum compared with other parenteral agents.
Oral or parenteral fluoroquinolones (ciprofloxacin or levofloxacin) are also reasonable alternatives if the patient has not had a urinary isolate resistant to fluoroquinolones in the prior three months and the community prevalence of E. coli fluoroquinolone resistance is not known to be higher than 10%.
Ciprofloxacin 400 mg IV every 12 hours
Ciprofloxacin 500 mg orally every 12 hours
Ciprofloxacin extended-release 1000 mg orally once daily
Levofloxacin 750 mg IV once daily
Levofloxacin 750 mg orally once daily
Concern for particular pathogens should further inform the choice between these options.
If Enterococcus or Staphylococcus species are suspected (e.g., because of prior urinary isolates or gram-positive cocci on a current urine Gram stain), piperacillin-tazobactam is preferred because it has activity against these organisms
If the patient cannot use piperacillin-tazobactam because of allergies or otherwise, Vancomycin plus one of the other gram-negative agents can be used.
If drug-resistant gram-positive organisms are suspected because of previous urinary isolates or other risk factors add:
Vancomycin (for MRSA) OR
Linezolid (for VRE) OR
Daptomycin (for VRE)
If there is a risk of P. aeruginosa (e.g., because of prior urinary isolates or febrile neutropenia) choose:
Piperacillin-tazobactam at a higher dose (4.5 grams IV every 6 hours) OR
A fluoroquinolone
Other antipseudomonal agents that can be used include:
Cefepime 2 grams IV every 8 hours and
Ceftazidime 2 grams IV every 8 hours
At least one risk factor for infection with a MDR gram-negative organism.
Empiric treatment with an antipseudomonal carbapenem:
Imipenem 500 mg IV every 6 hours OR
Meropenem 1 gram IV every 8 hours OR
Doripenem 500 mg IV every 8 hours
If Enterococcus species or MRSA are suspected because of prior urinary isolates or gram-positive cocci on a current urine gram stain add:
Vancomycin (for MRSA) OR
Daptomycin (for VRE) OR
Linezolid (for VRE)
Advanced cephalosporin or carbapenem combinations with beta-lactamase inhibitors such as ceftazidime-avibactam, ceftolozane-tazobactam, and meropenem-vaborbactam also have activity against some ESBL-producing and multidrug-resistant P. aeruginosa isolates and are effective for acute complicated UTI,112-114 but because of cost and antimicrobial stewardship concerns, they should only be used in select cases of highly resistant infections.
If carbapenem resistance is suspected based on prior susceptibility testing results, an infectious diseases consult should be obtained.
Results of urine culture and susceptibility testing should be followed to ensure that the chosen empiric antimicrobial regimen is appropriate and to guide selection of definitive therapy.
Patients who can be treated in an outpatient setting with acute complicated UTI include:
Acute complicated UTI of mild to moderate severity
Patients who can take oral medications reliably
The approach to the selection of an empiric outpatient antimicrobial regimen depends on the risk factors for infection with a MDR organism (in particular ESBL-producing isolates).
Whether fluoroquinolones can be used (accounting for contraindications or concerns for fluoroquinolone resistance specifically) is also an important consideration in regimen selection.
In the absence of resistance, fluoroquinolones provide a broad spectrum of antimicrobial activity against most uropathogens (including P. aeruginosa) and achieve high levels in the urinary tract. Studies of acute complicated UTI have shown that the fluoroquinolones are generally comparable or superior to other broad-spectrum antimicrobials, including parenteral regimens.110,115 However, increasing rates of resistance to fluoroquinolones among uropathogens, even among outpatients, are diminishing their value for this purpose.116
When a fluoroquinolone can be used:
Ciprofloxacin-most common agent
Levofloxacin-most common agent
Other less commonly used fluoroquinolones that are effective for UTIs include:
Ofloxacin
Norfloxacin
Moxifloxacin attains lower urinary levels than other fluoroquinolones and should not be used.
Although there are concerns about the potential adverse effects, including Clostridium difficile infection and ecological effects (i.e., selection of resistant organisms) of the fluoroquinolones, their benefits are thought to outweigh their risks for acute complicated UTI.
For outpatients with acute complicated UTI and no risk factors for infection with an MDR gram-negative organism (Table 3 above), empiric antimicrobial regimen selection depends on contraindications to or other concerns with fluoroquinolones. These include:
Allergy or intolerance to the fluoroquinolone class (including prolonged QT interval or other risk factors for torsades de pointes) OR
An unmodifiable drug interaction
Fluoroquinolone-Based Regimens
For patients who have no contraindications to fluoroquinolone and are at low personal risk for a fluoroquinolone-resistant isolate, an oral fluoroquinolone for empiric therapy is suggested. Appropriate regimens include117-121:
Ciprofloxacin 500 mg orally every 12 hours for 5 to 7 days OR
Ciprofloxacin 1000 mg extended release once daily for 5 to 7 days OR
Levofloxacin 750 mg once daily for 5 to 7 days
In the case that community prevalence of E. coli fluoroquinolone resistance is known to be higher than 10%, a single dose of a long-acting parenteral agent prior to administering the fluoroquinolone is suggested122:
Ceftriaxone (1 gram IV or IM once) because of its safety, efficacy, and microbial spectrum.
Ertopenem (1 gram IV or IM once) is an alternative for patients with an allergy that precludes ceftriaxone use or expected resistance to ceftriaxone.
Aminoglycosides (gentamicin or tobramycin 5 mg per kg IV or IM once) are reserved for patients who cannot use the other two.
Since timely use of an agent with in vitro activity is essential to treat acute complicated UTI and minimize progression of infection, the threshold for selecting an antimicrobial for empiric broad-spectrum therapy should be set at a relatively low resistance prevalence. For fluoroquinolones, a resistance prevalence of 10% has been suggested based on expert opinion.109
The benefits of fluoroquinolones are thought to outweigh their risks for acute complicated UTI, but patients should be advised about the uncommon but potentially serious musculoskeletal and neurologic adverse effects associated with fluoroquinolones.
Fluoroquinolone-Sparing Regimens
For patients who have contraindications to fluoroquinolones or other concerns about fluoroquinolone use, the approach depends on the relative severity of illness. For those with mild infection, a single dose of a long-acting parenteral agent is suggested followed by a non-fluoroquinolone oral agent.122
Ceftriaxone (1 gram IV or IM once) as a long-acting parenteral agent because of its safety, efficacy, and microbial spectrum.
Ertapenem (1 gram IV or IM once) is an alternative for patients with an allergy that precludes ceftriaxone use or expected resistance to ceftriaxone.
Aminoglycosides (gentamicin OR tobramycin 5 mg per kg IV or IM once) are reserved for patients who cannot use the other two.
Following the dose of the parenteral agent, options include the following:
TMP-SMX – one double-strength (160 mg/800 mg) tablet orally every 12 hours for 7 to 10 days
Amoxicillin-clavulanate – 875 mg orally every 12 hours for 10 to 14 days
Cefpodoxime – 200 mg orally every 12 hours for 10 to 14 days
Cefdinir – 300 mg orally every 12 hours for 10 to 14 days
Cefadroxil – 1 g orally every 12 hours for 10 to 14 days
For outpatients who are more ill or are at risk for more severe illness, continuing the parenteral therapy pending culture results is reasonable.
Results of urine culture and susceptibility testing should be followed to ensure that the chosen empiric antimicrobial regimen is appropriate and to guide modification of the regimen, if necessary.
For outpatients with acute complicated UTI and risk factors for infection with a MDR gram-negative organism (Table 3 above), an initial dose of ertapenem 1 gram IV or IM is suggested.
For patients who have no contraindications to fluoroquinolones (i.e., allergy or expected intolerability, including risk factors for torsades de pointes, or unmodifiable drug interaction) and have not had fluoroquinolone use or a fluoroquinolone-resistant urinary isolate in the prior three months, this dose of ertapenem is followed by a fluoroquinolone such as117-121:
Ciprofloxacin 500 mg orally every 12 hours for 5 to 7 days
Ciprofloxacin 1000 mg extended release orally once daily for 5 to 7 days
Levofloxacin 750 mg once daily for 5 to 7 days
The benefits of fluoroquinolones are thought to outweigh their risks for acute complicated UTI, but patients should be advised about the uncommon but potentially serious musculoskeletal and neurologic adverse effects associated with fluoroquinolones.
For patients who have either contraindications or concern for fluoroquinolone resistance, administration of ertapenem 1 gram IV or IM daily in the outpatient setting until culture and susceptibility testing results return. Once available, these results should guide selection of definitive therapy.
Results of urine culture and susceptibility testing should be used to confirm that the chosen empiric regimen is active and to tailor the regimen, if appropriate. In many cases, broad-spectrum empiric regimens can be replaced by a more narrow-spectrum agent.
Patients who were initially treated with a parenteral regimen can be switched to an oral agent once symptoms have improved, as long as culture and susceptibility testing allows. Appropriate oral agents to treat acute complicated UTI include117-119:
Levofloxacin 750 mg orally once daily for 5 to 7 days
Ciprofloxacin 500 mg orally every 12 hours OR 1000 mg extended release once daily for 5 to 7 days
TMP-SMX – one double-strength (160 mg/800 mg) tablet orally every 12 hours for 7 to 10 days
Oral beta-lactams are less effective for acute complicated UTI but are appropriate alternatives if susceptibility is documented and the other agents are not feasible. If Enterococcus is isolated, amoxicillin (500 mg orally every eight hours OR 875 mg orally every 12 hours) is the agent of choice if the organism is susceptible.123
Occasionally, susceptibility results preclude the use of an oral regimen, and a parenteral agent is needed to complete the course of treatment. Options for outpatient administration of parenteral antimicrobials include the use of a peripherally inserted central catheter, a preexisting central catheter, or IM injection.
Total duration of antimicrobial therapy generally ranges from 5 to 14 days, depending on the rapidity of clinical response and the antimicrobial chosen to complete the course.124
Fluoroquinolones are given for 5 to 7 days
TMP-SMX are given for 7 to 10 days
Beta-lactams are given for 10 to 14 days
Longer durations may be warranted in patients who have a nidus of infection (such as a nonobstructing stone) that cannot be removed. The duration of antimicrobial therapy need not be extended in the setting of bacteremia in the absence of other complicating factors. There is no evidence that bacteremia portends a worse prognosis.125
Several trials have indicated that five- or seven-day regimens of fluoroquinolones are comparable to longer durations.118,126 There are limited data evaluating the use of other oral agents for acute complicated UTI.124,127,128
In addition to antimicrobial therapy, the possibility of urinary obstruction should be considered and managed, if identified. Patients who have underlying anatomical or functional urinary tract abnormalities (including neurogenic bladder, indwelling bladder catheters, nephrostomy tubes, urethral stents) may warrant additional management, such as more frequent catheterization to improve urinary flow, exchange or removal of a catheter, and/or urologic or gynecologic consultation. Antimicrobials alone may not be successful unless such underlying conditions are corrected.129
Symptoms should improve promptly if antimicrobial therapy is effective. Among patients treated as outpatients, those who had pyelonephritis should have close follow-up either face-to-face or by telephone within 48 to 72 hours.
Any patients who have worsening symptoms following initiation of antimicrobials, persistent symptoms after 48 to 72 hours of appropriate antimicrobial therapy, or recurrent symptoms within a few weeks of treatment should have additional evaluation, including abdominal/pelvic imaging (generally with computed tomography if not already performed) for factors that might be compromising clinical response. Urine culture and susceptibility testing should be repeated, and treatment should be tailored to the susceptibility profile of other causative organisms isolated.
The major strategy to prevent complicated UTI involves characterizing and correcting the underlying genitourinary abnormality that promotes infection. When correction is not possible, patients with persistent abnormalities remain at risk for recurrent infection. Clinical trials of prophylactic antimicrobial therapy suggest this approach is ultimately unsuccessful due to reinfection with resistant organisms.
Prospective, randomized trials of prophylactic antimicrobial therapy have been reported for patients with short-term indwelling catheters130,132 and spinal cord injury patients.133,134 While a decrease in the frequency of symptomatic infection may initially occur, emergence of resistant organisms ultimately limits efficacy.131,133 Currently, there are no adult populations at risk for recurrent complicated UTI in whom long-term prophylaxis to prevent urinary infection is routinely recommended.
A prospective, randomized, placebo-controlled crossover trial of cranberry tablets three times daily to prevent infection in spinal cord injury patients reported no impact of cranberry products on bacteriuria or pyuria.135 However, a randomized, controlled trial of an educational program designed to reduce urinary infection in spinal cord injured patients demonstrated significantly lower bacterial counts and a trend to fewer symptomatic episodes in subjects randomized to the educational intervention.136 The elements of the educational program included written material, a self-administered test of bladder management, review of catheter technique by an experienced nurse, discussion with a physician about accessing care for urinary infection, and follow-up by telephone. The observed improvement continued for at least six months.
Investigations of different antibacterial catheter materials and coatings to prevent infection in patients with indwelling urological devices, including urethral catheters, have not shown consistent benefit.13,137 Antibacterial substances added to the catheter drainage bag do not prevent symptomatic infection138-140 and daily periurethral care with either soap and water or antiseptics does not decrease infection acquisition in patients with indwelling catheters.141-143 Future developments in catheter biomaterials to inhibit biofilm formation may limit biofilm-associated infections, but benefits from this approach have not yet been realized for clinical practice.144
The term acute complicated UTI refers to an acute UTI with any features that suggest that the infection extends beyond the bladder. These include fever (e.g., >99.9°F/37.7°C), other signs or symptoms of systemic illness (including chills, rigors, or altered mental status), flank pain, and costovertebral angle tenderness. By this definition, pyelonephritis is a complicated UTI, regardless of patient characteristics. This definition is distinct from traditional categorizations of UTI and is more focused on the clinical presentation and severity of illness.
Relevant uropathogens include primarily Escherichia coli, but also other Enterobacteriaceae, other gram-negative bacilli (including Pseudomonas aeruginosa), staphylococci, enterococci, and Candida species. Risk factors for resistant organisms include recent broad-spectrum antimicrobial use, health care exposures, and travel to parts of the world where multidrug-resistant organisms are prevalent.
Acute complicated UTI should be suspected in patients with dysuria, urinary frequency or urgency, or suprapubic pain who also have fever, chills, flank pain, or otherwise appear clinically ill. Acute pyelonephritis, specifically, should be suspected in patients presenting with fever and flank pain, even in the absence of typical symptoms of cystitis. In men, pelvic or perineal pain accompanying urinary symptoms suggests prostatitis. UTI is also often suspected in patients with pyuria and bacteriuria who have nonspecific signs of systemic illness, such as lethargy or delirium, and in patients with nonlocalizing fever or sepsis.
For patients with suspected acute complicated UTI, urine should be sent for both urinalysis (either by microscopy or by dipstick) and culture with susceptibility testing. Imaging is generally reserved for those who are severely ill, have suspected urinary tract obstruction, have persistent symptoms despite 48 to 72 hours of appropriate antimicrobial therapy, or have recurrent symptoms.
The diagnosis of acute complicated UTI is made in patients who have consistent clinical findings, as well as, pyuria and bacteriuria. UTI is unlikely if pyuria is absent.
Outpatient management is acceptable for patients with acute complicated UTI of mild to moderate severity which can be stabilized, if necessary, with rehydration and antimicrobials in an outpatient facility or the emergency department and discharged on oral antimicrobials with close follow-up.
The approach to empiric therapy of acute complicated UTI depends on the severity of illness, the risk factors for resistant pathogens, and specific host factors.
For patients who are critically ill or have urinary tract obstruction, an antipseudomonal carbapenem plus vancomycin is suggested.
For other hospitalized patients, ceftriaxone or piperacillin-tazobactam are suggested if there are no risk factors for a MDR gram-negative infection. Oral or parenteral fluoroquinolones are also reasonable options. For such patients who have risk factors for an MDR gram-negative infection, an antipseudomonal carbapenem is suggested.
For outpatients without risk factors for an MDR gram-negative infection an oral fluoroquinolone, such as levofloxacin or ciprofloxacin is suggested. If the community prevalence of E. coli fluoroquinolone resistance is known to be higher than 10%, a single dose of a long-acting parenteral agent prior to administering the fluoroquinolone is suggested.
For outpatients with risk factors for an MDR gram-negative infection, an initial dose of Ertapenem is suggested. Subsequently, an oral fluoroquinolone or daily ertapenem can be used.
Results of urine culture and susceptibility testing should be used to confirm that the chosen empiric regimen is active and to tailor the regimen, including switching a parenteral regimen to an oral agent once symptoms have improved. Appropriate oral agents to treat acute complicated UTI include fluoroquinolones (e.g., levofloxacin or ciprofloxacin given for 5 to 7 days) and Trimethoprim-sulfamethoxazole given for 7 to 10 days. Oral beta-lactams (given for 10 to 14 days) are less effective for acute complicated UTI but are appropriate alternatives if susceptibility is documented and the other agents are not feasible.
Patients who have underlying anatomical or functional urinary tract abnormalities (including neurogenic bladder, indwelling bladder catheters, nephrostomy tubes, urethral stents) may warrant additional management, such as more frequent catheterization to improve urinary flow, exchange or removal of a catheter, and/or urologic or gynecologic consultation.
Mrs. Vinge is a 63-year-old, retired, widowed, not sexually active, Caucasian female who comes to Urgent Care with c/o increasing fatigue, lower back pain with fevers to 103.5? self-treated with Tylenol 500 mg po every 12 hours for the past three days. This morning upon first urination she reports gross hematuria. Denies frequency, urgency, dysuria, vaginal discharge. The patient denies vaginal discharge or itching. No sexual activity in the past 20 years. LMP 1999. No travel outside of the country since 2006. No urinary procedures entire lifetime. She denies prior UTI’s entire lifetime.
PMH: Osteoporosis-diagnosed 2005 C-section March 1979 T&A 1955
NKDA
Current medications: Ibandronate sodium 150 mg once a month Vitamin D po q day Tylenol 500 mg prn Motrin 200 mg prn
Physical examination: Febrile: 102.5 po-last Tylenol 4 hours ago. Neuro: Alert, oriented, cooperative, follows all commands appropriately. PERRLA. HEENT: WNL Lungs: CTA. No rales, rhonchi or wheezes. Cardiac: HR 100 regular, regularity. No murmurs nor rubs. BP 130-140/70-84. Abdominal: Abdomen soft, non-tender with bowel sound in all quadrants. Costovertebral angle tenderness bilaterally. GU: Urine cloudy with gross hematuria. PVS: No edema.
Patient is considered to be low risk for infection with a MDR gram-negative organism. Since the community prevalence of fluoroquinolone resistance in E. Coli is <10%, Ciprofloxacin 500 mg orally twice daily for 7 days is prescribed. Follow-up with Primary Care physician in seven days or sooner should symptoms worsen.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Kline KA, Schwartz DJ, Lewis WG, Hultgren SJ, Lewis AL. Immune activation and suppression by group B Streptococcus in a murine model of urinary tract infection. Infect Immun. 2011;79:3588–3595.
Ronald A. The etiology of urinary tract infection: traditional and emerging pathogens. Am J Med. 2002;113 (Suppl 1A):14S–19S.
Levison ME, Kaye D. Treatment of complicated urinary tract infections with an emphasis on drug-resistant Gram-negative uropathogens. Curr Infect Dis Rep. 2013;15:109–115.
Fisher JF, Kavanagh K, Sobel JD, Kauffman CA, Newman C. A Candida urinary tract infection: pathogenesis. Clin Infect Dis. 2011;52 (Suppl 6):S437–S451.
Chen YH, Ko WC, Hsueh PR. Emerging resistance problems and future perspectives in pharmacotherapy for complicated urinary tract infections. Expert Opin Pharmacother. 2013;14:587–596.
Jacobsen SM, Stickler DJ, Mobley HL, Shirtliff ME. Complicated catheter-associated urinary tract infections due to Escherichia coli and Proteus mirabilis. Clin Microbiol Rev. 2008;21:26–59.
Nicolle LE. Asymptomatic bacteriuria in the elderly. Infect Dis Clin North Am 1997;11:647-67.
Bakke A, Digranes A. Bacteriuria in patients treated with clean intermittent catheterization. Scand J Infect Dis 1991;23:577-82.
Bennett CJ, Young MN, Darrington H. Differences in urinary tract infections in male and female spinal cord injury patients on intermittent catheterization. Paraplegia 1995;33:69-72.
Kostakioti M, Hultgren SJ, Hadjifrangiskou M. Molecular blueprint of uropathogenic Escherichia colivirulence provides clues toward the development of anti-virulence therapeutics. Virulence. 2012;3:592–594.
Paterson DL. Resistance in Gram-negative bacteria: Enterobacteriaceae. Am J Infect Control. 2006;34:S20–S28.
Garau J. Other antimicrobials of interest in the era of extended-spectrum β-lactamases: fosfomycin, nitrofurantoin and tigecycline. Clin Microbiol Infect. 2008;14:198–202.
Pendleton JN, Gorman SP, Gilmore BF. Clinical relevance of the ESKAPE pathogens. Expert Rev Anti Infect Ther. 2013;11:297–308.
Gupta K, Bhadelia N. Management of urinary tract infections from multidrug-resistant organisms. Infect Dis Clin North Am. 2014;28:49–59.
Bradford PA. Extended-spectrum β-lactamases in the 21st century: characterization, epidemiology, and detection of this important resistance threat. Clin Microbiol Rev. 2001;14:933–951.
Hannan TJ, et al. Host–pathogen checkpoints and population bottlenecks in persistent and intracellular uropathogenic Escherichia coli bladder infection. FEMS Microbiol Rev. 2012;36:616–648.
Subashchandranose S, et al. Host-specific induction of Escherichia coli fitness genes during human urinary tract infection. Proc Natl Acad Sci USA. 2014;111:18327–18332.
Lo E, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35:464–479.
Chenoweth CE, Gould CV, Saint S. Diagnosis, management, and prevention of catheter-associated urinary tract infections. Infect Dis Clin North Am. 2014;28:105–119.
Nicolle LE. A practical approach to the management of complicated urinary tract infection. Drugs and Aging 2001;18:243-54.
Nicolle LE. The chronic indwelling catheter and urinary infection in long-term-care facility residents. Infect Control Hosp Epidemiol 2001;22:316-21.
Lipsky BA. Urinary tract infections in men. Epidemiology, pathophysiology, diagnosis, and treatment. Ann Intern Med 1989;110:138-50.
Raz R, Gennesin Y, Wasser J, et al. Recurrent urinary tract infections in postmenopausal women. Clin Infect Dis 2000;30:152-6.
Khawcharoenporn T, Vasoo S, Singh K. Urinary Tract Infections due to Multidrug-Resistant Enterobacteriaceae: Prevalence and Risk Factors in a Chicago Emergency Department. Emerg Med Int 2013; 2013:258517.
Killgore KM, March KL, Guglielmo BJ. Risk factors for community-acquired ciprofloxacin-resistant Escherichia coli urinary tract infection. Ann Pharmacother 2004; 38:1148.
Walker E, Lyman A, Gupta K, et al. Clinical Management of an Increasing Threat: Outpatient Urinary Tract Infections Due to Multidrug-Resistant Uropathogens. Clin Infect Dis 2016; 63:960.
Smithson A, Chico C, Ramos J, et al. Prevalence and risk factors for quinolone resistance among Escherichia coli strains isolated from males with community febrile urinary tract infection. Eur J Clin Microbiol Infect Dis 2012; 31:423.
Linsenmeyer K, Strymish J, Gupta K. Two Simple Rules for Improving the Accuracy of Empiric Treatment of Multidrug-Resistant Urinary Tract Infections. Antimicrob Agents Chemother 2015; 59:7593.
Zilberberg MD, Shorr AF. Secular trends in gram-negative resistance among urinary tract infection hospitalizations in the United States, 2000-2009. Infect Control Hosp Epidemiol 2013; 34:940.
Talan DA, Takhar SS, Krishnadasan A, et al. Fluoroquinolone-Resistant and Extended-Spectrum β-Lactamase-Producing Escherichia coli Infections in Patients with Pyelonephritis, United States(1). Emerg Infect Dis 2016; 22.
Lautenbach E. Editorial commentary: flying under the radar: the stealth pandemic of Escherichia coli sequence type 131. Clin Infect Dis 2013; 57:1266.
Colpan A, Johnston B, Porter S, et al. Escherichia coli sequence type 131 (ST131) subclone H30 as an emergent multidrug-resistant pathogen among US veterans. Clin Infect Dis 2013; 57:1256.
Fairley KF, Carson NE, Gutch RC, et al. Site of infection in acute urinary-tract infection in general practice. Lancet 1971; 2:615.
Cardenas DD, Hooton TM. Urinary tract infection in persons with spinal cord injury. Arch Phys Med Rehabil 1995;76:272-80.
Dembry LM, Andriole VT. Renal and perirenal abscesses. Infect Dis Clin North Am 1997;11:663-80.
Patterson JE, Andriole VT. Bacterial urinary tract infections in diabetes. Infect Dis Clin North Am1997;11:735-50.
Trop CS, Bennett CJ. Autonomic dysreflexia and its urological implications: A review. J Urol1991;146:1461-9.
Rapp NS, Gilroy J, Lerner AM. Role of bacterial infection in exacerbation of multiple sclerosis. Am J Phys Med Rehabil 1995;74:415-8.
Nicolle LE. Consequences of asymptomatic bacteriuria in the elderly. Int J Antimicrob Agents1994;4:107-11.
Orr P, Nicolle LE, Duckworth H, et al. Febrile urinary infection in the institutionalized elderly. Am J Med 1996;100:71-7.
Potts L, Cross S, MacLennan WJ, Watt B. A double-blind comparative study of norfloxacin versus placebo in hospitalised elderly patients with asymptomatic bacteriuria. Arch Gerontol Geriatr 1996; 23:153.
Dasgupta M, Brymer C, Elsayed S. Treatment of asymptomatic UTI in older delirious medical in-patients: A prospective cohort study. Arch Gerontol Geriatr 2017; 72:127.
Sundvall PD, Elm M, Ulleryd P, et al. Interleukin-6 concentrations in the urine and dipstick analyses were related to bacteriuria but not symptoms in the elderly: a cross sectional study of 421 nursing home residents. BMC Geriatr 2014; 14:88.
Sundvall PD, Ulleryd P, Gunnarsson RK. Urine culture doubtful in determining etiology of diffuse symptoms among elderly individuals: a cross-sectional study of 32 nursing homes. BMC Fam Pract 2011; 12:36.
Tambyah PA, Maki DG. The relationship between pyuria and infection in patients with indwelling urinary catheters: A prospective study of 761 patients. Arch Intern Med 2000;160:673-82.
Gribble MJ, McCallum NM, Schechter MT. Evaluation of diagnostic criteria for bacteriuria in acutely spinal cord injured patients undergoing intermittent catheterization. Diagn Microbiol Infect Dis1988;9:197-206.
Monane M, Gurwitz JH, Lipsitz LA, Glynn RJ, Choodnovskiy I, Avorn J. Epidemiologic and diagnostic aspects of bacteriuria: A longitudinal study in older women. J Am Geriatr Soc 1995;43:618-22.
Ouslander JG, Schapira M, Fingold S, Schnelle J. Accuracy of rapid urine screening tests among incontinent nursing home residents with asymptomatic bacteriuria. J Am Geriatr Soc 1995;43:772-5.
LaRocco MT, Franek J, Leibach EK, et al. Effectiveness of Preanalytic Practices on Contamination and Diagnostic Accuracy of Urine Cultures: a Laboratory Medicine Best Practices Systematic Review and Meta-analysis. Clin Microbiol Rev 2016; 29:105.
Baerheim A, Digranes A, Hunskaar S. Evaluation of urine sampling technique: bacterial contamination of samples from women students. Br J Gen Pract 1992; 42:241.
Lifshitz E, Kramer L. Outpatient urine culture: does collection technique matter? Arch Intern Med 2000; 160:2537.
Schneeberger C, van den Heuvel ER, Erwich JJ, et al. Contamination rates of three urine-sampling methods to assess bacteriuria in pregnant women. Obstet Gynecol 2013; 121:299.
Gupta K, Trautner B. In the clinic. Urinary tract infection. Ann Intern Med 2012; 156:ITC3.
Hooton TM. Clinical practice. Uncomplicated urinary tract infection. N Engl J Med 2012; 366:1028.
Bent S, Nallamothu BK, Simel DL, et al. Does this woman have an acute uncomplicated urinary tract infection? JAMA 2002; 287:2701.
Koeijers JJ, Kessels AG, Nys S, et al. Evaluation of the nitrite and leukocyte esterase activity tests for the diagnosis of acute symptomatic urinary tract infection in men. Clin Infect Dis 2007; 45:894.
McNeeley SG, Baselski VS, Ryan GM. An evaluation of two rapid bacteriuria screening procedures. Obstet Gynecol 1987; 69:550.
Pfaller MA, Koontz FP. Laboratory evaluation of leukocyte esterase and nitrite tests for the detection of bacteriuria. J Clin Microbiol 1985; 21:840.
Pappas PG. Laboratory in the diagnosis and management of urinary tract infections. Med Clin North Am 1991; 75:313.
Williams GJ, Macaskill P, Chan SF, et al. Absolute and relative accuracy of rapid urine tests for urinary tract infection in children: a meta-analysis. Lancet Infect Dis 2010; 10:240.
Devillé WL, Yzermans JC, van Duijn NP, et al. The urine dipstick test useful to rule out infections. A meta-analysis of the accuracy. BMC Urol 2004; 4:4.
St John A, Boyd JC, Lowes AJ, Price CP. The use of urinary dipstick tests to exclude urinary tract infection: a systematic review of the literature. Am J Clin Pathol 2006; 126:428.
Little P, Turner S, Rumsby K, et al. Dipsticks and diagnostic algorithms in urinary tract infection: development and validation, randomised trial, economic analysis, observational cohort and qualitative study. Health Technol Assess 2009; 13:iii.
Meister L, Morley EJ, Scheer D, Sinert R. History and physical examination plus laboratory testing for the diagnosis of adult female urinary tract infection. Acad Emerg Med 2013; 20:631.
Little P, Turner S, Rumsby K, et al. Validating the prediction of lower urinary tract infection in primary care: sensitivity and specificity of urinary dipsticks and clinical scores in women. Br J Gen Pract 2010; 60:495.
Hessdoerfer E, Jundt K, Peschers U. Is a dipstick test sufficient to exclude urinary tract infection in women with overactive bladder? Int Urogynecol J 2011; 22:229.
Stamm WS. Catheter-associated urinary tract infections. Epidemiology, pathogenesis and prevention. Am J Med 1991;91(Suppl B):65S-71S.
33. Riedl CR, Plas E, Hubner WA, Zimmerl H, Ulrich W, Pfluger H. Bacterial colonization of ureteral stents. Eur Urol 1999;36:53-9.
Wilson ML, Gaido L. Laboratory diagnosis of urinary tract infections in adult patients. Clin Infect Dis 2004; 38:1150.
Gupta K, Hooton TM, Roberts PL, Stamm WE. Patient-initiated treatment of uncomplicated recurrent urinary tract infections in young women. Ann Intern Med 2001; 135:9.
Czaja CA, Scholes D, Hooton TM, Stamm WE. Population-based epidemiologic analysis of acute pyelonephritis. Clin Infect Dis 2007; 45:273.
Gupta K, Hooton TM, Roberts PL, Stamm WE. Short-course nitrofurantoin for the treatment of acute uncomplicated cystitis in women. Arch Intern Med 2007; 167:2207.
McKinnell JA, Stollenwerk NS, Jung CW, Miller LG. Nitrofurantoin compares favorably to recommended agents as empirical treatment of uncomplicated urinary tract infections in a decision and cost analysis. Mayo Clin Proc 2011; 86:480.
Rubin RH, Shapiro ED, Andriole VT, Davis RJ, Stamm WE. Evaluation of new anti-infective drugs for the treatment of urinary tract infection. Infectious Diseases Society of America and the Food and Drug Administration. Clin Infect Dis 1992;15(Suppl 1):S216-27.
Stark RP, Maki DG. Bacteriuria in the catheterized patient. What quantitative level of bacteriuria is relevant? N Engl J Med 1984;311:560-4.
Tenney JH, Warren JW. Bacteriuria in women with long-term catheters: Paired comparison of indwelling and replacement catheters. J Infect Dis 1988;157:199-202. (Erratum in 1988;157:1112).
Kass EH. Asymptomatic infections of the urinary tract. Trans Assoc Am Physicians 1956; 69:56.
Platt R. Quantitative definition of bacteriuria. Am J Med 1983; 75:44.
Pollock HM. Laboratory techniques for detection of urinary tract infection and assessment of value. Am J Med 1983; 75:79.
Sanford JP, Favour CB, Mao FH, Harrison JH. Evaluation of the positive urine culture; an approach to the differentiation of significant bacteria from contaminants. Am J Med 1956; 20:88.
Tapsall JW, Taylor PC, Bell SM, Smith DD. Relevance of "significant bacteriuria" to aetiology and diagnosis of urinary-tract infection. Lancet 1975; 2:637.
Stamm WE, Wagner KF, Amsel R, et al. Causes of the acute urethral syndrome in women. N Engl J Med 1980; 303:409.
Kunin CM, White LV, Hua TH. A reassessment of the importance of "low-count" bacteriuria in young women with acute urinary symptoms. Ann Intern Med 1993; 119:454.
Komaroff AL. Acute dysuria in women. N Engl J Med 1984; 310:368.
Stamm WE, Counts GW, Running KR, et al. Diagnosis of coliform infection in acutely dysuric women. N Engl J Med 1982; 307:463.
Naber KG, Schito G, Botto H, et al. Surveillance study in Europe and Brazil on clinical aspects and Antimicrobial Resistance Epidemiology in Females with Cystitis (ARESC): implications for empiric therapy. Eur Urol 2008; 54:1164.
De Backer D, Christiaens T, Heytens S, et al. Evolution of bacterial susceptibility pattern of Escherichia coli in uncomplicated urinary tract infections in a country with high antibiotic consumption: a comparison of two surveys with a 10 year interval. J Antimicrob Chemother 2008; 62:364.
Heytens S, Boelens J, Claeys G, et al. Uropathogen distribution and antimicrobial susceptibility in uncomplicated cystitis in Belgium, a high antibiotics prescribing country: 20-year surveillance. Eur J Clin Microbiol Infect Dis 2017; 36:105.
Hooton TM, Roberts PL, Cox ME, Stapleton AE. Voided midstream urine culture and acute cystitis in premenopausal women. N Engl J Med 2013; 369:1883.
Heytens S, De Sutter A, Coorevits L, et al. Women with symptoms of a urinary tract infection but a negative urine culture: PCR-based quantification of Escherichia coli suggests infection in most cases. Clin Microbiol Infect 2017; 23:647.
Hooton TM, Stamm WE. Diagnosis and treatment of uncomplicated urinary tract infection. Infect Dis Clin North Am 1997;11:551-81.
American College of Radiology. ACR Appropriateness Criteria for Acute Pyelonephritis. (Visit Source). Accessed on July 27, 2018.
Meyrier A, Condamin MC, Fernet M, et al. Frequency of development of early cortical scarring in acute primary pyelonephritis. Kidney Int 1989; 35:696.
Kawashima A, LeRoy AJ. Radiologic evaluation of patients with renal infections. Infect Dis Clin North Am 2003; 17:433.
Tsugaya M, Hirao N, Sakagami H, et al. Computerized tomography in acute pyelonephritis: the clinical correlations. J Urol 1990; 144:611.
Brandt WE. Adrenal glands and kidneys. In: Bryant WE and Helms CA, ed. Fundamentals of Diagnostic Radiology. Philadelphia, PA: Lippincott Williams & Wilkins; 2012.
Guideline.gov. (Visit Source) Accessed on July 27, 2018.
Demertzis J, Menias CO. State of the art: imaging of renal infections. Emerg Radiol 2007; 14:13.
Soulen MC, Fishman EK, Goldman SM. Sequelae of acute renal infections: CT evaluation. Radiology 1989; 173:423.
Ward G, Jorden RC, Severance HW. Treatment of pyelonephritis in an observation unit. Ann Emerg Med 1991; 20:258.
Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis 2011; 52:e103.
Singh KP, Li G, Mitrani-Gold FS, et al. Systematic review and meta-analysis of antimicrobial treatment effect estimation in complicated urinary tract infection. Antimicrob Agents Chemother 2013; 57:5284.
Golan Y. Empiric therapy for hospital-acquired, Gram-negative complicated intra-abdominal infection and complicated urinary tract infections: a systematic literature review of current and emerging treatment options. BMC Infect Dis 2015; 15:313.
Popejoy MW, Paterson DL, Cloutier D, et al. Efficacy of ceftolozane/tazobactam against urinary tract and intra-abdominal infections caused by ESBL-producing Escherichia coli and Klebsiella pneumoniae: a pooled analysis of Phase 3 clinical trials. J Antimicrob Chemother 2017; 72:268.
Carmeli Y, Armstrong J, Laud PJ, et al. Ceftazidime-avibactam or best available therapy in patients with ceftazidime-resistant Enterobacteriaceae and Pseudomonas aeruginosa complicated urinary tract infections or complicated intra-abdominal infections (REPRISE): a randomised, pathogen-directed, phase 3 study. Lancet Infect Dis 2016; 16:661.
Kaye KS, Bhowmick T, Metallidis S, et al. Effect of Meropenem-Vaborbactam vs Piperacillin-Tazobactam on Clinical Cure or Improvement and Microbial Eradication in Complicated Urinary Tract Infection: The TANGO I Randomized Clinical Trial. JAMA 2018; 319:788.
Hooper DC, Wolfson JS. Fluoroquinolone antimicrobial agents. N Engl J Med 1991; 324:384.
Sanchez GV, Master RN, Karlowsky JA, Bordon JM. In vitro antimicrobial resistance of urinary Escherichia coli isolates among U.S. outpatients from 2000 to 2010. Antimicrob Agents Chemother 2012; 56:2181.
Talan DA, Stamm WE, Hooton TM, et al. Comparison of ciprofloxacin (7 days) and trimethoprim-sulfamethoxazole (14 days) for acute uncomplicated pyelonephritis pyelonephritis in women: a randomized trial. JAMA 2000; 283:1583.
Peterson J, Kaul S, Khashab M, et al. A double-blind, randomized comparison of levofloxacin 750 mg once-daily for five days with ciprofloxacin 400/500 mg twice-daily for 10 days for the treatment of complicated urinary tract infections and acute pyelonephritis. Urology 2008; 71:17.
Talan DA, Klimberg IW, Nicolle LE, et al. Once daily, extended release ciprofloxacin for complicated urinary tract infections and acute uncomplicated pyelonephritis. J Urol 2004; 171:734.
Sandberg T, Skoog G, Hermansson AB, et al. Ciprofloxacin for 7 days versus 14 days in women with acute pyelonephritis: a randomised, open-label and double-blind, placebo-controlled, non-inferiority trial. Lancet 2012; 380:484.
Vellinga A, Tansey S, Hanahoe B, et al. Trimethoprim and ciprofloxacin resistance and prescribing in urinary tract infection associated with Escherichia coli: a multilevel model. J Antimicrob Chemother 2012; 67:2523.
Sanchez M, Collvinent B, Miró O, et al. Short-term effectiveness of ceftriaxone single dose in the initial treatment of acute uncomplicated pyelonephritis in women. A randomised controlled trial. Emerg Med J 2002; 19:19.
Shah KJ, Cherabuddi K, Shultz J, et al. Ampicillin for the treatment of complicated urinary tract infections caused by vancomycin-resistant Enterococcus spp (VRE): a single-center university hospital experience. Int J Antimicrob Agents 2018; 51:57.
Hooton TM. Clinical practice. Uncomplicated urinary tract infection. N Engl J Med 2012; 366:1028.
Mombelli G, Pezzoli R, Pinoja-Lutz G, et al. Oral vs intravenous ciprofloxacin in the initial empirical management of severe pyelonephritis or complicated urinary tract infections: a prospective randomized clinical trial. Arch Intern Med 1999; 159:53.
van Nieuwkoop C, van der Starre WE, Stalenhoef JE, et al. Treatment duration of febrile urinary tract infection: a pragmatic randomized, double-blind, placebo-controlled non-inferiority trial in men and women. BMC Med 2017; 15:70.
Warren JW, Abrutyn E, Hebel JR, et al. Guidelines for antimicrobial treatment of uncomplicated acute bacterial cystitis and acute pyelonephritis in women. Infectious Diseases Society of America (IDSA). Clin Infect Dis 1999; 29:745.
Cronberg S, Banke S, Bergman B, et al. Fewer bacterial relapses after oral treatment with norfloxacin than with ceftibuten in acute pyelonephritis initially treated with intravenous cefuroxime. Scand J Infect Dis 2001; 33:339.
Nicolle LE. A practical guide to the management of complicated urinary tract infection. Drugs 1997; 53:583.
Mountokalakis T, Skounakis M, Tselentis J. Short-term versus prolonged systemic antibiotic prophylaxis in patients treated with indwelling catheters. J Urol 1985;134:506-8.
Nyren P, Runeberg L, Kostiala AI, Renkonen OV, Roine R. Prophylactic methenamine hippurate or nitrofurantoin in patients with an indwelling urinary catheter. Ann Clin Res 1981;13:16-21.
Butler HK, Kunin CM. Evaluation of specific systemic antimicrobial therapy in patients while on closed catheter drainage. J Urol 1968;100:567-72.
Gribble MJ, Puterman ML. Prophylaxis of urinary tract infection in persons with recent spinal cord injury: A prospective, randomized, double-blind, placebo-controlled study of trimethoprim-sulfamethoxazole. Am J Med 1993;95:141-52.
Riley DK, Classen DC, Stevens LE, Burke JP. A large randomized clinical trial of a silver-impregnated urinary catheter: Lack of efficacy and staphylococcal superinfection. Am J Med 1995;98:349-56.
Linsenmeyer TA, Harrison B, Oakley A, Kirshblum S, Stock JA, Millis SR. Evaluation of cranberry supplement for reduction of urinary tract infections in individuals with neurogenic bladders secondary to spinal cord injury. A prospective, double-blinded, placebo-controlled, crossover study. J Spinal Cord Med2004;27:29-34.
Cardenas DD, Hoffman JM, Kelly E, Mayo ME. Impact of a urinary tract infection educational program in persons with spinal cord injury. J Spinal Cord Med 2004;27:47-54.
Morton SC, Shekelle PG, Adams JL, et al. Antimicrobial prophylaxis for urinary tract infection in persons with spinal cord dysfunction. Arch Phys Med Rehabil 2002;83:129-38.
Thompson RL, Haley CE, Searcy MA, et al. Catheter-associated bacteriuria. Failure to reduce attack rates using periodic instillations of a disinfectant into urinary drainage systems. JAMA 1984;251:747-51.
Gillespie WA, Simpson RA, Jones JE, Nashef L, Teasdale C, Speller DC. Does the addition of disinfectant to urine drainage bags prevent infection in catheterised patients? Lancet 1983;1:1037-9.
Leone M, Garnier F, Dubuc M, Bimar MC, Martin C. Prevention of nosocomial urinary tract infection in ICU patients: Comparison of effectiveness of two urinary drainage systems. Chest 2001;120:220-4.
Huth TS, Burke JP, Larsen RA, Classen DC, Stevens LE. Randomized trial of meatal care with silver sulfadiazine cream for the prevention of catheter-associated bacteriuria. J Infect Dis 1992;165:14-8.
Burke JP, Jacobson JA, Garibaldi RA, Conti MT, Alling DW. Evaluation of daily meatal care with poly-antibiotic ointment in prevention of urinary catheter-associated bacteriuria. J Urol 1983;129:331-4.
Burke JP, Garibaldi RA, Britt MR, Jacobson JA, Conti M, Alling DW. Prevention of catheter-associated urinary tract infections. Efficacy of daily meatal care regimens. Am J Med 1981;70:655-8.
Schierholz JM, Yucel N, Rump AF, Beuth J, Pulverer G. Antiinfective and encrustation-inhibiting materials - myth and facts. Int J Antimicrob Agents 2002;19:511-6.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.