This course will be updated or discontinued on or before Friday, July 30, 2027
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
FPTA Approval: CE25-1318407, CE26-1318407. Accreditation of this course does not necessarily imply the FPTA supports the views of the presenter or the sponsors.
CEUFast, Inc. is recognized by the New York State Education Department's State Board for Physical Therapy as an approved provider of physical therapy and physical therapist assistant continuing education.
Outcomes
≥ 92% of participants will know the signs and symptoms of pelvic floor dysfunction, how to effectively screen for pelvic floor dysfunction, and foundational treatment concepts.
Objectives
After completing this continuing education course, the participant will be able to meet the following objectives:
Outline screening tactics to identify signs and symptoms related to pelvic floor dysfunction.
Evaluate the need for a comprehensive approach to pelvic rehab.
Identify pertinent anatomy and physiology related to pelvic floor dysfunction.
Distinguish between common complaints, their causes, and the treatment of pregnant women.
Formulate an appropriate post-partum recovery program within your scope of practice.
Compare and contrast stress incontinence and urge incontinence.
Recognize subtypes and define symptoms of various pelvic pain conditions.
Outline how pelvic floor dysfunction may contribute to bowel and gastrointestinal conditions.
Distinguish key differences between common male and female pelvic health conditions.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
The prevalence of pelvic floor dysfunction in women is high. According to the National Institute of Health (NIH), between 25-50% of all women experience pelvic floor issues ranging from a broad range of conditions (Snyder, 2024). A recent study conducted by the University of Iowa found that at least 32% of over 25,000 adult women had at least one pelvic floor disorder diagnosis. This consisted of women who may or may not have been initially seeking care for pelvic floor problems (Meretighan, 2023). Although most attention is directed toward women with pelvic floor dysfunction, it has been found that 16% of men were identified with pelvic floor dysfunction (Grimes & Stratton, 2023). These numbers may very well be under-reported due to embarrassment, stigma, or the belief that there is nothing that can be done to improve the problem. It is also estimated that pelvic floor dysfunction will rise by 35% in the next 12 years, which greatly increases the demand and need for pelvic health professionals (Meretighan, 2023).
Pelvic floor rehab is one of the fastest-growing specialties in physical therapy. Each day, providers are becoming more educated, spreading awareness, and achieving better clinical outcomes with pelvic health. This drives a demand for clinicians to raise the standard of care by intentionally refining their skills and knowledge of this subject matter. While educational programs typically offer a brief overview of pelvic floor rehab, most new graduates still begin their careers lacking a basic competency to screen for pelvic floor conditions.
This course will provide information about common pelvic floor conditions, how to screen for them, and treatment options for clinicians based on their setting and experience level. Written from a clinical perspective and supported by research to allow for a combination of evidence-based practice and to highlight the many nuances involved in pelvic health, this course will cover several key objectives to allow participants to gain awareness of pelvic floor symptoms and improve their clinical decision-making. This course does not prepare nurses, physical therapists, or occupational therapists for internal pelvic exams or treatment. Following this course, it is recommended that providers new to pelvic floor rehab concepts seek continuing education with lab components to be clinically competent with internal examinations. Current pelvic health providers or orthopedic providers hoping to gain more knowledge of the pelvic floor will benefit from updated research, case studies, and possibly a different perspective on familiar concepts with this course. It is also a goal that this course material can create a better interprofessional understanding of what pelvic floor rehab encompasses and how patients can benefit from pelvic floor rehabilitation.
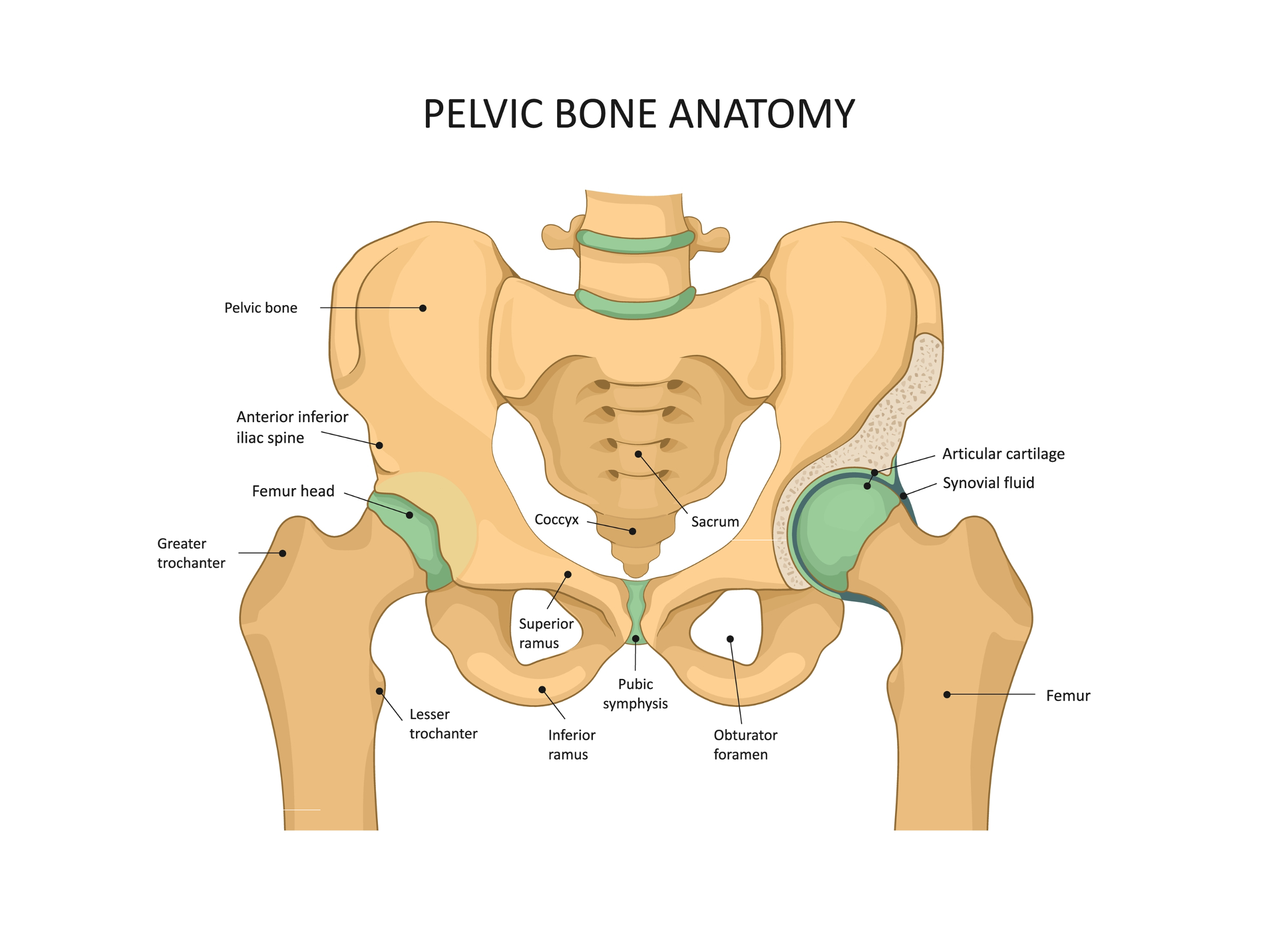
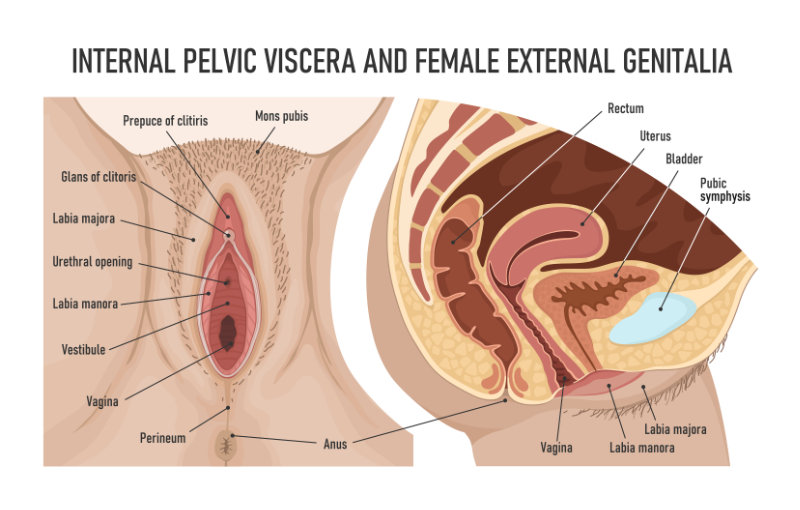
There are many key anatomical components of the pelvic cavity and pelvic floor. The bony components include the fusion of the ilium, ischium, and pubis on either side of the body to articulate with the appendicular skeleton at the femoro-acetabular joint, and the axial skeleton at the sacroiliac joint. Anteriorly, the pubic bones form a thick cartilaginous joint called the pubic symphysis. This creates a bowl-like structure that contains the pelvic floor musculature, which supports the abdominopelvic viscera (bladder, distal segments of the ureters, sigmoid colon, rectum, and reproductive structures).
(*Please click on the image above to enlarge.)
Image 1:Bony Anatomy
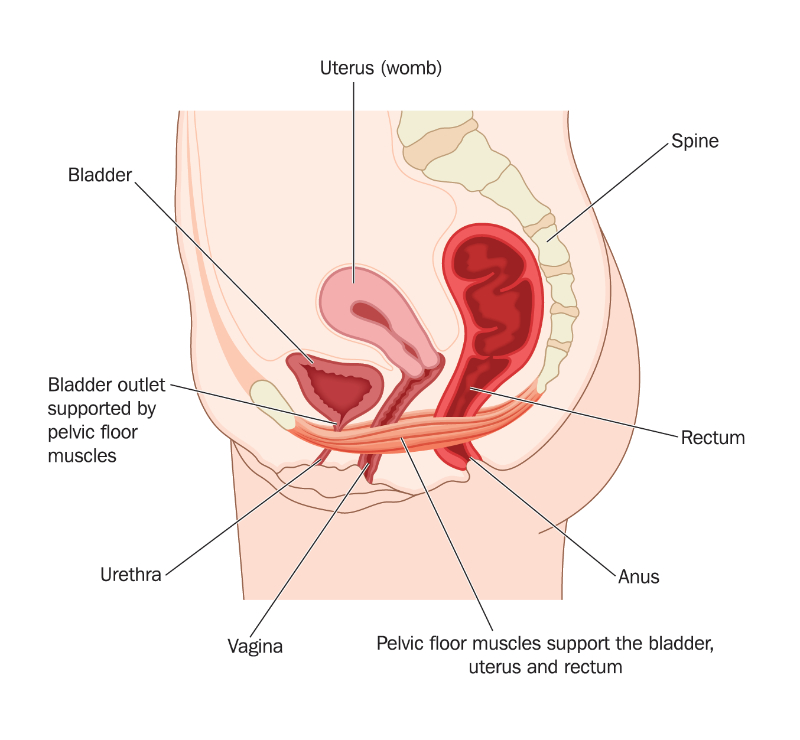
Image 2: Pelvic Floor
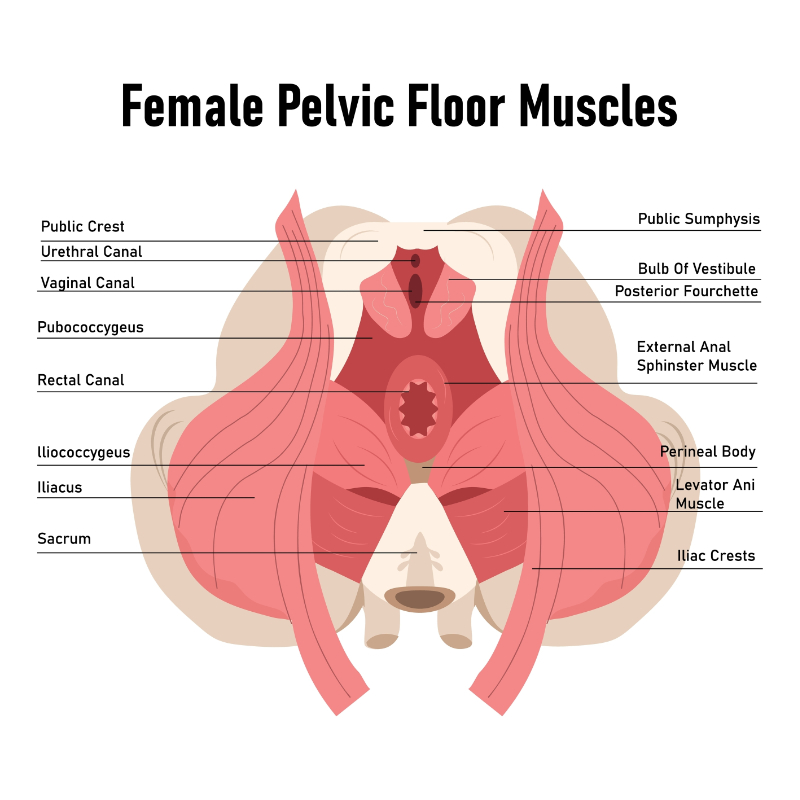
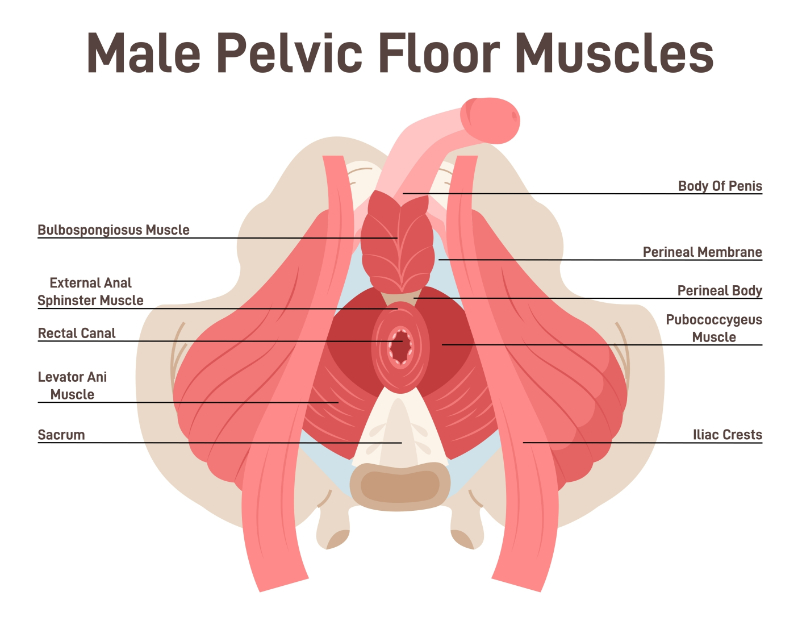
The pelvic floor muscles can be broken up into three layers. The superficial layer is referred to as the urogenital triangle and consists of bulbospongiosus (bulbocavernosus), ischiocavernosus, transverse perineal muscles, and the external anal sphincter (EAS) (Fahmy et al., 2022). Each of these muscles is innervated by the perineal nerve, aside from the EAS, which is innervated by the inferior rectal nerve. Both nerves are terminal branches of the pudendal nerve (Kinter & Newton, 2023). Ischiocavernosus originates from the ischial tuberosity and the ischiopubic ramus and forms the lateral boundary of the perineum. It attaches to the undersurface of the crus clitoris and the crus penis. The contraction of this muscle aids in erectile function of the penis and clitoris by reducing venous return from these tissues (Fahmy et al., 2022). Bulbospongiosus has different anatomical origins in males and females. In males, the compression of the bulbospongiosus aids in emptying the penile urethra during urination and ejaculation (Peikert et al., 2015). In both sexes, the contraction of the muscle aids in the process of erection by forcing blood from the corpus spongiosum in males and the bulb of the vestibule in females to more distal structures (Fahmy et al., 2022). The transverse perineal muscles originate from the anterior and medial aspect of the ischial tuberosity and are inserted into the perineal body while stabilizing it (Fahmy et al., 2022).
Image 3: Female Pelvic Floor Musculature
Image 4: Male Pelvic Floor Musculature
The perineal body is another important pelvic floor structure that divides the anus from the urogenital structures. It is referred to as the central tendon of the perineum. It supports the pelvic floor through multiple muscle, fascia, and sphincter attachments and has anatomical connections with each layer of the pelvic floor. Notably, the internal and external anal sphincters adhere to the perineal body posteriorly. The area is commonly damaged in females during childbirth (Bordoni & Launico, 2024). Perineal tearing of the external anal sphincter can lead to postpartum fecal incontinence. The perineal body is an important landmark for gynecological and gastrointestinal surgeries (Bordoni & Launico, 2024).
Image 5 Female Pelvic Viscera
The second muscle layer is called the urogenital diaphragm, or, in anatomical research, the perineal membrane (Bolla et al., 2023). It separates the superficial pelvic floor structures from the deep pelvic floor layers via a strong muscular membrane in the anterior portion of the pelvic floor between the pubic symphysis and ischial tuberosities (Raizada & Mittal, 2008). The perineal membrane contains the urethral sphincter and neurovascular structures supplying the external genitalia in males and females (Bolla et al., 2023).
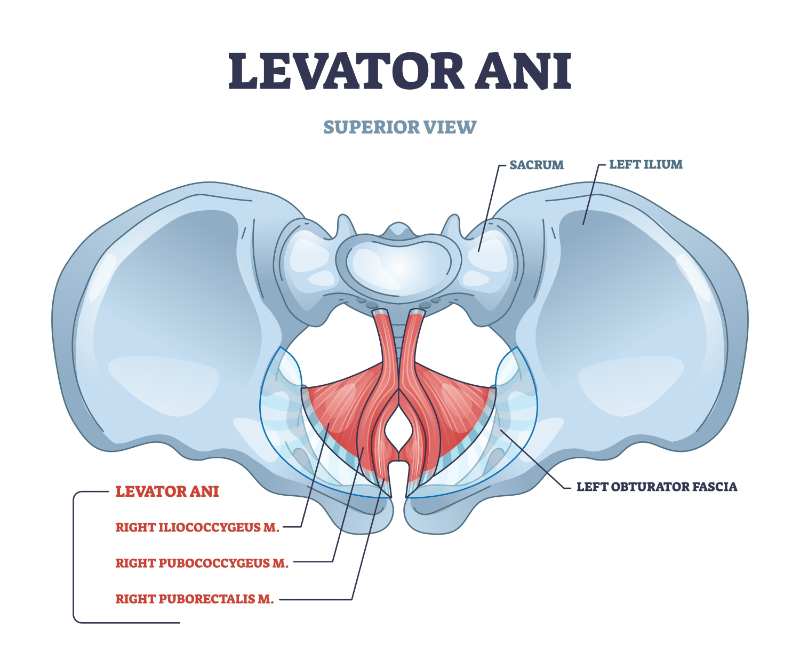
The third layer of pelvic floor musculature is a group of three muscles that together form the levator ani. These muscles are the pubococcygeus, puborectalis, and iliococcygeus. The levator ani has a complex innervation from S2, S3, and S4 branches of the sacral plexus, along with some components having direct innervation from the pudendal nerve. The role of the levator ani is to support the pelvic viscera, but it also aids in sexual function, urination, and defecation (Gowda & Bordoni, 2022). The levator ani manages mechanical pressures and distributes load with human movement. Also notable is this muscle group’s role in managing intra-abdominal pressure and coordinated activity with breathing, which will be discussed in further detail later in the course.
Puborectalis is the most medial muscle of the levator ani group, and it has fibers interworking with the anal sphincters. It originates from the pubic bone anteriorly and forms a sling around the rectum. It has a primary role in defecation and fecal continence. Pubococcygeus is more lateral and has attachments to the perineal body and coccyx. In females, fibers from this muscle support the vagina, and in males, it aids with prostate function. Iliococcygeus, otherwise referred to as coccygeus, is the most lateral of the levator ani group. It attaches to the fascia of the obturator internus muscle, running posteriorly to the coccyx. It is continuous with the anococcygeal ligament, which is a posterior anchor for the pelvic floor. Importantly, the fascia from the obturator internus forms the pudendal canal, also referred to as Alcock’s canal. This canal in the ischioanal fossa is a passage for the pudendal nerve and vascular supply (Kinter & Newton, 2023). This is a common place for pudendal nerve entrapment with various pelvic floor pathologies.
Image 6: Levator Ani
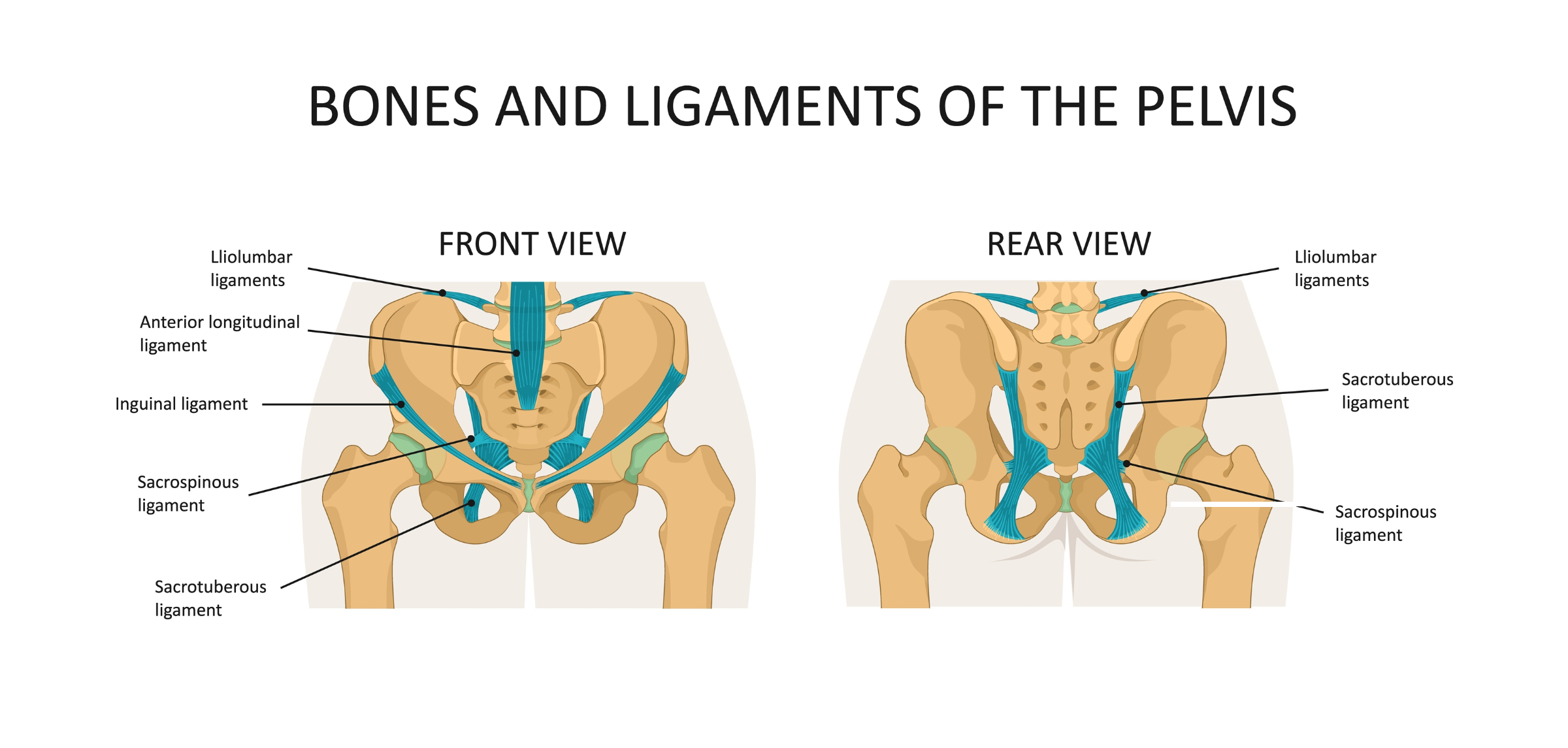
There are many ligaments in and around the pelvic cavity. The sacrotuberous ligament is a thick, strong band of connective tissue extending from the inferior parts of the sacrum and the upper portion of the coccyx to either ischial tuberosity. Its primary role is posterior bony stability of the pelvis. The sacrospinous ligament is triangular in shape, originating from the anterior portion of the lower sacrum and coccyx, which narrows and attaches to the ischial spine (Chaudhry et al., 2023). The sacrospinous ligament divides a bony opening to form the greater and lesser sciatic foramen, where neurovascular structures pass through. The iliolumbar and sacroiliac ligaments are strong supportive structures in the articulation between the axial and appendicular skeleton, but typically involve more orthopedic components with pelvic pain.
(*Please click on the image above to enlarge.)
Image 7: Bones and Ligaments of the Pelvis
Several supportive ligaments have clinical relevance in females, especially in the pregnant population. The round ligament of the uterus runs from the ‘cornu’ or the uterine horn and travels through the inguinal canal and blends with the labia majora and the mons pubis (Chaudhry et al., 2023). As the uterus expands with pregnancy, beginning in the 2nd trimester, women can start to experience lower abdominal pain, which is often caused by the stretching of the round ligament (Chaudhry & Chaudhry, 2023). This pain tends to resolve on its own with rest, but can also be addressed with manual therapy treatment performed by an experienced clinician during pregnancy. The broad ligament of the uterus is a sheet of pelvic peritoneum extending in each direction from the pelvic sidewalls to the uterus in the midline. The broad ligament folds over the fallopian tubes and ovaries and covers them anteriorly and posteriorly (Chaudhry et al., 2023). The broad ligament has three tissue layers, and it contains neurovascular structures. Its function is to support the position of the uterus and the relationship between the uterus, fallopian tubes, and ovaries. The cardinal ligament, or transverse cervical ligament, is attached from the lateral aspect of the cervix to the respective pelvic wall. It forms the lower border of the broad ligament and contains the uterine artery and uterine veins. The pubocervical ligament is attached to the cervix and extends to the posterior surface of the pubic symphysis. The uterosacral ligaments, along with the cardinal ligaments, provide additional support for the uterus within the pelvis and attach from the cervix below the peritoneum backward to the anterior aspect of the sacrum (Chaudhry et al., 2023).
When screening for pelvic floor dysfunction (PFD), any issue relating to the urinary system, bowel, support, sexual function, and pelvic pain should be considered. The Cozean screening tool was developed to help rehab providers with clinical decision-making and streamline the identification of PFD.
In 2018, a retrospective analysis survey of 10 questions was given to patients with known pelvic floor dysfunction to analyze the most common symptoms. The goal was to help identify characteristics of PFD so it may improve screening and awareness across the medical system and, in turn, allow patients to get faster treatment. Below is the questionnaire. If 3+ questions are answered with “yes,” this indicates a 91% likelihood that pelvic floor dysfunction is likely.
It should be noted that in this survey, 70% of the patients with PFD also had orthopedic pain. Orthopedic physical therapists must acknowledge that it is common for low back pain, hip pain, and sciatica to be related to pelvic floor dysfunction. Orthopedic therapists taking this course should be able to use this tool to effectively manage or refer patients for specialty care when treating patients with pelvic pain.
☐ I sometimes have pelvic pain (in genitals, perineum, pubic, or bladder area) or pain with urination that exceeds a ‘3’ on a 1-10pain scale, with 10 being the worst pain imaginable. ☐ I can remember falling onto my tailbone, lower back, or buttocks (even in childhood) ☐ I sometimes experience one or more of the following urinary symptoms
Accidental loss of urine
Feeling unable to completely empty my bladder
Having to void within a few minutes of a previous void
Pain or burning with urination
Difficulty starting or frequent stopping/starting of urine stream
☐ I often or occasionally have to get up to urinate two or more times at night ☐ I sometimes have a feeling of increased pelvic pressure or the sensation of my pelvic organs slipping down or falling out ☐ I have a history of pain in my low back, hip, groin, or tailbone, or have had sciatica ☐ I sometimes experience one or more of the following bowel symptoms
Loss of bowel control
Feeling unable to completely empty my bowels
Straining or pain with a bowel movement
Difficulty initiating a bowel movement
☐ I sometimes experience pain or discomfort with sexual activity or intercourse ☐ Sexual activity increases one or more of my other symptoms ☐ Prolonged sitting increases my symptoms
IF YOU CHECKED 3 OR MORE BOXES, PELVIC FLOOR DYSFUNCTION IS LIKELY Source Link
A comprehensive pelvic floor exam should include a gathering of relevant medical history including any mental, physical, or sexual trauma, timing and frequency of symptoms, diet and lifestyle habits, liquid intake (type and quantity), and a review of any imaging or urology exams such as urinalysis, urodynamic testing, or prostate-specific antigen (PSA), or physicians medical notes. An orthopedic screen should be performed, looking at back and hip range of motion, posture, and strength. The strength assessment should include core strength and coordination. Following this, pelvic floor therapists should consider an abdominal exam to assess for tenderness, visceral mobility, and breathing patterns. Next, an external pelvic floor assessment can be done, which is easiest with the patient in a hook-lying position, draped with a sheet. Therapists can assess the superficial pelvic floor (bulbospongiosus, ischiocavernosus, and the transverse perineum) for tightness, tenderness, and reproduction of familiar symptoms. Therapists might also consider assessment of the ischial tuberosities, which could give insight into pelvic floor symptoms as well as the pubic rami, bladder, sacrospinous, and sacrotuberous ligaments. And finally, an internal muscle assessment should be performed digitally. This can be done in hooklying, sidelying, or prone, depending on patient comfort level and therapist preference.
Women in the pregnancy and postpartum period are among the most common patients seeking pelvic floor therapy. The body goes through significant changes while pregnant. All body systems change and adapt during pregnancy to grow and support a fetus in utero. Musculoskeletal, hormonal, and vascular changes are most significant to identify and treat as a rehab provider.
Estrogen levels increase steadily throughout pregnancy and reach a 100-fold increase of preconception levels by the 3rd trimester (Jee & Sawal, 2024). This tends to result in urinary incontinence, as well as low back, sacroiliac (SI) joint, and pubic symphysis pain because estrogen increases the laxity within the connective tissue along with the relaxin hormone. Urinary incontinence tends to develop during pregnancy because of tissue laxity around the urethral sphincter. This will be discussed in further detail in the next section.
Pelvic girdle pain is estimated to affect half of all pregnant women (Fiani et al., 2021). The sacroiliac joint, in particular, serves a complex role in transmitting force between the limbs and trunk with movement. Because of the increased levels of estrogen and relaxin present during pregnancy, the SI joints develop significant laxity to allow for widening of the uterus and eventually the pelvic outlet during birth. As the fetus develops, the lumbar spine tends to develop an increased lordosis, putting even more mechanical stress on the SI joints (Fiani et al., 2021). Symphysis pubis dysfunction (SPD) is another common form of pelvic pain during pregnancy due to increased mobility of the joint in a similar fashion as described above. Patients will report a variety of symptoms with SPD, but the most common include pain, tenderness, and occasional radiating symptoms focused around the pubic region, especially with activities that include transferring weight or changing positions like climbing stairs or rolling in bed (Howell, 2012).
Although joint laxity-related pelvic pain cannot be completely avoided during pregnancy, physical therapists should utilize proper strengthening and stability principles to mitigate these changes. This is a growing area of research interest, and preliminary reviews have found that guided stabilization interventions can alleviate pelvic girdle pain during pregnancy (Puri et al., 2023). There is also evidence for positive effects on mental health and quality of life during pregnancy with strength training (Redondo-Delgado et al., 2025). The problem with this area of research is that there is no consensus on the best interventions to alleviate pelvic girdle pain with pregnancy. This should prompt a physical therapist to choose a symptom-based and individualized approach. A combination of manual therapy, modalities, strengthening/stabilization exercises, and aerobic exercise can be used depending on the patient’s goals and activity level. As a starting point, interventions focusing on the large muscle groups with attachments to the pelvic girdle tend to be effective in clinical practice. For example, hamstring activation and concentric strengthening can reduce the lumbar spine's hyperlordotic curvature and reduce SI joint pain. Isometrics and manual therapy interventions to reduce hypertonicity in the adductor group are an effective method for treating SPD. Fortunately, the amount of information and education on treating pelvic girdle pain is always increasing, and providers should be confident in helping alleviate symptoms of pelvic girdle pain in their clinical practice.
Pelvic floor rehabilitation is multifaceted, and it is beyond the scope of this course to encompass the full range of clinical considerations during pregnancy and postpartum. It is, however, worth briefly touching on several other musculoskeletal changes that occur with pregnancy. Posture changes significantly throughout the body. Starting from the floor, foot arch height typically decreases while foot width increases, mostly due to blood volume and increased body weight by the third trimester (Conder et al., 2019). At the knee, increased ligament laxity tends to result in hyperextension to offset the anterior shift in the center of gravity (Chu et al., 2019). In addition to the changes in the pelvis and lumbar spine, the thoracic spine’s kyphotic curve tends to increase along with a widening of the infrasternal angle at the rib cage. This causes an upward displacement of the diaphragm that usually persists into the postpartum period (LoMauro & Aliverti, 2015). Restoring normal breathing mechanics and rib cage angle is essential to postpartum rehab. Patients will have difficulty restoring core strength, spine mobility, and intra-abdominal pressure regulation without addressing this. These musculoskeletal changes will alter gait mechanics and proprioceptive awareness (Conder et al., 2019).
As the uterus grows with pregnancy, the ligaments that support and anchor it to the pelvis stretch. The round ligament is a structure that can cause sharp, sudden pain in the lower abdomen, which becomes more common later in pregnancy (Chaudhry & Chaudhry, 2023). Providers can utilize hip and back mobility exercises, pelvic floor relaxation techniques, and manual therapy with proper training to alleviate these symptoms. Interventions to improve anterior chain mobility, particularly in the hips, are also useful for this symptom presentation.
Maternal blood volume increases approximately 45% during pregnancy along with a 20% increase in oxygen demand (Soma-Pillay et al., 2016). Practitioners need to recognize these changes when prescribing exercise. The CDC and the American College of Obstetricians and Gynecologists (ACOG) recommend 150 minutes of moderate physical activity per week for pregnant women. Physical inactivity is an independent risk factor for gestational diabetes and obesity (Artal, 2015). Despite this recommendation, the most recent research found that less than 25% of pregnant women meet this physical activity threshold (Hesketh & Evenson, 2016). Given the combination of cardiovascular changes during pregnancy, along with the fact that the baseline activity level of many of these patients will be low, practitioners should bring increased awareness to monitoring vitals when prescribing exercise to pregnant individuals.
Preeclampsia is particularly important to monitor during the 2nd and 3rd trimesters. It is defined by a blood pressure increase to 140/90 measured two separate times at least 4 hours apart when there are no pre-existing hypertensive issues (Karrar et al., 2024). Symptoms of preeclampsia include the onset of abdominal pain, shortness of breath, visual disturbances, and elevated protein levels in the urine. Pregnant clients should regularly be monitored for these changes, especially after 20 weeks of gestation. Preeclampsia incidence also rises near full term, and it unfortunately leads to over 50,000 maternal deaths every year, worldwide (Karrar et al., 2024).
In addition to physical therapy treatments, supplemental items can make a difference in reducing discomfort during pregnancy. Belly bands or similar support garments can support the core, alleviating low back pain and pelvic girdle pain, especially in the 2nd and 3rd trimesters (Quintero Rodriguez & Troynikov, 2019). SI belts are sometimes recommended to compress and stabilize the expanding pelvis. Compression socks can help venous return and prevent lower extremity edema (Saliba-Júnior et al., 2022). Vulvar support garments can increase maternal blood volume and are an option to reduce perineal pressure and pain.
Pelvic floor therapists play an important role in teaching proper pushing techniques to minimize birthing injuries; however, this is highly dependent on proper fetal positioning, fetal size, and any medical interventions involved with birthing. Pelvic floor therapists also teach patients to relax the levator ani muscles before birth. The inability to relax the pelvic floor musculature has been associated with longer second stage of labor and increased cesarean delivery rate (Youssef et al., 2021). Therapists may use a combination of manual release techniques, central nervous system downtraining, breathwork, and guided self-release techniques.
In the immediate postpartum period, the mother’s body undergoes significant changes in hormone levels as the uterus, cervix, vagina, and perineum begin to recover from the birthing process. Women should be encouraged to rest as much as possible in the early postpartum period and seek proper nutrition and hydration. From a pelvic floor perspective, birth is an injury to the musculature that needs to be healed and rehabbed, just like other body regions where patients expect a full return to activity.
Hemorrhoids often develop in the third trimester and during the birthing process. A prior history of perianal disease, constipation, and prolonged straining during delivery are independent risk factors for developing hemorrhoids or anal fissures (Poskus et al., 2014). Women should be encouraged to keep their stool soft to avoid excessive strain on the pelvic floor with bowel movements. They can also be taught to use proper toilet positioning and slow, controlled breathing to improve pelvic floor relaxation and reduce straining. This will be discussed further in the GI section of the course.
Typically, a patient’s midwife or OBGYN will clear them for intercourse and intravaginal manual therapy around 6 weeks postpartum. Pelvic floor therapists trained in internal muscle treatment can assess for hypertonicity, scar tissue, tenderness, and pain in structures such as the levator ani, obturator internus, urethra, endopelvic fascia, and superficial pelvic floor. At this stage, women can be screened for pelvic organ prolapse, diastasis recti abdominis (DRA), as well as general musculoskeletal complaints from pregnancy and birth.
Diastasis Recti Abdominis is a common postpartum finding. This is caused by a weakening and stretching of the anterior abdominal wall in the linea alba during pregnancy (Hall & Sanjaghsaz, 2023). This typically presents as a midline bulge in the abdominal region that worsens with a crunch or increased abdominal pressure, such as sneezing or coughing. The diagnostic criteria are not definitive, but typically the width between the walls of the rectus abdominis is measured at the level of the umbilicus and 3 cm above and below (Qu et al., 2021). A separation greater than 20 mm is generally considered a significant clinical finding, but does not necessarily mean it is pathological. The practitioner measures this separation in the clinic using their finger widths for approximate quantification. DRA typically worsens with multiple pregnancies, but physical therapy can be useful in closing the abdominal wall. Healing DRA is multifaceted, but rehab should focus on three specific areas. Deep core stabilization exercises have been shown to make a statistically significant difference in closing the abdominal gap and increasing quality of life in the postpartum period (Thabet & Alshehri, 2019). Avoiding postures and activities with excessive thoracic kyphosis that create excessive intra-abdominal pressure will also facilitate DRA closure. And third, increasing mobility in the thoracolumbar region of the spine through manual therapy, breathwork, and corrective exercise is highly effective in the clinical setting.
Image 8: Diastasis Recti Abdominus
Once postpartum moms have gotten through the early stages of core strengthening and breath control and are ready to return to exercise, there are a few more considerations for rehab providers. Urinary incontinence will be discussed in the next section. Still, it is worth mentioning that addressing tension and tenderness in the pelvic muscles will aid in recovery and awareness, as well as teaching patients the difference between an anterior and posterior pelvic floor contraction.
Caesarian (C-section) deliveries are becoming increasingly common, especially in the past 30 years. In 1990, only 7% of live births occurred via C-section, compared to 21% in 2023 (Angolile et al., 2023). A physical therapist’s role in assisting with the rehabilitation of this procedure is becoming more important. Pre-operative physical therapy and education before elective C-section have been shown to reduce hospital stay length, pain after delivery, and pain when returning to functional activities (Weerasinghe et al., 2022). Postoperatively, the rehab mindset must include scar healing and core function principles. The C-section scar should be given 6 weeks to heal, but before this, education on posture, breathing, and functional activities such as holding the baby while getting in/out of bed or up/down from a chair can assist in core recovery and pain management. Physical therapists can begin soft tissue work at six weeks to ensure optimal healing, progress core engagement, and minimize pain. There is limited research on scar mobilization, but one study showed a reduction in pain and improved tissue mobility with a 2-week protocol (Gilbert et al., 2022). Evidence also supports kinesio taping to the scar and abdominal muscles for quicker return of core muscle function compared to exercise alone (Gürşen et al., 2016). Anecdotally, scar mobility, visceral mobilization, cupping, and breathwork can also be effective techniques to help patients recover from c-sections.
The progression of core rehabilitation from either a vaginal or C-section delivery should include these basic principles: First, teaching equal rib expansion (lateral and posterior) with inhalation will prevent excessive pressure to the abdomen. Belly breathing is not the most helpful type of deep breathing. Instead, use “360 breathing”. After a full inhale is established, gradual transverse abdominis activation can begin. This is palpable and visualized by feeling and seeing the lower abdominals contract and draw slightly upward. When the patient understands this deep lower core activation, movement and loading can be added. Exercises such as supine marching, dead bugs, and paloff presses are great neutral spine movements to increase tension and endurance as the abdominal wall heals. More complex movements, such as oblique twists or crunches, can be added as this foundation builds.
Incontinence is among the most common symptoms associated with pelvic floor dysfunction. A recent study examining the prevalence and factors of urinary incontinence found that over 32% of U.S. adult women experienced urinary incontinence every month (Patel et al., 2022). Recent research has also found that the prevalence is increasing due to factors such as obesity, prior vaginal birth, anxiety, depression, and age. Urinary incontinence has also been found to cause a significant reduction in quality of life due to the correlation with comorbidities in the older adult population, as well as increased incidence of anxiety and depression in the younger adult population (Pizzol et al., 2021).
There are five general categories of urinary incontinence, but symptoms and treatment options can overlap. This course will cover the two main types: stress urinary incontinence (SUI) and urge urinary incontinence. ‘Continence’ can be defined as voluntary control of bowel and/or bladder function (Haylen et al., 2010). When a pelvic physical therapist evaluates a patient, they can often deduce the type of urinary incontinence a patient may be experiencing with the subjective interview.
Before beginning a hands-on assessment, rehab providers can ask interview questions such as when their patient leaks, what activities they perform, and what sensations they experience. They should incorporate past medical history with psychosocial awareness. Common subjective reports for patients experiencing SUI include:
Leakage when coughing or sneezing
Leakage with jumping or running
Leaking on their way to the restroom while they have a strong urge to urinate
Leaking or sudden urge caused by environmental cues, such as turning on the shower
Pregnancy and menopause are life events that also increase the likelihood of experiencing SUI due to hormonal and postural changes.
Stress urinary incontinence (SUI) was most recently defined by the International Continence Society along with the International Urogynecological Association as the “Complaint of involuntary loss of urine on effort or physical exertion, including sporting activities, or on sneezing or coughing” (Doumouchtsis et al., 2023). From a clinical perspective, women who present with SUI most often experience symptoms with higher-impact activities such as running, jumping, and participation in recreational activities, as well as sneezing and coughing. SUI is by far the most common type of urinary leakage and is among the most common diagnoses pelvic floor rehab clinicians will see in their practice (Sam et al., 2025).
To properly and effectively treat urinary incontinence, pelvic floor rehab providers should identify the contributing factors to urinary leakage during physical exertion. For simplicity, this can typically be categorized as either intrinsic sphincter deficiency or urethral hypermobility.
When intrinsic sphincter deficiency is the issue, the patient cannot produce enough urethral closure pressure to withstand the pressure changes in the abdominopelvic cavity. In the medical setting, providers such as urologists may use a bladder or cough stress test with patients with few comorbidities or complicating lifestyle factors. This test aims to assess whether the urethral closure pressure is strong enough to resist intra-abdominal pressure with the force of a cough. This is performed by having the patient cough forcefully 1-4 times with roughly 200-400 mL bladder volume, and the provider observes the urethral opening for urine leakage (Guralnick et al., 2018). From a more practical but less researched standpoint, the Urine Stream Interruption Test can be used to assess pelvic floor muscle strength and intrinsic sphincter deficiency. This test is performed with the patient sitting on the toilet with a mostly full bladder. They are instructed to initiate urination and instructed to stop the flow 4-5 seconds later. The data collected from this test is the time it takes the patient to stop the flow of urine from the point where they are instructed to stop (Sampselle & DeLancey, 1992). This is an old study, but the results found that continent women were able to stop the flow of urine more quickly than those who experienced SUI. Despite the age of the research, the value of the Urine Stream Interruption Test is that it is inexpensive, easy to perform for the patient, and demonstrates high repeatability. If a patient is unable to stop the flow of their urine within a reasonable timeframe, it could be deduced that urethral sphincter weakness is contributing to their symptoms of SUI, and treatment options for this will be discussed in the following section.
When a patient can voluntarily stop the flow of urine but still experiences urinary incontinence with coughing, sneezing, and physical activity, they may be experiencing symptoms due to urethral hypermobility. This occurs when the anatomic fascial support of the urethra has been compromised. The most common causes for acquired urethral hypermobility are childbirth and physiologic hormonal changes throughout life. There is a strong link between SUI in the postpartum period and second-stage labor (“pushing stage”) lasting more than 2 hours (Jin et al., 2022). This is due to the increased likelihood of fascial damage and pudendal nerve damage while the fetal head is in the birth canal. The superficial perineal branch of the pudendal nerve innervates the urethral sphincters and has multiple branches innervating the superficial pelvic floor as well. Higher infant birth weight, head circumference, and third to fourth-degree perineal tears are also risk factors for pudendal nerve injury due to excessive stretching forces (Sam et al., 2025). It should be noted that pudendal nerve injury can lead to intrinsic sphincter weakness, and facial damage can lead to urethral hypermobility, both of which need specific treatment modalities.
It is also important to note the role of estrogen in urinary incontinence. The urethral sphincter has estrogen receptors, and in periods of low estrogen, such as immediately postpartum and the menopausal timeframe, urethral atrophy occurs, causing intrinsic sphincter weakness. In menopause, this is due to reduced blood supply to the urethral sphincter, causing it to shrink and weaken. This can be treated by using topical vaginal estradiol cream, which is highly effective with appropriate patients, but does require a physician consultation and prescription (Te West et al., 2023). Pregnancy is another period of high estrogen levels, which causes a loosening effect on the connective tissue and leads to urethral hypermobility-related urinary incontinence (Chidi-Ogbolu & Baar, 2019). Although it is not the primary role of the rehab provider to diagnose and treat the hormonal factors contributing to SUI, it is important to be aware of these normal biologic changes to guide treatment.
Historically, when patients are diagnosed with urinary incontinence, they are prescribed Kegel exercises by their OBGYN or rehab provider. A Kegel exercise aims to voluntarily contract the levator ani muscles to aid urethral closure. The levator ani muscles can support urethral closure by lifting the urethra, vagina, and anal canal in an anterior and superior direction (Bordoni & Launico, 2024). This essentially compresses the lumen of the urethra between the levator ani and the pubic bone to aid with urinary continence. Sometimes Kegel exercises are combined with an internal or external biofeedback device to give the patient visual and/or auditory feedback on the strength and timing of the pelvic floor muscle contraction. Although this method of pelvic floor strengthening can be effective in certain situations, newer research has provided clearer guidelines on when levator ani strengthening can be effective for reducing SUI.
A 2021 study examined the pathophysiology of SUI and found that the strongest predictor of someone experiencing stress urinary incontinence was the maximum strength of the urethral closure pressure, not levator ani muscle strength.(Falah-Hassani et al., 2021). This review also found that ‘defects of the periurethral ligaments were found in 76% of stress-incontinent women’, which is the structural cause of urethral hypermobility. It is important to recognize that pelvic floor muscle strengthening will likely not alleviate symptoms when fascial damage to the urethral support system is damaged. Another recent study showed levator ani muscle strength was not independently associated with decreased symptomatic SUI (Antônio et al., 2022). It should also be noted that overtraining the pelvic floor with Kegel exercises can lead to a worsening of symptoms. This is due to the relationship between the levator ani and the obturator internus muscle. When the levator ani becomes chronically hypertonic, this can lead to a compression of the perineal branch of the obturator nerve. Remember that the pudendal nerve passes through Alcock’s canal, which splits into branches, including the inferior rectal nerve, perineal nerve, and continues as the terminal branch to the dorsal nerve of the penis or clitoris (Kinter & Newton, 2023). The perineal nerve can become impinged in this region with a hypertonic obturator internus, leading to denervation of the external urinary sphincter. Fascinatingly, this is a reason why a patient can present with a ‘strong’ pelvic floor but also experience urinary incontinence. To summarize, pelvic floor muscle training can be an effective rehab strategy to cure or improve about 74% of people with SUI (Dumoulin et al., 2018).
It should be noted that pelvic floor muscle training aims to target the urethral sphincter to improve its strength. To specifically target the urethral sphincter, the instruction for the patient to contract their pelvic floor should bias the anterior pelvic floor. Someone may bias contracting their posterior pelvic floor muscles with a “Kegel,” which has little effect on the urethra. Remember, the neural innervation of the levator ani is by the nerve to levator ani, and the urethral sphincter is a branch of the pudendal nerve. Bulbocavernosus, the muscle within the vaginal opening, is also innervated by the same branch of the pudendal nerve. Cuing the patient to focus on the contraction of the bulbocavernosus in the superficial layer is a helpful way to instruct these exercises. An example is “squeeze your pelvic floor like you are trying to pick up a blueberry,” which is very different from “squeeze like you are holding back gas”. Therefore, it should also be noted that pelvic floor muscle training likely helps SUI because it helps strengthen the urethral sphincter, not the levator ani. Also, remember, in postpartum and post-menopausal women, there can be atrophy in the urethral sphincter from low estrogen levels that weakens the external urinary sphincter. This is effectively treated with vaginal estradiol cream in conjunction with pelvic floor muscle training (PFMT) (Te West et al., 2023).
Based on the current data we have related to SUI, about 25% of people will not respond significantly to pelvic floor muscle training. These are cases where there is likely fascial damage around the structures that support the urethral hypermobility. In cases of urethral hypermobility, an incontinence device such as a pessary or urethral support such as the Poise Impressa or Urestra should be considered. These devices sit in the vaginal canal and offer increased support to the urethra when intra-abdominal pressure increases. Incontinence pessaries can be sized and fit by a trained OBGYN, Urologist, or pelvic floor physical therapist. The over-the-counter options usually include a self-sizing kit with instructions for patients to navigate themselves. These devices are excellent options for self-management of urinary incontinence and allow many women to return to their desired activity level without concerns of leakage. There are surgical options for fixing urethral hypermobility as well.
It is important that treatment of either type of SUI also includes a comprehensive assessment of the patient's functional movement, including breathing patterns, intra-abdominal pressure management strategies, hip strength and range of motion, and other orthopedic factors such as impact training for running and jumping.
The diagnosis of urge incontinence falls under the diagnostic umbrella of Overactive Bladder (OAB), which is an incredibly vast and complex diagnosis that has a menu of treatment options. According to the American Urologic Association Guidelines, OAB has been defined as “urinary urgency, usually accompanied by frequency and nocturia, with or without urgency urinary incontinence (UUI), in the absence of urinary tract infection (UTI) or other obvious pathology.
From a rehab strategy perspective, the treatment revolves around addressing elevated sympathetic nervous system, behavioral strategies, and decreasing hypertonic or overactive pelvic floor musculature, which emphasizes the importance of the internal examination. It is also important to rule out constipation with this population, as excessive stool in the rectum can apply pressure forward to the bladder and cause urgency and leakage in certain cases. Evidence shows that transcutaneous tibial nerve stimulation (TTNS) can help with OAB symptoms as well (Bhide et al., 2020). TTNS aims to stimulate the L5-S3 nerve fibers via retrograde neuromodulation. This can increase the detrusor muscle's parasympathetic tone (relaxation), decreasing urinary urgency. If the clinician is properly trained, this can be performed with electrode pads or needle insertion and perineural electrical stimulation.
Clinically, it is possible to have a patient present with mixed urinary incontinence with any combination of stress, urge, overflow, or neurogenic components. To prescribe proper treatment modalities, the clinician must perform a thorough subjective interview to determine when the leakage occurs. Rehab providers should also understand that there are many nuances to address with OAB that go beyond the scope of this course. Often, referring this type of patient to a pelvic floor specialist is the best course of action.
Pelvic organ prolapse is a common diagnosis in the pelvic rehab setting, but it is a complex diagnosis to manage effectively. To fully understand pelvic organ prolapse (POP), we must first recognize the interplay of the support structures of the pelvic organs. The pelvic organs are supported by fascia and ligamentous structures, and the muscular structures support the fascia. To effectively treat POP, we need to understand which support structures within the pelvic cavity are compromised and how to functionally assess and address the strategies the patient has adopted to manage their symptoms that may not be effective.
According to the International Urogynecological Association, the criteria for diagnosis of pelvic organ prolapse require the descent of at least one vaginal wall (anterior, apical, or posterior) to be at or beyond the hymen, plus either bothersome characteristics or functional complications, such as incomplete bowel emptying (Collins et al., 2021). Objectively, assessing POP is done by performing a “POP-Q”, which is done by taking a series of measurements of the resting position of the bladder, uterus, and rectum, and then the position of each organ under strain or in the standing position. The test shows the movement of each of the vaginal walls when under strain, thus quantifying the degree of pelvic organ prolapse anatomically. An additional measurement in the POP-Q is the length of the Levator Hiatus (LH), which is the distance of the urethral meatus to the center of the anal opening. The LH can also be described as the Genital Hiatus (GH) + Perineal Body (PB). This is an important and clinically relevant measurement, as it is found that there is a correlation between the size of LH with symptom severity and prognosis of prolapse (Muñiz et al., 2021).
It should be noted that research has found that pelvic floor muscle training is appropriate and effective in managing stage 1 or 2 pelvic organ prolapse. A 2017 study showed a 43% symptomatic improvement in women with stage 1 or 2 prolapse after 6 months of pelvic floor muscle training(PFMT) (Panman et al., 2017). This is a positive change, but it should be noted that there was no change in anatomical prolapse. Remember that the primary organ support is fascial. Also, note that the purpose of PFMT is to improve the support function of the pelvic floor; this is different from solely improving the strength of a pelvic floor muscle contraction. When done effectively, PFMT may help reduce the size of the levator hiatus. Cuing for PFMT in these cases can include contraction of posterior to anterior to achieve full levator ani contraction: “Squeeze like you are pulling your rectum toward your pubic bone”. Incorrect PF muscle contraction is associated with SUI and POP (Henderson et al., 2013). Pelvic floor rehab providers play an important role in teaching their patients proper contraction, coordination, and awareness of the pelvic floor musculature.
If the organ is sitting within the levator hiatus, or past the hymen (which is a stage 3 or 4 prolapse), treatment options have to expand beyond PFMT. This is where pessary use or surgical intervention becomes the most beneficial choice. A pessary is a medical-grade silicone device that is individually fitted according to the person’s anatomical needs, which helps lift the organ. With the organ sitting higher, pressure is taken off the fascial structures being stretched downward, and PFMT can now be more effective. A 2020 study showed that when combining pessary use and pelvic floor muscle training, more women perceived improvements in symptoms and quality of life (Bugge et al., 2020).
A fascinating case study showed potential for POP recovery when pessaries and PFMT are used in the immediate postpartum period. A woman sought care at 1 year postpartum with significant symptoms and anatomical prolapse of all three compartments. She was fitted with a cube pessary and instructed on PFMT. Within 7 months, she had no symptoms, no need to wear the pessary daily, her LH had gone from 6cm to 4cm, and her uterus was in a normal anatomical position with no anterior or posterior wall prolapse (Nemeth & Ott, 2011). No large studies have been done on the immediate postpartum period, but this is a very exciting finding and an important population to which to apply these concepts.
Typically, OBGYNs and urogynecologists are trained in fitting pessaries, but it is becoming more common for pelvic physical therapists to be trained in fitting pessaries. Co-managing risks, infections, or hormonal implications with the patient’s doctor must be considered.
It is important to recognize that the research shows us there is a difference in anatomical recovery depending on the type of prolapse. A uterine or bladder prolapse may improve when treated with a combination of a pessary and pelvic floor strengthening. Still, a rectocele does not show anatomical change with the same approach. There can, however, still be symptomatic improvement with a rectocele, but it is important to understand and explain the difference to the patient. There is currently no evidence that levator ani muscle strength, presence of levator avulsion, or LH size is linked with posterior POP recovery (Berger et al., 2018; Dietz & Simpson, 2008). If a patient presents with a rectocele and has issues with incomplete bowel emptying, it has been shown that intra-vaginal and perineal splinting can improve bowel emptying (Apostolis et al., 2012). Splinting is performed by teaching the patient to place one finger intravaginally on the posterior vaginal wall while having a bowel movement. If symptoms cannot be managed with conservative and lifestyle treatment, surgery is the best option for posterior prolapses or rectoceles.
As noted in the SUI section, it is imperative that pelvic therapists also assess and treat the patient’s ability to manage pressure in their abdomen when coughing, sneezing, and lifting, and truly understand the patient's lifestyle habits that may contribute to their symptoms. For example, someone with a bladder prolapse may strain when they urinate to be able to fully empty, but this may further weaken their pelvic floor. In this case, a pessary and addressing toileting positions may help prevent the straining and allow the pelvic floor to strengthen properly. Pelvic therapists also need to address other musculoskeletal impairments, such as hip weakness or ankle stiffness, to improve biomechanics and the system's resilience. This is our role in helping each patient functionally.
Pelvic pain is an umbrella term for many differential diagnoses that can range from sexual dysfunction to bowel and bladder changes, nerve entrapments, autoimmune conditions, and orthopedic abnormalities. The goal of this section is to highlight some of these differential diagnoses and common conditions, improve confidence in screening for them, and provide the most effective treatment options.
Coccydynia, or tailbone pain, is a common complaint in pelvic floor therapy. The most common causes of tailbone pain are external trauma from something like a backward fall onto the coccyx or internal trauma from childbirth. Remember that the Cozean Pelvic dysfunction Screening has a question specific to falling on your tailbone or lower back. Also, remember that the levator ani attaches to the anterior portion of the coccyx and the sacrotuberous and sacrospinous ligaments. The position and anatomy of the coccyx provide weight-bearing support while sitting upright, and aid in voluntary bowel control as a posterior anchor point for the levator ani (Lirette et al., 2014). A vaginal exam can be utilized to identify muscle tension that reproduces tailbone pain, but a rectal exam is often more specific. Secondarily, the external mobility of the sacrum and muscle guarding in the gluteals can also help the therapist identify coccyx dysfunction. Manual muscle release can be useful in alleviating symptoms, but sometimes the coccyx itself is the source of pain, which might require further imaging and medical intervention. Educating patients on proper sitting position and using a donut pillow, or coccyx relief pillow, is sometimes necessary to allow patients to tolerate sitting when they do not respond to physical therapy. Steroid injections are sometimes necessary to reduce pain and inflammation, and in extreme cases, surgical removal of the coccyx may be a last resort (Lirette et al., 2014).
Vaginismus is a pelvic pain condition that is defined by recurrent or persistent involuntary spasms of the musculature of the outer third of the vagina. This results in a fear of vaginal penetration and is characterized as more of a psychological disorder than physical (Raveendran & Rajini, 2024). Vaginismus may also present with signs such as glute hypertonicity and an autonomic response to palpation in the genital region. This contrasts with dyspareunia, which is a more generalized term for pelvic or genital pain specifically with penetration, tampons, or pelvic exams, and the symptoms are more physical than psychological. Dyspareunia typically responds well to pelvic floor muscle release and patient education. This differs from the approach to treating vaginismus, which should incorporate a bio-psycho-social model, and also brings up the importance of trauma-informed care.
Painful intercourse can be a complex topic because the patient may have a history of sexual, emotional, or psychological trauma that needs to be addressed either with a counseling professional or with a physical therapist, depending on their comfort level. Not only should pelvic therapists be open to discussing this topic, but sexual trauma is so prevalent in women that all patients should at least be screened for this in their intake paperwork. When patients have an openness to the role of trauma when it comes to pelvic pain, this tends to lead to more progress with pelvic floor therapy.
Vulvodynia is a condition characterized by vulvar pain and sensitivity that can cause bowel and bladder changes along with painful intercourse. A vulvar exam can be performed visually to identify the need for a referral to a gynecologist or dermatologist if discoloration, atrophy, or fissures are present (Prendergast, 2017). For pelvic floor therapists, treatment should be multimodal and focus on tissue desensitization and pelvic floor muscle release. Trauma-informed care should be incorporated as well.
Interstitial Cystitis or Bladder Pain Syndrome is a complex medical condition that affects the urinary bladder. It is characterized by chronic, non-infectious urinary symptoms such as urgency, frequency, and bladder pain. Research is improving in this field, but it is still viewed as a diagnosis of exclusion that should incorporate a multi-disciplinary approach (Lim et al., 2024). The American Urological Association released a guideline for the treatment of interstitial cystitis. Manual therapy performed by trained pelvic floor physical therapists was the only recommendation made with Grade A evidence (Clemens et al., 2022). This is due to a high prevalence of pelvic floor dysfunction present in individuals with interstitial cystitis. This topic is highly complex and will also require a symptom-based approach, but pelvic floor therapy is currently one of the best treatments available.
Endometriosis is the presence of ectopic endometrial glands and stroma outside the uterus (Chaudhry & Chaudhry, 2023). This is a condition that is characterized by painful, heavy periods, abdominal pain, and bloating, which can lead to fertility issues. Endometriosis can be diagnosed with ultrasound, but an exploratory laparoscopy is often performed. In cases where women are not interested in preserving fertility, a hysterectomy with or without oophorectomy may be performed (National Institute for Health and Care Excellence [NICE], 2024). In cases where women want to avoid hysterectomy, endometriosis excision surgery is the preferred treatment. Historically, endometrial ablation surgeries were performed, but were less effective due to residual scarring and inflammation (Bignardi et al., 2019). Women with endometriosis may seek out pelvic floor therapy before, during, or after medical management, and may want to avoid surgery altogether. Treatment should focus on manual therapy interventions to reduce pelvic pain, as well as general exercise prescription for anti-inflammatory effects. Visceral manual therapy should be considered due to the likelihood of adhesions, scarring, and inflammation in the abdominopelvic cavity (Wójcik et al., 2022).
Pudendal Neuralgia is another common condition in pelvic floor rehab, but orthopedic therapists will also experience this in their practice. This is a peripheral nerve entrapment that can cause bowel and bladder dysfunction, autonomic dysfunction, and perineal pain/numbness. The most common report is symptoms exacerbated by sitting, and the nerve can be entrapped in several different sites, which will dictate treatment. The areas that the pudendal nerve can be entrapped include (Leslie et al., 2024):
Type I: Below the piriformis as the nerve exits through the greater sciatic notch
Type II: between the sacrospinous and sacrotuberous ligaments; the most common site of pudendal nerve entrapment
Type III: within Alcock's canal
Type IV: terminal nerve branches only (ie, inferior rectal nerves, superficial and deep perineal nerves, and the dorsal nerve of the penis or clitoris)
Myofascial release, scar mobilization, central nervous system (CNS) downtraining, TENS, and activity modification are the primary treatments from a physical therapy standpoint. Patients experiencing chronic pudendal neuralgia will likely need interprofessional management with other possible treatments such as pudendal nerve blocks, pharmaceuticals, and cognitive behavioral therapy (Leslie et al., 2024). Remember that vaginal birth can also damage the pudendal nerve and contribute to urinary incontinence. This condition, pudendal neuropraxia, results in temporary or permanent atrophy of the external urethral sphincter (Cramer et al., 2021).
Constipation is a common complaint in the pelvic floor rehab setting. It is estimated that 15% of the U.S. population experiences chronic constipation, and upwards of 30% in older adults (Diaz et al., 2023). This number will likely continue to grow as the general population becomes increasingly more sedentary and consumers of highly processed diets. The American College of Gastroenterology defines constipation based upon symptoms, including unsatisfactory defecation with infrequent stools, difficulty passing stool, or both. Constipation can develop for various reasons, and symptom resolution depends on identifying the root cause. Unfortunately, pelvic floor therapy is not usually recommended until multiple treatments have failed and symptoms have become more chronic. In the realm of pelvic floor rehabilitation, the following exam components and treatment options serve as a good starting point.
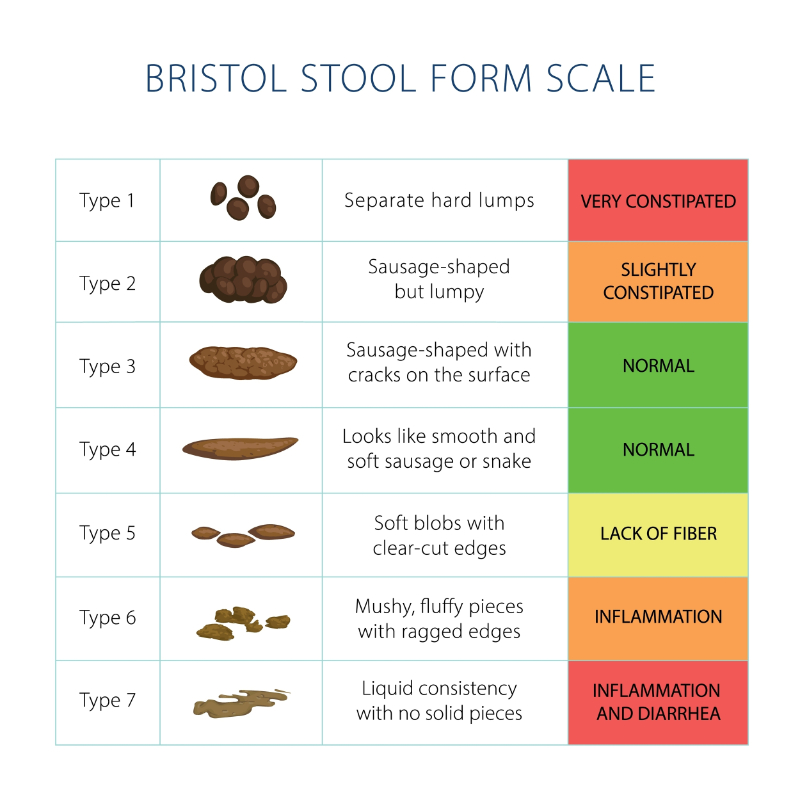
A thorough history of symptoms, frequency of bowel movements, quality of bowel movements, time spent on the toilet, toilet position, and stress/anxiety levels should be asked about during the subjective interview. Using the Bristol Stool Scale when asking about stool quality is helpful, as well as asking if the patient passes stool completely or partially. In cases where patients report incomplete emptying, pelvic floor tightness, and anal sphincter control should be assessed.
Image 9: Bristol Stool Chart
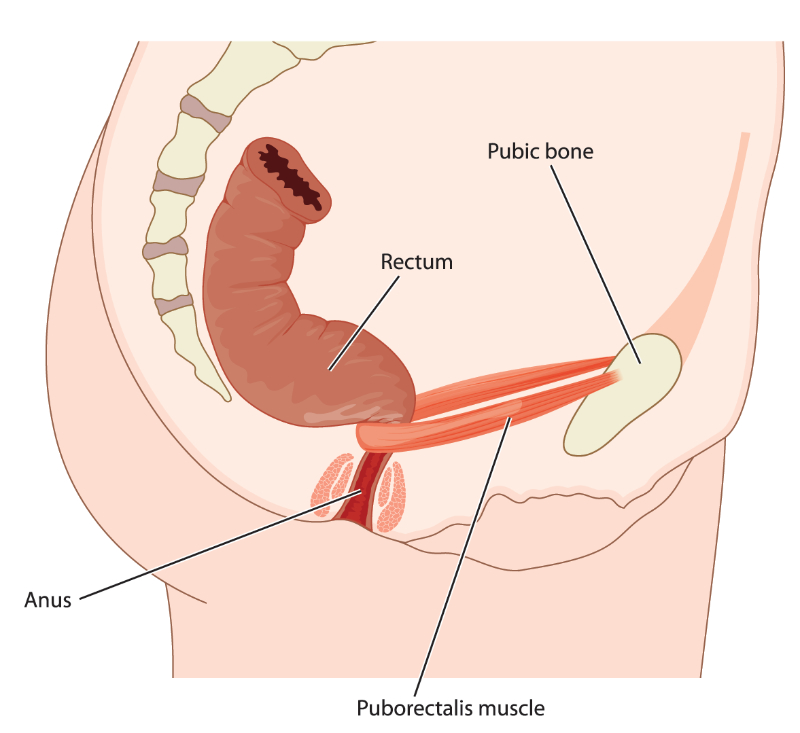
A 2010 study looked at the influence of body position on defecation. Their primary results found that greater hip flexion angles aided defecation by straightening the rectum and requiring less straining (Sakakibara et al., 2010). This is due to the anatomy of the levator ani, specifically the puborectalis, which creates a sling around the rectum and tightens to maintain fecal continence. The puborectalis muscle relaxes more with deeper angles of hip flexion, and this leads pelvic floor therapists to often recommend a stool, such as a squatty potty, for improved bowel function. The loss of deep hip flexion in the elderly population could also explain why the prevalence of constipation increases with age.
Image 10: Rectal Anatomy
In 2022, the American Physical Therapy Association (APTA) released a clinical practice guideline for the interventions that should be utilized with functional constipation in adults. Strong evidence supports the following interventions (LaCross et al., 2022).
Electromyographic biofeedback with internal or external anal sensors.
Rectal balloon catheter biofeedback training.
Anorectal manometry biofeedback training.
Abdominal massage, including visceral mobilization.
Electrical stimulation and general manual therapy were also suggested, with weak quality of evidence.
When appropriate, the use of biofeedback should be the first line of treatment for pelvic floor therapists treating constipation. Unfortunately, therapists in traditional outpatient settings do not usually have access to the types of biofeedback devices recommended in this CPG, nor do they have the training to utilize them. In cases where therapists cannot access biofeedback or are not properly trained, visceral and abdominal massage can be performed with great results (Gu et al., 2023). Therapists can show patients how to perform a ‘colon massage’ with appropriate training. This is done starting at the cecum in the right lower quadrant, and having the patient gently sink into their abdomen to perform several circular motions with their hands. This pattern can be followed up the ascending colon, across the transverse colon, and down the descending colon with proper training of landmarks and pressure to the organ. Manual pressure on the valves of the gastrointestinal system can also aid with bloating, distention, and constipation. This includes the lower esophageal sphincter, pyloric sphincter, sphincter of Oddi, duodenojejunal junction, and the ileocecal valve. Because these valves require more skilled and specific palpation to effectively treat, this should be reserved for those with ongoing visceral manipulation/mobilization education.
Another component of managing constipation includes evaluating pelvic dyssynergia. This occurs when abdominal pressure with bearing down and pelvic floor relaxation cannot be properly coordinated. It is estimated that up to half of all people who experience chronic constipation have defecation dyssynergia (Rao & Patcharatrakul, 2016). This can be assessed manually by feeling if the posterior pelvic floor tenses or relaxes while bearing down. When biofeedback is available, patients can see when they are contracting and relaxing their posterior pelvic floor.
A final consideration for therapists treating constipation is the role of the central nervous system. The gut-brain axis is a bidirectional communication system between the central nervous system and the digestive tract. The vagus nerve is the primary communication between the brain and the intestine and is responsible for regulating digestion and contracting smooth muscle in the viscera (Kraimi et al., 2024). This study highlights the fact that there is growing evidence to support the link between psychological health and gastrointestinal disorders. This includes stress, anxiety, sleep disorders, and depression, to name a few. While gut-brain axis disorders apply to much more than constipation, therapists should utilize CNS down-training techniques, vagus nerve stimulation, breathwork, and other appropriate modalities to comprehensively treat those experiencing chronic gastrointestinal dysfunction.
Fecal incontinence (FI) is another condition that pelvic floor rehab providers may see in the clinic. Fecal incontinence or fecal smearing is present in 7-15% of adults. Still, this number may be underreported due to providers not screening for it and patients not volunteering this information (Bharucha et al., 2015). The cause of FI is not always clear, but common risk factors include baseline bowel disorders like diarrhea, fecal urgency, as well as chronic disease, comorbidities, anal sphincter injuries, and pelvic floor disturbances like rectal prolapse. The treatment of fecal incontinence will again involve a symptom-based approach and depend on identifying underlying mechanisms. Remember that the autonomic nervous system innervates the internal anal sphincter, and the inferior rectal nerve innervates the external anal sphincter via the pudendal nerve. Because of this, CNS downtraining and pelvic floor awareness should both be utilized as a starting point.
Although the vast majority of pelvic floor rehab is provided to females, there are multiple common male pelvic floor conditions that rehab providers should be aware of and prepared to treat. The goal of this section is to understand the basic pathology and treatment options for the most common clinical presentations, while also building confidence in therapists’ abilities to treat males in the pelvic floor rehab space. Similar to the female exam, a comprehensive male pelvic floor exam should include a gathering of relevant medical history including any mental, physical, or sexual trauma, timing and frequency of symptoms, diet and lifestyle habits, liquid intake (type and quantity), and a review of any imaging or urology exams such as urinalysis, urodynamic testing, or prostate-specific antigen (PSA). A typical orthopedic screen, looking at back and hip ROM, posture, and strength, should be done. Following this, pelvic floor therapists should perform an external pelvic floor assessment and palpation of the ischial tuberosities, the pubic rami, bladder, and the sacrospinous and sacrotuberous ligaments. Finally, an intra-rectal muscle assessment should be performed digitally. This can be done in hooklying, sidelying, or prone, depending on patient comfort level and therapist preference. The rectal assessment is a critical component of the male pelvic floor exam because it can rule in/out so many different symptom contributors. Oftentimes, therapists may lack the confidence or training to perform a rectal exam, but without it, it is not possible to get the full clinical picture of why the patient has come for treatment.
Urinary incontinence is among the most common reasons men seek out pelvic floor physical therapy. After a thorough exam with a male client, treatment options will depend on identifying the primary causes of symptoms. There is not much consensus on post-micturition dribbling (PMD) rates, but it is estimated that 20-30% of middle-aged men experience it. The prevalence also increases with age and is correlated with incomplete bladder emptying (Liu et al., 2023). The male urethra is approximately 4-5 times longer than the female urethra. This can be an explanation of why some men experience post-micturition dribbling. Urine can be retained in different parts of the urethra following urination, but there are several evidence-based remedies. The simplest way to relieve post-void dribbling is bulbar urethral massage. The patient does this technique by placing his hand behind the scrotum shortly after urination in the area of the bulbar urethra. He is then instructed to massage the tissue anteriorly toward the penis several times until there is no residual urine (Yang & Lee, 2019). This study found that combining bulbar urethral massage with pelvic floor muscle training of the bulbospongiosus and ischiocavernosus to be highly effective in relieving post-micturition dribbling. The focus on anterior pelvic floor muscle training is the key to urinary incontinence in men. Clinicians can provide manual feedback with intra-rectal palpation. When done correctly, the patient should create a lifting sensation in the anterior pelvic floor. Verbal cues can also be utilized, such as ‘contract as if you are trying to stop the flow of urine’ or ‘try to lift your penis.’This is in contrast to a posterior pelvic floor contraction, where the patient could be asked to hold back gas. Clinicians should also be mindful to limit pelvic floor muscle training dosage to avoid creating hypertonicity.
Prostate enlargement or Benign Prostatic Hypertrophy (BPH) is another common condition in the pelvic floor rehab space. The NIH National Cancer Institute defines BPH as a benign (non-cancerous) condition in which the prostate gland is enlarged. This can cause symptoms of a weak urine stream, difficulty initiating a urine stream, urinary dribbling, and painful urination or ejaculation. BPH also increases with age, and upwards of 80% of men over 70 experience the disorder (Ng et al., 2024). Unfortunately, this results in urinary retention and causes men to have to strain to pee and use the bathroom frequently. The best course of action is to refer this type of patient to a urologist. Medical management of BPH can be effective either through pharmaceutical options such as Flomax (tamsulosin), which helps relax the bladder and prostate tissue for easier urination, as well as several surgical options to reduce the size of the prostate or reduce compression of the urethra. Pelvic floor therapists may see a patient before, during, or after they have had medical interventions for BPH, and their role is to optimize the function of the surrounding tissue.
When prostate pathology is cancerous, men may go through several forms of treatment, including chemotherapy, radiation, hormone therapy, and, in some cases, prostatectomy. Medical advancements are making treatment more effective while also minimizing side effects. Despite this, urinary incontinence is a common complication of a partial or radical (complete) prostatectomy. Once cleared by their surgeon, males should be referred to pelvic floor physical therapy. A 2022 study examined the effectiveness of pelvic floor muscle training following radical prostatectomy (Szczygielska et al., 2022). Their study was performed with subjects experiencing urinary incontinence and divided into three groups:
Pelvic floor muscle training with radical prostatectomy less than 6 weeks prior
Pelvic floor muscle training plus biofeedback with radical prostatectomy less than 6 weeks prior
Pelvic floor muscle training with radical prostatectomy greater than 6 weeks prior
A 10-week program was utilized with supervised pelvic floor muscle training in supine, seated, and standing positions and a home exercise protocol. Subjects were also instructed to initiate and then stop the flow of urine once per day to increase the tone of the urethral sphincter. The results were assessed by measuring the amount of urine leaked onto a pad in the hour following their in-person sessions. The group results were as follows at 10 weeks:
60% of participants regained full control of micturition
85% of participants regained full control of micturition
45% of participants regained full control of micturition
The takeaway from this study is that pelvic floor muscle training causes a significant positive change in urinary incontinence symptoms. There is a positive correlation between starting treatment sooner and completing the resolution of symptoms. Biofeedback should be used in addition to pelvic floor muscle training when available. It is also worth mentioning that certain prostate surgery techniques, such as a transurethral resection, can permanently damage the internal urethral sphincter. Because the external urethral sphincter is preserved, the patient may not have any effect on continence, but would experience retrograde ejaculation (Sam et al., 2025).
Pelvic floor physical therapy can also be beneficial in the treatment of erectile dysfunction (ED), but will not be discussed in detail in this course. Many of the interventions already discussed can help with ED, such as manual therapy techniques to reduce hypertonicity, breathwork for pelvic floor relaxation, and pelvic floor muscle training when hypertonicity is not the primary driver of symptoms. ED should also be evaluated from a behavioral point of view and can involve other healthcare providers outside of a physical therapist's scope of practice (Yaacov et al., 2022).
Hernias are another common condition that pelvic floor therapists will see in men and women. There are several primary types of hernias that rehab providers should be able to treat pre- and post-operatively. We will focus on umbilical and inguinal hernias in this course due to the primary mechanisms in which they occur. Umbilical hernias are common during pregnancy and postpartum in women. This is due to the stretching of the abdominal tissue and separation of the rectus abdominis described earlier in the diastasis recti section. This type of hernia can also occur with poor intra-abdominal pressure management, core weakness, and obesity in both genders. Inguinal hernias are the most common type of hernia, accounting for approximately 75% of cases, and are more common in men by a factor of 10, according to the Cleveland Clinic. Inguinal hernias can be managed conservatively, but patients often opt for surgery due to pain and activity limitations. Most surgeons do not refer patients to PT after surgical hernia repairs. A 2022 study surveyed physicians’ perceptions and utilization of physical therapy following surgical hernia repair and reported that the overall use of PT was listed as ‘occasionally’ 42% of the time and ‘rarely’ 27% of the time. The common reasons selected from those not referring to physical therapists included lack of education and evidence of clinical benefit (Renshaw et al., 2022). Another study reviewed the reoperation rate for recurrent hernias and found that 18.8% of minimally invasive hernia repairs required reoperation within 10 years of the initial surgery (Howard et al., 2022). This should be a call to action for physical therapists to educate their patients, local surgeons, and the community on what we can do to help people heal following hernia repair and reduce waste in the medical system.
A physically active 61-year-old male presents to physical therapy, self-referred, 3 weeks status post direct inguinal hernia repair with mesh placement. He enjoys mountain biking, hiking, and cross-country skiing, and would like to return to the activity as soon as possible without exacerbating the hernia pain. Several weeks prior, he had been doing a core workout that included several hundred crunches, bicycles, and russian twists, and he would do this 3 times per week. During a russian twist, he felt a subtle pop in his groin and had to stop his workout due to 4/10 pain. Symptoms subsided over the next week but came on more intensely when he described rotating and picking up a suitcase to load his car for a trip. Pain was so severe that he could not stand up straight or exert himself beyond simple mobility around the house. At this point, he had a surgical consult, and the hernia repair with mesh was completed 4 weeks later. The patient’s surgeon did not give him any guidelines beyond ‘resting’ and ‘taking it easy’ for 3 weeks, and then he could gradually return to activity. Because the patient had an upcoming ski trip planned 3 weeks post-op and was interested in restoring some strength and endurance before this, he sought out pelvic physical therapy on his own.
On exam, the patient had severely limited lumbar mobility primarily in extension, along with limited thoracic rotation, hypertonicity in the glutes and tensor fascia latae bilaterally, tenderness to palpation over the hernia repair site, and demonstrated no awareness of the transverse abdominis muscle. The patient was also guided to reschedule his ski trip to allow for complete surgical healing, and he complied.
The first treatment session consisted of manual therapy and dry needling to reduce pain and tension in the hip flexors and thoracolumbar junction. The home exercise program consisted of thoracic rotation exercises and 360 breathing to incorporate lower rib cage motion and reduce pressure on the hernia repair. One week later, the patient returned with reports that he had begun walking outside daily and only had minimal pain. The second treatment session focused on introducing the deep core brace. This was challenging for the patient, both physically and mentally, because he had difficulty recruiting a part of his core that had not been trained in the past. His home exercise program in the second and third week consisted of endurance holds with the deep core while breathing to achieve proper intra-abdominal pressure management. By six weeks post-op, his spine mobility, core activation, and breathing patterns were all improving. This session incorporated basic lower body lifting principles with core activation and breathwork, and he responded well with 1 day of mild soreness in his back and glutes. At 8 weeks post-op, the patient could perform more complex core movements such as dead bug and bird dog while breathing and maintaining deep core activation. He was cleared by physical therapy to resume progressive strengthening and return to skiing.
The treatment plan was simple from a physical therapy standpoint. Still, it is important to highlight this case because most physical therapists possess the knowledge and training to rehab this type of surgery and minimize long-term complications. This patient lacked a proper foundation of core stability, breathing patterns, and mobility, which we can assume were all contributing factors to the initial injury. After just 5 weeks of rehab, this patient left with a remarkable change in his mindset towards core work and had the confidence to return to all activities without the fear of re-injury.
A 47 y/o female presenting with painful intercourse, urinary leakage, and bowel and bladder urgency. She also has back pain, a recent elbow surgery, and a high degree of stress due to moving out of state recently. Her pelvic floor history included three vaginal deliveries, an umbilical hernia repair, IBS, and partial hysterectomy. She reported she changes clothes multiple times a day due to leakage and has to strain to empty her bowels. She was anxious about leaking, her pain, and feeling generally weak and fearful of injuring herself.
Her evaluation found she had left > right Pelvic floor muscle hypertonicity and tenderness in the second and third layers. Right glute medius strength was 2 / 5 with manual muscle testing with a compensated Trendelenburg gait pattern. She had poor intra-abdominal pressure management and approximately three finger (3 cm) diastasis recti with doming that also caused bearing down into the pelvic floor when she would cough, laugh, or try to recruit her core. Also of note is that she could not rise from a kneeling to a standing position due to back pain and lower extremity weakness.
Initial treatment included breathing coordination, manual trigger point release of the pelvic floor muscles, and teaching inner core activation. Initially, manual pelvic floor release would take 45 minutes with breathwork, downtraining, external tissue slacking, and passive hip range of motion exercise. Next, she was instructed on proper core activation, starting with isometric adduction of the hips during the exhale and adding recruitment of the anterior pelvic floor and lower core. This treatment progressed over the next 4 weeks. During these initial 4 weeks, she began seeing improvements in leakage and urgency. She noted that intercourse was less painful after 6 weeks of treatment.
At this stage, the treatment focus was transitioned to lower extremity and hip strengthening exercises. The foundation of inner core activation and exhaling on exertion was utilized to assist her coordination. During this time, she had a few episodes of mid-back pain flares. A bio-psycho-social approach to addressing her fears, helping calm her nervous system, and addressing fear with movement was also implemented. Her treatment progressed to dynamic core and lower extremity strengthening. After 3 months of treatment, she felt confident to join a local gym and began some group exercise classes.
This case study highlights several components of pelvic floor rehab. The first being that patients will oftentimes be experiencing multiple pelvic floor symptoms by the time they are evaluated, and will benefit from a comprehensive exam to identify all of the contributing factors. It should also be noted that myofascial and trigger point release of the pelvic floor can sometimes take multiple sessions, and the therapist should use this time to educate and bring awareness to an area of the body that many patients lack an understanding of. Finally, rehab does not stop when patients stop experiencing symptoms, but rather when the tissues and body systems are resilient enough to allow lasting changes.
In conclusion, pelvic floor rehabilitation plays a crucial role in restoring function, reducing pain, and improving quality of life for individuals affected by pelvic floor dysfunction. Through a combination of evidence-based interventions such as pelvic floor muscle training, biofeedback, manual therapy, and patient education, clinicians can offer effective, individualized care. Continued research and interdisciplinary collaboration are essential to advance treatment outcomes and refine therapeutic approaches. As awareness and understanding of pelvic floor health continue to grow, so too does the potential for rehabilitation to make a lasting impact on patient well-being.
For those still interested in pelvic floor rehab, the next best step is to register for an in-person lab-based pelvic floor course to gain hands-on patient treatment skills.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Angolile, C. M., Max, B. L., Mushemba, J., & Mashauri, H. L. (2023). Global increased cesarean section rates and public health implications: A call to action. Health Science Reports, 6(5), e1274. Visit Source.
Antônio, F. I., Rodrigues, M. P., Brooks, K., Varette, K., & McLean, L. (2022). What improvements in levator ani motor function lead to improvement in stress urinary incontinence signs and symptoms in females? International Urogynecology Journal, 33(10), 2735–2747. Visit Source.
Apostolis, C., Wallace, K., Sasson, P., Hacker, M. R., Elkadry, E., & Rosenblatt, P. L. (2012). Assessment of women with defecatory dysfunction and manual splinting using dynamic pelvic floor magnetic resonance imaging. Female Pelvic Medicine & Reconstructive Surgery, 18(1), 18–24. Visit Source.
Artal R. (2015). The role of exercise in reducing the risks of gestational diabetes mellitus in obese women. Best practice & research. Clinical Obstetrics & Gynaecology, 29(1), 123–132. Visit Source.
Berger, M. B., Kolenic, G. E., Fenner, D. E., Morgan, D. M., & DeLancey, J. O. L. (2018). Structural, functional, and symptomatic differences between women with rectocele versus cystocele and normal support. American Journal of Obstetrics and Gynecology, 218(5), 510.e1–510.e8. Visit Source.
Bharucha, A. E., Dunivan, G., Goode, P. S., Lukacz, E. S., Markland, A. D., Matthews, C. A., Mott, L., Rogers, R. G., Zinsmeister, A. R., Whitehead, W. E., Rao, S. S., & Hamilton, F. A. (2015). Epidemiology, pathophysiology, and classification of fecal incontinence: state of the science summary for the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) workshop. The American Journal of Gastroenterology, 110(1), 127–136. Visit Source.
Bhide, A. A., Tailor, V., Fernando, R., Khullar, V., & Digesu, G. A. (2020). Posterior tibial nerve stimulation for overactive bladder-techniques and efficacy. International Urogynecology Journal, 31(5), 865–870. Visit Source.
Bignardi, T., Khong, S. Y., & Lam, A. (2019). Excisional versus ablative surgery for peritoneal endometriosis. The Cochrane Database of Systematic Reviews, 2019(7), CD008979. Visit Source.
Bolla, S. R., Hoare, B. S., & Varacallo, M. A. (2023). Anatomy, abdomen and pelvis: Deep perineal space. In StatPearls. StatPearls Publishing. Visit Source.
Bordoni, B., & Launico, M. V. (2024). Anatomy, abdomen and pelvis, perineal body. In StatPearls. StatPearls Publishing. Visit Source.
Bugge, C., Adams, E. J., Gopinath, D., Stewart, F., Dembinsky, M., Sobiesuo, P., & Kearney, R. (2020). Pessaries (mechanical devices) for managing pelvic organ prolapse in women. The Cochrane Database of Systematic Reviews, 11(11), CD004010. Visit Source.
Chaudhry, S. R., & Chaudhry, K. (2023). Anatomy, abdomen and pelvis: Uterus round ligament. In StatPearls. StatPearls Publishing. Visit Source.
Chaudhry, S. R., Imonugo, O., Jozsa, F., & Chaudhry, K. (2023). Anatomy, abdomen and pelvis: Ligaments. In StatPearls. StatPearls Publishing. Visit Source.
Chidi-Ogbolu, N., & Baar, K. (2019). Effect of estrogen on musculoskeletal performance and injury risk. Frontiers in Physiology, 9, 1834. Visit Source.
Chu, S. R., Boyer, E. H., Beynnon, B., & Segal, N. A. (2019). Pregnancy results in lasting changes in knee joint laxity. PM & R: the Journal of Injury, Function, and Rehabilitation, 11(2), 117–124. Visit Source.
Clemens, J. Q., Erickson, D. R., Varela, N. P., & Lai, H. H. (2022). Diagnosis and treatment of interstitial cystitis/bladder pain syndrome. The Journal of Urology, 208(1), 34–42. Visit Source.
Collins, S. A., O'Shea, M., Dykes, N., Ramm, O., Edenfield, A., Shek, K. L., van Delft, K., Beestrum, M., & Kenton, K. (2021). International urogynecological consultation: Clinical definition of pelvic organ prolapse. International Urogynecology Journal, 32(8), 2011–2019. Visit Source.
Conder, R., Zamani, R., & Akrami, M. (2019). The biomechanics of pregnancy: A systematic review. Journal of Functional Morphology and Kinesiology, 4(4), 72. Visit Source.
Cramer, M. S., Boniface, E. R., Holland, A., & Gregory, W. T. (2021). Changes in morphology of the urethral rhabdosphincter postpartum. Female Pelvic Medicine & Reconstructive Surgery, 27(3), 181–185. Visit Source.
Diaz, S., Bittar, K., Hashmi, M. F., & Mendez, M. D. (2023). Constipation. In StatPearls. StatPearls Publishing. Visit Source.
Dietz, H. P., & Simpson, J. M. (2008). Levator trauma is associated with pelvic organ prolapse. BJOG: An International Journal of Obstetrics and Gynaecology, 115(8), 979–984. Visit Source.
Doumouchtsis, S. K., de Tayrac, R., Lee, J., Daly, O., Melendez-Munoz, J., Lindo, F. M., Cross, A., White, A., Cichowski, S., Falconi, G., & Haylen, B. (2023). An International Continence Society (ICS)/ International Urogynecological Association (IUGA) joint report on the terminology for the assessment and management of obstetric pelvic floor disorders. International Urogynecology Journal, 34(1), 1–42. Visit Source.
Dumoulin, C., Cacciari, L. P., & Hay-Smith, E. J. C. (2018). Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. The Cochrane Database of Systematic Reviews, 10(10), CD005654. Visit Source.
Fahmy, M. W., Sanganeria, T., & Munakomi, S. (2022). Anatomy, abdomen and pelvis: Superficial perineal space. In StatPearls. StatPearls Publishing. Visit Source.
Falah-Hassani, K., Reeves, J., Shiri, R., Hickling, D., & McLean, L. (2021). The pathophysiology of stress urinary incontinence: A systematic review and meta-analysis. International Urogynecology Journal, 32(3), 501–552. Visit Source.
Fiani, B., Sekhon, M., Doan, T., Bowers, B., Covarrubias, C., Barthelmass, M., De Stefano, F., & Kondilis, A. (2021). Sacroiliac joint and pelvic dysfunction due to symphysiolysis in postpartum women. Cureus, 13(10), e18619. Visit Source.
Gilbert, I., Gaudreault, N., & Gaboury, I. (2022). Exploring the effects of standardized soft tissue mobilization on the viscoelastic properties, pressure pain thresholds, and tactile pressure thresholds of the cesarean section scar. Journal of Integrative and Complementary Medicine, 28(4), 355–362. Visit Source.
Gowda, S. N., & Bordoni, B. (2022). Anatomy, abdomen and pelvis: Levator ani muscle. In StatPearls. StatPearls Publishing. Visit Source.
Grimes, W. R., & Stratton, M. (2023). Pelvic Floor Dysfunction. StatPearls - NCBI Bookshelf. Visit Source.
Guralnick, M. L., Fritel, X., Tarcan, T., Espuna-Pons, M., & Rosier, P. F. W. M. (2018). ICS Educational Module: Cough stress test in the evaluation of female urinary incontinence: Introducing the ICS-Uniform Cough Stress Test. Neurourology and Urodynamics, 37(5), 1849–1855. Visit Source.
Gürşen, C., İnanoğlu, D., Kaya, S., Akbayrak, T., & Baltacı, G. (2016). Effects of exercise and Kinesio taping on abdominal recovery in women with cesarean section: A pilot randomized controlled trial. Archives of Gynecology and Obstetrics, 293(3), 557–565. Visit Source.
Gu, X., Zhang, L., Yuan, H., & Zhang, M. (2023). Analysis of the efficacy of abdominal massage on functional constipation: A meta-analysis. Heliyon, 9(7), e18098. Visit Source.
Hall, H., & Sanjaghsaz, H. (2023). Diastasis recti rehabilitation. In StatPearls. StatPearls Publishing. Visit Source.
Haylen, B. T., de Ridder, D., Freeman, R. M., Swift, S. E., Berghmans, B., Lee, J., Monga, A., Petri, E., Rizk, D. E., Sand, P. K., & Schaer, G. N. (2010). An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. International Urogynecology Journal, 21(1), 5–26. Visit Source.
Henderson, J. W., Wang, S., Egger, M. J., Masters, M., & Nygaard, I. (2013). Can women correctly contract their pelvic floor muscles without formal instruction? Female Pelvic Medicine & Reconstructive Surgery, 19(1), 8–12. Visit Source.
Hesketh, K. R., & Evenson, K. R. (2016). Prevalence of U.S. Pregnant Women Meeting 2015 ACOG Physical Activity Guidelines. American Journal of Preventive Medicine, 51(3), e87–e89. Visit Source.
Howard, R., Thumma, J., Ehlers, A., Englesbe, M., Dimick, J., & Telem, D. (2022). Reoperation for recurrence up to 10 years after hernia repair. JAMA, 327(9), 872–874. Visit Source.
Howell E. R. (2012). Pregnancy-related symphysis pubis dysfunction management and postpartum rehabilitation: two case reports. The Journal of the Canadian Chiropractic Association, 56(2), 102–111. Visit Source.
Jee, S. B., & Sawal, A. (2024). Physiological changes in pregnant women due to hormonal changes. Cureus, 16(3), e55544. Visit Source.
Jin, X., Wu, S., Huang, J., Tong, X., Li, H., & Chu, L. (2022). Effect of prolonged second stage of labor on pelvic floor function: A prospective cohort study. International Urogynecology Journal, 33(6), 1633–1638. Visit Source.
Karrar, S. A., Martingano, D. J., & Hong, P. L. (2024). Preeclampsia. In StatPearls. StatPearls Publishing. Visit Source.
Kinter, K. J., & Newton, B. W. (2023). Anatomy, abdomen and pelvis, Pudendal Nerve. In StatPearls. StatPearls Publishing. Visit Source.
Kraimi, N., Ross, T., Pujo, J., & De Palma, G. (2024). The gut microbiome in disorders of gut-brain interaction. Gut Microbes, 16(1), 2360233. Visit Source.
LaCross, J. A., Borello-France, D., Marchetti, G. F., Turner, R., & George, S. (2022). Physical therapy management of functional constipation in adults: A 2021 evidence-based clinical practice guideline from the American Physical Therapy Association's Academy of Pelvic Health Physical Therapy. Journal of Women’s Health Physical Therapy, 46(3), E59-E89. Visit Source.
Leslie, S. W., Antolak, S., Feloney, M. P., & Soon-Sutton, T. L. (2024). Pudendal neuralgia. In StatPearls. StatPearls Publishing. Visit Source.
Lim, Y., Leslie, S. W., & O'Rourke, S. (2024). Interstitial cystitis/bladder pain syndrome. In StatPearls. StatPearls Publishing. Visit Source.
Lirette, L. S., Chaiban, G., Tolba, R., & Eissa, H. (2014). Coccydynia: an overview of the anatomy, etiology, and treatment of coccyx pain. Ochsner Journal, 14(1), 84–87. Visit Source.
Liu, S. -P., Ko, P. -W., & Ho, C. -H. (2023). Prevalence and risk factors of postmicturition dribble in men. Urological Science, 34(4), 199-203. Visit Source.
LoMauro, A., & Aliverti, A. (2015). Respiratory physiology of pregnancy: Physiology masterclass. Breathe (Sheffield, England), 11(4), 297–301. Visit Source.
Meretighan, E. (2023). Pelvic Health Physical Therapy: The Future is Bright and Diverse - APTA Pelvic Health. Visit Source.
Muñiz, K. S., Voegtline, K., Olson, S., & Handa, V. (2021). The role of the genital hiatus and prolapse symptom bother. International Urogynecology Journal, 32(4), 829–834. Visit Source.
Nemeth, Z., & Ott, J. (2011). Complete recovery of severe postpartum genital prolapse after conservative treatment--a case report. International Urogynecology Journal, 22(11), 1467–1469. Visit Source.
Ng, M., Leslie, S. W., & Baradhi, K. M. (2024). Benign prostatic hyperplasia. In StatPearls. StatPearls Publishing. Visit Source.
National Institute for Health and Care Excellence (NICE). (2024). Endometriosis: Diagnosis and management. National Institute for Health and Care Excellence. Visit Source.
Panman, C., Wiegersma, M., Kollen, B. J., Berger, M. Y., Lisman-Van Leeuwen, Y., Vermeulen, K. M., & Dekker, J. H. (2017). Two-year effects and cost-effectiveness of pelvic floor muscle training in mild pelvic organ prolapse: A randomised controlled trial in primary care. BJOG: An International Journal of Obstetrics and Gynaecology, 124(3), 511–520. Visit Source.
Patel, U. J., Godecker, A. L., Giles, D. L., & Brown, H. W. (2022). Updated prevalence of urinary incontinence in women: 2015-2018 National Population-Based Survey Data. Female Pelvic Medicine & Reconstructive Surgery, 28(4), 181–187. Visit Source.
Peikert, K., Platzek, I., Bessède, T., & May, C. A. (2015). The male bulbospongiosus muscle and its relation to the external anal sphincter. The Journal of Urology, 193(4), 1433–1440. Visit Source.
Pizzol, D., Demurtas, J., Celotto, S., Maggi, S., Smith, L., Angiolelli, G., Trott, M., Yang, L., & Veronese, N. (2021). Urinary incontinence and quality of life: A systematic review and meta-analysis. Aging Clinical and Experimental Research, 33(1), 25–35. Visit Source.
Poskus, T., Buzinskienė, D., Drasutiene, G., Samalavicius, N. E., Barkus, A., Barisauskiene, A., Tutkuviene, J., Sakalauskaite, I., Drasutis, J., Jasulaitis, A., & Jakaitiene, A. (2014). Haemorrhoids and anal fissures during pregnancy and after childbirth: A prospective cohort study. BJOG: An International Journal of Obstetrics and Gynaecology, 121(13), 1666–1671. Visit Source.
Prendergast S. A. (2017). Pelvic floor physical therapy for vulvodynia: A clinician's guide. Obstetrics and Gynecology Clinics of North America, 44(3), 509–522. Visit Source.
Puri, S. N., Fating, T., & Dhage, P. P. (2023). The impact of functional stability exercises on alleviating pelvic girdle pain in pregnancy: A review. Cureus, 15(11), e48769. Visit Source.
Qu, E., Wu, J., Zhang, M., Wu, L., Zhang, T., Xu, J., & Zhang, X. (2021). The ultrasound diagnostic criteria for diastasis recti and its correlation with pelvic floor dysfunction in early postpartum women. Quantitative Imaging in Medicine and Surgery, 11(2), 706–713. Visit Source.
Quintero Rodriguez, C., & Troynikov, O. (2019). The effect of maternity support garments on alleviation of pains and discomforts during pregnancy: A systematic review. Journal of Pregnancy, 2019, 2163790. Visit Source.
Raizada, V., & Mittal, R. K. (2008). Pelvic floor anatomy and applied physiology. Gastroenterology Clinics of North America, 37(3), 493–vii. Visit Source.
Rao, S. S., & Patcharatrakul, T. (2016). Diagnosis and treatment of dyssynergic defecation. Journal of Neurogastroenterology and Motility, 22(3), 423–435. Visit Source.
Raveendran, A. V., & Rajini, P. (2024). Vaginismus: Diagnostic challenges and proposed diagnostic criteria. Balkan Medical Journal, 41(1), 80–82. Visit Source.
Redondo-Delgado, P., Blanco-Giménez, P., López-Ortiz, S., García-Chico, C., Vicente-Mampel, J., & Maroto-Izquierdo, S. (2025). Effects of strength training on quality of life in pregnant women: A systematic review. Acta Obstetricia et Gynecologica Scandinavica, 104(7), 1231–1243. Visit Source.
Renshaw, S., Peterson, R., Lewis, R., Olson, M., Henderson, W., Kreuz, B., Poulose, B., & Higgins, R. M. (2022). Acceptability and barriers to adopting physical therapy and rehabilitation as standard of care in hernia disease: A prospective national survey of providers and preliminary data. Hernia: The Journal of Hernias and Abdominal Wall Surgery, 26(3), 865–871. Visit Source.
Sakakibara, R., Tsunoyama, K., Hosoi, H., Takahashi, O., Sugiyama, M., Kishi, M., Ogawa, E., Terada, H., Uchiyama, T., & Yamanishi, T. (2010). Influence of body position on defecation in humans. Lower Urinary Tract Symptoms, 2(1), 16–21. Visit Source.
Saliba-Júnior, O. A., Rollo, H. A., Saliba, O., & Sobreira, M. L. (2022). Positive perception and efficacy of compression stockings for prevention of lower limb edema in pregnant women. Jornal Vascular Brasileiro, 21, e20210101. Visit Source.
Sam, P., Jiang, J., Leslie, S. W., & LaGrange, C. A. (2025). Anatomy, abdomen and pelvis, sphincter urethrae. In StatPearls. StatPearls Publishing. Visit Source.
Sampselle, C. M., & DeLancey, J. O. (1992). The urine stream interruption test and pelvic muscle function. Nursing Research, 41(2), 73–77. Visit Source.
Snyder, A. (2024). Pelvic Floor PSA. National Institute of Health Record. Visit Source.
Soma-Pillay, P., Nelson-Piercy, C., Tolppanen, H., & Mebazaa, A. (2016). Physiological changes in pregnancy. Cardiovascular Journal of Africa, 27(2), 89–94. Visit Source.
Szczygielska, D., Knapik, A., Pop, T., Rottermund, J., & Saulicz, E. (2022). The effectiveness of pelvic floor muscle training in men after radical prostatectomy measured with the insert test. International Journal of Environmental Research and Public Health, 19(5), 2890. Visit Source.
Te West, N. I. D., Harris, K., Jeffrey, S., de Nie, I., Parkin, K., Roovers, J. P., & Moore, K. H. (2023). The effect of 12 weeks of estriol cream on stress urinary incontinence post-menopause: A prospective multinational observational study. Neurourology and Urodynamics, 42(4), 799–806. Visit Source.
Thabet, A. A., & Alshehri, M. A. (2019). Efficacy of deep core stability exercise program in postpartum women with diastasis recti abdominis: A randomised controlled trial. Journal of Musculoskeletal & Neuronal Interactions, 19(1), 62–68. Visit Source.
Weerasinghe, K., Rishard, M., Brabaharan, S., & Mohamed, A. (2022). Effectiveness of face-to-face physiotherapy training and education for women who are undergoing elective caesarean section: A randomized controlled trial. Archives of Physiotherapy, 12(1), 4. Visit Source.
Wójcik, M., Szczepaniak, R., & Placek, K. (2022). Physiotherapy management in endometriosis. International Journal of Environmental Research and Public Health, 19(23), 16148. Visit Source.
Yaacov, D., Nelinger, G., & Kalichman, L. (2022). The effect of pelvic floor rehabilitation on males with sexual dysfunction: A narrative review. Sexual Medicine Reviews, 10(1), 162–167. Visit Source.
Yang, D. Y., & Lee, W. K. (2019). A current perspective on post-micturition dribble in males. Investigative and Clinical Urology, 60(3), 142–147. Visit Source.
Youssef, A., Brunelli, E., Pilu, G., & Dietz, H. P. (2021). The maternal pelvic floor and labor outcome. American Journal of Obstetrics & Gynecology MFM, 3(6S), 100452. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.