Congestive heart failure (CHF), also simply called heart failure, is a life-threatening condition in which the heart can no longer pump enough blood to meet the metabolic needs of the body. The very name echoes with the sound of doom. To the person being informed that they have it, the term CHF possesses an emotional impact equal to being diagnosed with cancer. CHF is the number 1 killer of our time with 6.5 million Americans living with it and 960,000 new cases diagnosed each year. Of those hearing these words applied to them for the first time, nearly half will die of complications related to this condition within the first 5 years after diagnosis, resulting in 1 out of every 9 deaths in the United States each and every year being in some fashion related to CHF.1,2,3
Despite such horrendous statistics, new studies show that the actual number of Americans receiving a new diagnosis of CHF is happily, very slightly on the decline! Over the past 10 years for which statistics from studies are available, the death rate from heart disease has fallen about 44 percent. As though to balance this, however, the continuing increase in the aging population has brought the total number of those who are struggling to live with CHF to new, record highs.4
At this time, there is no cure for CHF. Current treatment relies on early recognition and management of this life-threatening condition. Recognition of early signs and symptoms of this disease process allows interventions to be implemented as early as possible to manage the physiologic disease changes that occur. Disease management simply does not get any more complicated than with CHF. Recent studies show that gains are being achieved in the treatment of CHF and that with knowledge, determination and the compassionate provision of care, even CHF can be managed.
Congestive heart failure is, in a nutshell, the end stage for all chronic disease affecting the heart, and as such is a major cause of sickness and eventual death. CHF by simple definition is the inability of the heart to pump enough blood to meet the body’s needs. The term CHF does not mean that the heart as an organ has failed completely, but rather infers that the functioning of the heart is not sufficient or strong enough to meet the body’s needs at times of stress or increased activity. This inability to pump effectively is the reason for the descriptive word Congestive, as in congestive heart failure or CHF, one of the more descriptive used terms associated with this condition.
The reasoning behind associating the term congestive with the disease process of Heart Failure (HF) begins with the left ventricle of the heart that normally receives blood from the lungs before pushing this blood through arteries to the brain, internal organs, and extremities. When the left ventricle is weak, the affected person may experience symptoms of ‘dropsy’ or show that they possess a ‘weak heart.’ Both of these are older terms referring to the diminishment in cardiac output with its associated feelings of fatigue and dizziness, along with symptoms of fluid congestion such as painful edema, partially related to the lack of oxygenated blood flow to the kidneys which prevents the functional removal of excess fluid.5
Excess of fluid accumulates wherever it can, mainly in the feet, legs, abdomen and lungs. Often this accumulation of fluid is combined with shortness of breath on exertion, the inability to breathe while lying flat, and the tendency to awaken during sleep with shortness of breath. If the congestion of CHF becomes severe, excess fluid will accumulate in the lungs causing a life-threatening condition known as pulmonary edema which is accompanied by severe respiratory difficulties. As the disease progresses to the point where the right ventricle of the heart also fails, the patient will have an increase in the symptoms of low cardiac output and experience fluid build-up in the tissues of the body, resulting in leg swelling and fluid congestion of the internal organs.
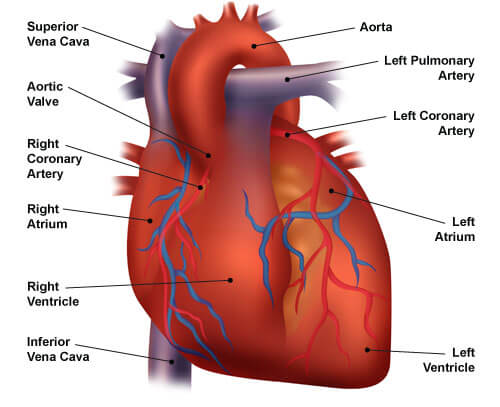
Diagram of the heart
Congestive heart failure is by no means a new disease. Descriptions of CHF exist in writings from ancient Egypt, Greece, and India. The Romans were known to use the plant foxglove (Digitalis, Digoxin, Lanoxin) as an elixir or tea to treat the condition. Widespread understanding of the nature and anatomy of CHF seems to have been scarce until William Harvey first published a detailed description of the circulation in 1628. Roentgen’s discovery of the principles of x-rays and the coinciding development by Einthoven of electrocardiography around the 1890s led to vast improvements in the ongoing investigation into CHF. The more modern advents of echocardiography, cardiac catheterization and nuclear medicine have much improved early diagnosis and investigation into the causes and treatment of CHF.
Strong suspicion exists among scholars that the historical practice of bloodletting and leeches were primarily intended to be a specific treatment for the symptoms resulting from the increased vascular load associated with CHF, that is before the popularization of the practice resulted in the use of bloodletting as the aspirin equivalent throughout medieval Europe.
It should be acknowledged that ancient medical practitioners did achieve varying degrees of success in the treatment of CHF for centuries. William Withering, for instance, published the documented benefits of digitalis (foxglove) on the dropsy of CHF in 1785. Many scholars believe that he merely set into the newly available format of the printing press the mainstay treatment that had been in use since the days of Rome. Still, another arguably successful old-time treatment from the 19th and early 20th centuries for CHF associated with fluid retention utilized those horrid yet effective replacements of the leech known as Southey's tubes, which were inserted into edematous peripheries, allowing a limited drainage of fluid.
Southey's tubes
Southey’s tubes are big bore needles with blunt - extended bevel tips for insertion directly into edematous tissue in order to allow the release of trapped edema. The visual impression they give to the eyes of modern health professionals is somewhat like an early Frankenstein relative of the modern vacutainer.
The practice of medicine in the 20th century brought with it new forms of medications that have proven to be revolutionary in the treatment of CHF. The first mercurial based generations of diuretics, though effective, were associated with substantial toxicity, a risk greatly diminished in their replacements, the thiazide diuretics that were introduced in the 1950s. The use of vasodilators in the treatment of CHF did not truly begin until the development of angiotensin-converting enzyme inhibitors in the 1970s. By using these new families of medications in combination with other agents possessing a more direct effect on the cardiac system, today’s treatments are more effective for the control of this, as of yet, incurable disease process.
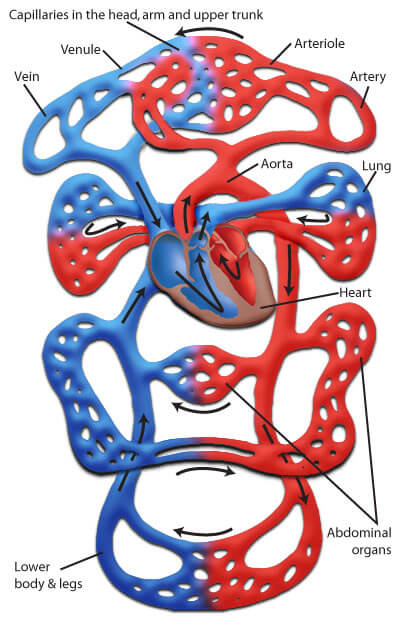
The normal function of the heart is to provide a gentle pulsatile pressure, which propels a stream of blood carrying oxygen and nutrients to the living cells of the body. This repetitive process ensures, with its bellows-like action that the flow of blood delivers oxygen and nutrients to the cells and carries away waste materials from the cells. Both at rest and during exercise, this pulsating pressure known as cardiac output (CO) continues, providing just enough force to keep blood moving in the pulse-by-pulse journey of cellular life. Cardiac output, distribution of oxygenated blood to the tissues, and venous return are all delicately balanced by neurohumoral and intrinsic cardiac factors.
The disease condition known as CHF is the failure of the heart to carry out its function. It has no simple cause. It also has no simple treatment. CHF is the end result of most, if not all, of the disease processes and conditions that affect the heart. CHF can involve the heart's left side, right side, or, as in most cases, both sides and is manifested by systolic or diastolic dysfunction or both. Combinations of systolic and diastolic abnormalities are common in CHF.
In systolic dysfunction (primarily a problem of ventricular contraction), the heart fails to provide enough blood flow to ensure the delivery of oxygen and nutrients to the tissues. This is a problem of inadequate cardiac output resulting in disparities of oxygen and nutrients, a wide variety of problems with energy utilization, energy supply, electrophysiological functions and cellular contractile element interaction. This last bit appears to reflect abnormalities in intracellular Calcium++ ion modulation and cyclic adenosine monophosphate (or cAMP) production.6
Video licensed from
Diastolic dysfunction in the left heart ventricle creates resistance to ventricular filling, referred to as heart failure with preserved ejection fraction (HFpEF), and is believed to account for more than half of heart failure cases diagnosed.7 Ventricular resistance is generally associated with a prolonged ventricular relaxation time as measured during isovolumic relaxation (the time between aortic valve closure and mitral valve opening when ventricular pressure falls rapidly). Resistance to filling (ventricular stiffness) relates directly to ventricular diastolic pressure. This filling resistance appears to increase with age, probably reflecting myocyte loss. Myocytes are the special muscle cells that make up heart muscle and contribute to increased interstitial collagen deposition. Diastolic dysfunction is presumed to be dominant in hypertrophic cardiomyopathy where the ventricles of the heart expand to replace damaged tissues, circumstances with marked ventricular hypertrophy (e.g., hypertension, advanced aortic stenosis), and amyloid infiltration of the myocardium.8
Terminology Turbocharge8, 9:
Heart failure with preserved ejection fraction (HFpEF), also called diastolic failure (or diastolic dysfunction) - The left ventricle is losing its ability to relax normally (muscle has become stiff). The heart is unable to fill properly with blood during the resting period between each contraction.
Heart failure with reduced ejection fraction (HFrEF), also called systolic failure - The left ventricle loses its ability to contract normally. The heart muscle is unable to pump with enough force to push enough blood into circulation during contraction.
NOTE: HFpEF and HFrEF have shown themselves to be distinct symptoms with at times subtle differences. While both are failures of the left heart ventricle (LV), cellular changes in the cardiomyocytes and extracellular heart matrix differ between types, suggesting differing future paths in the treatment of LV heart failure may be on the horizon.
Be aware that the terms HFpEF and diastolic heart dysfunction, though used interchangeably, are not actually the same things. Diastolic dysfunction simply means that mechanical problems are occurring in the left ventricle, where HFpEF refers to heart failure specific changes in LV function (stiffness). In short, the presence of HFpEF tends to go hand-in-hand with mechanical difficulties. However, it is possible to have mechanical shortcomings without heart failure symptoms. Ironically, and part of the terminology confusion, any LV mechanically impaired heart will inevitably drift toward heart failure – generally HFpEF.
High output failure is HF associated with a persistent high cardiac output that eventually results in ventricular dysfunction, literally wearing the heart muscle out. Conditions associated with high cardiac output include anemia, beriberi, thyrotoxicosis, pregnancy, advanced Paget's disease and arteriovenous fistula.10 CHF symptoms that develop in response to high-output states are often controllable and somewhat reversible with early, aggressive treatment of the underlying cause. Cardiac output is elevated in various forms of cirrhosis and the onset of congestion reflects cardiac and hepatic mechanisms of fluid retention.
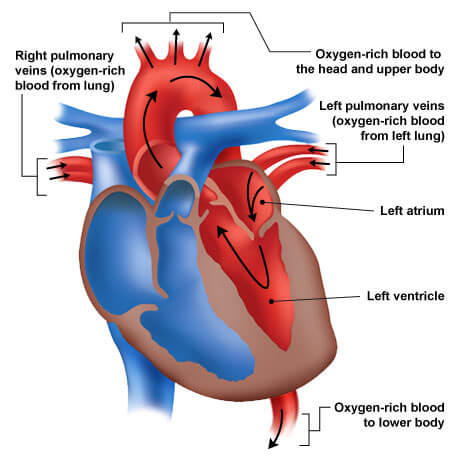
The left side of the heart is made up of two chambers starting with the left atrium (or upper chamber) and the larger left ventricle (or lower chamber). The left atrium receives oxygenated blood from the left and right superior and inferior pulmonary veins draining the left and right lungs respectively. The left atrium pumps the blood through the mitral valve into the left ventricle. The left ventricle during ventricular systole then pumps the blood through the aortic valve into the aorta which disperses it throughout the circulation.
If the left ventricle loses its ability to contract forcefully (called systolic failure), it cannot exert enough force to pump the volume of blood that is needed through the circulatory system. If the left ventricle loses its ability to relax (diastolic failure) because the left ventricular muscle has become stiff, it cannot properly fill with blood during the resting period between each beat. This is an important distinction because the treatments for each type of failure, left or right can be different.
Blood flow through the Left Heart chambers and vessels
In left ventricular failure, cardiac output decreases and pulmonary venous pressures increase. The elevation of pulmonary capillary pressures can rise to levels that exceed the functional pressure of the plasma proteins that form the barrier between vascular fluids and atmospheric gases, about 24 mm Hg. This leads to increased fluid in the lungs, reduced pulmonary compliance and a rise in the oxygen cost of the work of breathing. This high vascular pressure, known as pulmonary venous hypertension, along with the pulmonary edema resulting from left ventricular failure significantly alters the function of the lungs and those tricky ventilation perfusion relationships. Air hunger, therefore, correlates with elevated pulmonary venous pressure and the resultantly increased work of breathing, although the precise relationship is still being debated.
Due to the vascular layout of the pulmonary system, pleural effusions characteristically accumulate in the right hemithorax, though they later manifest bilaterally. In an effort to deal with this fluid crisis, lymphatic drainage is greatly enhanced, but cannot overcome the increase in fluid in the lungs. Unoxygenated pulmonary arterial blood ends up being shunted past nonaerated alveoli, decreasing mixed pulmonary capillary PO2. These changes often progress to the point where an arterial blood gas analysis reveals an increased pH and a reduced PaO2 (pulmonary oxygen concentration), that is to say, a respiratory alkalosis. A PaCO2 (pulmonary carbon dioxide concentration) above normal signifies alveolar hypoventilation, possibly due to respiratory muscle failure and typically requires urgent ventilatory support.
Mimi is a 42-year-old female who started walking 30 minutes a day to decrease her weight and to build up her physical tolerance. She is 5’4’’ and weighs 185 pounds. She has been exercising routinely for only a week. She is a non-smoker. Drinks at least 10 cups of coffee a day, mostly at work. A year ago she had developed hypertension and is a borderline diabetic. She can tell when her blood sugar gets low because she gets an odd taste in her mouth. She carries peanut butter crackers with her which seems to bring her blood sugar up.
Last week her shoes started to get tight, and she noticed her ankles swelling. Mimi attributed this to being on her feet all the time at her workplace. She loves her job and is a hardworking waitress, who works on limited sleep and at odd hours. She developed chest pain a few weeks ago and attributed it to moving boxes of food supplies. She suddenly felt weak, dizzy, and short of breath at work. Her manager called 911 when Mimi became pale, very short of breath (SOB) and started to pass out. He had to ease her to the floor.
When the ambulance arrived, Mimi had a blood pressure of 200/110; respirations were 28 with an oxygen saturation of 88%. She was extremely SOB. Her heart rate was 140, and she was in sinus tachycardia. Her temperature was 97.6 F. Her blood glucose was 90. She had no chest pain yet could feel heart palpitations, which scared her.
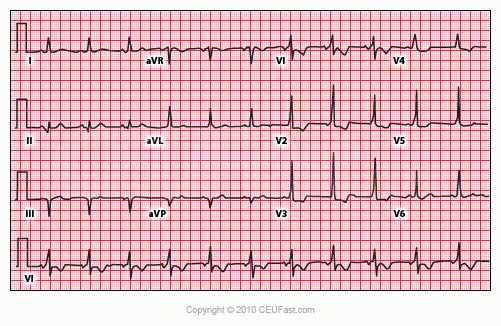
The ambulance paramedic placed her on a cardiac monitor, started her on oxygen 4 liters per minutes via a nasal cannula which increased her Oxygen saturation to 96%. A peripheral IV was started with normal saline. Her EKG revealed a normal sinus rhythm varying to a narrow complex sinus tachycardia ranging from 98 to 130. One non-coated ASA was given. A station-based cardiologist read the EKG and would be evaluating her once she arrived in the emergency room.
Individuals with left ventricular failure in general initially present to health care practitioners in one of three ways:
With a syndrome of decreased exercise tolerance
With a syndrome of fluid retention
With no symptoms whatsoever, the heart failure is incidentally discovered during checkup or examination for something completely different
Should either systolic or diastolic failures be present, blood coming into the left side of the heart from the lungs will congest or ‘back up,’ with the pressure difference from this increase in congestion causing fluid or ‘lung water’ as it is sometimes referred to, to exude into the lung fields. This is, of course, pulmonary hypertension. This form of hypertension is incredibly damaging to the pulmonary tissues and sets up the conditions that are needed for the dreaded condition of pulmonary edema, also at times referred to as ‘drowning in your own fluid.’ As the heart's ability to effectively pump decreases, peripheral blood flow slows down, typically causing fluid to build up in tissues throughout the body (generalized edema). It is because of this excess of fluid or congestion that the descriptive term congestive heart failure is a bit more widely used than the more correct term, heart failure.
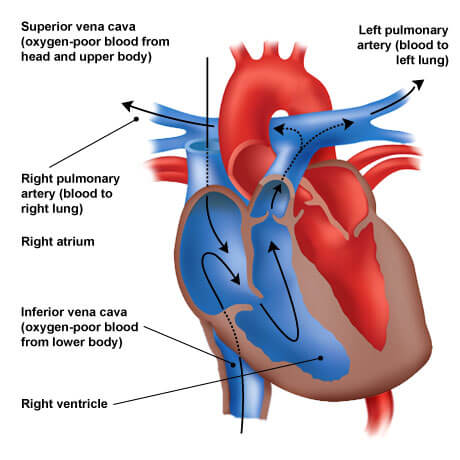
The right atrium is the receiving chamber for venous (unoxygenated) blood from the systemic circulation - from the arms, head, abdomen, and legs. It receives blood that returns to the heart through the superior vena cava (draining blood from the head and upper extremities), inferior vena cava (draining blood from the abdominal viscera and the lower extremities), the coronary sinus (draining blood from the circulation of the heart muscle itself) and the many tiny Thebesian veins (draining small amounts of blood directly from the atrial vessel walls). The blood is then propelled through the tricuspid valve during right atrial systole into the right ventricle where it then is ejected through the pulmonic valve into the left and right pulmonary arteries and into the lungs where the blood is replenished with oxygen.
Right-sided ventricular failure usually, but not always, is secondary to left-sided heart failure. The reason both the left and right ventricles tend to be affected in a domino fashion is that when the left ventricle fails, increased fluid pressure is, in effect, transferred backward through the lungs, ultimately damaging the heart's right side. When the right side loses pumping power, blood backs up in the body's veins. This usually causes unsightly and medically hazardous swelling in the legs and ankles.
Blood flow through the Right Heart (i.e. from the body into the lungs)
The most common cause of right ventricular heart failure is prior left-sided heart failure which increases pulmonary venous pressure. Increased pulmonary venous pressure leads to a state of generalized pulmonary arterial hypertension which results in a thickening of the muscular walls of the right atrium and ventricle.11 In a similar fashion, tricuspid regurgitation may also result in right ventricular failure. The force of blood being pushed backward past an incompetent tricuspid valve can set up conditions for pulmonary hypertension and right ventricular heart failure. This is just one example of why it is so important that a complete diagnostic workup is made routinely. Other causes of strictly right-sided failure can be mitral stenosis, primary pulmonary hypertension, multiple pulmonary emboli, pulmonary artery or valve stenosis, and right ventricular myocardial infarction.
Right-sided ventricular failure is closely associated with the development of systemic venous congestive symptoms. The sluggish venous congestion, in turn, leads to a moderate hepatic dysfunction that is common in CHF secondary to right-sided heart failure. The pressure affected liver manifests with what are usually modest increases in both conjugated and unconjugated bilirubin, prothrombin time, and in hepatic enzymes (e.g., alkaline phosphatase, AST, ALT). None of these abnormal laboratory values by themselves is particularly diagnostic for CHF. However, as circulation becomes increasingly compromised, these tells along with red flags such as markedly reduced splanchnic blood flow and hypotension begin to manifest. Gradually, when these are present, a state of central necrosis begins to form around the hepatic veins causing inflammation and acute symptoms that may be severe enough to suggest hepatitis with acute liver failure. If that is not enough to tweak a clinician’s attention, hepatic circulation slows down, directly contributing to a reduced aldosterone breakdown by the impaired liver.12 This is a very important indicator and will further contribute to overall fluid retention.
Do be aware that generalized volume overload and increased systemic venous pressure can occur in instances of polycythemia, over-perfusion of blood products, acute renal failure with overhydration, or in obstruction of either vena cava. If these conditions occur, they may readily “simulate CHF.” Myocardial function may be completely normal, merely masked by what is occurring throughout the rest of the vascular system.
It is important to remember that the presence of peripheral edema on its own is not a reliable sign of CHF. Another easily visible clue is the presence of an observable jugular venous distention and hepatojugular reflex, both of which are a very good visual indication that something is wrong with that individual’s heart pumping pressures. The hepatojugular reflex is an elevation of venous pressure visible in the jugular veins. It can be demonstrated when there is either active or impending right-sided heart failure by applying firm pressure with the flat hand over the person’s liver or upper abdomen.12
Notice the thickening of both ventricle walls in an effort to increase strength of heartbeat
Congestive heart failure is, largely, a chronic disease process. Lifestyle choices and the effects of other predisposing disease processes set up conditions that gradually worsen, with intervals of acute crisis. By the time a person is diagnosed with CHF, chances are very good that the heart has been losing pumping capacity little by little for quite some time.
At first, the heart tries to make up for the loss of effective pumping capacity by:
Enlarging: When a heart chamber enlarges, it is attempting to stretch further so that it can contract in a more forceful fashion and move more blood volume.
Developing more muscle mass: The increase in muscle mass occurs because the contracting cells of the heart actually do get bigger. This allows the heart to pump stronger, at least initially.
Pumping faster: This helps to increase the heart's overall cardiac output.
The heart is not in this alone. The rest of the body also tries to compensate for the loss of cardiac output.
Systemic blood vessels narrow or vasoconstrict in an attempt to elevate blood pressure thus attempting to structurally adjust and make up for the heart's centralized loss of power.
The body diverts blood away from less acutely critical tissues and organs in order to maintain flow to the most vital organs: the heart, lungs and brain.
The results of these temporary measures achieve little more than to mask the symptoms of CHF. They do not solve the problem. This is why many people are not aware of their condition until years after their heart becomes about as effective as a soggy sponge. Inevitably, the efforts to compensate made by the heart and body just cannot keep up with the demands placed on them, and the person experiences fatigue, breathing problems or other symptoms that prompt a trip doctor or emergency room.
Congestive heart failure results in hypoperfusion of oxygenated blood to the tissues and the inability to effectively carry away the flood pools of waste-filled, spent blood.
Perhaps the number one effect of CHF is the feeling of shortness of breath or difficulty breathing (i.e., dyspnea). This occurs as blood and fluid back up in the left and right pulmonary veins due to the failure of the left side of the heart. This backpressure causes fluid to leak into the lungs resulting in an unpleasant feeling of breathlessness during activity (most commonly), at rest, or while sleeping. This breathless feeling may come on suddenly and be intense enough to wake a person from sleep gasping for air. Those with CHF often have difficulty breathing while lying flat and may need to prop the upper body and head up on two or more pillows. They commonly complain of waking up tired or feeling anxious and restless, a complaint that should clue a healthcare provider that CHF may be lurking.
A companion symptom of lung congestion is the presence of persistent coughing or wheezing not related to another disease process such as the flu or a cold. This occurs as the fluid builds up in the lung tissues due to the congestion of the pulmonary vasculature. Generally, any long, ongoing bouts of coughing that consistently produce white or pink blood-tinged phlegm should be suggestive of CHF.
The buildup of excess fluid in body tissues, i.e., edema, is a sign of a definite circulatory problem and possibly CHF. This edema comes about as blood flow out of the heart slows, causing blood returning to the right side of the heart through the veins to back up. This back up is much more serious than a spoiled commute drive, however, as it is causing fluid to build up in the body tissues, areas not designed for excess fluid storage. The kidneys, for example, are less able to dispose of sodium and water when bogged down and the necessary brisk flow of blood is unavailable. This, in turn, causes additional fluid retention in the tissues, marked by swelling in the feet, ankles, legs or abdomen along with fluid weight gain. So, if your shoes are suddenly feeling a bit tight, there might be more going on than too much salt on last night's popcorn!
Forceful pump pressures falter leaving fluid further from the heart to puddle along
All this thinking about CHF making you tired? Maybe it is because your heart cannot pump enough blood to meet the needs of your body tissues. With CHF, unexplained fatigue is a major symptom of trouble ahead. The body starts diverting blood away from less vital organs, particularly muscles in the limbs, in order to send it to the heart and brain. When a person starts feeling tired all the time and has difficulty with everyday activities such as shopping, climbing stairs, carrying groceries, or walking, it is time to go visit the local healthcare professional. A body should not need to be performing daily activities dependent on emergency systems. The resulting wear and tear trashes vital organs in a most unappealing manner.
Directly related to this robbing of the blood supply are the symptoms of lack of appetite and/or nausea. When blood flow is being diverted to the brain and lungs, the digestive system receives less oxygen rich blood and problems with digestion compound. One such feeling that occurs is that of being both full and simultaneously nauseous.
Cyanosis, or observable discoloration in the extremities due to the lack of oxygenated blood flow, may occur with any form of CHF. The cause of CHF can be considered central and may reflect hypoxemia. A quick way to tell if the cause is central or peripheral is when improved color of the nail bed can be regained with vigorous massage. This is strongly suggestive of peripheral cyanosis. A cyanosis of central origin, in contrast, cannot be altered by increasing the local blood flow with massage, warming, or by any other peripheral means.12
The brain is the organ that is receiving the most attention during CHF. Confusion and impaired thinking are common companions of CHF. Changing levels of certain substances in the blood, such as sodium, can contribute to confusion, memory loss, and feelings of disorientation. Remember those poor bogged down kidneys? All organ systems interlock. No injury to one occurs without a cascade of effects influencing all the rest. An interesting side note to the confusion and sluggish thought processes that result with CHF is that family or friends are the ones that often seek help for the patient. Perhaps the very progressive nature of the disease condition itself makes it harder for an individual to know that they are in need of medical assistance.
Of the actual physical changes occurring to the heart in its attempt to compensate for decreased pumping ability, the only one likely to get noticed by the individual is an increased heart rate. This increase in rate is directly connected to an attempt to make up for the loss of pumping capacity. In order to increase capacity, the heart beats faster. This may be reflected in cardiac palpitations, which feel like the heart is racing or throbbing.
Diagram of dynamic circulatory flow patterns
Acute pulmonary edema is a life-threatening manifestation of left-sided heart failure, most often secondary to the sudden onset of pulmonary venous hypertension. A sudden rise in left ventricular filling pressure results in rapid movement of plasma fluid through the pulmonary capillaries and into the interstitial spaces and alveoli. This symptom of CHF is, in reality, a medical disaster in its own right and presents with extreme dyspnea, deep cyanosis, tachypnea, hyperpnea, restlessness and anxiety, accompanied by a sense of suffocation. Pallor and diaphoresis in this medical emergency are common. The pulse may be thready and a blood pressure difficult to obtain. Respirations are labored, and rales are widely dispersed over both lung fields anteriorly and posteriorly. Some individuals manifest with marked bronchospasm or wheezing (cardiac asthma). Noisy respiratory efforts often render cardiac auscultation difficult, but a summation gallop, merger of S3 and S4 sounds may often be heard. Hypoxemia is severe. CO2 retention in this emergency state is a late, ominous manifestation of secondary hypoventilation and requires immediate attention.12
Congestive heart failure can be tricky. Even though more Americans die from diseases of the heart and circulatory system than from any other cause, it is often a complete surprise when a person receives a CHF diagnosis. Often this is due to the progressive nature of the condition, and the nature in which the body attempts to compensate. Those who have advanced heart disease, i.e., heart failure, tend to have episodes of serious symptoms, then long periods in which nothing seems to happen. These compensatory periods are filled with happenings - it is just that they are difficult to feel or discern. One vital way of tracking change is careful monitoring of physical activity limitations. Even though the individual may feel back to snuff, in reality the continuing insufficient vascular perfusion works to diminish strength and physiologic responsiveness, one functional piece at a time. For this reason, the degree to which a person’s physical activity is limited provides a valuable means of determining the effect that the condition is having on that individual.
A well-accepted classification scale known as the New York Heart Association Functional Classification has been formatted and is in use to standardize categories of Functional Heart Class.13
Class 1: No limits -- ordinary physical activity fails to cause undue tiredness or shortness of breath. Current or no treatment is holding symptoms at bay.
Class 2: Slight or mild limits -- comfortable at rest, but ordinary physical activity results in tiredness or shortness of breath. Treatment is effective; if no treatment is in place, it should be considered at this point.
Class 3: Marked or noticeable limits -- comfortable at rest, but less than ordinary physical activity causes tiredness or shortness of breath despite active treatment. Treatment is of marginal or diminished effect.
Class 4: Severe limits -- inability to carry on any physical activity without discomfort. If any physical activity is undertaken, discomfort increases. Symptoms are present at rest. Treatment is unable to control symptoms.
November 8, 2001, the American College of Cardiology in collaboration with the American Heart Association released a new class system for heart failure patients. This new system is designed for use along with functional class systems such as the New York system described above. The new system classifies heart failure in stages A through D. Only stage C and D patients actually have the physical changes that are manifested by CHF. Do be cautious when using the new system until it gets familiar as it measures progression more in the manner of cancer classes. That is to say, even though treatment may make cancer disappear, the patient is still classified as a cancer patient. In the new heart failure system, patients who develop into stage C always remain in stage C even if they get better and their symptoms disappear. Their functional class might improve to class one, but they would remain in stage C anyway. Confused? Do not be. Once you become familiar with the change, the benefits of this style of classification system become obvious. For any in-depth questions, the entire guidelines are available from the American Heart Association or at their website.14
Stage A – This person is at high risk for developing heart failure (HF) because of the presence of conditions that are strongly associated with HF, but as of yet has no structural disorder of the heart. Examples: patients at high risk for developing HF because of high blood pressure, coronary artery disease, diabetes, a history of drug or alcohol abuse, history of rheumatic fever, family history of cardiomyopathy, etc.
Stage B – This person has a structural disorder of the heart but has never developed HF signs or symptoms. Examples: patients with structural heart disease such as left ventricular heart enlargement, heart fibrosis, valve disease, previous heart attack, asymptomatic valvular heart disease, previous myocardial infarction.
Stage C – This person has past or current HF symptoms and underlying structural heart disease (i.e., dyspnea or fatigue due to left ventricular systolic dysfunction). This includes those patients who are in current symptom remission who are undergoing treatment for prior symptoms of HF.
Stage D – This is a person who has advanced structural heart disease and marked symptoms of HF even at rest despite maximal medical therapy. These individuals exhibit an end-stage disease process and are frequently hospitalized for HF symptoms. This group also includes those who require special treatments such as a Left Ventricular Assistive Device (LVAD), an artificial heart, intravenous medications such as inotropic infusions, a heart transplant, or hospice care.
Case Study
Agnes Miller is a 47-year-old female with a mixed heritage of Pacific Islander and West African black. She is a working person, who has been complaining to her husband about not feeling well for several months. She had gone to an urgent care center two weeks previously with a persistent cough that just would not go away, and shortness of breath on exertion. At this time, she had been started on a general antibiotic. She now follows up with her family practitioner, who she has not visited in the last two years, her husband accompanies her. Her stated purpose is to get another cycle of antibiotics as she still has the cough and shortness of breath.
On questioning, it is revealed that she continues to smoke, 3 packs a day. Early last year she experienced a prolonged bout of the flu, characterized by severe abdominal gas pains that kept her in bed for over a week. Since that time, she has been feeling fatigued and having intermittent episodes of difficulty concentrating at work where she is a high-level actuary for an international insurance provider. Her job consists of desk and paperwork, with little physical activity, and includes many missed meals and late work nights.
Physical exam reveals faint right lower lung field crackles, a blood pressure of 190/120, pulse of 110, respiration of 22, and tympanic temperature of 99.7. She is hesitant about lying flat on her back, complaining of "snoring troubles" at home when she rests in this position. By palpation, it is evident that her liver is somewhat enlarged and a positive hepatojugular response is present.
Due to the findings of the physical exam and Mrs. Miller’s report, the initial impression is that of Class C, Functional Level 3 - Heart Failure, and not an infectious process, though that will be ruled out by laboratory testing.
The initial plan is to inform Mrs. and Mr. Miller that there may be more going on than another course of antibiotic will resolve, and gain their cooperation in further diagnostic testing, starting with a CXR, laboratory testing, then proceeding on as warranted.
Discussion – Mrs. Miller’s reported symptoms fall directly in line with developing and possibly advanced Heart Failure, of the Congestive type. In women, Myocardial Infarctions are often manifested as dyspnea with or without abdominal pain and discomfort, instead of left arm pain as is more typical in men. Her heritage and lifestyle as she reports it also falls in line with an increased risk for cardiac disease. Right-sided heart failure, where the pulmonary vascular pressures are high, often manifests with night coughs and crackles in the lung fields due to the presence of fluid in the lungs forced out of the vascular beds by pressure. The increase in overall blood pressure, as well as pulse, may be a compensatory mechanism by which the body is trying to deal with the heart failure forced on it by ischemic heart changes post myocardial infarction. The heightened respiratory rate may also be a compensation for vascular changes as well as overall lack of blood oxygenation.
Prognosis, grim.
Should diagnostic testing confirm the suspicion of advanced Heart Failure, immediate targeted treatment will need to be initiated. Due to the potentially advanced state of the condition, as it manifests, the Millers will be faced with hard choices as far as lifestyle changes and therapeutic options.
Prevention is the best means of dealing with heart failure, congestive or not. As the condition is the end result of stresses and damage to the vascular system, and not caused by an exclusive disease process, it becomes difficult to form preventive measures that would be specific to CHF. As the heart ages, for instance, some of the blood-pumping ability of the heart muscle naturally decreases. The serious loss of vascular ability called CHF is the result of stress to our heart from a wide variety of health conditions that either damage the heart muscle itself, or create conditions that lead to the work that the heart is doing being so difficult that the heart damages itself. All of the behaviors associated with heart disease such as smoking, being overweight, eating foods high in fat and cholesterol, and lack of exercise contribute to CHF. In some individuals, however, lifestyle has been shown to have absolutely nothing to do with the formation of CHF. For instance, some people who go on to develop CHF are born with structural heart defects, while in others a virus or other infectious process has damaged the heart muscle. Any measure of prevention, therefore, must be aimed at maintaining an overall healthy lifestyle, though it does seem prudent to institute preventive measures aimed at known disease processes that cause damage to the heart and vascular system.
Preventive Recommendations for High Risk Clients12(Stage A)
Control of systolic and diastolic hypertension
Treatment of lipid disorders
Avoidance of high risk behaviors (e.g. smoking, alcohol, illicit drugs)
Control of ventricular rate in those with known supraventricular tachyarrhythmias
Treatment of thyroid disorders
Routine evaluation (at least yearly)
Regular exercise
Prudent reduction of dietary salt
Routine use of nutritional supplements known to be beneficial to general health and also those that aid in prevention of development of structural heart disease
Addition of ACE inhibitory medications if there is a history of prior myocardial infarction
Valve replacement or repair for known hemodynamically significant disease that is present
(Uddin, 2007) (Merck Manual, 2005).
The following is a discussion of some of the conditions most commonly associated with being causes of CHF, along with where available, their population attributable risk.11,12
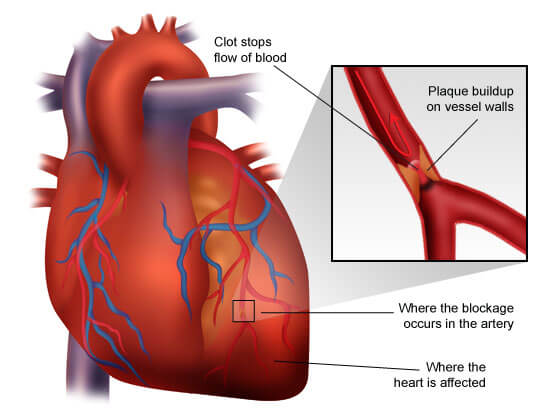
Ischemic Heart Disease robs the heart muscle of the vitality it needs to function, it attempts to compensate by making structural changes
The most commonly reported cause of CHF is ischemic heart disease. Ischemia is reduced blood flow, usually caused by blocked arteries that supply blood for the use of the heart muscle itself. It accounts for about 62% of CHF cases in the US in men and 56% in women.
Hypertension is often considered the third most common cause of CHF, occurring as a cause in approximately 10% of cases, although it is a slippery one to pin down as it often accompanies other causes in a sick sort of supporting role. It is known that uncontrolled high blood pressure increases a person's risk of developing CHF by two to three times. When pressure in the blood vessels is too high, the heart has to pump harder than normal to keep the blood circulating. This takes a toll on the heart, and over time, the chambers get larger and weaker.
The attributable risk from tobacco use, according to the First National Health and Nutrition Examination Study (NHANES), increases the chance of experiencing heart failure by 17%.
Increased body mass has shown a definite population significant risk factor, averaging around an 8% increase in heart failure rates. Some researchers such those from the Framingham Heart Study feel obesity is a more significant risk, estimating an 11% risk factor in men and a 14% rise in risk due to obesity alone.
Diabetes is the next most common predisposing factor to CHF. Extra strain is placed on the heart, and diabetes has been identified as the causative factor in about 3% of CHF cases. People with diabetes also tend to be overweight and have high blood pressure and high cholesterol, all of which makes the heart work harder.
Twitchy heart valves is an increasing risk factor, currently coming in at around a 2% predisposing rate for heart failure, yet with extension in life spans becoming ever more frequent as is seen by the uptick in calcific aortic stenosis requiring surgical intervention.
Though ironically somewhat difficult to categorize as a predisposing entity, myocardial infarction is a frequent cause of CHF. A heart attack occurs when an artery that supplies blood to the heart fails (which blurs with ischemic heart disease). The loss of oxygen and nutrients damages the heart's muscle tissue. Part of it essentially dies. The remaining healthy tissue has to pump even harder to keep up. This cause again overlaps, as a history of myocardial infarctions plays an integral role in the formation of ischemic heart disease, hypertension and coronary artery disease.
Ischemia, necrosis and heart failure, oh my! Heart attacks do damage that is significant even when they are survived
When cholesterol and fatty deposits build up in the heart's arteries, less blood reaches the heart muscle. This damages the muscle, and the healthy heart tissue that remains is forced to work harder.
Cardiomyopathy or inflammation of the heart (myocarditis), are terms used to label heart muscle disease states. Any damage to the heart muscle whether due to drug or alcohol use, viral infections or unknown reasons increases the risk of CHF. Cocaine, as well as, methamphetamine use produces an accumulative toll of heart damage. Alcohol is by far the most common culprit.
Heart defects present at birth are still another initiating stress that creates the conditions necessary for CHF to occur. If the heart and its chambers fail to develop correctly, the healthy parts have to work harder to make up for it. This hyperplasia of the heart muscle progresses on into remodeling and CHF with every subsequent beat.
When the lungs do not work properly, the heart has to work harder to get available oxygen to the rest of the body. This results in heart muscles stretching, growing to compensate, which in turn leads to neurohormonal release from cardiac muscle cells, and the process of heart chamber remodeling begins its inevitable cascade out of control.
Low red blood cell counts such as occur in disease states such as anemia force the body to hustle around the available blood cells. When there are not enough red blood cells to carry oxygen, the heart tries to move the small number of cells at a faster heart rate. It can become overtaxed from extended effort. An interesting side-note is that sickle cell anemia is occasionally linked to CHF as well.
An overactive thyroid gland (hyperthyroidism) is the jet fuel of CHF. This condition causes the body to work at a faster pace, and the heart can be overworked trying to keep up.
Kidney damage or disease not related to diabetes initiates the process that results in CHF. The overall stress placed on the heart and vascular system by lack of kidney function is tremendous. The results of this wearing damage manifest in many disease conditions and processes, CHF being just one of many.
This is a very uncommon disease of unknown cause involving the medium and small pulmonary arteries. It results in right ventricular failure or fatal syncope generally within 2 to 5 years after detection. Women are affected twice as often as men, with the median age at diagnosis around 35 years old. Younger individuals who have been diagnosed with this condition have a worse overall prognosis. Thickening of the blood vessel wall known as Intimal Hyperplasia, and the consequent narrowing of the vessel lumen, is present in this disease. Areas of medial hypertrophy and hyperplasia, irreversible plexiform lesions, and necrotizing arteritis (plexogenic arteriopathy) occur in more advanced cases. Similar vascular lesions and clinical course have been observed in some patients with cirrhosis and in a few patients taking the once popular appetite suppressant drug combination dexfenfluramine-phentermine (fen-phen), which is no longer marketed in the United States.
Abnormal heart rhythms (arrhythmia or dysrhythmia) contribute increased levels of stress and strain on the tissues of the heart. When the heart beats too quickly, too slowly, or in an irregular fashion, it may not be able to pump enough blood to meet all the body's needs. While dysrhythmias may contribute to or even cause CHF, their presence can be a result of having existing CHF.
Those conditions that affect the tough membranous sac that surrounds the heart (the pericardium) are known as pericardial diseases. Disease processes that produce fluid accumulation (effusion), infection/inflammation (pericarditis), or abnormal thickening (constriction) are the more common ones. As expected, given the nature of the disease process present with pericardial conditions, they add greatly to the labor and stress of the heart, often long after the acute disease process is resolved.
Congestive heart failure has plagued humankind for as long as recorded history. Only in recent years have we been able to recognize it as a condition brought about by disease, trauma, and even congenital abnormalities, anything that causes the heart itself to function in an abnormal and stressful manner for extended lengths of time. Now we can anticipate its development by recognizing the conditions that cause it to occur. We even have the screening tools to measure it, such as the New York Functional Assessment and the American Heart Association/American College of Cardiology Heart Failure Staging Tool, so we can better focus on early treatment and aggressive control with medications, invasive procedures, and especially with lifestyle changes. These areas will be discussed in detail in sections two and three of this special three-part series, Congestive Heart Failure.
Implicit Bias Statement
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Heart Disease and Stroke. Heart Disease and Stroke | Healthy People 2020. (Visit Source). Published November 8, 2017. Accessed November 11, 2017.
Benjamin EJ, et al. Heart Disease and Stroke Statistics-2017 Update: A Report from the American Heart Association. Circulation. (Visit Source). Published March 7, 2017. Accessed November 11, 2017.
Division for Heart Disease and Stroke Prevention. Centers for Disease Control and Prevention. (Visit Source). Published June 16, 2016. Accessed November 11, 2017.
Husten L. Sudden Death Declining in Heart Failure. CardioBrief. (Visit Source). Published July 5, 2017. Accessed November 11, 2017.
Villines Z. Congestive heart failure: Stages, symptoms, and causes. Medical News Today. (Visit Source). Published October 18, 2017. Accessed November 11, 2017.
Smith TW, Morgan JP. Excitation contraction coupling in myocardium. UpToDate. (Visit Source). Published October 11, 2017. Accessed November 12, 2017.
Tobushi T, Nakakano M. Improved Diastolic Function Is Associated with Higher Cardiac Output in Patients with Heart Failure Irrespective of Left Ventricular Ejection Fraction. Journal of the American Heart Association. (Visit Source). Published February 28, 2017. Accessed November 12, 2017.
Borlaug, BA. Pathophysiology of heart failure with preserved ejection fraction. UpToDate. (Visit Source). Published December 20, 2016. Accessed November 12, 2017.
Nguyen VQ. Dilated Cardiomyopathy. Practice Essentials, Background, Pathophysiology. (Visit Source). Published July 17, 2017. Accessed November 13, 2017.
Givertz MM, Haghighat A. High-output heart failure. High-output heart. UpToDate. (Visit Source). Published August 19, 2016. Accessed November 15, 2017.
Ramachandran VS, Wilson PW. Epidemiology and causes of heart failure. UpToDate. (Visit Source). Published November 30, 2016. Accessed November 15, 2017.
Shah SS. Heart Failure (HF) - Cardiovascular Disorders. Merck Manuals Professional Edition. (Visit Source). Published March 1, 2017. Accessed November 15, 2017.
Colucci WS, Dunlay SM. Clinical manifestations and diagnosis of advanced heart failure. UpToDate. (Visit Source). Published June 14, 2017. Accessed November 15, 2017.
Colucci WS. Determining the etiology and severity of heart failure or cardiomyopathy. UpToDate. (Visit Source). Published November 2, 2017. Accessed November 16, 2017.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.