This course will be updated or discontinued on or before Saturday, August 14, 2027
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will know the components of the atopic triad and how to identify these conditions.
Objectives
After completing this continuing education course, the participant will be able to:
Identify the risk factors for atopic conditions.
Explain the different pathophysiologies of the conditions within the atopic triad.
Outline the common environmental triggers for conditions within the atopic triad.
Differentiate between the clinical presentations of conditions within the atopic triad.
Determine the diagnostic tests used for identifying conditions within the atopic triad.
Identify the comorbid conditions for patients with atopy.
Describe the important patient education for patients with atopic conditions.
Interpret the potential complications of atopic conditions.
Determine the appropriate management strategies for conditions within the atopic triad.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Atopy is a genetic proclivity for an increased inflammatory response and subsequent development of allergic conditions with exposure to certain environmental and food triggers. Individual and hereditary factors make some people more susceptible to atopic conditions than others and often the manifestations of the allergic response will overlap across body systems, contributing to and worsening the manifestations of the inflammation.
There is a common cluster of conditions that are frequently seen together and are referred to as The Atopic Triad. These conditions include (Emfietzoglou, 2025):
Allergies (allergic rhinitis)
Asthma
Atopic Dermatitis (eczema)
Knowledge about these conditions separately and together is important for healthcare professionals in all specialties but may be of particular interest for nurses working in allergy, general pediatrics, or primary care. This course serves to provide foundational knowledge about the atopic triad’s prevalence, presentation, management, and nursing implications. You will learn how to assess risk, gather a history, identify signs and symptoms, and manage and educate about the complex interplay of this cluster of conditions.
As briefly mentioned above, the triad is composed of allergies, or more specifically allergic rhinitis, asthma, and atopic dermatitis. The reason that these three conditions are termed “the atopic triad” is because all three tend to occur together in an individual patient (Emfietzoglou, 2025). In other words, many patients suffer from all three. The typical progression of this triad cluster is that it begins as atopic dermatitis, more commonly known as eczema, and then develops into comorbid allergic rhinitis and finally asthma. This development is known as the “atopic march”. People with one or more of the conditions in the triad are at an increased risk of developing the other conditions and are typically highly sensitized to allergens and have an overactive inflammatory response (Emfietzoglou, 2025).
Each condition in the triad has its own causes, signs and symptoms, and treatments, but all share an overlapping chronic pathology of a highly sensitive inflammatory response (Emfietzoglou, 2025). Current data suggest that 31.8% of adults suffer from any one atopic condition and that anywhere from 2-6% of adults have all 3 coexisting conditions (Ng & Boersma, 2023; Pullerits et al., 2021).
Atopic dermatitis, or eczema, categorized by itchy and irritated patches of skin, is among the most common of atopic conditions and accounts for nearly 30% of all visits to a dermatology specialist annually (National Institute of Allergy and Infectious Diseases, 2024).
This condition affects 10%-30% of children and 2%-10% of adults nationwide (National Institute of Allergy and Infectious Diseases, 2024). The incidence is highest in children aged 0-5 years and begins to slowly taper off into adolescence and early adulthood. There is a slightly higher incidence among females compared to males. When considering race as a risk factor, Black individuals are the most likely to suffer from eczema (Shaw, 2023). Among adults with eczema, around 20% also have asthma (Mulick et al., 2022). This comorbidity rate is as high as 80% in children (Mulick et al., 2022). Having eczema is also the number one risk factor for developing food allergies (National Institute of Allergy and Infectious Diseases, 2024).
Allergic rhinitis is characterized by symptoms like frequent sneezing, nasal itching, and rhinorrhea. National Institute of Health (NIH) data from 2021 indicates that 25.7% of U.S. adults suffer from allergic rhinitis, with variation across race, sex, and age (Ng & Boersma, 2023).
White individuals are the most likely to experience allergic rhinitis, followed closely by Black individuals, with a 28.4% and 24.0% prevalence respectively (Ng & Boersma, 2023). Women are again more likely to experience this condition. And people in middle age (45-64 years) had the highest incidence at 27.9%, with incidence declining later in life (Ng & Boersma, 2023). Among children, up to 40% experience allergic rhinitis by age 6 (Licari et al., 2023). There is a significant link between allergic rhinitis and asthma, with up to 40% of patients with allergic rhinitis also having a diagnosis of asthma (Akhouri & House, 2023).
While less common in the atopic triad, food allergy is closely related and often goes hand in hand with seasonal allergies and eczema. Around 6.2% of adults have one or more food allergies, most commonly amongst women (7.8%), Black Americans (8.5%), and ages 45-64 (6.7%) (Ng & Boersma, 2023).
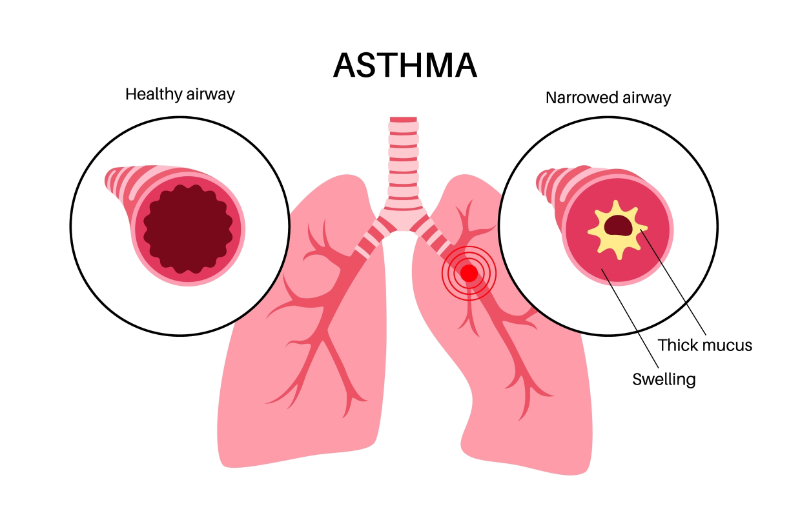
And finally, asthma, which is characterized by recurrent airway constriction and inflammation, affects 7.7% of the United States’ population (National Center for Environmental Health, n.d.).
Children under the age of 4 have the lowest incidence of asthma (around 2%) and this increases to about 9% in older children and adolescents. Up until about 19 years of age, asthma occurs more frequently in males than females, and then from 20 years onward this flips and is more common in females. Black individuals have a prevalence around 10% while white individuals are around 7% (National Center for Environmental Health, n.d.).
Across all three main conditions, family history is the greatest predictor of atopy of any kind, with 80% of people with an atopic condition having a family history of allergies (Justiz Vaillant et al., 2024).
Social determinants of health also serve as risk factors and need to be carefully considered. There are higher rates of atopy among people living in urban and impoverished areas where living conditions may be poorer, leading to increased exposure to triggers like dust, mold, and cockroaches (Polaskey & Chovatiya, 2025). Air quality is also more likely to be low with increased pollution in urban areas (Polaskey & Chovatiya, 2025).
Not only do certain social factors make people more likely to experience atopy, those same factors (and many others) also make it more difficult to receive care for the conditions, directly impacting the severity of disease (Polaskey & Chovatiya, 2025). For example, education level and socioeconomic status frequently impact a person’s insurance status and their ability to receive healthcare services. People who are under- or uninsured are less likely to be able to afford specialist visits and monthly medications to manage symptoms or flare-ups. Immigration status can also make it difficult to access care, both due to the increased likelihood to be under-/uninsured and also the increased difficulty in navigating the healthcare system when English is a second language (Polaskey & Chovatiya, 2025).
Transportation to appointments can also serve as a barrier, with people living in rural locations sometimes needing to travel several hours to see a specialist (Polaskey & Chovatiya, 2025). People of low socioeconomic status may also lack reliable transportation methods. People with disabilities, small children, or jobs with low flexibility may also encounter a whole host of difficulties making arrangements to get to appointments as needed (Polaskey & Chovatiya, 2025).
Chronic disease flare-ups can lead to lost hours at work and school, perpetuating lower education levels and socioeconomic status for these individuals. In a perpetual circle of risks, social disparities make individuals more likely to experience atopic conditions and also less likely to be able to manage those same conditions, furthering their risk and creating large gaps in health outcomes.
As with any chronic condition, these diseases require frequent utilization of healthcare services, including specialty appointments for maintenance, acute care for flare-ups or complications, and prescription medications for both chronic and acute use.
According to the Centers for Disease Control and Prevention (CDC), there are around 1.8 million emergency department visits, and 183,000 hospitalizations related to asthma each year (Centers for Disease Control and Prevention [CDC], 2023b). Only around 1% of emergency department visits are for allergic reactions, however, there are more than 4 million outpatient visits for allergy symptoms annually (CDC, 2023a). Eczema accounts for nearly 2 million primary care and dermatology office visits annually (Singh & Silverberg, 2023).
The financial impact is also significant, both on an individual and systemic level. Recent data estimates that annual healthcare costs for people with eczema can range from $8,000 (for mild disease) to nearly $24,000 (for more severe disease) (Wang et al., 2022). Cost of asthma care is around $4,000 annually for individuals, and the individual cost of allergy management is around $300 annually (Asthma and Allergy Foundation of America [AAFA], 2025; Roland et al., 2021). The Asthma and Allergy Foundation of America estimates that more than $82 billion is spent annually in the United States on management of these conditions (AAFA, 2025).
There is also the consideration of vulnerable groups with increased risks of financial hardship when managing chronic disease. Not only does this lead to poorly managed atopic disease, but financial hardship further contributes to poverty and risk of severe disease, creating a vicious cycle that is difficult to escape. On a societal level, this just perpetuates the health disparities among the poor and vulnerable. Special care should be taken to identify vulnerable populations and understand the impacts of social determinants of health on atopic disease (AAFA, 2025). On a broad level, efforts to identify those at risk and ensure appropriate management of these conditions can reduce burden on the healthcare industry as a whole.
In a general sense, atopy is an exaggerated immune response to harmless substances. There is a strong genetic component with atopy, which primes the body to respond with hypersensitivity when exposed to a variety of allergens or antigens (Justiz Vaillant et al., 2024).
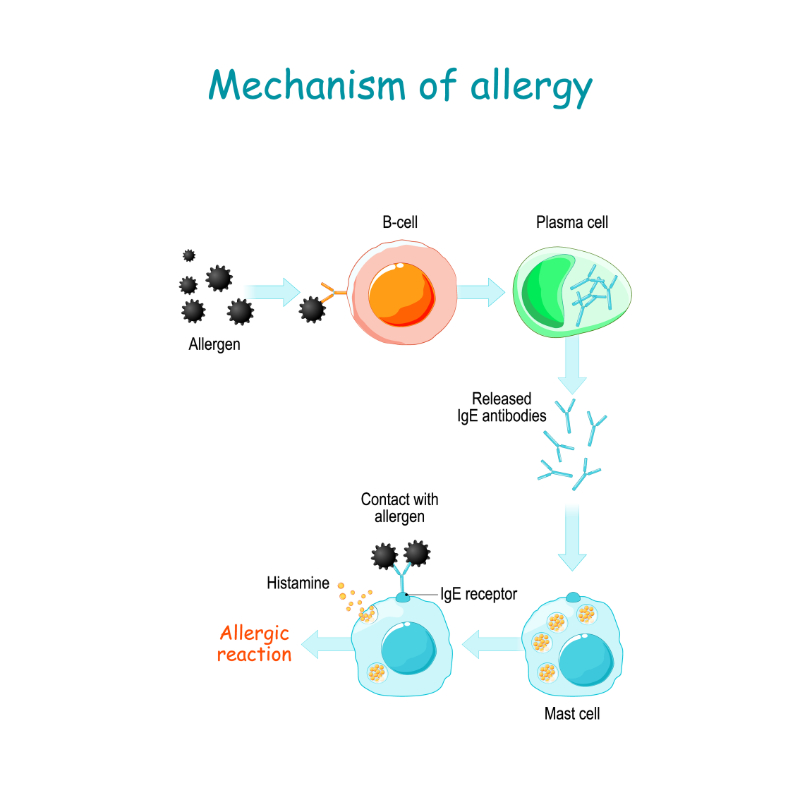
Image 1: Allergic Response
An initial exposure to an allergen triggers a response pathway that includes B cells, that further differentiate into plasma cells. Plasma cells produce an influx of IgE antibodies that are allergen-specific (Justiz Vaillant et al., 2024). The IgE antibodies bind to mast cells which are a widespread part of host defense and heavily present in the body’s mucosal surfaces (Justiz Vaillant et al., 2024). With subsequent exposure to a trigger, the mast cells are activated, causing a variety of mediators to be released, including histamine, leukotrienes, cytokines, prostaglandins, and tryptases, resulting in the signs and symptoms of an allergic reaction (Justiz Vaillant et al., 2024).
The specific way this response manifests is dependent on an individual’s unique genetic predisposition, the type of trigger, and the site of the allergen’s contact with the immune system. The skin, upper respiratory tract, and lungs are some of the most common sites for allergens to come in contact with, which leads to the conditions in the atopic triad.
These conditions all involve different body systems and present with unique signs and symptoms, but they all begin with a shared trigger of hyperresponsiveness and a complex interplay of genetics and environmental factors. Though the conditions can occur separately, the state of hyperresponsiveness at the root of the problem predisposes an individual to develop symptoms in other body systems, which is why the rate of comorbid atopic conditions is so high. The involvement of multiple body systems creates increased discomfort and symptoms for patients and complicates treatment. We will go into further detail of each individual disorder now.
Eczema, often the first condition to develop of the atopic triad, is a complex condition with many causative and contributing factors, most often a combination of genetic and environmental factors (Cleveland Clinic, 2022).
There is a substantial genetic component to eczema, with family history being a common risk factor (Cleveland Clinic, 2022). The genes most often involved lead to dysfunctional skin barrier and hyperresponsiveness of the immune system.
In addition to genetic factors, environmental factors that contribute to the condition can include (Cleveland Clinic, 2022):
Cold temperature
Low humidity climates
Calcium carbonate content in water (or “hard” water)
Fragrances in soaps
Fabric softeners
Cosmetics
Textured fabrics/clothing (such as wool, polyester, or other synthetic fabrics)
Sensitization to certain proteins in foods (such as eggs, nuts, or dairy)
Environmental allergens like dust mites
Air pollutants common in urbanized areas
There is also growing evidence to suggest that early life colonization and the makeup of a person’s normal skin and gut flora has an impact on the rates of atopic dermatitis (Nemeth et al., 2024).
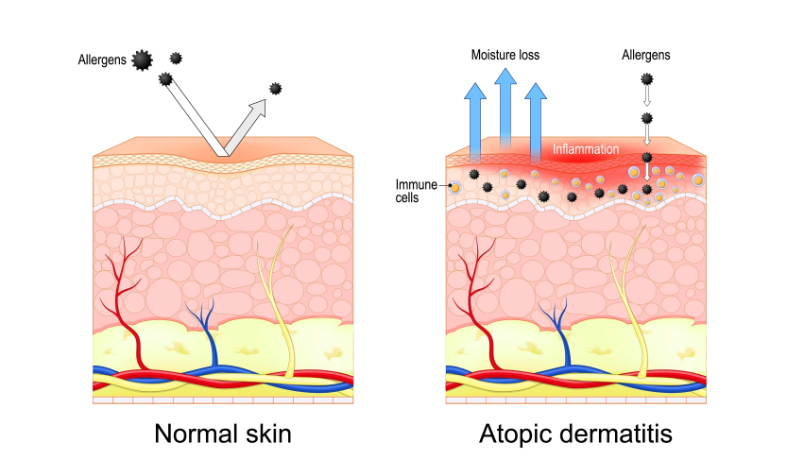
Regardless of what particular triggers and risks an individual has, the condition typically begins with a disruption in the epidermal layer of the skin. The epidermis serves as the outermost layer of the skin, providing a protective barrier against pathogens, environmental toxins, and water loss. It also plays a key role in regulating hydration, producing keratin for structural integrity, and generating melanin to protect against ultraviolet (UV) radiation.
Image 2: Atopic Dermatitis
Mutations of genes like the filaggrin gene (FLG) lead to a loss of lipid production and moisture protection, allowing for water loss and penetration of antigens or allergens into this layer of skin. This barrier dysfunction can also lead to disruption of normal skin flora and allow for bacterial overgrowth (Nemeth et al., 2024).
In addition to general dryness, the above factors lead to activation of the inflammatory response, with a barrage of mast cells, eosinophils, and T-cells responding to the area, causing inflammation and pruritus. When affected individuals scratch the area, this furthers the release of inflammatory markers and pruritogens, creating a vicious cycle. Keratinocytes also respond to the site of injury and eventually lead to lichenification of the skin (Nemeth et al., 2024).
The resulting signs and symptoms of eczema include (Cleveland Clinic, 2022):
Dry patches
Itchiness
Scaly, flaky, or crusty skin
Thick leathery patches
On physical examination, patients with eczema will often have (Cleveland Clinic, 2022):
Erythema
Scaly or even crusted patches or plaques
Excoriation
Vesicles
Lichenification
Image 3: Eczema
Though eczema can occur anywhere, affected areas of the body are most often exposed areas of skin, particularly over joints or bony prominences. This includes the hands, wrists, elbows, ankles, knees, face (particularly the cheeks), ears, and lips (Cleveland Clinic, 2022). The condition is typically diagnosed with history and exam alone, though additional allergy testing, serum labs, or skin biopsy is sometimes needed to rule out other conditions and determine triggers (Cleveland Clinic, 2022).
Eczema tends to appear in specific locations repetitively, based on age.
Table 1: Atopic Dermatitis Sites
Atopic Dermatitis Location Per Age Group
Age Group
Common Rash Location
Birth to 2 years of age
Face, back of scalp, chest, outer surfaces of arms and legs
2 years of age to puberty
Joint creases including knees and elbows, wrists, hands, around the eyes, around the mouth, behind the ears
Adults
Hands, fingers, elbows, scalp, eyelids, around the eyes, nipples
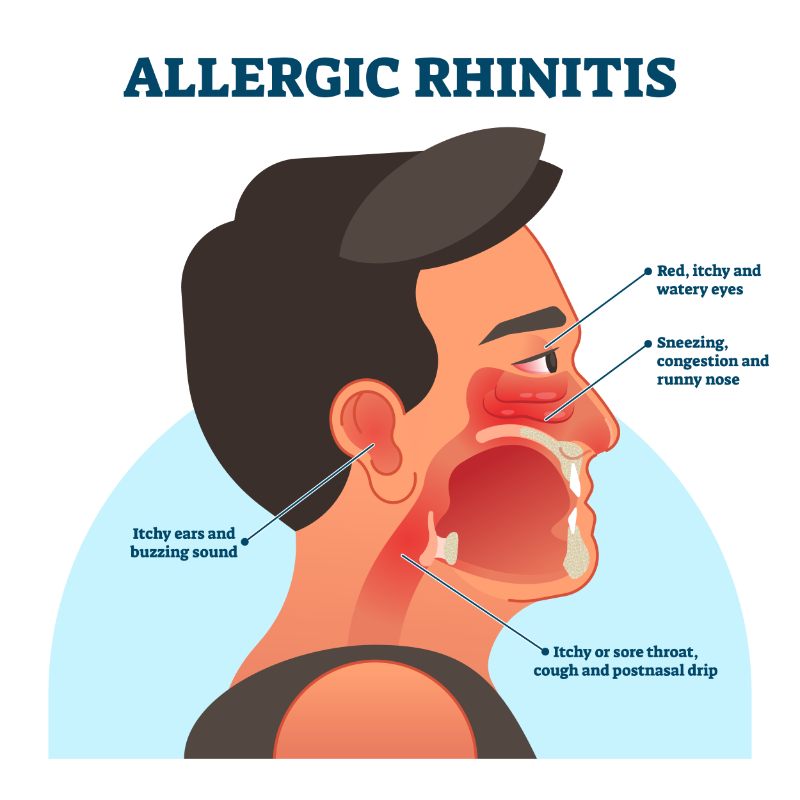
Allergic rhinitis is also the result of a complex interaction between genetics and environmental factors. Pollens are among the most common causes of the condition, with hundreds of different trees, grasses, and weeds dispersing pollen into the air that then comes in contact with the upper respiratory tract of humans, causing sensitization (Cleveland Clinic, 2023). Mold spores, pet dander, dust mites, and cockroaches are also common culprits (Cleveland Clinic, 2023).
Image 4: Allergic Rhinitis
For people without allergic sensitization, coming in contact with these environmental allergens is harmless and does not typically involve the immune system. However, for people with a genetic inclination for atopy, inhaling allergens through the nose or mouth may allow the allergen to penetrate the barrier of the nasal or oral mucosa. The allergen is engulfed by an Antigen Presenting Cell (APC) and then taken to CD4+ helper T cells, triggering an immune response (Akhouri & House, 2023). A cascade of inflammatory cytokines and IgE immunoglobulins follows. After this initial sensitization, the release of histamines, leukotrienes, prostaglandins, and many other inflammatory markers will occur every subsequent time the allergen is encountered (Akhouri & House, 2023). This leads to symptoms such as (Cleveland Clinic, 2023):
Nasal congestion or rhinorrhea
Sneezing
Red or watery eyes
Itchy nose, throat, eyes
Sinus pressure and headaches
Increased mucus in the nasopharynx
Postnasal drip and subsequent sore throat
Fatigue
Coughing, wheezing, and difficulty breathing
On physical examination, patients with allergic rhinitis may have (Cleveland Clinic, 2023):
Rhinorrhea
Boggy, bluish-gray nasal turbinates (swollen) in the nose
Nasal polyps
Conjunctival injection (redness of the sclera of the eye)
Middle ear effusion (fluid behind the eardrum)
“Allergic shiners” (dark circles beneath eyes due to nasal congestion)
“Allergic salute” (transverse nasal crease from frequent rubbing of the nose)
Postnasal drip causing red, irritated throat
Image 5: Allergic Shiners
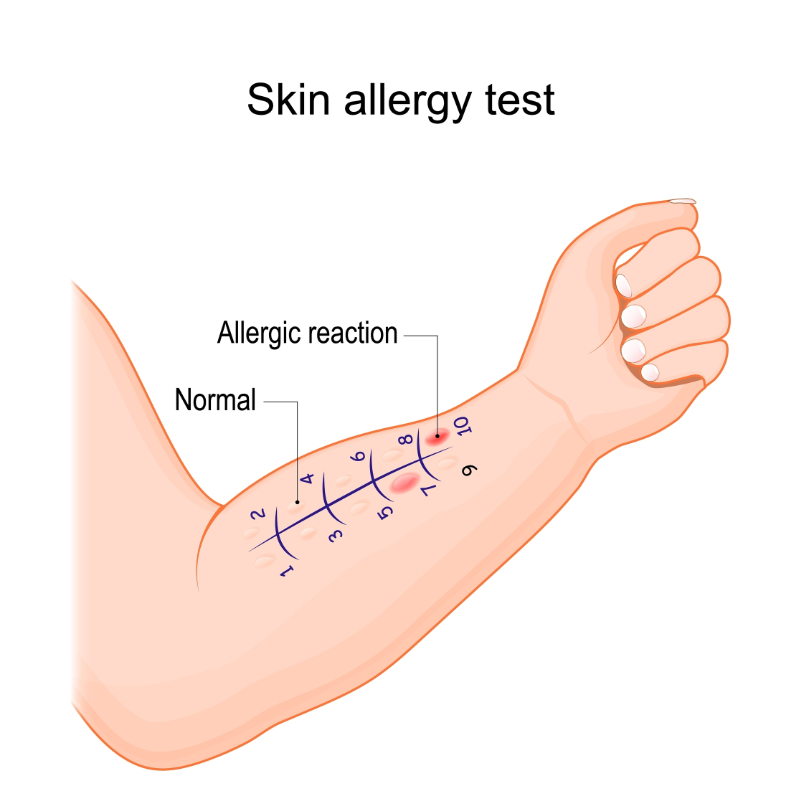
A history and physical exam can again usually help determine a diagnosis of allergic rhinitis and rule out other conditions such as viral colds. Blood allergy tests to check for IgE for specific allergens can also be performed, or intradermal tests can be done to check for a localized skin reaction when patients are injected with a small amount of allergen antigen (Cleveland Clinic, 2023).
Finally, asthma, which often develops later for people who have already suffered from eczema and/or allergic rhinitis, is again an interplay between genetic and environmental factors. Over 25 different genes affecting inflammation or the immune system can play a role in asthma development. There is a strong genetic correlation, with twins both experiencing the disease 25% of the time (Sinyor & Concepcion Perez, 2023). Individuals who are genetically predisposed to asthma are more likely to develop the disease if they have exposure to environmental risk factors as well (Sinyor & Concepcion Perez, 2023).
Environmental factors that increase the prevalence of asthma include (Sinyor & Concepcion Perez, 2023):
Frequent exposure to allergens (like pollen)
Cigarette smoke
Pollution
Pesticides
Metal or wood dust
Paint fumes
Glues
Dyes
Mold
There is a direct association between poor air quality (below U.S. Environmental Protection Agency or EPA standards) in industrialized areas and rates of asthma. Indoor air quality can also be impacted by gas stoves, pet dander, dust mites, and cockroaches (Sinyor & Concepcion Perez, 2023).
There is also a link between hygiene and bacterial colonization and development of asthma. Improved hygiene in modern society reduces the exposure to viruses and bacteria, which is actually shown to increase the rates of asthma (Sinyor & Concepcion Perez, 2023). The rate of asthma for children who live on farms, have frequent exposure to animals, and have more siblings is actually lower than that of children in smaller families with “cleaner” living conditions (Sinyor & Concepcion Perez, 2023). Birth by cesarean section and antibiotic use early in life both impacts development of the microbiome and have been shown to increase the risk of developing asthma (Sinyor & Concepcion Perez, 2023).
As a result, people with the genetic predisposition and sensitization to triggers have airway hyperresponsiveness. Various stimuli can cause an increased release of histamine from mast cells and increased free calcium that enhances smooth muscle contractility, both of which can occur in a much more hyperresponsive state than in people without asthma (Sinyor & Concepcion Perez, 2023).
There are two main phases of asthma exacerbation in the lungs. The early phase occurs when an individual encounters a trigger in their environment; IgE antibodies circulating in the body bind to mast cells and basophils which then release cytokines, histamine, prostaglandins, and leukotrienes when they come in contact with pollutants or triggers. Those cells contract the smooth muscles of the respiratory tree, causing airway narrowing.T lymphocytes produce interleukins to sustain inflammation and promote survival of eosinophils and basophils (Sinyor & Concepcion Perez, 2023).
This evolves into the late phase after a few hours, and the immune cells localize to the lungs, increasing bronchoconstriction and inflammation. There is also an influx of white blood cells (WBCs) and exudate and mucus in the respiratory tree, further blocking the airway. The combination causes significant airway obstruction and can increase work of breathing (Sinyor & Concepcion Perez, 2023).
Image 7: Asthma
Over time, scarring and increased epithelial cells leads to a thickening of the basement membrane of the bronchial tree and irreversible airway remodeling (Sinyor & Concepcion Perez, 2023).
Symptoms of asthma commonly include (Cleveland Clinic, 2025):
Coughing (often at night)
Wheezing
Shortness of breath
Chest tightness
On physical examination, patients with asthma will often have (Cleveland Clinic, 2025; Sinyor & Concepcion Perez, 2023):
Wheezing in one or more lung lobes
Cough
Drainage from nose (or postnasal)
Edema of nasal turbinates
Edema of throat
Barrel chest
Signs of increased work-of-breathing including nasal flaring, grunting, tripod positioning, retractions, and/or accessory muscle use
The triggers as well as frequency and intensity of symptoms determine what classification of asthma a person has. For frequency, asthma can be classified as either intermittent or persistent(Cleveland Clinic, 2025):
Patients with intermittent asthma only have symptoms some of the time and can feel normal in between.
Patients with persistent asthma have symptoms most of the time and may not ever feel a complete resolution of symptoms, even when well-controlled.
Causes of asthma can be allergic, from environmental triggers like pollution and allergens, or non-allergic from factors like exercise, weather changes, stress, and illness (Cleveland Clinic, 2025).
The intensity level of asthma symptoms can be categorized as either mild, moderate, or severe based on how much the symptoms impact a person’s ability to breathe and how easily the symptoms are managed with medications (Cleveland Clinic, 2025).
Asthma is often differentiated from other respiratory illnesses through history and exam. Unlike a self-limiting viral infection, asthma symptoms recur over a period of time. Symptoms of asthma are also responsive to bronchodilators and can be reversed, whereas cough and wheezing from viral illness often does not respond to bronchodilators (Cleveland Clinic, 2025). A history of eczema and allergic rhinitis also strengthens the probability of an asthma diagnosis.
Additional testing like spirometry and chest x-ray may be used to support a diagnosis of asthma (Cleveland Clinic, 2025). Spirometry, the most commonly used test to diagnose asthma, measures three main metrics to determine the extent of airway obstruction and remodeling (Sinyor & Concepcion Perez, 2023):
Forced vital capacity (FVC), which is the total amount of air exhaled after a full breath
Forced expiratory volume (FEV1), which is the amount of air a person can forcibly exhale in 1 second
Peak expiratory flow rate (PEFR), which is the fastest rate a person can forcibly exhale air
With a spirometry test, a FEV1/FVC ratio of less than 0.7 confirms airflow obstruction that can be associated with conditions such as asthma or chronic pulmonary obstructive disorder (COPD) (Sinyor & Concepcion Perez, 2023). Obtaining a spirometry measurement before and then after the administration of a bronchodilator, would reveal an improvement in airflow or what is termed a “reversible change” or “bronchodilator responsiveness”, that is very suggestive of asthma (Sinyor & Concepcion Perez, 2023; American Lung Association, 2024).
While a chest x-ray is normal for up to 75% of asthma patients and cannot diagnose asthma by itself, it can help to provide valuable clues for a patient who is hospitalized with trouble breathing, during a severe attack, or can help eliminate other potential conditions that cause similar symptoms (Sorgen, 2025). It can also be most helpful as a diagnostic tool for children less than five years of age that are commonly unable to perform breathing tests or spirometry (Sorgen, 2025). Possible asthma signs and complications that can be detected via chest x-ray include atelectasis (collapsed alveoli), pneumomediastinum (air trapped between the lungs), mucous plugging, increased bronchovascular markings, bronchial wall thickening, and pulmonary hyperinflation (Sorgen, 2025; StatPearls, 2025; Bell, 2025).
Treatment for all three conditions in the triad is often centered on minimizing exposure to allergens as a primary mode of management, and reduction of inflammation and immune response is a secondary approach to management.
For eczema, prevention looks like utilizing unscented soaps, fabric softeners, and hypoallergenic cosmetics, wearing nonabrasive clothing, and avoiding exposure to smoke, temperature extremes, pollutants, and allergens (food, environmental, or otherwise) as much as possible (Cleveland Clinic, 2022). In addition to avoiding triggers, patients are often advised to promote skin moisturization and repair the skin’s natural barriers. This is done through frequent moisturization of the skin with emollients like Vaseline ® or petroleum jelly, running humidifiers in the house, and keeping baths and showers short and with warm (not hot) water (Cleveland Clinic, 2022).
Persistent dryness and itching may need to be treated with topical corticosteroids to reduce inflammation and the overactive immune response. Topical steroids can be used for short bursts during flare-ups, usually twice daily. Common examples include (Nemeth et al., 2024):
There are also steroid free products like tacrolimus, pimecrolimus, and Eucrisa ® (crisaborole) that can be used to reduce side effects such as skin thinning or discoloration that can occur from frequent steroid use (Nemeth et al., 2024).
Because pruritus can be especially bothersome at nighttime, oral antihistamines can be used at night to reduce sleep disruption from itching (Nemeth et al., 2024). Diluted bleach baths once per week and intranasal mupirocin are also recommended for some patients to reduce the occurrence of secondary cutaneous infections (Nemeth et al., 2024). In severe cases, oral steroids and even immunosuppressant drugs may be indicated when trigger avoidance and more conservative treatment is not enough (Nemeth et al., 2024).
The prevention of allergic rhinitis also begins with avoidance of allergens. This can look like avoiding exposure to certain pets, high quality air purifiers and filters in the home, hard floors that are frequently swept, keeping windows closed, utilizing dust covers on bedding, getting rid of carpeting, frequently washing hands, and avoiding touching the face (Cleveland Clinic, 2023).
Whenever prevention is not enough, or exposure is unavoidable, antihistamines are the first line treatment. Antihistamines come in a variety of formulations, including oral pills and liquids, eye drops, nasal sprays, and inhalers. Common antihistamine choices include (Cleveland Clinic, 2023):
Loratadine
Cetirizine
Fexofenadine
Levocetirizine
These antihistamines work by blocking the histamine response and reduce nasal congestion, itchiness, and sneezing (Cleveland Clinic, 2023).
Short-term use of nasal decongestants like phenylephrine and pseudoephedrine can also be used to relieve sinus pressure and nasal congestion (Cleveland Clinic, 2023). Nasal and inhaled steroids like fluticasone can be used to reduce itchiness, congestion, and sinus pressure as well (Cleveland Clinic, 2023).
While the majority of the above treatment options are available over the counter, sometimes a prescription strength treatment is necessary. This can include leukotriene receptor blockers, which also play a role in the inflammatory response. Montelukast is a common choice for management of allergies when antihistamines are not enough. Oral tablets or subcutaneous injection for immunotherapy, or allergy shots, are also used in severe cases where symptom control has not been maintained with other measures (Cleveland Clinic, 2023).
For patients with asthma, avoiding triggers looks very similar to home maintenance measures used to minimize allergic rhinitis; frequent vacuuming and dusting to reduce dust mites, air purifiers and filters, getting rid of carpet in the home, keeping pets off of furniture, avoiding smoke, and keeping windows closed (Cleveland Clinic, 2025). Asthma can also be flared with exercise or with viral upper respiratory infections, so keeping an eye on symptoms and respiratory function is important (Cleveland Clinic, 2025).
Treatment of asthma is done via a stepwise approach. At a minimum, all patients with asthma will have an inhaled short-acting beta agonist (SABA), like albuterol, that can be used to relieve airway constriction, coughing, and shortness of breath, should those symptoms occur (National Heart, Lung, and Blood Institute, 2021). SABAs, or bronchodilators, work by selectively relaxing the smooth muscles surrounding the airways, relieving airway constriction and chest tightness. These can also be used preventively, such as before exercise, to keep airways open and reduce the occurrence of respiratory symptoms.
For patients with more persistent and frequent symptoms, a range of low, medium, and high dose inhaled corticosteroids (ICS) should be prescribed (National Heart, Lung, and Blood Institute, 2021). These medications include options such as (National Heart, Lung, and Blood Institute, 2021):
Fluticasone
Budesonide
Mometasone
It is significant to note here that the Global Initiative for Asthma (GINA) recommendations are now emphasizing the importance of incorporating the use of early ICS-formoterol rather than SABAs as monotherapy (Dubin et al., 2024; Global Initiative for Asthma [GINA], 2024; Beasley et al., 2019). One main rationale is that SABAs are treating the symptoms, but not the disease (GINA, 2024). Reliever treatment with ICS-formoterol, such as budesonide-formoterol, has been associated with a substantial reduction in severe asthma exacerbations and emergency room visits as they help to reduce the inflammation in addition to creating bronchodilation (Watto & Williams, 2025; Krings et al., 2023; Beasley et al., 2019). In fact, according to Beasley et al. (2019), their published study on a year-long randomized controlled trial (RCT) including over 650 adult patients with mild asthma, budesonide-formoterol, being used as needed, was determined to be superior to albuterol alone, being used as needed, for the prevention of asthma exacerbations (Beasley et al., 2019).
Oral montelukast and inhaled long-acting beta agonists (LABAs) like salmeterol or formoterol, can also be added in until symptoms are well controlled and not interfering with sleep or daily function (National Heart, Lung, and Blood Institute, 2021).
Once well-controlled, patients with asthma may still experience flare-ups, either due to an increase in seasonal triggers, physical activity, or other illnesses (particularly viral upper respiratory illnesses). In the case of flare-ups with coughing and wheezing not managed by use of a SABA or when the patient is exceeding the recommended use of SABA inhalers (using it more and more often), a short burst of high dose oral corticosteroids is needed (National Heart, Lung, and Blood Institute, 2021). Recommended oral corticosteroids can include (National Heart, Lung, and Blood Institute, 2021):
Prednisone
Prednisolone
Dexamethasone
Use of a peak flow meter at home to track patients’ baseline lung function as well as detect exacerbations is recommended (National Heart, Lung, and Blood Institute, 2021).
There are plenty of symptoms in all of the above conditions to impact quality of life for atopic individuals, but there are also a host of common complications and comorbid conditions that need to be considered.
With consideration for eczema, secondary infection of the skin is a common complication. Skin barrier dysfunction as well as breaks in the skin from rashes and scratching make overgrowth of bacterial, fungal, and viral pathogens all too easy. The most common organism responsible for a secondary skin infection in eczema is Staphylococcus aureus (S. aureus), which colonizes the skin of around 90% of people with eczema, compared to only 10% of the rest of the population.
Image 8: Staphylococcus Aureus
Impetigo, boils, folliculitis, and cellulitis can all occur with an overgrowth of S. aureus. Intranasal mupirocin and diluted bleach baths can help reduce the density of S. aureus colonization on the skin and, therefore, reduce the risk of secondary bacterial infection. If an infection does occur, it can be treated with broad spectrum antibiotics ranging from topical, oral, and even intravenous, depending on infection severity. Antibiotic resistance due to improper and overuse of antibiotics sometimes complicates treatment of secondary bacterial infections (National Eczema Society, 2023; Nemeth et al., 2024). Therefore, antibiotics should be used judiciously in patients with eczema to reduce future treatment difficulties (National Eczema Society, 2023; Nemeth et al., 2024).
People with eczema are also more susceptible to herpes simplex virus (HSV) causing a secondary infection through compromised skin integrity (Nemeth et al., 2024). This condition is known as eczema herpeticum and causes widespread clusters of blisters as well as systemic symptoms like fever, fatigue, and malaise. Though this condition is very rare, it is a medical emergency and can lead to viral meningitis, encephalitis, and death (Nemeth et al., 2024).
Another secondary viral pathogen of concern with eczema is the coxsackie virus responsible for the common childhood illness, hand, foot, and mouth disease (HFMD). Eczema coxsackium presents with blisters over areas affected by eczema and additional symptoms like fever and diarrhea (Nemeth et al., 2024). Treatment of secondary viral skin infections is largely supportive in nature as well as maintaining hygiene of the existing lesions and the rest of the skin to prevent opportunistic bacterial infections.
Fungal pathogens such as candida and dermatophytes responsible for tinea may also cause secondary infection over eczema lesions, particularly on areas of the skin that are frequently dark or moist, such as between folds. Topical antifungals are often adequate to treat these secondary infections and there is not an issue of resistance as there is with bacteria (National Eczema Society, 2023).
Over time, chronic skin inflammation and scratching can lead to lichenification (thickened and leathery) and scarring.Long-term use of topical corticosteroids, especially at higher doses, can also atrophy the skin, causing a shiny, translucent appearance with loss of pigmentation and spider veins and more visible blood vessels beneath (National Eczema Society, 2023). Skin changes with the rash and with side effects from treatment can negatively impact self-esteem and potentially lead to anxiety or depression, especially in patients with more severe disease (National Eczema Society, 2023).
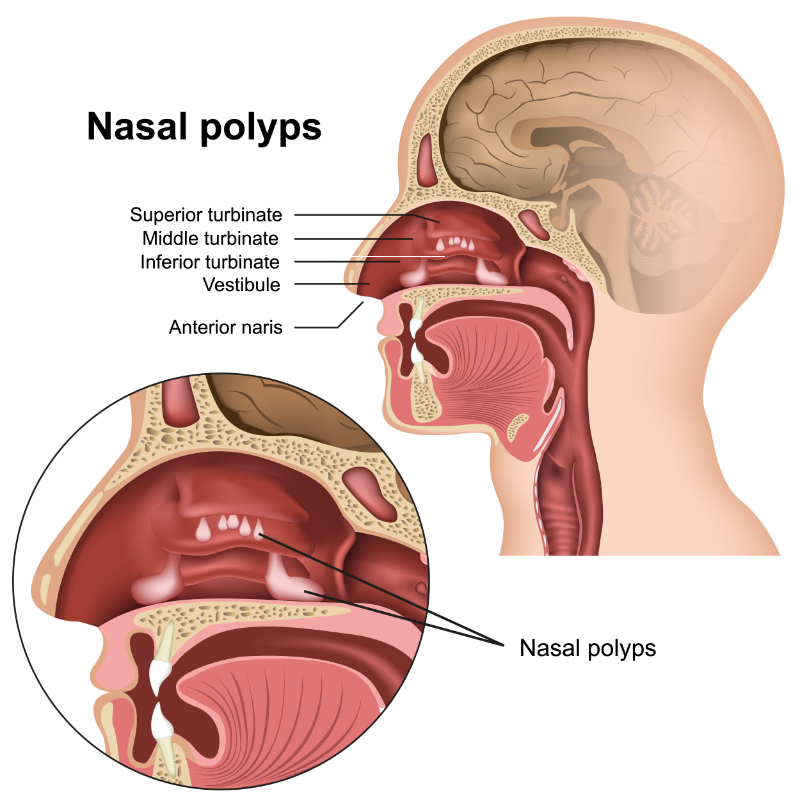
Allergic rhinitis that persists for more than 3 months at a time can develop into chronic rhinosinusitis, characterized by chronic inflammation of the paranasal sinus mucosa, causing nasal polyps to develop. While polyps themselves are typically benign, they can cause and contribute to a variety of symptoms like (Akhouri & House, 2023):
Nasal congestion
Loss of taste and smell
Snoring
Facial pain or pressure
Image 9: Nasal Polyps
Nasal polyps can often be managed with steroid nasal sprays and saline irrigation, though surgical removal may be indicated for patients with numerous or large polyps that do not respond to more conservative treatment (Akhouri & House, 2023).
Hypertrophy of the adenoids and eustachian tube dysfunction are also common in patients with allergic rhinitis due to the chronic inflammation in the upper airway (Akhouri & House, 2023). These patients may report a feeling of ear fullness or pain, and frequent popping or pressure change sensations. This can further develop into otitis media with effusion and cough from postnasal drip (Akhouri & House, 2023).
Use of allergen desensitization treatment (or allergy shots) can lead to an increased risk of acute exacerbations or even anaphylaxis with the dosed exposure to allergens (Akhouri & House, 2023).
The chronic nature of asthma can cause a variety of acute and long-term complications, the most significant of which is airway remodeling. Permanent thickening of airways, increased mucus production, and loss of elasticity of the lungs reduces lung function and permanently impacts airflow (Hashmi & Cataletto, 2024). This contributes to (Hashmi & Cataletto, 2024):
Coughing
Wheezing
Chest tightness
Activity intolerance
Increased hyperresponsiveness
Exacerbations
Airway remodeling and use of corticosteroids also increases the risk of respiratory infections like cold viruses, influenza, and pneumonia. These types of infections are more likely to cause severe symptoms and asthma exacerbations in these patients.
Long-term use of inhaled corticosteroids can cause side effects like thrush and voice changes. Use of systemic corticosteroids can also have many side effects over time, including (Hashmi & Cataletto, 2024):
Weight gain
Osteoporosis
Hypertension
Diabetes
Reduced immune function making patients more susceptible to infection
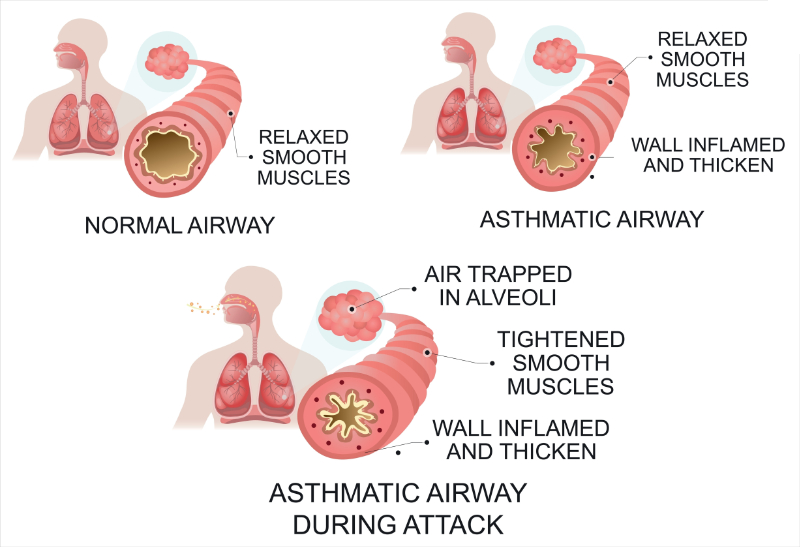
A prolonged asthma attack that does not respond to rescue treatment is known as status asthmaticus and is a medical emergency. This condition can lead to respiratory failure and death if not addressed emergently with intravenous corticosteroids, supplemental oxygen, nebulized bronchodilators, and mechanical ventilation if needed (Hashmi & Cataletto, 2024).
Image 10: Asthma Attack
Frequent symptoms and exacerbations can negatively impact quality of life and contribute to mental health concerns like anxiety and depression as well (Hashmi & Cataletto, 2024). Therefore, anxiety and depression can be commonly suffered comorbidities of patient with asthma (Hashmi & Cataletto, 2024).
As mentioned previously, food allergies are a common comorbid condition for atopic individuals. It would make sense that people with hypersensitive immune systems would also experience an atopic response to food proteins, which is the primary allergy trigger in foods. As with other atopic conditions, there is a lot of overlap; up to 39% of people with eczema also have food allergies and 35%-50% of people with food allergies also have asthma (Asthma and Allergy Network, 2024).
Being sensitized to food proteins can present in a variety of ways and may affect different body systems in mild to severe ways:
In the integumentary system, symptoms that often result include:
Flushing
Itching
Hives
As far as upper respiratory symptoms, the following are often seen:
Hoarseness
Mouth or throat itching or swelling
Sneezing
Rhinorrhea
Lower respiratory symptoms that are elicited include:
Difficulty breathing
Coughing
Wheezing
Chest tightness
Gastrointestinal symptoms that are seen can include:
Nausea
Vomiting
Cramping
Diarrhea
Other general signs and symptoms can include:
Dizziness
Syncope
Confusion
Anxiety or feelings of impending doom
These symptoms can also overlap with symptoms of other conditions in the atopic triad, so it is important to have a thorough understanding of a patient’s history and disease management to help differentiate the cause of symptoms at any particular time and to avoid missing a food reaction. For example, skin irritation is a common presentation of food allergy; if a patient is treated with a skin care regimen and topical corticosteroids (as with classic eczema) but the food allergen is not removed, symptom management and reduction of symptoms will be limited, and the flare-ups will continue until the causative agent is removed (Kim & Burks, 2025).
A person can be sensitized to any food, but there are certain groups that are more commonly allergy-inducing than others. The most common food allergens are milk, eggs, fish, shellfish, tree nuts, peanuts, wheat, soybeans, and sesame. These foods are all required by the U.S. Food and Drug Administration (FDA) to be included on food labels in order to make allergen avoidance easier for consumers (U.S. Food and Drug Administration [FDA], 2024).
Take a look at some more of the top most common allergens in the following image, keeping in mind that “soya” is a common term for “soy,” especially in British English (Cunha, 2020).
Image 11: Top Allergens
Current recommendations to reduce allergies are to introduce common allergic foods early in life for infants to reduce the risk of sensitization (American Academy of Pediatrics [AAP], 2019). Additives like peanut powder can be added in small amounts to baby food to expose infants to small amounts of the food whenever solids are begun around 6 months of age. Any time new foods are introduced, infants should be monitored for signs of an allergic reaction, particularly in those with a family history of atopy or in children who already have eczema (AAP, 2019).
For patients who have food allergies, treatment includes (American Academy of Allergy Asthma and Immunology [AAAAI], 2025):
Avoidance of the food
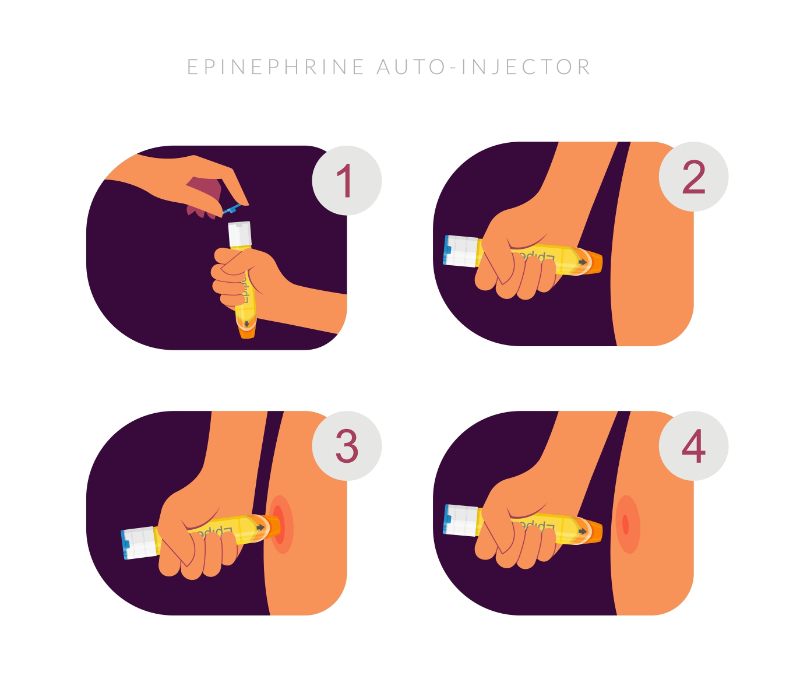
Carrying an epinephrine injector pen for severe allergies
Image 12: Epinephrine Auto-Injector Use
For patients with known severe food allergies, having an epinephrine auto-injector at all times is absolutely essential as anaphylactic symptoms are always a risk with subsequent exposures to the known allergen (AAAAI, 2025).
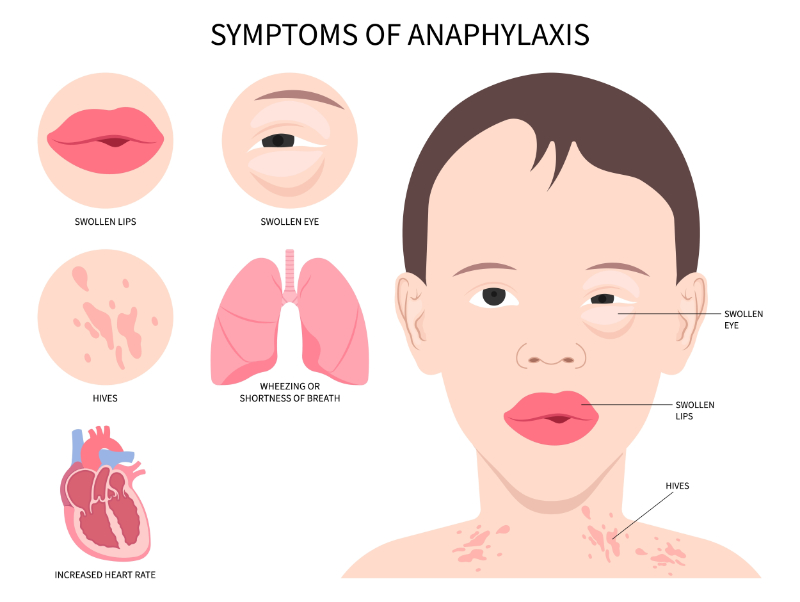
Take a look at the following image to review some of the signs and symptoms of an anaphylactic reaction to an allergen (AAAAI, 2025).
Image 13: Symptoms of Anaphylaxis
Immunotherapy with daily oral or sublingual administration of carefully dosed allergens can also help patients build a slight tolerance to the allergen. Immunotherapy is not curative and merely serves to create a safety net if a patient accidentally ingests a food containing their allergen; with immunotherapy, they are more likely to be able to consume a bite or two of an allergen food before an anaphylactic reaction would occur (AAAAI, 2025).
Treatment with oral immunotherapy (OIT) is intensive and requires frequent office visits for dosage adjustments and monitoring of increased doses. Doses must be taken daily for life to maintain therapeutic effect. There is also the risk of severe reaction to an OIT dose and epinephrine must always be kept on hand (AAAAI, 2025).
Nurses are a key component in the holistic management of patients with atopic disease and the execution of early identification of disease, patient education, and facilitation of treatment serves to improve patient outcomes and enhance quality of life. Nurses in every specialty are likely to encounter patients who suffer from atopic conditions, and implications will vary by setting and if the patients are healthy or ill. The following is a list of some of the most important implications, though this list is not exhaustive and there is always room to improve on comprehensive care to reduce disease severity and complications.
At any point in patient care and the diagnostic process, a detailed patient history is one of the most critical tools to identify risk factors, potential triggers, and patterns of disease overlap and progression. When gathering a history on patients with any indications for atopy, high suspicion for atopic disease should be present. Key historical components should include:
Family History:
Patients should be assessed for first degree relatives with eczema, allergic rhinitis, food allergies, asthma, and other atopic and hyper-responsive immune conditions.
Patients with a strong family history should be considered high risk for developing atopy symptoms themselves and any symptoms should be evaluated with this in mind.
Personal History (past medical and current illness):
Current or past diagnoses of any atopic conditions like eczema or allergies place a person at risk for developing future or comorbid atopic conditions.
History of severe reactions like anaphylaxis or hospitalization are also important for assessing disease severity.
Assess for any current flare-ups such as increased symptom severity, sleep disruption, pain, or signs of infection.
Assess for signs of compromised immune system like frequent infections.
Social determinants of health such as education level, socioeconomic status, neighborhood and home environment, access to healthcare services, etc all play an important role in determining a patient's risk of disease, severity, and ability to participate in disease management.
Assess barriers to utilizing the healthcare system such as affordability, transportation, language, etc. Does the patient have insurance and is it adequate to cover the costs of atopic disease?
Triggers:
Ask about exposure to and management efforts for in-home triggers such as pet dander, carpeted rooms, cigarette smoke, dust mites, cockroaches, mold, and poor ventilation.
External environmental triggers like air pollution and chemicals or seasonal changes like pollen, temperature extremes, and humidity fluctuations may also be triggering and are much less in a patient’s control to manage.
Also ask about hygiene practices and cosmetic usage, looking for hard water, fragrances, harsh soaps or cleaning products, and bathing habits (frequency and water temperature) and skin response to these triggers.
Medications & Treatment Adherence:
Reconcile medication list and look for prescription of and compliance with topical or systemic steroids, antihistamines, corticosteroid or bronchodilator inhalers, and immunotherapy.
Ask about side effects to any prescribed medications.
Assess compliance with non-prescription management techniques like skin care routines and use of moisturizer.
Understanding the ways that atopy affects multiple body systems is important and guides assessment. Even if a patient presents with a complaint of only one affected body system, the overlap in inflammatory response makes it prudent for nurses to assess other body systems to ensure simultaneous symptoms and atopic processes are not developing. Particular areas to pay attention to should include:
Skin:
Assess skin color, texture, moisture, and uniformity.
Note any lesions or areas of impaired skin integrity, particularly in areas like the hands, wrists, elbows, and knees.
Note signs of secondary infection like crusting, pustules, weeping, and pain.
Note any skin thinning, pigment loss, hair loss, or other signs of side effects from long-term use of topical medications.
Ear/Nose/Throat (ENT):
Assess the nasal mucosa for pale, blue, or boggy turbinates or nasal polyps.
Assess for postnasal drip, allergic shiners, and transverse nasal crease.
Assess for shotty cervical lymph nodes and otitis media with effusion.
Monitor for mouth breathing, watery eyes, and conjunctival injection.
Respiratory:
Assess for cough, dyspnea, decreased oxygen saturation.
Listen to lungs, paying attention to any wheezing or decreased air exchange.
Assess for signs of respiratory distress, including retractions, nasal flaring, or tripod positioning.
Assess for signs of airway remodeling such as barrel chest and prolonged expiration.
Systemic Assessment:
Assess for fatigue, sleep disruptions, difficulty concentration, or dizziness.
Mental Health:
Assess for self-esteem impact, chronic absenteeism from work or school, social isolation, anxiety, or depression.
Patient education is a foundational principle for the nursing role and there is plenty of room for teaching when caring for patients with atopic conditions. The cornerstone of managing atopy is managing and avoiding triggers to prevent symptoms and flare-ups from occurring.
Eczema Prevention Teaching:
Bathing practices should include use of lukewarm water limited to 5-10 minutes, avoiding harsh or heavily fragranced soaps, and adding water softeners where needed. Diluted bleach baths once per week are recommended for secondary infection prevention purposes.
A moisturizing routine of fragrance-free emollients twice daily is necessary even when skin is clear. Running a humidifier in living spaces during dry months is also useful.
Patients should avoid irritating, rough fabrics like wool, polyester, or other synthetic materials.
Dust frequently, vacuum often, cover bedding with hypoallergenic covers, and do not allow pets to sit on furniture or beds.
Allergic Rhinitis Prevention Teaching:
Utilize a HEPA filter indoors. Keep windows closed. Clean frequently to remove and prevent dust, cockroaches, and mold.
Use nasal sprays or rinses to clear nasal passages.
Check pollen counts. Shower and change clothes after being outdoors during high pollen seasons.
Asthma Prevention Teaching:
Educate on correct inhaler technique with a spacer.
Discourage cigarette smoking or exposure to second-hand smoke.
Encourage bronchodilator usage before exercise.
Encourage annual flu and covid vaccines, avoiding sick contacts, and wearing a mask when in crowded or public spaces.
The following image is of an inhaler spacer, as briefly mentioned above, that can be used to improve the use and effectiveness of inhalers by helping to deliver the medication more directly to the lungs versus it getting stuck in the mouth or throat (Roland, 2025).
Image 15: Inhaler Spacer
In addition to trigger avoidance, education is also needed regarding maintenance therapy to reduce severity and avoid exacerbations. It is also important to teach patients about red flags and when to seek treatment for exacerbations.
Eczema Management Patient Teaching:
Teach about appropriate usage of prescribed topical corticosteroids, usually used twice daily, or nonsteroidal topical medications.
Red flags include worsening itching, redness, pain, pustules, crusting, satellite lesions, or weeping lesions.
Allergic Rhinitis Management Patient Teaching:
Counsel on use of daily antihistamines or leukotriene modifiers and/or nasal corticosteroids.
Discuss when allergen immunotherapy might be useful and refer when needed.
Red flags include itching and swelling of the respiratory tract, chest tightness, or difficulty breathing.
Asthma Management Patient Teaching:
Teach about appropriate use of daily inhaled corticosteroid versus as-needed bronchodilators.
Assess for appropriate symptom control or when a patient may need to move up the stepwise approach of asthma management.
Teach the patient to utilize a peak flow meter periodically at home to monitor asthma symptoms and to detect potential exacerbations early on.
Utilize an asthma action plan to teach patients how to manage breakthrough symptoms and recognize when a flare-up is occurring.
Red flags include severe wheezing, difficulty breathing or speaking, no improvement with multiple uses of rescue inhaler, nasal flaring, retractions, cyanosis, and tripod position.
Nurses who work in urgent cares, emergency departments, and hospital settings are more likely to encounter patients who are experiencing a flare-up or severe disease. Patients may seek emergency care or require hospitalization for severe secondary skin infections, anaphylaxis, or other severe allergic reactions, and respiratory distress.
Nursing interventions common for patients experiencing atopic flare-ups can include:
Administration of intravenous antibiotics or corticosteroids
Assessment of wounds and changing dressings
Administration of nebulized bronchodilators
Monitoring respiratory status to detect worsening distress or signs of pending respiratory failure
Administration of supplemental oxygen or monitoring of mechanical ventilation
Administration of intramuscular epinephrine
In the event that epinephrine is necessary, it is important to remember that the half-life of epinephrine is fairly short and the reaction to an allergen may outlast its effects. Therefore, patients who have had epinephrine administered for anaphylaxis need to be monitored for a return of symptoms and the need for subsequent epinephrine injection.
Additional monitoring that can be required in emergent situations is for the development of systemic infection or sepsis. Vital signs should be monitored for fever, tachycardia, and hypotension.
Collin is a 10-year-old male presenting to the pediatric clinic with complaints of frequent coughing with activity and disrupting sleep at nighttime for the past 3-4 weeks.
Collin has a history of eczema and allergic rhinitis related to seasonal pollen and cats. For his eczema, he uses a daily emollient and occasionally needs to use topical triamcinolone 0.1% BID for flare-ups. His allergic rhinitis is fairly well managed with air purifiers at home, keeping windows closed, and 10 mg cetirizine daily. The cetirizine also helps with his eczema itching at night. He does have an increase in nasal congestion when he lets the family cat sleep in his bed.
His mother has a history of eczema and asthma, and his older sister has a food allergy to peanuts.
Today, he reports around a month of a frequent dry cough and chest tightness when running in PE and after school soccer. It has gotten so bad that he has had to stop playing several times in the last week. This has increased to an intermittent dry cough even at rest, especially at night. His mother reports she let him use her albuterol inhaler on one occasion which seemed to help quickly.
On exam, he has clear eyes and ears, boggy nasal turbinates, and postnasal drip noted into the pharynx. His lungs have faint wheezing heard in the lower lobes as well as a diminished expiratory effort.
Collin is given a 5-day steroid burst of high dose prednisone to be taken daily and treat the current airway constriction. He is also given an albuterol inhaler for PRN use with cough, wheezing, and shortness of breath.
Collin returns in 2 weeks for a follow-up. His lungs are clear and he reports it is easier to breathe, but he is still experiencing nighttime coughing and significant coughing with activity, even with the albuterol prior to sports.
Because of this, he is started on a twice daily low dose fluticasone inhaler and given a diagnosis of mild, persistent asthma.
When he returns in a few more weeks, he reports that his symptoms are very well managed now, and he is no longer coughing at night or with activity. He did have a soccer practice last week where he forgot to use his albuterol beforehand and experienced some coughing, but this resolved quickly when he stopped playing to use the albuterol inhaler.
He is scheduled for follow-up in another 3 months to assess how he is doing with the season change.
Collin’s case is a classic demonstration of the progression of the atopic triad, with eczema preceding allergic rhinitis and asthma and a strong family history of atopic conditions. There is a high level of interconnectedness between the immune dysregulation of these conditions.
Management of the triad focuses on underlying inflammation and hypersensitive immune response, with slightly different and sometimes overlapping approaches for each affected body system.
Collin has an involved family who is used to making necessary home environment changes to minimize symptoms of atopy. Use of HEPA filters and keeping windows closed at home will help minimize his asthma symptoms as well as his allergy symptoms.
He is brought to the clinic in a timely manner to evaluate the new onset of cough and is started with treatment quickly. He is already utilizing an appropriate dosage of an antihistamine for eczema and allergic rhinitis which may help reduce his allergen and potential trigger exposure for his new diagnosis of asthma.
There is a gap in the time between when Collin is first assessed and given an oral steroid and when he is diagnosed with asthma and prescribed a daily inhaled corticosteroid. Given his family history of asthma as well as his existing presence of atopic conditions, his risk of asthma is relatively high, and he could have received more aggressive treatment or even referral for spirometry testing to better evaluate his lung capacity and the extent of obstruction.
It also seems that he could use more education on reducing exposure to triggers, like keeping the cat out of his room and using albuterol prior to activity.
At his age, the impact on his symptoms of his ability to participate in sports and peer activities may also affect his self-esteem or contribute to a comorbid mental health condition like anxiety or depression. Assessment of baseline mental health as well as monitoring intermittently for any emerging symptoms is important, especially in childhood when much of developmentally appropriate activity centers on interaction with peers and physical activity.
Collin’s case illustrates the complexity of managing the atopic triad, emphasizing the importance of a multidisciplinary approach. With proper interventions, education, and lifestyle modifications, his symptoms can be controlled, allowing him to lead a healthy and active life. Continued follow-up with healthcare providers will be essential to adjust treatment as needed and ensure optimal disease management.
Akilah is a 32-year-old woman with a history of the atopic triad (eczema, seasonal allergic rhinitis, and moderate persistent asthma). She presents to her primary care provider with a 2-week history of an eczema flare-up with increasing itchiness and pain.
Akilah’s symptoms are typically very well controlled. She adheres to a strict routine of moisturizing her skin, as well as taking 10 mg daily loratadine during spring months (currently not on it) and BID mometasone inhaler year-round. She reports recently moving to a different apartment and has had an increase in nasal congestion and sneezing. She has also needed her albuterol inhaler 3-4 times over the last week.
She noted that her hands were becoming drier and itchier than usual and developing a flare-up of irritated, scaly lesions. She has a prescription for 2.5% hydrocortisone for such symptoms but was unable to find it after moving. Her hands have worsened to painful, crusting, and oozing lesions over the last 4-5 days.
On exam, there are erythematous plaques with serous weeping and honey-colored crusting on the tops of her hands and onto her wrists with mild edema and tenderness. She also has some dry, scaly plaques on her antecubital and popliteal fossae.
Akilah is given a 10-day course of oral cephalexin 500 mg BID for a secondary bacterial infection, likely Staphylococcus aureus or Streptococcus pyogenes. She is also given a medium potency topical steroid, triamcinolone 0.1% for BID use to the dry patches. Skin care routines and triggers are reviewed. She is advised to restart her springtime loratadine for management of itching, especially at night.
When she returns 2 weeks later, the secondary infection has healed, and the erythema and scaling of the lesions has improved but not resolved. She also has a few new lesions on her neck and forearms that have come up since the previous visit. She is using the topical triamcinolone, which is keeping the lesions from becoming worse or infected, but is not resolving them.
Despite restarting the loratadine, she has persistent nasal congestion, though it is a little better. Her mometasone dosage is increased to combat persistent asthma symptoms.
After several more months of flare-ups and increased allergy and asthma symptoms, it is discovered that there is significant cockroach infestation and mold at the apartment Akilah had recently moved to. She is able to end her lease and move to a new location in a different part of town and her symptoms all begin to resolve very quickly, restoring her previous level of symptom control.
The prolonged exposure to indoor allergens in her new apartment perpetuated chronic inflammation, resulting in worsened skin barrier dysfunction, increased histamine response, and heightened immune system activation. The persistence of symptoms despite appropriate medical therapy suggests that the inflammatory response was being continuously triggered by the environmental exposures.
This case also highlights how housing conditions and environmental allergens play a major role in chronic disease management. Many patients, particularly those in urban areas or low-income housing, face barriers to managing allergen exposure due to factors such as mold, dust mites, cockroaches, and poor ventilation.
In Akilah’s case, ending her lease and relocating significantly improved her symptoms, demonstrating the powerful impact of environmental control in managing atopic disease. Healthcare providers should proactively screen for environmental and socioeconomic barriers and provide resources for allergy-proofing living spaces when possible.
Akilah typically has good management of the triad of conditions and normally has her symptoms under very good control. Prompt identification of a flare-up requiring medical attention helped her receive treatment in a timely manner. Her secondary skin infection was treated appropriately and resolved quickly without spreading. Overlapping treatment of her conditions allowed her to easily resume her antihistamine to manage nighttime skin pruritus.
Focusing solely on the secondary skin infection as a singular condition, and then later on the increasing asthma severity, rather than recognizing a simultaneous flare-up of all conditions in the triad limited the healthcare provider from recognizing that a systemic reaction was occurring and a more thorough history of triggers from being conducted. Earlier recognition of exposure to new triggers at a new housing location could have prevented this patient from experiencing prolonged exacerbation of symptoms. Inclusion of an assessment of living conditions should be a routine component of assessment of chronic conditions and patient history.
Akilah’s case highlights the importance of recognizing the interconnected nature of atopic conditions and the need for a holistic, patient-centered approach in managing chronic inflammatory diseases. Her history of the atopic triad indicates an underlying hypersensitivity to environmental allergens, which ultimately played a central role in her exacerbation. Her social history, primarily her housing conditions, needs to be considered as an important intertwined factor.
Healthcare professionals in any specialty may encounter individuals suffering from the atopic triad. A solid baseline understanding of this condition as a cluster, as well as individual conditions, is important to providing high quality nursing care. These diagnoses have significant implications for how a patient’s inflammation response works, what types of symptoms or complications they are at risk for, and what types of medications they may be prescribed. With an evidence-based understanding of this cluster, nurses can provide quality and comprehensive care and improve patient outcomes at all levels of care and across a wide range of settings.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Akhouri, S., & House, S. A. (2023). Allergic rhinitis. In StatPearls. StatPearls Publishing. Visit Source.
American Academy of Allergy Asthma and Immunology. (AAAAI). (2025). The current state of oral immunotherapy. American Academy of Allergy Asthma and Immunology (AAAAI). Visit Source.
American Academy of Pediatrics. (AAP). (2019). AAP clinical report highlights early introduction of peanut-based foods to prevent allergies. HealthyChildren.org. Visit Source.
Asthma and Allergy Foundation of America. (AAFA). (2025). Cost of asthma on society. Asthma and Allergy Foundation of America (AAFA). Visit Source.
Asthma and Allergy Network. (2024). The asthma-food allergy connection. Asthma and Allergy Network. Visit Source.
American Lung Association. (2024). Spirometry implementation quick glance guide. American Lung Association. Visit Source.
Beasley, R., Holliday, M., Reddel, H. K., Braithwaite, I., Ebmeier, S., Hancox, R. J., Harrison, T., Houghton, C., Oldfield, K., Papi, A., Pavord, I. D., Williams, M., & Weatherall, M. (2019). Controlled trial of budesonide–formoterol as needed for mild asthma. The New England Journal of Medicine, 380(21), 2020–2030. Visit Source.
Bell, D. (2025). Asthma. Radiopaedia. Visit Source.
Centers for Disease Control and Prevention. (CDC). (2023a). Allergies. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2023b). Most recent national asthma data. Centers for Disease Control and Prevention (CDC). Visit Source.
Cunha, J. (2020). What are the top 14 food allergens? eMedicineHealth. Visit Source.
Dubin, S., Patak, P., & Jung, D. (2024). Update on asthma management guidelines. Missouri Medicine, 121(5), 364. Visit Source.
Emfietzoglou, M. (2025). Atopic triad. Osmosis from Elsevier. Visit Source.
Hashmi, M. F., & Cataletto, M. E. (2024). Asthma. In StatPearls. StatPearls Publishing. Visit Source.
Global Initiative for Asthma. (GINA). (2024). 2024 GINA main report: Global strategy for asthma management and prevention. Global Initiative for Asthma (GINA). Visit Source.
Justiz Vaillant, A. A., Modi, P., & Jan, A. (2024). Atopy. In StatPearls. StatPearls Publishing. Visit Source.
Kim, E.H. & Burks, W. (2025). Patient education: Food allergy symptoms and diagnosis (Beyond the basics). UpToDate. Visit Source.
Krings, J. G., Gerald, J. K., Blake, K. V., Krishnan, J. A., Reddel, H. K., Bacharier, L. B., Dixon, A. E., Sumino, K., Gerald, L. B., Brownson, R. C., Persell, S. D., Clemens, C. J., Hiller, K. M., Castro, M., & Martinez, F. D. (2023). A call for the United States to accelerate the implementation of reliever combination inhaled corticosteroid–formoterol inhalers in asthma. American Journal of Respiratory and Critical Care Medicine, 207(4), 390–405. Visit Source.
Licari, A., Magri, P., De Silvestri, A., Giannetti, A., Indolfi, C., Mori, F., Marseglia, G. L., & Peroni, D. (2023). Epidemiology of allergic rhinitis in children: A systematic review and meta-Aanalysis. The Journal of Allergy and Clinical Immunology. In practice, 11(8), 2547–2556. Visit Source.
More, D. (2024). How age affects eczema. Verywell Health. Visit Source.
Mulick, A. R., Henderson, A. D., Prieto-Merino, D., Mansfield, K. E., Matthewman, J., Quint, J. K., Lyons, R. A., Sheikh, A., McAllister, D. A., Nitsch, D., & Langan, S. M. (2022). Novel multimorbidity clusters in people with eczema and asthma: a population-based cluster analysis. Scientific Reports, 12(1), 21866. Visit Source.
National Center for Environmental Health. (n.d.). Asthma surveillance in the United States 2001-2021. Centers for Disease Control and Prevention (CDC). Visit Source.
National Eczema Society. (2023). Skin infections and eczema. National Eczema Society. Visit Source.
National Heart, Lung, and Blood Institute. (2021). 2020 Focused updates to the asthma management guidelines. National Institutes of Health (NIH). Visit Source.
National Institute of Allergy and Infectious Diseases. (2024). Eczema (Atopic dermatitis). National Institutes of Health. Visit Source.
Nemeth, V., Syed, H. A., & Evans, J. (2024). Eczema. In StatPearls. StatPearls Publishing. Visit Source.
Ng, A. E., & Boersma, P. (2023). Diagnosed allergic conditions in adults: United States, 2021. NCHS data brief, (460), 1–8. Visit Source.
Polaskey, M. T., & Chovatiya, R. (2025). Moving beyond biology: The critical role of social and structural determinants in atopic dermatitis. International Journal of Dermatology, 64(2), 272–281. Visit Source.
Pullerits, T., Rönmark, E. P., Ekerljung, L., Palmqvist, M. A., Arvidsson, M., Mincheva, R., Backman, H., Kankaanranta, H., Ilmarinen, P., Rådinger, M., Lundbäck, B., & Nwaru, B. I. (2021). The triad of current asthma, rhinitis and eczema is uncommon among adults: Prevalence, sensitization profiles, and risk factors. Respiratory Medicine, 176, 106250. Visit Source.
Roland, J. (2025). Inhaler spacers: What you need to know. Healthline. Visit Source.
Roland, L. T., Wise, S. K., Wang, H., Zhang, P., Mehta, C., & Levy, J. M. (2021). The cost of rhinitis in the United States: A national insurance claims analysis. International Forum of Allergy & Rhinology, 11(5), 946–948. Visit Source.
Shaw, M. (2023). Eczema prevalence varies by race and ethnicity, with overall increase seen. The American Journal of Managed Care (AJMC). Visit Source.
Sinyor, B., & Concepcion Perez, L. (2023). Pathophysiology of asthma. In StatPearls. StatPearls Publishing. Visit Source.
Singh, P., & Silverberg, J. I. (2023). Outpatient utilization patterns for atopic dermatitis in the United States. Journal of the American Academy of Dermatology, 88(2), 357–363. Visit Source.
Sorgen, C. (2025). Chest x-ray for asthma: Uses and what it can tell. Verywell Health. Visit Source.
StatPearls. (2025). Status asthmaticus. StatPearls Publishing. Visit Source.
U. S. Food and Drug Administration. (FDA). (2024). Food allergies: what you need to know. U. S. Food and Drug Administration (FDA). Visit Source.
Wang, X., Boytsov, N. N., Gorritz, M., Malatestinic, W. N., Goldblum, O. M., & Wade, R. L. (2022). US health care utilization and costs in adult patients with atopic dermatitis by disease severity. Journal of Managed Care & Specialty Pharmacy, 28(1), 69–77. Visit Source.
Watto, M., & Williams, P. (2025). Still recommending albuterol for asthma? Time for an update. Medscape. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.