FL APRN Autonomous Practice Applicant (Differential Diagnosis): Neonatal Jaundice Management
1 Contact Hour
Only FL APRN Autonomous Practice Applicants will receive credit for this course.
Listen to Audio
Get one year unlimited nursing CEUs $39Sign up now
This course is only applicable for Florida nurse practitioners who need to meet the autonomous practice initial licensure requirement.
This peer reviewed course is applicable for the following professions:
Advanced Practice Registered Nurse (APRN)
This course will be updated or discontinued on or before Friday, February 12, 2027
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will know how to assess for and mitigate neonatal jaundice.
Objectives
After completing this continuing education course, the participant will be able to:
Define the physiology of bilirubin production and metabolism.
Differentiate between various types of neonatal hyperbilirubinemia.
Identify the complications of neonatal hyperbilirubinemia.
Describe the methods of clinical assessment for neonatal hyperbilirubinemia.
Determine the management of and treatment for neonatal hyperbilirubinemia.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Jaundice is one of the most common physiological problems affecting children in the newborn period. The causes and management of jaundice in neonates has a different significance and is approached differently than jaundice in older children or adults.
All infants, term or preterm, healthy or ill, change bilirubin metabolism after birth. These normal transitional changes may lead to physiologic jaundice. Some infants exaggerate normal transitional changes or additional health alterations that result in an accumulation of excess bilirubin, or what is known as pathologic jaundice.
Understanding the clinical significance, signs and symptoms, and management of each type of jaundice is important for nurses working in neonatal and pediatric settings.
Unconjugated hyperbilirubinemia (UHB) is very common, occurring in about 60% of term and 80% of preterm newborns in the first two weeks of life. Physiologic jaundice accounts for around 75% of UHB cases and is transient and self-limiting. While much more serious, pathologic jaundice is also much more rare and accounts for only 25% of UHB cases (Ansong-Assoku et al., 2024; Yu et al., 2019).
Fortunately, only about 10% of all jaundiced neonates will require phototherapy, though the frequency of this treatment is skewed greatly based on gestational age. In fact, premature infants are far more likely to require phototherapy than infants born at term.
Risk factors for physiologic jaundice include (Ansong-Assoku et al., 2024; Yu et al., 2019):
Prematurity
Breastfeeding
Low birth weight
Bruising or cephalhematoma acquired during delivery
Risk factors for pathologic jaundice include (Ansong-Assoku et al., 2024; Yu et al., 2019):
Southeast ancestry
East Asian ancestry
ABO incompatibility with the mother
G6PD deficiency
Complications such as acute bilirubin encephalopathy are rare, occurring at a rate of only 1 in 10,000 live births (Ansong-Assoku et al., 2024; Yu et al., 2019).
Conjugated hyperbilirubinemia (CHB) is much more rare than UHB, occurring in only 1 in 2,500 live births. The possible causes of CHB include infection, cholestasis, and biliary atresia (Ansong-Assoku et al., 2024; Yu et al., 2019).
Treatment for neonatal jaundice stands to impose significant costs on individual families as well as the healthcare system, with the mean cost of phototherapy for an individual being about $2,703 (Romero et al., 2018; Xie et al., 2012). Neonatal jaundice is the most common cause of hospital readmission in the first 30 days after birth (Romero et al., 2018; Xie et al., 2012). It is known that hospital management of this condition is estimated to cost around $14,000 per child (Romero et al., 2018; Xie et al., 2012).
Jaundice is a yellowing of the skin that develops because of hyperbilirubinemia, or elevated bilirubin levels in the blood (Ansong-Assoku et al., 2024; Yu et al., 2019).
The primary source of bilirubin in the body is from the breakdown of red blood cells (RBCs) in the liver and spleen (Ansong-Assoku et al., 2024; Yu et al., 2019). After completion of the natural span of the RBC, or with premature destruction, the aging or hemolyzed red blood cell membrane ruptures, releasing phagocytized hemoglobin by macrophages. The hemoglobin molecule then splits into a heme portion and a globulin portion. Bilirubin is derived from the heme portion of hemoglobin (Ansong-Assoku et al., 2024; Yu et al., 2019).
Production of bilirubin begins whenever hemoglobin is broken down (Hansen, 2024). The heme portion is oxidized into a compound called biliverdin by the enzyme heme oxygenase. Another enzyme, biliverdin reductase, then acts on the biliverdin and converts it into unconjugated (indirect) bilirubin (Hansen, 2024). This unconjugated bilirubin is then released into the body’s circulation where it binds with albumin and is transported to the liver (Hansen, 2024).
Unconjugated bilirubin’s ability to bind is affected by plasma pH and medications (Hansen, 2024). Most bilirubin is bound to albumin (Hansen, 2024). Only a small amount of unconjugated bilirubin is free within the plasma. Once it reaches the liver, unconjugated bilirubin unbinds from the albumin and is transported by ligandin or Y carrier proteins into hepatocytes, the active cells of the liver (Hansen, 2024).
Once in the liver, conjugation takes place via the enzyme uridine diphosphoglucconosyl transferase (UDPGT). This enzyme binds the bilirubin to simple sugar, known as glucuronic acid, and forms a compound called monoglucuronide (Hansen, 2024). About two-thirds of this is conjugated further and forms diglucuronide. Together, the monoglucuronide and diglucuronide compounds are then known as conjugated bilirubin (Hansen, 2024). Adequate stores of glucose and access to oxygen is needed for the conjugation process to occur properly (Hansen, 2024).
Carrier proteins then transport the conjugated bilirubin into the biliary tree, or the biliary system of ducts that move bile from the liver to the small intestines (Hansen, 2024). Here, the conjugated bilirubin mixes with bile and moves into the small intestines. In the gastrointestinal tract, normal flora breaks bilirubin down into urobilinogen and stercobilinogen which are excreted mostly through the stool. The typical yellow-brown color of stool comes from the compound stercobilinogen (Hansen, 2024). There is a small amount of urobilinogen that is reabsorbed from the colon back into the circulation and then excreted through the urine, though this is not the primary method of excretion (Hansen, 2024).
Image 1: Bilirubin Metabolism
Some conjugated bilirubin may also be deconjugated through hydrolyzation in the intestines and then is reabsorbed back into the enterohepatic circulation and conjugated for a second time in the liver (Hansen, 2024).
Now, understanding the metabolism of bilirubin, it is clear that there are 2 main types of hyperbilirubinemia, unconjugated and conjugated (also called indirect or direct). Each has different causes, significance, and treatment implications. Let’s go over those now.
Unconjugated hyperbilirubinemia (UHB) is the most common type of jaundice (Ansong-Assoku et al., 2024; Yu et al., 2019). UHB generally occurs when hemoglobin is being broken down faster than the body can keep up with conjugating the bilirubin byproduct. There are 3 main etiologies for elevated levels of unconjugated bilirubin in neonates:
There are many reasons a neonate may have an increased production of bilirubin as they adjust to extrauterine life. Even healthy, term newborns often have an increased red blood cell (RBC) load at birth as well as an immature RBC lifespan, resulting in an increased rate of hemolysis while the infant adjusts and regulates RBC production and concentration (Ansong-Assoku et al., 2024).
Delayed cord clamping is popular and has many benefits but may also increase the risk of jaundice as the excess RBCs are broken down.
Other causes of increased RBC transfer to the neonates before or shortly after birth include (Ansong-Assoku et al., 2024):
Intrauterine growth restriction (IUGR)
Large for gestational age (LGA)
Diabetic mother
Smoking in the mother
Living at high altitude
Twin to twin transfusion
Any bleeding or trauma during birth, such as cephalohematoma or intracranial hemorrhage also increases RBC destruction and contributes to hyperbilirubinemia (Ansong-Assoku et al., 2024).
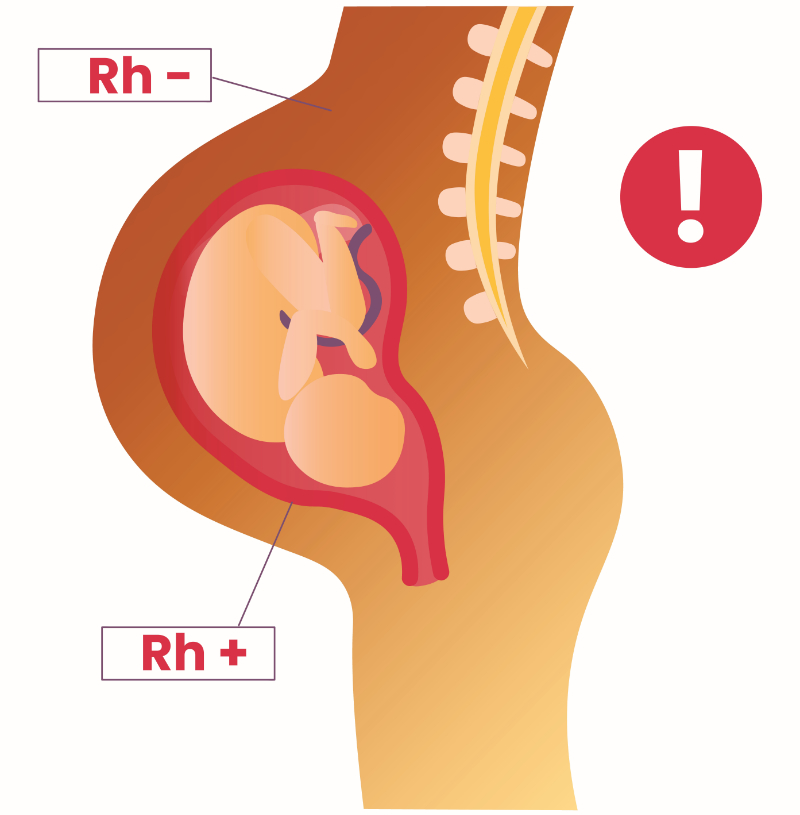
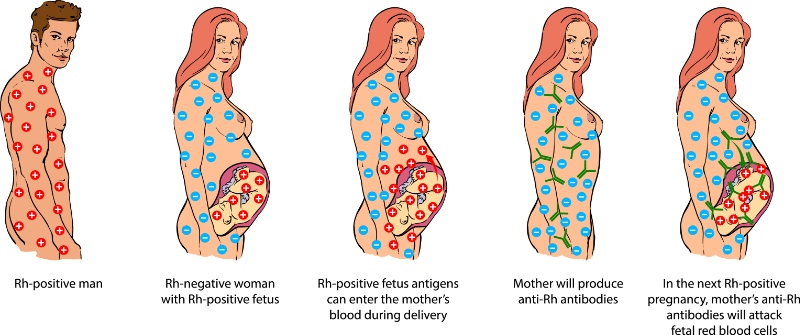
Immune-mediated hemolysis can occur in response to blood group incompatibilities like ABO and Rh issues. ABO incompatibility occurs when the mother and baby have different blood types and the mother’s body produces antibodies that attack the newborn’s RBCs (Ansong-Assoku et al., 2024). This most commonly occurs in mothers with type O blood, as they have antibodies for both A and B blood antigens (Ansong-Assoku et al., 2024). ABO incompatibility occurs in around 15% of pregnancies but only results in hemolysis approximately 4% of the time (Ansong-Assoku et al., 2024). Similarly, mothers with Rh-negative blood exposed to Rh-positive blood during pregnancy develop antibodies against the Rh antigen.
Image 2: Rh Factor
The IgM antibodies formed during the initial pregnancy exposure cannot cross the placenta and are, therefore, not a threat to the current pregnancy, however, eventually IgG antibodies develop and may cross the placenta to cause hemolysis in subsequent pregnancies (Ansong-Assoku et al., 2024).
Image 3: Rh Incompatibility
This serious immune response can be mediated, as explained and recommended by the American College of Obstetricians and Gynecologists (ACOG), with the administration of anti-D immune globulin injection for Rh-positive or unknown blood type mothers at 28 weeks gestation (Ansong-Assoku et al., 2024).
A Coombs test, a routine part of prenatal care, is a serum lab that checks a mother’s blood for signs of antibodies that could cause hemolysis in the neonate (Ansong-Assoku et al., 2024). Awareness of a mother’s blood type, Rh factor, and Coombs test result are an important part of caring for the neonate, particularly those exhibiting jaundice (Ansong-Assoku et al., 2024).
Additional causes of RBC destruction and, therefore, increased bilirubin production include enzyme defects, sepsis, and defects in the RBC membrane (Ansong-Assoku et al., 2024).
The most common RBC enzyme defect is a hereditary, X-linked condition called glucose-6 phosphatase dehydrogenase (G6PD) deficiency (Ansong-Assoku et al., 2024). Under normal conditions, the G6PD enzyme protects RBCs against oxidative damage when exposed to stressors like illness, certain medications, and certain foods. For people with a G6PD deficiency, that protection is no longer there, and hemolysis occurs under those stressors, resulting in anemia and hyperbilirubinemia (Ansong-Assoku et al., 2024).
Another condition, pyruvate kinase deficiency (PKD), is an autosomal recessive disorder that interferes with glycolysis and production of cellular energy, frequently causing hemolysis and anemia (Ansong-Assoku et al., 2024). There are also conditions like hereditary spherocytosis and elliptocytosis, which involve structural protein mutations that lead to irregularly shaped RBCs and increased hemolysis (Ansong-Assoku et al., 2024).
These conditions are not routinely tested for on newborn screenings, however, they should be considered for further evaluation in infants with a family history of a hereditary disorder and for those with severe hyperbilirubinemia, especially when phototherapy is not proving effective (Ansong-Assoku et al., 2024).
Whether in the presence of typical or excessive destruction of RBCs, the neonate’s ability to clear bilirubin from the body also impacts severity and duration of hyperbilirubinemia (Ansong-Assoku et al., 2024).
The most common reason for decreased bilirubin clearance is a defect in the UDPGT enzyme that conjugates bilirubin. Genetic conditions like Gilbert syndrome and Crigler-Najjar syndrome cause a decrease and absence in UDPGT activity respectively. Presentation of jaundice due to Gilbert syndrome is typically rare in the newborn period, however Crigler-Najjar syndrome will usually present as severe hyperbilirubinemia, including encephalopathy, within a few days of life (Ansong-Assoku et al., 2024).
There are some additional conditions that can lead to UHB without immune-mediated or genetic causes. Certain medications like ceftriaxone, penicillins, and sulfa medications may increase bilirubin levels by displacing albumin binding sites and making conjugation more difficult or through strain on the immature liver which then struggles to metabolize both the medication and the excess bilirubin (Ansong-Assoku et al., 2024).
Remember that bilirubin is excreted through the stool, so any condition that reduces intestinal motility may also increase bilirubin levels (Ansong-Assoku et al., 2024). This could include intestinal obstruction, pyloric stenosis, or suboptimal intake for breastfed infants. In fact, “breastfeeding jaundice” is very common as neonates and mothers adjust to the on-demand relationship of breastfeeding and supply regulation. For mothers with an inadequate supply or infants who are struggling to properly latch, poor intake may lead to mild dehydration and decreased intestinal motility and stooling. Breast milk jaundice is likely to present later in the first week of life and peak during the 2nd week, though it may persist for longer (Ansong-Assoku et al., 2024). For infants with adequate intake and good weight gain, close monitoring is often all that is needed. Further assessment and management of the breastfeeding relationship is beyond the scope of this course but should be heavily considered in management of hyperbilirubinemia in the breastfeeding newborn and help of an international board-certified lactation consultant (IBCLC) or similarly trained lactation professional should be sought whenever available (Ansong-Assoku et al., 2024).
Other miscellaneous causes may include mothers with diabetes, as these infants often have polycythemia, and congenital hypothyroidism which is associated with decreased gut motility, decreased hepatic uptake of bilirubin, and impaired enzyme activity (Ansong-Assoku et al., 2024).
Often, newborns with UHB will have a combination of factors that increase their risk of hyperbilirubinemia, such as prematurity, familial history of jaundice, exclusive breastfeeding, and Asian ethnicity (Ansong-Assoku et al., 2024).
Depending on the underlying etiology, cases of UHB may then be divided into physiologic or pathologic in nature. The distinction is important as it guides management decisions and the risk of complications.
The majority of neonatal jaundice cases are physiologic UHB, usually appearing after the first 24 hours of life and peaking around 48-96 hours of life (Ansong-Assoku, et al., 2024). Physiologic jaundice tends to be caused by uncomplicated extrauterine adjustment processes like high levels of RBCs, shortened RBC lifespan, and liver immaturity and typically resolves by 2-3 weeks of age (Ansong-Assoku et al., 2024). Management is often straightforward and effective.
Pathologic UHB occurs much more rarely, often presents within the first 24 hours of life, and increases rapidly (Ansong-Assoku et al., 2024). There is typically an underlying condition or process beyond normal adjustment to extrauterine life that needs to be identified such as blood type incompatibility, hemolytic disease, or infection. Pathologic jaundice requires more aggressive treatment of the underlying cause and may persist or worsen for several weeks (Ansong-Assoku et al., 2024).
In contrast to UHB, neonates may also experience conjugated hyperbilirubinemia (CHB), though this is much more rare. This elevated bilirubin level occurs late in the process of bilirubin metabolism and excretion, when the bilirubin has been conjugated in the liver by the UDP glucuronosyltransferase (UDPGT) enzyme. After conjugation, it is typically taken into the biliary tree to mix with bile and enter the intestines for further processing and excretion. Dysfunction of the hepatobiliary system at this step leads to decreased excretion and rising conjugated bilirubin levels. CHB is nearly always pathologic and requires swift evaluation and treatment. The common causes of CHB, which will be discussed in more detail below, include (Ansong-Assoku et al., 2024; Ashraf & Piper, 2021).
Congenital infections such as syphilis, toxoplasmosis, HIV, herpes simplex virus (HSV), cytomegalovirus (CMV), and rubella all must be considered in the presence of CHB, even if neonates are asymptomatic (Ansong-Assoku et al., 2024). Assessment should include maternal history, urine and blood cultures, and serologic and viral testing. The severity of these infections may cause injury to the cells of the liver or may even release toxins that further damage hepatocytes, interrupting the normal hepatobiliary function for excretion of conjugated bilirubin (Ansong-Assoku et al., 2024).
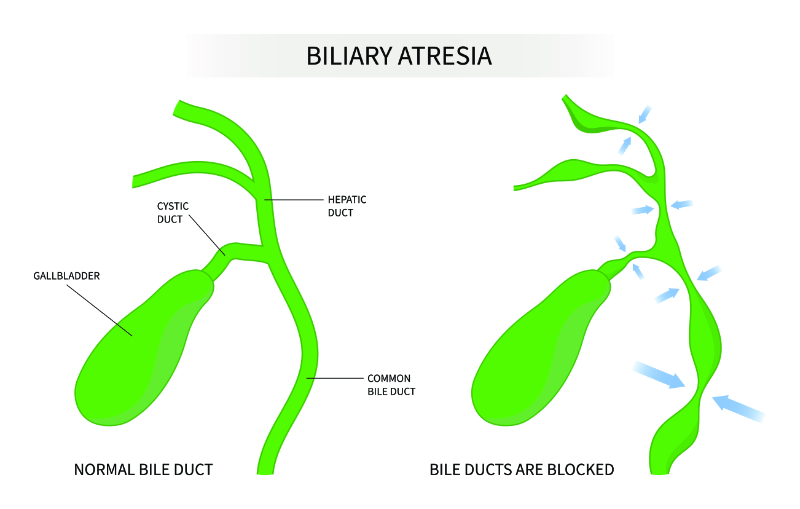
Structural changes of damage to the hepatobiliary system may also lead to CHB. Such conditions include biliary atresia, neonatal sclerosing cholangitis, choledochal cysts, and cholelithiasis (Ansong-Assoku, et al., 2024; Ashraf & Piper, 2021).
Image 4: Biliary Atresia
Biliary atresia is among the most common of these conditions, but is still fairly rare, occurring about once in every 12,000 births in the United States (Ansong-Assoku et al., 2024).
There are many genetic conditions which may impact hepatobiliary function and lead to CHB in the neonatal period. The most common of these is Alagille syndrome (ALGS), which is an autosomal dominant disorder that causes a lack of interlobular bile ducts (Ansong-Assoku et al., 2024). These infants may have other clues that this disorder has occurred, including congenital heart defects, poor kidney function, dysmorphic features (broad forehead and small chin), and vertebral abnormalities (Ansong-Assoku et al., 2024).
Cystic fibrosis (CF) is another genetic condition that may cause abnormal function of the bile ducts. CF is characterized by thick mucus buildup in the body and neonatal cholestasis from clogged bile ducts may be one of the first symptoms that eventually lead to a diagnosis of CF (Ansong-Assoku et al., 2024).
Alpha-1-antitrypsin deficiency is another common cause of cholestasis in infancy. Cells called anti-trypsin polymers accumulate in the liver and cause damage and death to hepatocytes, eventually leading to cholestasis and cirrhosis in later childhood (Ansong-Assoku et al., 2024).
Inborn errors of metabolism such as galactosemia, fructosemia, and tyrosinemia may also cause neonatal cholestasis. Galactose-1-phosphate uridyl transferase (GALT) deficiency, specifically, leads to accumulation of galactose metabolites in various organs, which are toxic and damaging to the cells (Ansong-Assoku, et al., 2024).
Another genetic mutation, progressive familial intrahepatic cholestasis (PFIC) includes 3 genetic disorders, with types 1 and 2 presenting in the neonatal period and progressing to cirrhosis and end-stage liver disease by childhood (Ansong-Assoku, et al., 2024).
There are many other genetic conditions that can lead to liver damage, among other symptoms, and may present as CHB during the neonatal period. Thorough family history and consultation with a genetic specialist may be necessary when liver damage and dysfunction without apparent cause presents in the newborn period.
Conditions not categorized with any of the above are considered miscellaneous and may include idiopathic neonatal hepatitis, parenteral nutrition-induced cholestasis, neonatal hemochromatosis, hypotension, and gestational alloimmune liver disease. Other conditions like sepsis and necrotizing enterocolitis (NEC) all have the potential for liver injury as well (Ansong-Assoku et al., 2024).
Gestational alloimmune liver disease (GALD) is a condition where maternal antibodies attack fetal hepatocytes and lead to liver failure (Ansong-Assoku, et al., 2024).
Parenteral nutrition-associated cholestasis (PNAC) is of significant concern for preterm infants receiving parenteral nutrition in the neonatal intensive care unit (NICU). Premature intestines, biliary function, and longer duration of parenteral nutrition all increase the risk of this condition, though the complete mechanism of this condition is not fully understood.
Initially, bilirubin is transported in the blood plasma bound to albumin at two sites (Wong & Bhutani, 2024a):
A primary binding site that has a strong bond, and
A secondary site that has a weak bond
When available albumin-binding sites are saturated, bilirubin then circulates freely in the plasma. This portion of unconjugated bilirubin can cross the blood brain barrier and migrate into brain cells, causing damage known as kernicterus. Kernicterus is a major complication of neonatal hyperbilirubinemia in which there is the presence of yellow pigment in the brain (basal ganglia) (Wong & Bhutani, 2024a). Kernicterus may result in encephalopathy and permanent brain damage of the basal ganglia.
Unconjugated bilirubin has toxic effects on the brain and the central nervous system (CNS). The term “kernicterus” was originally used to describe the appearance of the brain on autopsy when an infant had died from jaundice. The modern term, “bilirubin encephalopathy” is actually a more appropriate phrase for the clinical effects of bilirubin on the CNS (Wong & Bhutani, 2024a).
The occurrence of kernicterus is related to the amount of diffusible, loosely bound bilirubin and albumin binding sites available. Free bilirubin easily crosses the blood-brain barrier and is transferred into the brain cells, causing obvious yellow staining of the brain tissue, similar to its effect on the skin (Wong & Bhutani, 2024a). The brain's areas usually affected by the staining are the hypothalamus, dentate nucleus, and the cerebellum. Kernicterus is associated with varying degrees of neurological damage, but a direct correlation between serum bilirubin levels and the severity of involvement cannot be drawn (Wong & Bhutani, 2024a).
The incidence of severe hyperbilirubinemia in full-term infants has reduced drastically in the last few decades, thanks to routine screening and preventative treatment for Rh-negative mothers, as well as the availability of phototherapy and exchange transfusions (Wong & Bhutani, 2024a).
Early discharge has contributed to increased incidences of kernicterus. The American Academy of Pediatrics (AAP) has recommended guidelines for the management of all infants. The AAP recommends that a healthcare professional evaluate all infants discharged prior to 48 hours of age within 48 hours after discharge (Kemper et al., 2022). The education of healthcare professionals regarding kernicterus has become a priority for the AAP (Kemper et al., 2022).
Many factors can influence the bilirubin-binding capacity and increase the risk of kernicterus at lower bilirubin levels. Some of those factors include (Kemper et al., 2022):
The total amount of available serum albumin
The presence of other substances competing for available binding sites
Acidosis and hypoxia
Premature infants normally experience relative hypoproteinemia and have fewer albumin-binding sites available for free bilirubin (Kemper et al., 2022). Certain drugs, such as sulfisoxazole and salicylates, compete with bilirubin for binding sites or replace bilirubin loosely attached to binding sites. Acidosis and hypoxia increase hydrogen ions' production, and implementation of anaerobic metabolism can impede bilirubin binding. Albumin's ability to bind bilirubin drops to one-half of its potential at a serum pH of 7.1, with free fatty acids produced during anaerobic metabolism competing for albumin-binding sites (Kemper et al., 2022). When acidosis and hypoxia, which can open the blood-brain barrier, are concurrently present in a sick infant, said infant could be exposed to kernicterus at much lower serum levels. Evidence suggests that subsequent CNS abnormalities are better correlated with tests evaluating bilirubin-binding capacity than serum bilirubin concentrations (Kemper et al., 2022).
Clinical Manifestations of kernicterus are as follows (Kemper et al, 2022):
Early Signs
Middle Signs
Late Signs
Difficulty feeding/sucking
High-pitched cry
Abnormal eye movements
Irritability
Muscle spasticity
Not feeding
Hypotonia
Arched back/heels
Fever
No startle reflex
Severe jaundice to skin and sclera
Seizures
Lethargy
Serum bilirubin levels are 30 mg/dL or greater (in term infants)
In the full-term infant, jaundice becomes apparent within two to four days after birth and lasts until the sixth day, reaching a peak concentration of 6 to 7 mg/dL (Bhandari, 2024). The newborn produces up to 8.5 to 10 mg/kg/day of bilirubin, and production is inversely correlated to gestational age (Bhandari, 2024).
The preterm infant has cord blood levels similar to those of the term infant, but peak levels are higher, jaundice lasts longer, and levels peak later at five to seven days (Bhandari, 2024). In fact, 63% of preterm infants achieve 10 to 19 mg/dL levels, and 22% will reach levels greater than 15 mg/dL (Bhandari, 2024).
Clinicians have been observing jaundice and gauging its severity before we even had a good understanding of what bilirubin was. Jaundice can be observed with the naked eye, especially in bright or natural light. Pressing down lightly with a finger on an infant’s check, nose, or cheek and observing the presence or absence of yellow discoloration with blanching is an easy and noninvasive technique that can be used by anyone. Hyperbilirubinemia over 5 mg/dL can create visible staining of the skin and sclera, and blanching is not needed (Bhandari, 2024). A simple visual estimate, paired with knowledge of jaundice’s cephalocaudal progression (progression of yellow coloring moving from head-to-toe), can be used to help judge the need for a serum bilirubin test and more specific assessment (Bhandari, 2024).
The head-to-toe progression of jaundice over the body gives a crude estimate of bilirubin level. The neonate’s body can roughly be divided into dermal zones. Zone 1, from the head to clavicle, indicates a serum bilirubin level of approximately 5 mg/dL. Zone 2, the clavicle to umbilicus, is approximately 6-8 mg/dL. Jaundice that reaches zone 3, which spans from the umbilicus to the knees, is approximately 9-12 mg/dL. The knees to the ankles is considered zone 4 and indicates a serum bilirubin level of approximately 13-15 mg/dL. And finally, zone 5 is when the palms and soles are affected by visible jaundice and indicates an approximate bilirubin level of over 15 mg/dL.
There are also reference devices available, including the Ingram Icterometer which has been around since the 1960s and includes a color reference chart for indicated severity of jaundice.
For infants whose visible jaundice level is determined to need further evaluation, a serum bilirubin level should be obtained using either venous, arterial, or capillary blood. A transcutaneous bilirubin (TcB) machine may also be used to offer a more accurate, but noninvasive, quantification of jaundice level. It is important to know your own unit’s policy for what methodology is preferred as some NICUs utilize both a TcB to measure, and then a serum blood sample to confirm.
Regardless of the method used to estimate or obtain a serum bilirubin level, whether the level of jaundice needs treatment or not is generally calculated based on the amount of bilirubin and the infant's age in hours or days, accounting for prematurity if applicable.
Standardized graphs or tools can help the clinician calculate the infant's risk. Once such tool is that of the BiliTool™, which has been around for over 15 years and is recommended by the Centers for Disease Control and Prevention (CDC) (Burgos & Turner, 2022). This tool assists the clinician by asking for a birth date and time, the bilirubin sample collection date and time, what the total bilirubin sample level is, the gestational age of the infant, and the opportunity to check-off from a few different clinical situations that would increase the risk of that child, such as hemolytic disease, G6PD deficiency, or a clinical suspicion of sepsis (Burgos & Turner, 2022). After inputting this information, what results is a summary with the input data, a section of recommendations if the level should be confirmed with a TcB or if phototherapy would be beneficial at this stage, or even if an exchange transfusion is necessary (Burgos & Turner, 2022). It even includes a graph that graphs the pinpoint of the current level that was input and shows the physical threshold levels in which an escalation of care such as initiating phototherapy would be advisable (Burgos & Turner, 2022). Take a look at this resource yourself here.
Once hyperbilirubinemia is confirmed, the AAP's new guidelines provide streamlined guidance for further workup and when and how to initiate treatment (Kemper et al., 2022).
The first step in the workup process is determining whether the jaundice is pathologic or not because these are the cases with a higher risk and urgency of diagnosis and treatment of underlying cause (Kemper et al., 2022). The majority of neonatal jaundice is not pathologic, as we have discussed, however the difference in severity and management is significant enough that the distinction requires vigilance. Jaundice visible in the first 24 hours of life is a red flag for pathologic jaundice (Kemper et al., 2022).
The AAP guidelines begin with a careful review of clinical and family history, as well as physical findings (Kemper et al., 2022). The following are signs and symptoms of potential differential diagnoses for different clinical causes of jaundice.
Differential Diagnosis: Hemolytic disease(Kemper et al., 2022):
Relatives with hemolytic disease
Onset of jaundice prior to 24 hours of lifeSerum bilirubin level increases of more than 0.5 mg/dL/hr
Pallor
Enlargement of the liver or spleen
Poor response to phototherapy
Rapid increase in the total serum bilirubin level after 24-48 hours (G6PD deficiency)
Ethnic background at risk for hereditary disease
Differential Diagnosis: Cholestatic jaundice(Kemper et al., 2022):
Urine positive for bilirubin
Dark urine
Light/clay-colored stool
Persistent jaundice lasting longer than 3 weeks
Differential Diagnosis: Increased RBC breakdown, other than hemolysis(Kemper et al., 2022):
Hematocrit > 65 (polycythemia)
Cephalohematoma
Ecchymosis
Infant of a Diabetic Mother (IDM)
Less than 37 weeks gestational age
Differential Diagnosis: Sepsis or Galactosemia(Kemper et al., 2022):
The AAP guidelines recommend laboratory assessment to include (Kemper et al., 2022):
Hemoglobin/hematocrit and RBC count
Maternal/infant blood types
Direct Coombs
Indirect Coombs
Total and direct bilirubin
Serology and viral testing, if congenital infection is suspected
Pathologic jaundice is characterized by jaundice at less than 24 hours of age, a rapidly rising bilirubin level (greater than 0.5 mg/dL/hr), or true hemolysis (Bhandari, 2024).
A total serum bilirubin level should be collected on any infant demonstrating visible jaundice during the first 24 hours of life (Bhandari, 2024). For levels greater than 7-8 mg/dL during that time frame, further workup, close observation, and possible initiation of treatment are needed (Bhandari, 2024). Lower levels found very early on (such as 8 hours of life) may still warrant a workup (Bhandari, 2024).
Further evaluation should include (Ansong-Assoku et al., 2024; Kemper et al., 2022):
Maternal ABO and Rh typing
Maternal serum screen for antibodies (if not already done)
Cord blood type
Direct Coombs
CBC with differential, retic count, and blood smear
Repeated serum bilirubin levels 4-6 hours
Additional tests as needed depending on clinical findings and condition of the neonate
Treatment is largely dependent on the type and underlying cause of jaundice as well as the severity of the bilirubin level relative to an infant’s age. For UHB, treatment can range from outpatient management and monitoring to more intensive inpatient monitoring and intervention.
For full term, healthy neonates over 24 hours of age and determined to be exhibiting non-pathologic jaundice, management can safely take place in the outpatient setting (Wong & Bhutani, 2024b). Even those requiring phototherapy can receive the treatment at home, via widely available fiber optic phototherapy blankets.
In order to qualify for at-home phototherapy, infants should be feeding well, appear well, and have a serum bilirubin level of less than 20-22 mg/dL (<18mg/dL for preterm infants) (Kemper et al., 2022). Home health nurses may be used to provide close and frequent assessments and monitor progress. Interventions from home health nurses can include (Kemper et al., 2022):
Unconjugated bilirubin is insoluble in water but very lipid soluble. Conjugation in the liver makes bilirubin more water-soluble and then allows it to be excreted from the body through stool (Woodgate & Jardine, 2015). Phototherapy uses blue-green light waves to alter bilirubin molecules and make them water-soluble and ready for excretion without needing to be conjugated in the hepatic system. Phototherapy may be used in both an outpatient and inpatient setting depending on resources available to an area, compliance and comfort level of the family, and clinical severity of the hyperbilirubinemia (Woodgate & Jardine, 2015).
Phototherapy is also thought to enhance the hepatic excretion of unconjugated bilirubin and increase bowel transit time (Woodgate & Jardine, 2015). With early phototherapy initiation, a 20% to 35% reduction in serum bilirubin concentrations is noted by the second day of life, with a 41% to 55% reduction by day four (Woodgate & Jardine, 2015). This reduction is more significant than the naturally occurring drop in the untreated infant (Woodgate & Jardine, 2015).
Irradiance is measured in microwatts per centimeter squared per nanometer (µW/cm2/nm). Irradiance and not the intensity of the light source are critical in successful management.
Blue light that is 450 nm is best absorbed, but the light of longer wavelengths, such as green light, is thought to penetrate infant skin more deeply (Ashraf & Piper, 2021). In addition to the appropriate wavelength, effective illumination must also be maintained. Spectroradiometer readings of 4 to 6 µW/cm2/nm are considered to be in the effective therapeutic range (Ashraf & Piper, 2021). Phototherapy units should be checked for adequate light levels with a radiometer before phototherapy is initiated and every eight to twelve hours while the lights are in use. The optimal distance between the light source and the infant is less than twenty inches (Ashraf & Piper, 2021).
Phototherapy in a term, healthy infant should continue until the bilirubin level is 25-50 µmol/L (1.5-3 mg/dL) below the initial level that indicated the initiation of treatment (Ashraf & Piper, 2021). Levels may rebound once phototherapy has been discontinued, therefore repeat bilirubin levels should be collected within 6-12 hours after stopping phototherapy (Ashraf & Piper, 2021). Rebound levels up to 1 mg/dL is regarded as normal.
For preterm infants who are ages 5 or more days, phototherapy can be discontinued when the bilirubin level is 12 mg/dL or less. For preterm infants who are less than 5 days old, therapy can be discontinued when the bilirubin level is below 10 mg/dL. Hospitalization for phototherapy and close monitoring is indicated for any infant not responding to at-home phototherapy.
Fiberoptic phototherapy may be available in some facilities and have some advantages over conventional overhead phototherapy. Advantages of fiberoptic phototherapy include:
Minimal risk of overheating
Eye shields not needed
Ability to deliver phototherapy with the infant in a bassinet next to the mother's bed
Easy to use at home
Able to be used in addition to conventional phototherapy for greater surface areas exposed, to work to lower bilirubin level quicker
Because the effects of prolonged exposure to phototherapy lights can potentially cause retinal damage, infants undergoing phototherapy do require eye protection. Phototherapy units and eye protection should be periodically removed throughout the day to provide the infant with visual stimulation and interaction with parents and caregivers, as well as to give the skin a break from any pressure of the means of eye protection to prevent any potential skin breakdown.
Image 5: Eye Protection for Phototherapy
Also of note in the above image is the covering of the infant’s genitalia. While maximum skin exposure is required, both the infant’s eyes and genitalia should be covered in order to protect them from the phototherapy light source.
When starting phototherapy, it is important to note that any interruptions should be minimized (Wong & Bhutani, 2024b). For infants with a total serum bilirubin level below 20 mg/dL, depending on unit policy and provider’s orders, phototherapy can potentially be interrupted occasionally for breastfeeding, bottle feeding, or parent/caregiver holding, typically for up to 20-30 minutes at a time (Wong & Bhutani, 2024b). For infants with total serum bilirubin levels above or equal to 20 mg/dL, phototherapy should be continuous, without interruption for holding or feeding (Wong & Bhutani, 2024b). An infant can be fed via bottle while still undergoing phototherapy. Continuous phototherapy still requires periodic discontinuation for a couple of minutes while eye protection is adjusted, and diaper changes need to take place.
Infants undergoing phototherapy require temperature stabilization appropriate for their size and overall condition. Adequate fluid intake and compensatory fluid adjustment for increased insensible water loss may be required to prevent dehydration in these infants. The infant under phototherapy will need periodic monitoring of bilirubin levels to check for therapy effectiveness. It is important to note that because phototherapy lights can alter blood bilirubin results, the lights should be turned off during blood drawing for accurate serum bilirubin determinations.
In general, phototherapy has no significant toxicity. The side effects of phototherapy are few and are reversible with the removal of the lights. These side effects can include (Stanford Medicine, 2025; Wong & Bhutani, 2024b):
For infants suspected of exhibiting pathologic jaundice, close hospital management with neonatology is indicated. Extensive workup will be needed as well and is easier to coordinate and adjust in an inpatient setting.
Among workup labs for pathologic jaundice, as we have discussed, is a hematocrit (HCT) level. Low or falling HCT levels indicate the presence of hemolysis, likely due to ABO incompatibility, which indicates a need for blood smear (Hanson, 2024). Serum bilirubin should be repeated every 4-6 hours until dropping measurably, 1 mg/dL or more (Hanson, 2024).
Presence of hemolytic disease or labs that indicate ABO incompatibility require aggressive treatment to prevent bilirubin levels from rising to dangerous levels (Hanson, 2024). However, phototherapy is often less effective for hyperbilirubinemia that is due to hemolytic disease. Exchange transfusions may be indicated for these infants if bilirubin levels reach 18-23 mg/dL for full term infants or 15-18 mg/dL for preterm infants (Hanson, 2024).
If bilirubin levels start to approach those associated with kernicterus despite phototherapy, exchange transfusion may be necessary to protect the jaundiced infant's CNS status (Wong & Bhutani, 2024b). Also, it is the intervention that is recommended for a rapidly rising bilirubin within the first 24 hours of life. This procedure aims to remove bilirubin and the antibody-coated RBCs from the newborn's circulation (Wong & Bhutani, 2024b).
After a single-volume exchange, 75% of the newborn's RBC mass is removed (Wong & Bhutani, 2024b). A double-volume exchange removes 85% to 90% of the cells.
Bilirubin removal is much less effective, with only 25% of the infant's total body bilirubin removed during a double-volume exchange (Wong & Bhutani, 2024b). This is likely the case because the major portion of bilirubin is in the extravascular compartment, an area not affected or touched by the exchange of blood volume (Wong & Bhutani, 2024b).
Rebound in bilirubin levels occurs within one hour of the exchange, and they reach as much as 55% of the pre-exchange values. The following criteria are used to determine the need and timing of exchange transfusion, particularly for infants with erythroblastosis fetalis (Wong & Bhutani, 2024b):
Cord blood indirect bilirubin level of more than 4 mg/dL
Hemoglobin of less than 8 g/dL and a bilirubin level of more than 6 mg/dL within one hour of delivery in a term infant
Hemoglobin of less than 11.5 g/dL and a bilirubin level of more than 3.5 mg/dL within one hour of delivery in a preterm infant
Increase in bilirubin level of more than 20 mg/dL by 24 to 48 hours in an uncompromised term infant and 17 to 18 mg/dL in the high-risk term newborn infant
Bilirubin level of more than 15 mg/dL in the stable preterm infant and of 10 to 12 mg/dL if hypoxia and acidosis are present
Selection and preparation of blood products aim to decrease the antigen-antibody reaction, remove toxic substances, substitute a higher, more efficient circulating RBC, and prevent biochemical imbalances caused by blood products during the exchange transfusion. Blood should be as fresh as possible, preferably less than 48 hours old.
Treatment for CHB is specific to the underlying etiology of the elevated bilirubin level. Surgical repair of biliary atresia is necessary within the first 2 months of life. Infections and sepsis must be treated with antimicrobial agents and supportive care for immature organ systems. Severe cholestasis and hepatic damage may require liver transplantation. IVIG treatments for auto-immune hepatic damage may be used. And parental nutrition should be reduced and discontinued as soon as possible.
Overall, treatment of CHB is very individualized to each specific patient’s case, presentation, and needs.
With prompt identification and treatment, UHB is extremely treatable, and prognosis is excellent. Although repeated assessments and blood draws and interruptions and additional stress over the breastfeeding relationship during treatment of UHB may be stressful for families during the first weeks of an infant’s life, the overall prognosis with appropriate monitoring and treatment is good (Ansong-Assoku et al., 2024).
The most significant risk for infant’s with UHB is the development of kernicterus and encephalopathy (Ansong-Assoku et al., 2024). Poor access to healthcare resources either due to being under or uninsured or geographic constraints on available facilities significantly increases the risk of poor outcomes. Diligent protocols about discharge criteria and follow up within 48 hours of discharge aim to keep newborns under close observation and provide many opportunities to educate parents about warning signs and red flags (Ansong-Assoku, et al., 2024).
Outcomes for infants with CHB will, of course, as had been mentioned, vary by underlying etiology. Multidisciplinary management is typically needed, and the treatment intensity and duration will vary. Early identification and sophistication of modern medicine does mean that even the most complex of cases has better outcome potential than in the past (Ansong-Assoku et al., 2024).
A 3-day old female infant, Lenora, is brought to the pediatrician for a routine weight and wellness check after being discharged from the hospital 36 hours prior. The infant was born via spontaneous vaginal delivery at 39 weeks and 4 days gestation with an uncomplicated pregnancy.
At birth, Lenora’s weight was 3,200 grams and today’s weight is 2,950, a 7.8% loss.
Lenora is exclusively breastfed and her mother states that she has been latching well every 2-3 hours with 5 wet diapers and 2 bowel movements in the last 24 hours.
Lenora’s parents note some yellow discoloration across the infant’s nose, forehead, and upper chest and want to know if this is concerning. The infant is alert and active during the visit.
Based on the history and relatively low risk of hyperbilirubinemia for this infant, as well as the extent of the visible jaundice, a transcutaneous bilirubin check is performed in the office. The result was a value of 10.5 mg/dL.
A confirmation serum bilirubin level was gathered as well, with a total bilirubin level of 11.0 mg/dL. This result is plotted below the low-intermediate risk zone on the Bhutani Nomogram chart. The plotted result on the chart and the infant’s presentation is consistent with physiologic jaundice.
This case is considered mild and within the expected range for physiologic jaundice. Without any concerning signs of pathologic jaundice, reassurance is provided, and the parents are encouraged to continue with breastfeeding on demand and follow up in 2 days to reassess weight and bilirubin levels.
Phototherapy or further intervention is not indicated at this time, but the provider does include information about signs of worsening jaundice or symptoms that warrant immediate intervention.
The prompt evaluation of this infant after discharge helps ensure she is being closely monitored, and that jaundice can be identified early on so that intervention could be started if necessary. Reassurance and education for the parents also ensures that appropriate care is being given at home to prevent worsening of symptoms.
Uneventful pregnancy is listed, however, a review of the mother’s labs to verify Coomb’s test results would help support the diagnosis of physiologic jaundice and low risk of complications.
Additionally, this infant’s number of wet diapers per day (5) is a little less than expected and may indicate suboptimal feeding which could lead to reduced stooling and rapidly progressing bilirubin levels. Observing a feeding in the office to ensure proper positioning and latch, perhaps even weighing after the feed, would help ensure the infant is transferring enough milk to begin gaining weight and promote hydration and stooling to help with bilirubin excretion.
Jaundice is one of the most common problems seen in newborns. All infants need to be assessed for risk factors that may make an infant likely to develop pathologic jaundice. Parents must be educated on the significance of early identification and treatment to prevent the serious complication of kernicterus.
A solid foundation of knowledge for how to identify and manage neonatal hyperbilirubinemia is necessary for any nurse working in a maternal-newborn or pediatric setting. Timely identification and care of these patients will lead to optimum outcomes and prevention of complications.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Ansong-Assoku, B., Shah, S. D., & Adnan, M. (2024). Neonatal jaundice. In StatPearls. StatPearls Publishing. Visit Source.
Ashraf, H. R., & Piper, M. H. (2021). Conjugated hyperbilirubinemia. Medscape. Visit Source.
Burgos, T., & Turner, S. (2022). BiliTool. BiliTool, Inc. Visit Source.
Bhandari, V. (2024). Neonatal jaundice. BMJ Best Practice. Visit Source.
Hansen, T. W. R. (2024). Neonatal jaundice. Medscape. Visit Source.
Kemper, A. R., Newman, T. B., Slaughter, J. L., Maisels, M. J., Watchko, J. F., Downs, S. M., Grout, R. W., Bundy, D. G., Stark, A. R., Bogen, D. L., Holmes, A. V., Feldman-Winter, L. B., Bhutani, V. K., Brown, S. R., Maradiaga Panayotti, G. M., Okechukwu, K., Rappo, P. D., & Russell, T. L. (2022). Clinical practice guideline revision: Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics, 150(3), e2022058859. Visit Source.
Romero, H. M., Ringer, C., Leu, M. G., Beardsley, E., Kelly, K., Fesinmeyer, M. D., Haaland, W. L., Johnson, J. B., & Migita, D. (2018). Neonatal jaundice: Improved quality and cost savings after implementation of a standard pathway. Pediatrics, 141(3), e20161472. Visit Source.
Wong, R. J., & Bhutani, V. K. (2024a). Unconjugated hyperbilirubinemia in the neonates: Etiology and pathogenesis. UpToDate. Retrieved March 13, 2024. Visit Source.
Wong, R. J., & Bhutani, V. K. (2024b). Unconjugated hyperbilirubinemia in term and late preterm newborns: Initial management. UpToDate. Visit Source.
Woodgate, P., & Jardine, L. A. (2015). Neonatal jaundice: Phototherapy. BMJ Clinical Evidence, 2015, 0319. Visit Source.
Xie, B., da Silva, O., & Zaric, G. (2012). Cost-effectiveness analysis of a system-based approach for managing neonatal jaundice and preventing kernicterus in Ontario. Paediatrics & Child Health, 17(1), 11–16. Visit Source.
Yu, T. C., Nguyen, C., Ruiz, N., Zhou, S., Zhang, X., Böing, E. A., & Tan, H. (2019). Prevalence and burden of illness of treated hemolytic neonatal hyperbilirubinemia in a privately insured population in the United States. BMC Pediatrics, 19(1), 53. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.