FL APRN Autonomous Practice Applicant (Differential Diagnosis): Wound Series Part 1: Assessing and Diagnosing Chronic Wounds of the Lower Extremity
1.5 Contact Hours
Only FL APRN Autonomous Practice Applicants will receive credit for this course.
Listen to Audio
Get one year unlimited nursing CEUs $39Sign up now
This course is only applicable for Florida nurse practitioners who need to meet the autonomous practice initial licensure requirement.
This peer reviewed course is applicable for the following professions:
Advanced Practice Registered Nurse (APRN), Certified Registered Nurse Practitioner
This course will be updated or discontinued on or before Sunday, March 12, 2028
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will know how to identify acute versus chronic wounds and differentiate key findings associated with venous, arterial, diabetic, and other common etiologies of lower extremity ulcers.
Objectives
After completing this course, the participant will be able to:
Describe phases of wound healing in acute wounds.
Compare and contrast differences between acute and chronic wound healing.
Determine skin changes in the aging process that may negatively impact wound healing.
Summarize common etiologies of chronic wounds of the lower extremities.
List common differences in wound characteristics that help differentiate wound etiologies.
Describe common diagnostic tools/methods that may be useful in determining the etiology of lower extremity wounds.
Outline essential items that should be included in all wound assessment documentation.
Explain modifiable contributing factors to impaired wound healing.
Identify at least one characteristic of skin pigmentation that may impact early detection of inflammation or pressure injuries.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Wounds have been occurring for thousands of years. The ancient Babylonians, Sumatrans, Egyptians, and Chinese (from 2600 B.C. to 1500 B.C.) described several types of wounds, including open wounds of the legs and common treatments that included "lint" (typically some kind of plant fiber), oil, grease, animal fat, mud, honey, resins, and vinegar or wine (Majno, 1975). Scientific advances have provided many evidence-based wound treatment methodologies. Medical technology has vastly improved over the past century. Science has refuted some ancient practices (such as using animal fat and mud as wound treatments) while affirming the effectiveness of certain wound care principles used over 2000 years ago, such as keeping the wound clean, the wound bed moist, and protecting the wound from infection (Sibbald et al., 2021). Unfortunately, throughout history and even in modern-day healthcare, far too many approaches to wound care are steeped in tradition rather than scientific evidence (Bryant & Nix, 2023), and many open wounds are often misdiagnosed. Arputhanathan et al. (2022) reported that 64% of non-healing wounds evaluated in a home study were not diagnosed accurately.
Clinical Pearl: Many historical wound treatments have supported moist wound healing. Moist wound treatments (those that keep the wound bed of open wounds moist) have been demonstrated to promote faster healing for most wounds versus letting the wound dry out. Modern wound management has centered around moist wound healing since George Winter’s pivotal research in the 1960’s conducted on wounds on live pigs (Armstrong & Meyr, 2022; Nuutila & Eriksson, 2021).
This educational course is intended to provide health care clinicians with a general overview of evidence-based open wound care, with a focus on chronic lower extremity wounds. This course reviews acute versus chronic wound healing and a simple initial approach for differentiating and diagnosing common chronic wounds of the lower extremities. This course focuses on assessment and does not significantly address management or treatment (that is covered in another course).
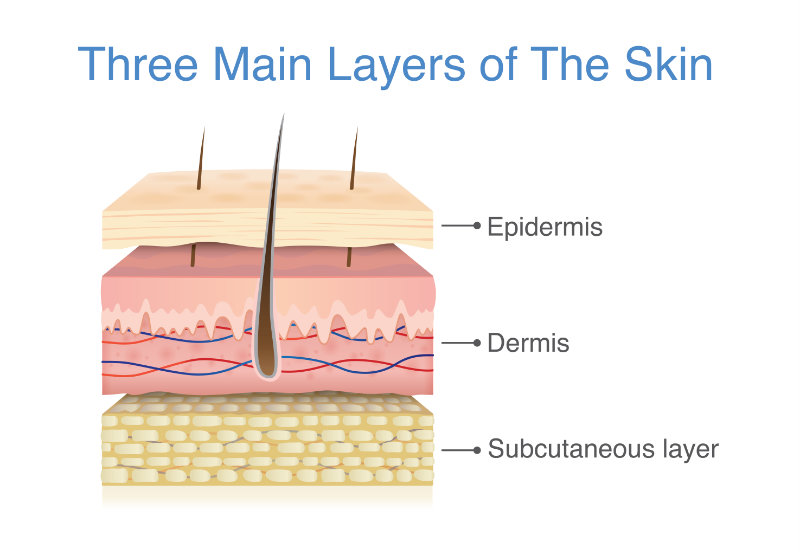
The skin covering the human body is the largest organ of the body. The skin's main role is protection (protecting the body from the environment, including chemical, radiation, microbial, and traumatic assault). However, the skin provides other essential functions, including important roles in metabolism and nutrition (fluid and electrolyte balance), thermoregulation, communication (sensation, touch, cell signaling, emotions, etc.), and immune function. The skin has also become important for medication or therapeutic substance administration, which can be administered topically and absorbed systemically. The skin tissues receive approximately 33% of the circulating blood volume in an adult and weigh up to 15% of the total body weight of an adult (Wysocki, 2023). The skin has three main layers: the epidermis, dermis, and hypodermis (or subcutaneous tissue).
Image 1: Layers of the Skin
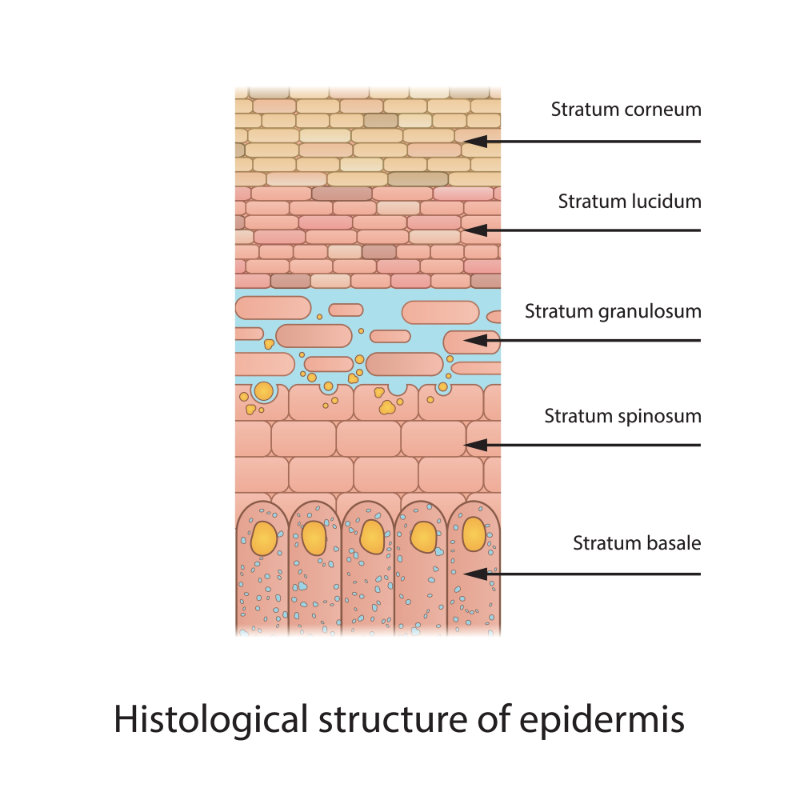
The epidermis is made up of keratinocytes or stratified squamous epithelial cells. It averages 0.075 millimeters (mm) to 0.15 mm thickness over most of the body, except on the soles and palms, where it is thicker (0.4 to 0.6 mm), and on eyelids and joints of the hands, where it is much thinner. The epidermis has five layers: stratum corneum, stratum lucidum, stratum granulosum, stratum spinosum, and stratum b or stratum germinativum (basal layer).
The epidermis is avascular and is constantly being renewed. The average turnover time ranges from 26 to 42 days, with complete regeneration between 45 and 75 days.
Image 2: Epidermis Structure
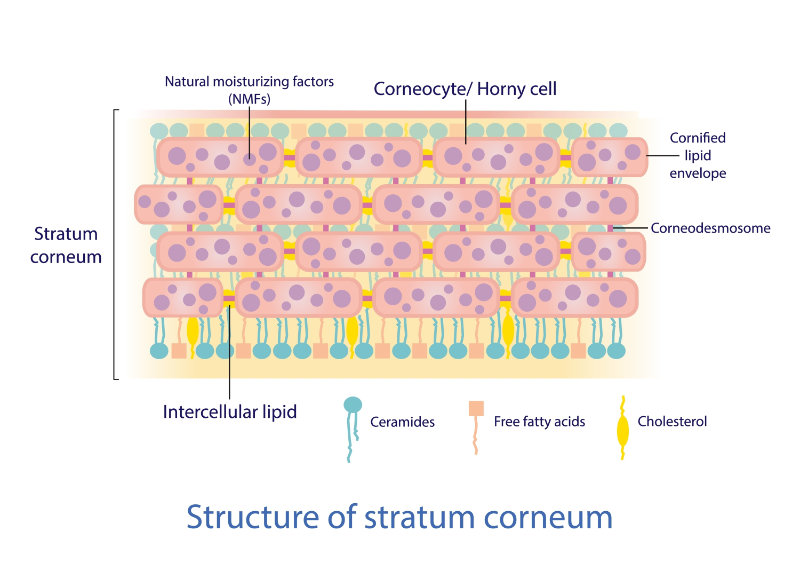
The stratum corneum (horny layer) is made up of dead keratinized cells (corneocytes) that are completely differentiated keratinocytes (80% of these cells are filled with keratin, which is insoluble, tough, and fibrous). The thickness of this layer varies with age, gender, and disease. The keratinocytes of this layer are mostly flat, pancake-shaped cells. Wysocki (2023, p.117) notes, "Keratin is resistant to changes in temperature and pH and to chemical digestion by trypsin and pepsin. This same protein is found in hair and nails; in these structures, keratin is referred to as 'hard' keratin compared with the 'soft' keratin of the skin." Additionally, the stratum corneum contains a lipid matrix that improves the skin's protection/barrier properties and comprises approximately 15% free fatty acids, 25% cholesterol, and 50% ceramides. This composition changes with aging.
Image 3: Stratum Corneum
The stratum lucidum is directly below the stratum corneum in areas where the epidermis is thicker (soles of feet and palms of hands), but is not present in areas of thinner skin (eyelids). The stratum lucidum (when present) is transparent and one to five cells thick. The actual differentiation between cells of this layer and adjacent layers can be difficult to identify under a light microscope because of the transitional nature of this layer. During transitional processes, active lysosomal enzymes degrade the nucleus and cellular organelles of keratinocytes before they are moved into the stratum corneum.
The stratum granulosum (granular layer) is one to five cells thick and lies directly beneath the stratum lucidum (when present); otherwise, it is directly beneath the stratum corneum. The stratum granulosum is named the granular layer because the keratinocytes in this layer contain keratohyalin granules. The keratinocytes of this layer are diamond-shaped because they have not yet been compressed and flattened. The cells of this layer also contain active nuclei. The keratohyalin granule structures contained in these cells are easily stained with basic dyes and an appropriate acid. Proteins in the keratohyalin granules of these keratinocytes include profilaggrin, intermediate keratin filaments, and loricrin. Loricrin is cross-linked to other protein components (cystatin A, small proline-rich proteins [SPRR1, SPRR2], elafin, envoplakin, and involucrin). Up to 70% of the molecular mass of the cells in this layer is comprised of these proteins combined.
The stratum spinosum layer is also known as the prickly layer because the keratinocytes of this layer are typically polyhedral and take on a prickly appearance due to the cytoplasmic structures in these cells. The protein involucrin is synthesized by cells in this layer, which provides a precursor of the cornified envelopes that are important in the transition of these keratinocytes into the stratum granulosum. The desmosome, a type of cell–cell junction, is one of the most prominent components of this layer. These desmosomes provide resistance to mechanical forces and increased adhesion between cells. The role and function of desmosomal proteins (plakoglobin, desmoplakin, plakophilins) and transmembrane glycoproteins (desmogleins, desmocollins) identified in this layer have been demonstrated to impact potential epidermal pathologies, such as pemphigus vulgaris, bullous impetigo, and others.
The basal layer is a single layer of basal keratinocytes, also known as basal cells.
The basal layer is the main layer of the epidermis with mitotically active cells (basal cells) that respond to several factors, such as glucose, growth factors, extracellular matrix, hormones, and vitamins. After leaving the basal layer, keratinocytes begin the differentiation process. Cells leave the basal layer in an upward migration that can take 14 days to reach the stratum corneum and an additional 14 days to move through the stratum corneum to the outermost skin surface.
The rete ridges at the base of the basal layer are partly responsible for anchoring the epidermis and helping ensure the skin's structural integrity. Important features of the basal layer include epidermal stem cells (which compose approximately 10% of the basal cell population), rete ridges or rete pegs, and melanocytes (approximately one melanocyte for every 36 basal cells).
Wysocki (2023, p.120) states, "Dendritic melanocyte structures are responsible for the transfer of pigment to a large number of keratinocytes. The primary difference between light- and dark-skinned individuals is the size, number, and distribution of melanosomes, the structures containing the melanin pigment, and the activity of the melanocytes. Carotene or carotenoids are responsible for imparting the yellow hue to the skin of some individuals."
The basement membrane zone, BMZ, or dermal-epidermal junction, has three distinct zones: the lamina lucida, the lamina densa, and the lamina fibroreticularis. One main function of the BMZ is to anchor the epidermis to the dermis. Since no blood vessels are in the epidermis, this BMZ junction facilitates nutrient flow for metabolites and other molecules into the epithelium.
This junction is affected in second-degree burns, blister formation associated with dermatologic diseases, full-thickness wounds, and mechanical trauma. With open wounds that extend deeper than the epidermis, the BMZ is disrupted and must be reformed. Wysocki (2023, p.121) states, "The major proteins found in the BMZ are fibronectin, an adhesive glycoprotein; laminin, a glycoprotein; type IV collagen, a non-fiber-forming collagen; and heparin sulfate proteoglycan, a glycosaminoglycan. A lesser amount of type VII collagen has also been detected, which forms anchoring fibrils that link the extracellular matrix of the dermis to the basement membrane."
The dermis, also known as the corium, is the thickest part of the skin: it averages 2 mm over most of the body but typically ranges from 2-4 mm in thickness. The dermis of the forehead, scalp, wrist, palm, thigh, and abdomen is thinner than the dermis of the back. Fibroblasts are the main cells found in the dermis and vary in size and number. Fibroblasts synthesize and secrete glycoproteins in the dermis, including fibronectin, thrombospondin, laminin, vitronectin, and tenascin. It has been reported that fibroblasts in darker-pigmented facial skin were larger, occurred in greater numbers, and were more likely to be binucleated or multinucleated compared with those with lightly pigmented skin. The implications of this for wound healing have yet to be fully explored. Unlike the epidermis, the dermis is innervated (has nerve structures) and is vascular (has blood vessels). Because the dermis is vascular, it serves the body by assisting with the inflammatory response, hemostasis, thermal regulation, immune support, nutritional support, and wound healing. Other cells found in the dermal layers help the skin's immune system to function properly, including lymphocytes, mast cells, and macrophages. Other structures in the layers of the dermis include sebaceous glands, eccrine and apocrine sweat glands, and hair follicles found within the dermal appendages.
The dermis consists of 2 layers: The papillary dermis and the reticular dermis. In wound healing, angiogenesis (forming new blood vessels from preexisting vessels) occurs in the dermis. Angiogenesis is stimulated by vascular endothelial growth factor (VEGF), secreted by keratinocytes in response to hypoxia/skin wounding. The dermis is also largely involved in disorders involving tumor growth and metastasis, hemangiomas, telangiectasia, psoriasis, and scleroderma. Two major proteins found in the dermis are collagen and elastin. Collagen is a fiber-forming protein that accounts for 25% of the skin's total weight and gives skin its tensile strength (the ability to be stretched to a point without breaking). Collagen is primarily made up of proline, glycine, hydroxyproline, and hydroxylysine. Elastin is a fiber-forming protein, like collagen. It accounts for less than 2% of the skin's total weight and gives the skin an elastic recoil (or "bounce back" when stretched and released and prevents the skin from being permanently misshapen). Elastin has a high amount of proline and glycine, but does not contain large amounts of hydroxyproline. "Ground substance" is also found in this layer, comprised of various proteins in the space between collagen and elastin fibers. Although these proteins account for only 0.2% of the dry weight of the dermis, they can bind up to 1000 times their volume. Thus, they play a role in regulating the water-binding capacity of the dermis, which helps determine dermal volume and compressibility.
The papillary dermis is immediately below the BMZ. In this dermal layer, papillae (finger-like projections) form interlocking structures with the rete ridges of the epidermis. Lymphatic vessels, which help control interstitial fluid pressure by fluid resorption, are found in the papillary dermis. These lymphatic vessels also assist in clearing the tissues of cells, lipids, bacteria, proteins, and other degraded substances. The dermal papillae contain papillary loops, which supply the necessary oxygen and nutrients to the overlying epidermis via the BMZ. The papillary lymph vessels drain into larger lymph vessels in the deep subpapillary venous plexus, connected to the reticular dermis lymph system. Fluid flow through this system is partially controlled through arterial pulsations, muscle contractions, and body movement.
The reticular dermis forms the base of the dermis. Cutaneous blood vessels are found in the reticular layer of the dermis. There is no clear separation of the papillary and reticular dermis layers because the size of the collagen fibers within these dermal layers changes gradually between the two layers.
The hypodermis, also known as subcutis or subcutaneous tissue, is not directly a layer of the skin but rather the subcutaneous layer below the dermis, which attaches the dermis to underlying structures.
The hypodermis attaches the dermis to the underlying structures. This hypodermis or subcutaneous tissue layer helps regulate temperature, provides protection (insulation for the body, additional cushioning), and stores energy (fat). The hypodermis also assists with the mobility of the skin over underlying structures (e.g., bones and joints). The hypodermis, or superficial fascia, forms a subcutaneous layer below the dermis. It is largely comprised of adipose (fat) tissue. Sweat glands (both apocrine and eccrine) and growing hair follicles can extend into the hypodermis. This hypodermis layer also contains a reservoir of adipose-derived stem cells that help modulate skin repair and (in concert with other cells) affect paracrine and endocrine systems. This reserve supply of stem cells is decreased with aging, and their ability to respond to skin repair is reduced (Wysocki, 2023, pp. 117-124).
Clinical Pearl: The hypodermis (subcutaneous adipose tissue) is where subcutaneous injections are given via a hypodermic needle. The hypodermis is largely absent or specifically affected in certain pathologic disease states, such as Werner syndrome (also known as adult progeria), lipodystrophy, lipedema, and scleroderma. Think about how this may impact healthcare. What considerations may be needed in these patients where the hypodermis is absent or sclerosed?
Make sure additional thermal regulation needs are met (extra blankets if hospitalized, adequate clothing, etc.).
May need to explore alternate routes of medication administration if subcutaneous injections are ordered.
Additional safety precautions to prevent falls and/or padding may be needed to reduce risk of bone/joint injury.
In addition, we are learning more about how different skin pigmentation may impact skin components, function, and wound healing. For instance, persons with darker pigmented skin are more prone to keloids (hypertrophic scarring), and vitiligo may have decreased vitamin D levels; the stratum corneum layer has higher lipid content and contains melanosomes (lighter skin does not have melanosomes in stratum corneum); skin tissues contain more blood vessels but less abundant elastin than lighter skin; the papillary and reticular layers contain more ground substance proteins (found in the space between collagen and elastin fibers); and significantly, early inflammation in darker pigmented skin is more difficult to identify (early discoloration/erythema may be masked or overlooked). This is especially important to note related to skin and wound assessment and early tissue damage recognition (such as stage 1 pressure injuries because darker pigmented skin may not "blanch"). Additionally, while darker skin pigmentation may be protective against certain skin cancers, precancerous and cancerous tumors may be more difficult to identify due to increased melanin. Darker pigmented skin is also associated with a higher prevalence of traumatic alopecia; it is also more prone to hair breakage and pseudofolliculitis due to the spiral shape and curvature of hair follicles. Thus, the unique characteristics and physiological differences found in individuals with different shades and hues of pigmented skin are important considerations for healthcare providers (Wysocki, 2023) and warrant further research to inform individualized treatment plans for skin protection and management of wounded skin across all degrees of skin pigmentation.
Clinical Pearl: Early skin damage and signs of inflammation are more difficult to detect amongst individuals with darkly pigmented skin. Therefore, early diagnosis can be more difficult because skin discoloration/erythema may be absent, masked, or overlooked. Assessment of darker pigmented skin should include visual inspection (early signs of injury may include darker, lighter, or unchanged color shades over the area), physical palpation (warmth, coolness, firmness, or bogginess when compared to surrounding skin), and subjective responses from the individual themselves (is there pain, tenderness, numbness, or a different sensation over the area in question compared to the surrounding skin?). This is especially important to note related to skin and wound assessment and early tissue damage recognition such as when attempting to identify stage 1 pressure injuries because darker pigmented skin may not “blanch”, therefore these injuries at a stage when they may be potentially reversed, are overlooked until the injury escalates to actual tissue loss and open wounds (stage 2 or stage 3).
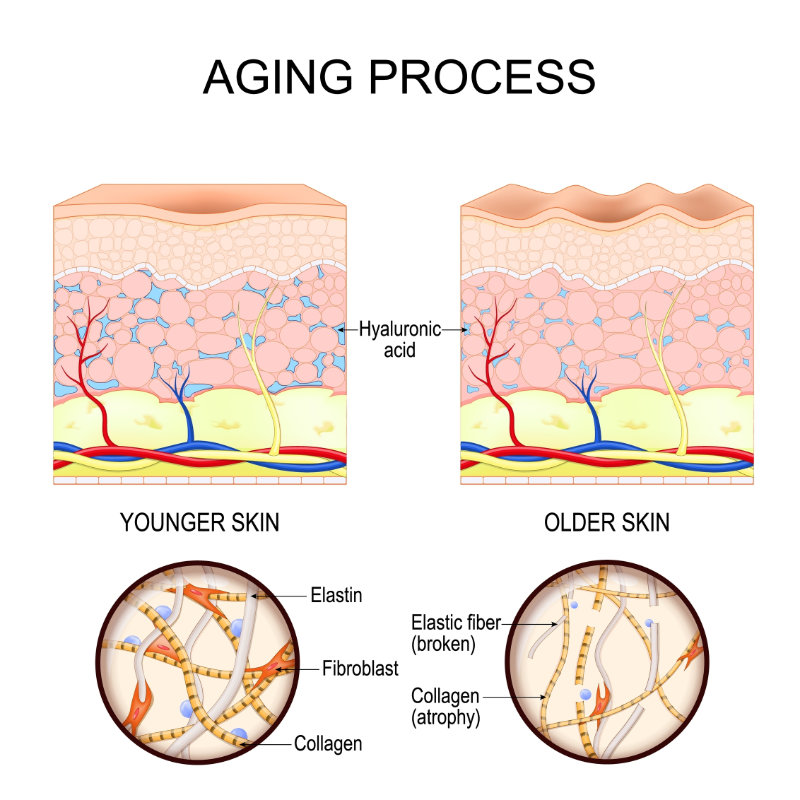
By 2040, approximately one in five Americans will be 65 years or older (Wysocki, 2023, p.128). It is important to consider the impact of the aging process on skin function and structure. So many of these changes in humans as they age can affect wound healing.
The following are key differences between adults (average age 35 years old) and older adults (aged over 65 years):
Skin thickness in older adults (over 65 years old) is decreased by 30 to 35%.
Skin elasticity decreases with age and is related to a combination of aging and solar damage.
Epidermis changes include the following:
Epidermal thinning (10%–50%) in older adults.
Decreased number of active melanocytes by 10%–20% each decade after adulthood.
Increased time it takes for epidermal turnover in older adults.
Loss of epidermal stem cell population in older adults.
Increase in apoptosis (programmed cell death) below the granular layer in older adults (these cells don't survive as long in older adults as in younger adults).
Flattening the dermal–epidermal junction with loss of rete pegs/dermal papillae in older adults results in easier separation of the epidermis from the dermis (more prone to skin tears and blisters).
Dermis changes include the following:
Approximately 20% loss of dermal thickness (potential 1% reduction each year after age 40).
Decrease in elastin synthesis in older adults.
Decrease in the number of fibroblasts in older adults.
Decrease in synthesis and turnover of collagen types I and III in older adults.
Increase in collagen cross-linking in older adults.
Slight decrease in levels of hyaluronic acid, glycosaminoglycans, and proteoglycans.
Increased matrix metalloproteinase expression in older adults.
Increase in advanced glycation end-products in older adults.
In older adults, subcutaneous fat is lost (resulting in a reduction of protection of underlying structures).
Vascular changes (these changes potentially prevent the older adult's body from responding as aggressively during inflammation and wound healing, including impaired leukocyte (such as neutrophils and monocytes) migration through the venular basement membrane).
Approximately 30% reduction in venular cross-sections in older adults.
Approximately 60% reduction in peak cutaneous blood circulation in older adults.
Reduced vascular response in older adults.
Up to 50% reduction in vascular wall thickness at age 80 years.
Decreased vasoconstriction/vasodilation arteriole response with aging.
Decrease in vascular endothelial growth factor in older adults.
Decreased endothelial cell permeability response with aging.
There are sensory changes with aging, including a 2/3rds reduction in the number of Pacinian and Meissner corpuscles, resulting in a reduction in sensation (pain threshold increases up to 20%) in older adults, which is an important consideration related to the prevention and assessment of the potential for neuropathic and pressure-related skin injury.
Reduced size and function of apocrine sweat glands (found in dermal appendages usually associated with hair follicles, such as in armpits and perineal region) are seen in older adults.
In older adults, there is a 15% reduction in the number of eccrine sweat glands, with a 70% reduction in sweating. These eccrine sweat glands are found all over the body, including the soles of the feet and palms of the hands. They are largely under the nervous system's control and have a role in thermoregulation.
Immune function/immune cells of the skin are reduced in older adults, leading to the following:
Host defense mechanisms are reduced in older adults.
Langerhans cells are reduced by 20%–50%.
Mast cells are reduced by up to 50%.
At the same time, there is an increase in the number of potentially harmful autoantibodies (such as bullous pemphigoid, antinuclear antibodies, antithyroglobulin, and rheumatoid factor).
In older adults, there is a decrease in the sebum production of the sebaceous glands (by approximately 65%), but the number and size of the actual glands remain similar to those of adults. Sebum is an oily or waxy substance that helps lubricate, moisturize, and protect the skin and hair from moisture loss.
Hair production and growth are diminished in older adults. There is a reduction in hair follicle density. Hair follicle melanocyte activity is reduced or absent. It takes longer for hair to grow in older adults. Adults typically develop up to 50% gray/white hair by age 50 years and experience a 20% decrease in hair follicles by 60 years. Hair diameter is reduced in older adults, and bitemporal hairline recession is noted in both genders with aging.
Clinical Pearl: Physiological changes in aging have significant implications for the healthcare of older adults. In particular, the implications of these changes should be considered in any older adult related to their ability to respond to skin and wound threats (risk of injury/skin breakdown), and how these factors may impact wound healing. Health care providers should consider these factors when assessing, diagnosing and managing the older adult with a wound.
Of interest, a study of 223 older adult residents of a nursing home found that “nearly every resident had at least one dermatological diagnosis” (Richbourg, 2022 p. 262).
The depth of the wound related to the layers of the skin can help classify wounds as either partial thickness in nature (depth of injury only involves the epidermis and sometimes the dermis but not beyond the subcutaneous tissue) or full thickness in nature (damaged tissue which extends down through the epidermis, dermis, and involves at least some subcutaneous tissue, muscle, tendon or bone (Betz, 2022; Bohn & Bryant, 2023). The extent of disruption to the layers of the skin potentially impacts many of the normal skin functions and should be considered when assessing and managing wounds (Wysocki, 2023).
Most partial-thickness wounds heal without scar tissue formation because they heal by re-epithelialization (Betz, 2022; Bohn & Bryant, 2023). A superficial epidermal tissue loss is experienced, and this epidermal skin is regenerated by cells readily available at the skin's surface or within hair follicles (mainly keratinocytes). These partial-thickness wounds heal faster than full-thickness wounds, which involve greater tissue loss and more extensive cellular damage, requiring more complex mechanisms of repair, with many more cell types and chemical messengers involved in the process to coordinate the healing efforts within the wound bed (Betz, 2022; Bohn & Bryant, 2023).
Full-thickness wound healing takes place by one of three main mechanisms (Betz, 2022; Bohn & Bryant, 2023):
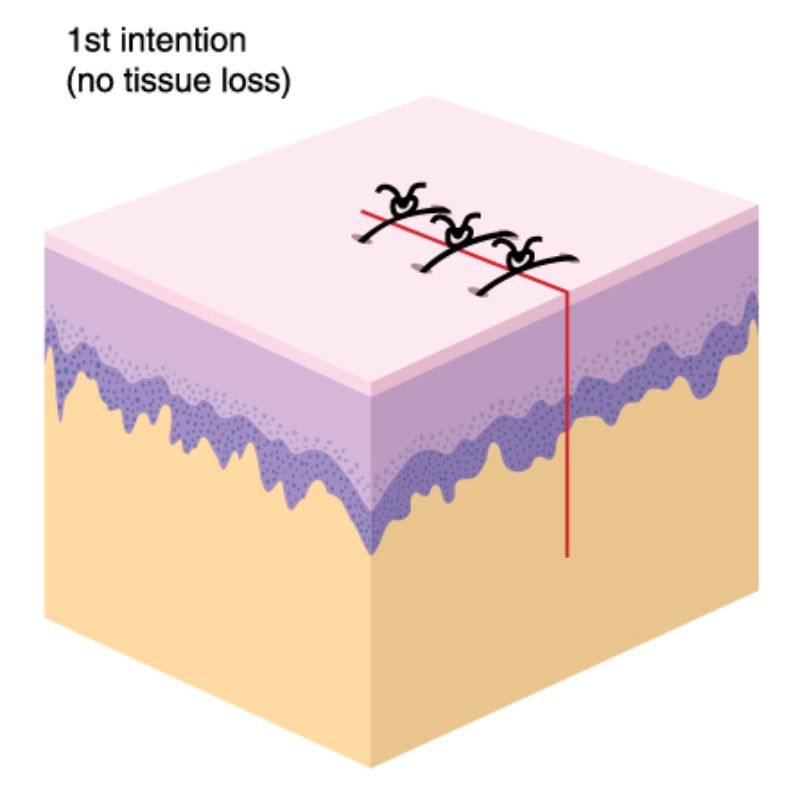
1. Primary intention (example: a surgical wound or incision is made in the skin, then the cut edges are brought together and closed with stitches, staples, adhesive strips, or some kind of skin bond).
Image 5: Primary Intention
2. Secondary intention (example: a wound is left open to heal from the inside out and form new/scar tissue).
3. Tertiary intention (example: a surgical wound left open for a time and is surgically closed/approximated at a later date).
Wounds healing by primary intention tend to heal faster than wounds left open to heal by secondary intention. They may heal as fast as partial thickness wounds because the wound edges have been approximated, and the body does not have to build or produce as much new tissue or extracellular matrix (scaffolding) or granulation tissue necessary for scar tissue formation. Since the body is repairing a defect similar to sewing together a torn garment, it takes fewer resources than manufacturing a patch, filling the hole, and holding it all together (Betz, 2022; Bohn & Bryant, 2023).
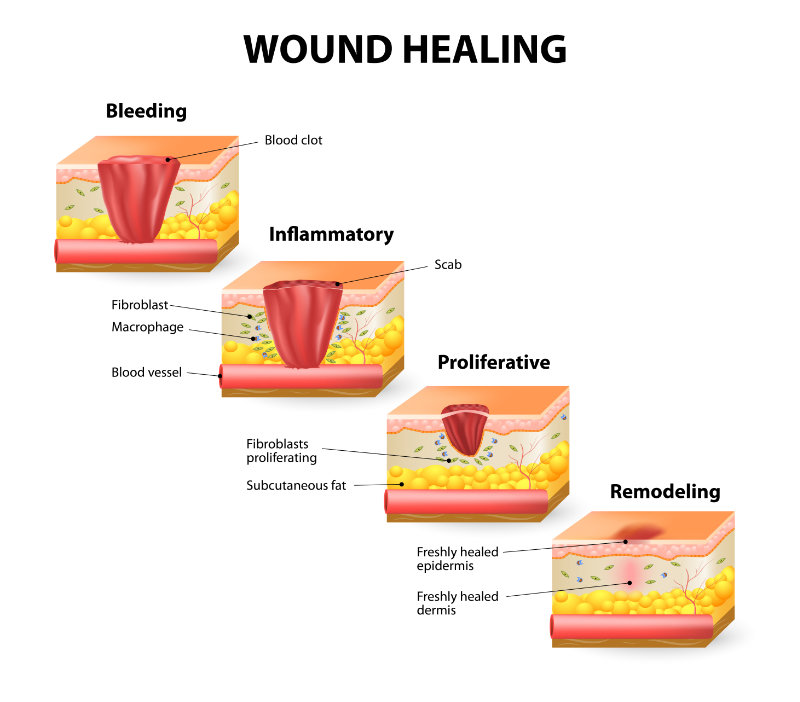
In an acute wound (such as when a teenager falls while skateboarding, causing a small amount of full-thickness tissue loss), the pathway to healing is expected to follow progressive phases of wound healing, typically over only a few weeks. Acute wounds follow an orderly, expected, and timely healing process. The normal and expected healing process contains the following phases, which may overlap throughout the healing process (Betz, 2022; Bowers & Franko, 2020). Some scientists have described three phases or steps, and others describe four or more overlapping phases or steps, but the mechanisms are the same.
Hemostasis and the inflammatory phase are initiated after a full-thickness injury. Immediately after injury, bleeding occurs, and the coagulation pathway commences (aggregation of platelets, the release of clotting factors, neutrophils, macrophages, and a host of chemical messengers to alert the body to stop the bleeding). Hemostasis is typically achieved within several minutes. At the same time the body completes hemostasis, it also sends immune cells such as neutrophils. These monocytes may convert to macrophages, other cells (fibroblasts), proteinases (enzymes), and chemical messengers to the area to clear invading pathogens and debris and begin the repair processes. The inflammatory phase typically lasts a few days (Bohn & Bryant, 2023).
The next overlapping phase is the proliferative phase. As the expected pathways to healing occur, cytokines (chemical messengers) alert fibroblasts and other cells to produce growth factors and build new capillaries (neoangiogenesis) and connective or "granulation" tissue largely made of collagen to fill in the open defect of any full-thickness wound (Bohn & Bryant, 2023). Enzymes such as more than 15 matrix metalloproteinases (MMPs), secreted by fibroblasts, epithelial cells, neutrophils, and macrophages, play a major role during the inflammatory and proliferative phases, breaking down damaged proteins (such as collagen) and debris. Epithelial cells (particularly keratinocytes) are very active during the proliferative phase, helping to make the wound smaller and smaller ("contracting" the wound edges). The proliferative phase typically lasts a few weeks (Bohn & Bryant, 2023).
Finally, there is the maturation phase (scar maturation), which occurs after the wound is closed (epithelialized). However, the protein-rich extracellular matrix (ECM) or new tissue "scaffolding" within the scar tissue is continuously broken down and replaced with stronger scar tissue. The 'scar tissue' comprises various types of collagens (our bodies produce more than ten types of collagens for this purpose), elastin, laminin, etc. The maturation phase can take up to 18 months or longer. It is important to remember that even after the scar maturation phase has concluded, the maximum tensile strength of the scar tissue of full-thickness wounds only reaches 70-80% of the tensile strength of the surrounding tissue (Bohn & Bryant, 2023). Therefore, once a full-thickness scar has formed, it may always be considered a 'weak link' or vulnerable area in the body, needing protection, particularly from the sun and pressure-related damage (Bohn & Bryant, 2023). Older adults are at risk of defective tissue remodeling in this phase (Richbourg, 2022), which may further impact tensile strength due to the changes in skin tissue function that occur in aging, such as compromised fibroblast function (refer back to the "The Impact of Aging on the Skin" section above). Scar tissue contains no melanocytes, so the scar will require sunblock to protect against the sun's rays on any exposed body part. Likewise, scars over bony prominences will require additional protection against pressure-related injury for the rest of the individual's life. These two realities are often overlooked by healthcare providers, caregivers, and patients, but should be incorporated into lifelong health promotion education for all applicable individuals.
In the past, clinicians have attempted to assign a specific timeframe for classifying wounds as acute or chronic. Many clinicians have mistakenly thought that any wound that heals within six weeks is acute and any wound that takes six weeks or more to close is chronic. Many clinicians have mistakenly thought that any wound that heals within six weeks is acute and any wound that takes six weeks or more to close is chronic. The scientific literature no longer supports the classification of acute versus chronic wounds (Bohn & Bryant, 2023).
The young 16-year-old skateboarder's knee abrasion would hopefully move through these healing phases with complete resolution within about four weeks. However, if this wound were complicated by infection, the involvement of joint or tendon or ligament, or worsened, or was just not improved within the expected time after wounding, we would consider it a chronic wound. Likewise, a large surgical wound may take more than six weeks to heal but still be considered acute (for example, a 15-centimeter [cm] long by 10 cm wide by 3 cm deep abdominal surgical wound left open to heal by secondary intention). As long as it continues to improve (get smaller) as expected, without any signs of infection or complications, it would be considered an acute-healing wound. Even though this surgical wound could be described as complex because of its size and nature, it could also be considered an 'acute' wound if it progresses through the phases of healing as expected. Other ways to differentiate acute versus chronic wounds have been predicated on the wound environment, particularly the levels of MMPs, tissue inhibitors of metalloproteinase (TIMP), and wound pH present in the wound bed of open wounds. Acute wounds have higher MMPs at the start during inflammatory processes, but they level off and drop to much lower levels than in chronic wounds. Considering potential impairments to wound healing and addressing those that are modifiable, some acute wounds may be prevented from deteriorating into chronic wounds. Common impediments to wound healing include repetitive injury, infection, vascular compromise, smoking, inadequate nutrition (and hydration), advanced age, certain medications, poor control of comorbid conditions (diabetes, immune disorders, etc.), and inappropriate wound treatments (cytotoxic products; products which disrupt moist healing environment; products impairing oxygenation, cellular signaling, or cellular migration). Acute wounds should be followed at least every 1-2 weeks after the initial visit. It may be followed less frequently if continuing to progress through the expected healing phases. The frequency of follow-up may depend on the size and complexity of the wound. Patients can be instructed to seek immediate care or contact the wound healthcare provider immediately if the wound deteriorates or worsens (e.g., fever, increased pain, signs or symptoms of infection, "bruising that seems to be growing," decreased mobility of the extremity or a joint near the wound, if applicable).
Brian is a 16-year-old Hispanic male skateboarder with no known chronic diseases. He is in high school and is very active. He appears well-groomed, alert, and oriented, and he speaks, reads, and writes English well. His height is 5'8". He weighs 123 pounds (body mass index [BMI] = 18.7). His temperature is 98.6°F orally. His blood pressure is 120/68, his pulse is 70 beats per minute, his respirations are 20 per minute, and his oxygen Saturation is 98%. He says he eats three times a day most days (plus snacks) and denies any problems with his teeth or swallowing. He admits to sometimes smoking "regular" cigarettes, but does not want to disclose how many. He did not want to answer questions about alcohol intake. He presented to the clinic with a 2 cm long by 1.5 cm wide by 0.2 cm deep wound to his right lower leg just below the knee. He reports he received the wound two days ago while skateboarding (without kneepads or a helmet), and he fell on a concrete sidewalk and lawn. He denied any other injury or hitting his head when he fell. He is current on all his immunizations and had a tetanus booster only two years ago.
He reports his mom poured hydrogen peroxide on the wound to clean it up and then applied an adhesive bandage with "some sort of ointment." It is clean appearing, has a pink wound bed, scant serosanguinous drainage (clear pink), and appears to be a partial thickness wound with only slight erythema extended out 0.3 cm from the periwound edges. The rest of the skin appears within normal limits for his age and skin tone. He denied any fever and said the pain is two out of ten. He says he sometimes takes ibuprofen for pain, headaches, or muscle aches if he needs it – on average, 1-2 times a week. He denies taking any other medications or street drugs. His motion of the knee does not appear to be affected.
Some things to consider:
Would you classify this as an acute or chronic wound?
What are potential impediments to wound healing for this young man? Some things to consider include nutritional intake may be inadequate (BMI is at the low end of normal), smoking (unknown amount), risky behavior (unknown alcohol intake habits, skateboarding without knee pads or helmet, and ibuprofen intake (if taken frequently or daily).
Given the young man's present wound, would you expect this wound to heal completely within four weeks?
When would you want to see this young man back in your clinic to examine the wound, such as in one day, two weeks, or four to six weeks later?
A chronic wound, on the other hand, is a wound that does NOT follow the expected pathway to healing (Betz, 2022; Wysocki, 2023). Current research demonstrates that most chronic wounds get "stuck" in the inflammatory phase of wound healing (Mervis, 2025). High levels of MMPs, enzymes, inflammatory cytokines (chemical messengers), and bacterial biofilms are common characteristics of chronic wounds. High levels of enzymes and pro-inflammatory cytokines in wounds are detrimental because they continue to break down new tissue and healthy cells before the wound bed can be repaired or "rebuilt." Bacterial biofilm also impairs wound healing (Betz, 2022; Bohn & Bryant, 2023). Biofilms are typically polymicrobial colonies of bacterial organisms that produce their own polymeric (plastic-like) coating to protect the community of organisms. Biofilms are felt to be responsible for 70% of infections in the human body (Sharma et al., 2023). Biofilm colonies in wounds establish tightly adherent "footers" into the wound bed, which extend 2-3 mm beneath the surface of the wound bed and help secure the biofilm in place.
Scientific literature demonstrates that biofilm is present in more than 60% of all chronic wounds (Weir & Schultz, 2022). Bacterial swab cultures may identify planktonic (free-floating) bacteria. Still, they may not accurately identify the many bacterial (and fungal) organisms that symbiotically exist in a biofilm (Weir & Schultz, 2022). In addition, research suggests that most topical wound products and systemic antibiotics typically cannot penetrate mature biofilm growth (Hurlow & Kalan, 2022; Weir & Schultz, 2022). One of the most effective ways to eliminate biofilm is to remove it physically, often by sharp debridement, ultrasonic cavitation, mechanical, waterjet, or larval debridement, for example (Brace, 2023; Hurlow & Kalan, 2022; Tran et al., 2023). However, biofilm is not visible to the naked eye, making it difficult to detect or determine when it has been completely removed (Hurlow & Kalan, 2023). Biofilms can cause direct tissue damage. They also inhibit keratinocyte migration and collagen synthesis and impair the activity of growth factors. Biofilm structures (both the bacteria contained within the protected biofilm community and those free-floating bacteria in the wound can impair cellular communication and compete with fibroblasts for oxygen and nutrients.
The result of these interferences is chronically high inflammatory responses in the wound bed, preventing the wound from moving into the proliferative phase of wound repair and delaying wound healing (Bohn & Bryant, 2023; Weir & Schultz, 2022). Of note, scientific literature indicates that all chronic wounds are "colonized" by bacteria, but they may not all be biofilm, and not all are clinically "infected" (Ermer-Seltun & Rolstad, 2022).
Other common impediments to wound healing include inadequate nutrition (especially inadequate protein intake and vitamin/mineral deficiencies), smoking, decreased immune function, advanced age, diabetes, poor oxygenation or perfusion of tissues, lymphedema, infection, certain medications (chemotherapy agents, non-steroidal anti-inflammatory drugs [NSAIDs], immune modulators) and continued or repeated mechanical trauma (especially pressure/friction/shearing forces). If wounds do not respond well to evidence-based treatment within two weeks, or if the wound worsens and the suspected wound etiology is being addressed, healthcare providers should consider further evaluation of (Davis & Hom, 2023):
Differential etiologies (including malignancy).
Other factors strongly associated with impaired wound healing.
In our previous example, the 16-year-old skateboarder's knee is expected to heal in 2-3 weeks (if there are no confounding reasons why his wound healing should take longer). However, if the wound is not improved (or worsens) within several weeks, it could be considered a chronic, complex, or recalcitrant wound, even though it may be smaller and is less than six weeks old. Another point to consider with all wounds, especially this skateboarder's knee, is the depth and location of the wound. A simple abrasion may seem rather shallow, but if it occurs over joints or where the dermis and epidermis are very thin (shin), there may be a joint capsule or bone involvement, severely complicating healing. Being mindful of these facts will help you to address wound healing more effectively.
Note: This course does not specifically address different treatments or dressings for chronic wounds. Still, even during an assessment, the clinician should always consider these factors and how treatments may potentially impact (promote/facilitate or impair/delay) the wound healing pathway.
Mr. Jones is a 74-year-old male who is seen in the primary care clinic with a non-healing wound on his left lower leg that he reports having for about two months. Would you know where to start? Below is a detailed example of one possible approach with the rationale discussed.
Chief complaint: Evaluate the patient's chief complaint (a wound on the left lower leg that is not healing). *Note the duration/date of onset of Mr. Jones' wound is two months duration.
Possible etiologies: How did the patient say he got the wound (trauma, stepping on a dirty nail, animal or human bite, maybe the patient does not know)? When considering possible etiologies, asking the patient how he thinks he got the wound and why he believes the wound is not healing is important (but realize the patient is not always correct about this). Other information to ascertain about the patient includes what treatments they have tried so far and any changes in the wound. He says he has washed it daily and kept a clean sock covering it. *Mr. Jones says he thinks he must have hit the outer part of his leg on his lawnmower two months ago, but cannot remember how the wound started. He has not used any wound products; he has just used soap and water.
Past medical history/comorbid conditions and physical limitations: Review important past medical history; comorbid conditions can lead you to suspect certain etiological factors. Diabetes, hypertension, high cholesterol, or cardiac diagnoses? Peripheral arterial disease (PAD) is likely in patients with an existing diagnosis of coronary artery disease (CAD) or related risk factors (diabetes, smoking, high cholesterol, and hypertension). The distal blood vessels are the smallest, so logically, the atherosclerotic arterial disease would first affect the distal blood vessels before the involvement of the larger coronary arteries is obvious. Respiratory or pneumonia (cardiovascular problems and anemia) are associated with potential wound oxygenation/perfusion issues. Rheumatoid arthritis, Crohn's disease, ulcerative colitis, and other autoimmune diseases are associated with impaired wound healing and a higher incidence of pyoderma gangrenosum (an autoimmune disease typically causing chronic wounds, especially of the lower extremities). Physical limitations are important to note because neuropathies and arthritis in the hands could make dexterity an issue in the patient's self-care of wounds. *Mr. Jones says he has some history of 'borderline high blood pressure,' but he does not take any medication for it. Otherwise, he denies chronic conditions.
Document allergies: Allergies may lead you to consider why treatment may not have been very successful and what treatments to avoid in the future. *Mr. Jones is allergic to sulfa medications.
Vaccination history: It is important to ask about (and document) the patient's last tetanus shot, especially if it has been ten years or more since the last tetanus vaccine or five years or more, and the wound was traumatic/dirty (stepped on a nail, hit the lower leg on the lawnmower). A tetanus booster vaccine should be given within 48 hours of the injury if it has been more than ten years since the last tetanus vaccination (or more than five years, and the wound is traumatic/dirty). Tetanus is a bacterial infection that is now rare (thanks to vaccination) but still very dangerous, and there is no cure. Two out of every ten people who get it will die. In the United States, deaths attributed to tetanus have dropped by 99% since 1947, largely due to the current Centers for Disease Control and Prevention (CDC) vaccination guidelines.
*Mr. Jones is current on his vaccinations and states he received a tetanus, diphtheria, and pertussis (Tdap) vaccine two years ago.
Clinical Pearl: Be aware that certain injuries (especially outdoor puncture wounds) and animal bites have a much higher incidence of serious infections. Particular types of bacteria are associated with particular animals or humans and cultures are recommended, but treatment may be started presumptively based on type of bite/injury. Individuals should be offered a tetanus vaccine as soon as possible after injury (48 hours), especially puncture wounds, but this also includes animal or insect bites (spider bites). In addition, certain animal bites may also warrant rabies vaccines and rabies immune globulin. See the CDC website for more information.
Social and dietary history: Assess and document all pertinent information, including social and current dietary/nutritional information. Pertinent social information (literacy level, health insurance, smoking, place of residence, electricity, running water, a caregiver at home, and heavy alcohol or illegal drug use) is important to note. It can influence the clinician's diagnosis and treatment options. Management approaches are available to the clinician and the patient. Assess the patient's current nutritional intake and dietary habits (three meals per day versus one meal per day, portion size, types of food). Poor nutritional intake is often overlooked, even though adequate nutrition (especially protein, essential micronutrients, and amino acids) is imperative for wound healing (Betz, 2022; Bonham et al., 2022; Bryant & Nix, 2023). *Mr. Jones is widowed, lives alone with his cat, has two grown sons who live in another state, and eats two meals a day on average: coffee for breakfast, early lunch (biggest meal; typically, meat and potatoes or rice and beans, sometimes salads), and early dinner around 5 pm (soup/sandwich most days). He denies drinking alcohol and denies any smoking or using street drugs.
Medications: The patient's medications (even over-the-counter medications) are also important to document. Corticosteroids and NSAIDs are common medications that may impair wound healing (McNichol et al., 2022). *Mr. Jones says he takes turmeric and fish oil supplements daily, sometimes takes aspirin or ibuprofen for headaches, and sometimes has an Epsom salt bath for muscle aches after yard work.
General exam and vital signs: While a focused exam of the wound is reasonable if that is the main purpose of the patient's visit, it is good to document general findings (especially general appearance, hygiene, skin lesions or rashes, edema) and vital signs (blood pressure, pulse, respiration, and temperature), height and weight (BMI). *Mr. Jones is well-groomed, wearing jeans and a flannel shirt. He is 5'11" and weighs 140 pounds (BMI= 19.5). His temperature is 98.6 degrees Fahrenheit orally, his blood pressure is 135/78, his pulse is 85 beats per minute, his respiration rate is 20, and his oxygen saturation is 97% on room air. His mucous membranes are moist but slightly pale. His gait is slow, and he limps slightly, favoring his left leg.
Assessing the lower extremity wound: Document the wound's location, size, and characteristics. The wound size and characteristics should be noted as length by width by depth at the deepest point in cm. The clock face is visualized over the wound, with 12 o'clock always pointing towards the head of the body and 6 o'clock pointing at the sole of the foot of the body - as a way to document the exact location of particular features of the wound, such as tunneling, undermining, etc. When the wound is measured, take care to note any tunneling or tracking in the wound bed (and where it tracks to, if possible. For instance, wound #1 tracks to/communicates via tunneling to wound #2, or if any undermining is present (a "lip" or "shelf" under unattached wound edges). Note the wound bed appearance for the presence of non-viable tissue and describe the color (white, grey, yellow, or black non-living tissue) versus healthy pink or red "granulating" tissue. List the amounts of these tissues in estimates of percentages covering the wound bed. In the wound bed, note any exposed bone, muscle, tendons, or ligaments. Be careful not to confuse any exposed tendons or ligaments with a linear, flat white or yellow appearance as non-living tissue. Drainage is documented by amount, color, and odor (e.g., a scant amount of clear yellow fluid with no remarkable odor). The location and appearance of the wound provide the clinician with important clues about the etiology or contributing factors to the wound. Physically assess the wound as described above, as well as the surrounding skin and the whole extremity (for example, are there any rashes, lesions, or other remarkable findings?). *Mr. Jones' wound is on his left lateral lower leg – just above the malleolus/ankle. The wound measures 2.0 cm in length by 2.0 cm in width by 0.4 cm in depth at 6 o'clock. The wound bed is 60% pale pink and 40% covered with yellow slough, mostly from 4-8 o'clock as you look at the wound. The exudate is yellow, in a small amount, and has no odor. There is some periwound erythema extending 0.5-1.0 cm from the inferior edge of the wound from about 4 o'clock to about 8 o'clock. The periwound skin from 3 o'clock to 7 o'clock is also macerated. No other rashes or skin lesions are noted, but the skin of the lower extremities and forearms appears very dry. Slight edema of the left foot (less than 1+ and non-pitting) is noted. The skin around the inferior border of the left leg wound is warmer to the touch than the surrounding skin. Otherwise, the skin of both legs is warm and dry.
Pain and sensation: It is also important to ask the patient about any wound pain and to document their answers. What are the relieving or aggravating factors (pain worse at night when the leg is elevated, or worse after all day on feet, and better when elevated at night)? What is their pain level on a scale of 1 to 10, and what is the character of the pain (constant, intermittent, throbbing, etc.)? Also, assess sensation and pain in the affected extremity, especially if the patient has diabetes (Bryant & Nix, 2023; Oropallo & Quraishi, 2023). *Mr. Jones reports his pain has been only about 3-4 out of ten for the past few weeks, but is now worse at night and has been 'throbbing' and increasing for the past three days.
Follow-up: Follow-up for non-healing or chronic wounds should ideally be one week after the initial assessment to evaluate the efficacy and response to the wound treatment orders and evaluate the need for debridement of non-viable tissue (Tran et al., 2023), and then in two weeks after that, if the wound is improving, progress to every 3-4 weeks. Ideally, it is a good idea to follow up more frequently if the wound worsens or if a wound treatment is changed, and restart the progressive frequency as long as the wound improves.
Some factors to consider for Mr. Jones include the following:
Would you classify this as an acute or chronic wound?
What are potential impediments to wound healing for this young man? Some things to consider include inadequate nutritional intake, his age, slough visible in the wound bed, and high bioburden in the wound.
Given Mr. Jones' present wound, would you expect this wound to heal completely within 2-4 weeks?
When would you want to see Mr. Jones back in your clinic to examine the wound after his first visit?
Always assess DP and PT pulses when any lower extremity wound is being assessed! Check popliteal pulses too, if warranted. In general, if there are strong DP and PT pulses (and capillary refill of the distal affected extremity appears normal/no other circulatory warning signs of arterial, venous or lymphatic insufficiency), they probably do not need further vascular evaluation by a specialist. However, if there are no palpable pulses in the affected lower extremity below the wound level, perform an ankle brachial index (ABI) of both lower extremities. This is a quick screening assessment for arterial insufficiency (Mavrogenis et al., 2018; Bonham, 2022). Toe pressures and toe brachial index is an alternative screening in individuals with incompressible ankle arteries or when there is an ankle wound (Bonham, 2022). If these are difficult to obtain, consider referral for further vascular studies such as doppler arterial blood flow studies, pulse volume recording, or transcutaneous oxygen tension testing to the periwound skin (> 40 millimeters of mercury [mmHg] is desired) to determine adequate arterial blood supply or perfusion to the affected extremity/wound area (Bonham, 2022; Mavrogenis et al., 2018). There is a nice quick reference guide for clinicians on how to perform ABI assessment here.
PAD affects more than 10 million people in the United States. Evidence-based clinical care guidelines strongly recommend assessing all patients with lower extremity wounds for arterial disease (level 1A evidence based on meta-analyses of multiple randomized controlled trials). Studies indicate that less than half of patients with PAD (7.5% to 33%) experience classic claudication symptoms, including increasing pain in the affected lower extremity with walking exercise (Schorr et al., 2017). Therefore, a diagnosis should not rest on this symptom alone. While venous insufficiency is the most common cause of lower extremity ulcers, mixed diseases (both venous and arterial insufficiency) have been reported in up to 25% of patients with lower extremity ulcers (Mavrogenis et al., 2018).
Wounds due to arterial insufficiency tend to be seen on the lower extremities over the toes and ankle joints (malleolus). The wound appearance for these arterial ulcers tends to be round with a "punched out" appearance. Wound beds for arterial ulcers tend to be pale and rather dry. The skin of the lower extremities in persons with arterial insufficiency is usually thin, with a shiny appearance and sparse hair growth. The patient may or may not demonstrate longer capillary refill times in the toe beds (over three seconds). The patient may demonstrate weaker pulses in the distal lower extremities (Mavrogenis et al., 2018). Please note that all patients with a wound on a lower extremity should have pulses evaluated in the most distal part of that extremity; any patient with absent or difficult-to-palpate pulses in the lower extremities should have a Doppler-derived ABI screening.
ABI of less than 0.9 indicates some measure of arterial insufficiency. ABI over 1.2 is likely due to incompressible (atherosclerotic) vessels of the lower extremity (more common with diabetics and patients with existing CAD). If ABI results are suspected to be falsely elevated, toe pressures may be obtained instead (and a toe brachial index may be calculated). A toe brachial index of less than 0.7 is strongly associated with lower extremity arterial disease (McNichol et al., 2022). The patient should be referred to a vascular diagnostic laboratory if the clinician does not have the equipment or expertise to perform an ABI or toe brachial index. Suppose an ABI cannot be obtained. In that case, other non-invasive diagnostic studies that may be useful for determining arterial blood flow, tissue perfusion, or severity of stenosis and occlusion include (but are not limited to) the following:
Transcutaneous tissue oxygenation (TcPO2) is measured on the tissue immediately surrounding the wound.
Readings over 40 mmHg are considered normal.
Readings less than 40 mmHg indicate some tissue perfusion impairment (readings over 30 mmHg are needed for wound healing).
Readings under 30 mmHg are > 80% unlikely to heal.
Segmental pressures (blood pressure cuffs and a continuous wave Doppler are used to obtain consecutive and contralateral levels/locations of blood pressure in the vessels of the lower extremity to determine the likelihood of stenosis or occlusion).
Levels/locations measured: ankle, just below the knee, just above the knee, and high thigh.
Of concern would be decreased pressure readings (> 20 mmHg) between two consecutive levels/locations in the same leg (indicating stenosis or occlusion) or between similar locations in both legs (indicating obstructive disease in the leg with lower pressures).
Duplex ultrasound scanning – this uses ultrasound technology to capture images of actual blood flow in the lower extremity vessels for visualization of areas of patency, stenosis, or occlusion.
Other diagnostic procedures include skin perfusion pressure, pulse volume recordings, magnetic resonance angiography, computed tomographic angiography, and multidetector (McNichol et al., 2022).
The primary cause of arterial insufficiency is atherosclerosis or arteriosclerotic vascular disease ("hardening of the arteries") due to plaque buildup and damage to arterial walls. Risk factors associated with PAD include the following:
Smoking
Hypertension
Obesity
Diabetes mellitus
High blood cholesterol
Physical inactivity
Age over 50
African American ethnicity
History of stroke
Heart disease
Other vascular diseases
Common symptoms of PAD include:
A "crampy" type of leg/foot pain in the muscles (not joints) that is worse with walking (early symptom).
Pain at rest when feet are elevated and improves when the foot is in a dependent position (late effects of PAD).
Cooler skin temperature of the lower extremities compared to the rest of the body.
Chronic venous insufficiency (CVI) remains the most common etiology of chronic wounds of the lower extremities, accounting for up to 80% of all leg ulcers. Although more commonly associated with older individuals, over 20% of venous leg ulcers (VLUs) occur in those under 40 years old, and almost 13% of VLUs develop in people under 30 years old (Wound, Ostomy, and Continence Nurses Society, 2017). Leg ulcers due to CVI tend to be shallow, irregularly shaped, indurated, or erythematous and often have macerated wound edges or periwound skin surrounding the ulcer. These wounds tend to be on the lower extremities over the fleshy parts of the legs, usually in the area just above the ankle to several inches below the knee. The lower leg area between the ankle and the knee is called the "gaiter" area because gaiters are protective clothing covering the shoe and lower pants leg. In the early 19th century, someone who could not afford regular riding boots for riding horses used leather 'gaiters' to protect the ankles and the lower leg below the knee. The lower leg area, about one handbreadth below the knee to just above the ankles, may display darkly discolored skin pigmentation. The darkening of the gaiter area of the leg is called hemosiderin staining; this is due to fluid leaking from the blood vessels into the interstitial spaces of the lower extremity tissues. Red blood cells die in the interstitial spaces and release hemoglobin (iron-carrying component), which is engulfed by macrophages (white blood cells responsible for "clean up" in the body). Macrophages break down hemoglobin, leaving hemosiderin in the tissue spaces, which discolors the tissues. Other skin changes frequently associated with VLUs include eczematous changes, lipodermatosclerosis (thickening and hardening of the tissue), purpura (small purple spots usually 4-10 mm in diameter just beneath the skin or in the mucous membranes due to small blood vessels bursting), and atrophy blanche, which is white to ivory colored scarring of tissue typically due to healed ulcers or vascular inflammation associated with livedoid vasculopathy (Marin & Woo, 2017).
In CVI, one or both legs typically demonstrate "pitting" edema. Pitting edema indicates an increase in interstitial fluid trapped in the tissues of the dependent extremities. With pitting edema, the skin will retain an indentation when pressure is applied by pressing down with your thumb (usually over the tibia). Pitting edema is usually documented with a 'plus' system: 1+ demonstrates an indentation of 2 mm, which rebounds quickly; 2+ demonstrates an indentation of 4 mm, which does not immediately rebound; 3+ demonstrates an indentation of 6 mm, which takes at least ten seconds to rebound, and 4+ demonstrates an indentation of 8 mm or more which takes more than 20 seconds to rebound (Wound, Ostomy, and Continence Nurses Society, 2017).
Venous insufficiency is caused by valvular incompetencies (or blockages) of the lower extremity deep veins, decreasing the efficacy of the venous return portion of the circulatory system and allowing the pooling of fluid in the dependent lower extremities. Varicose veins may be evident in one or both legs, but are not required to diagnose venous insufficiency. Risk factors for venous insufficiency include obesity, pregnancy, previous pelvic or leg surgery, frequent and prolonged periods of standing or sitting, inactivity, older age, history of deep vein thrombosis (clot), and genetics. Typical symptoms of venous insufficiency include swelling in the lower extremities below the knees, itching of the skin, dull aching or "heavy" feeling in the lower legs, and pain that worsens when standing for long periods. In advanced cases, the skin of the lower extremities in the gaiter area may demonstrate hemosiderin staining, as well as thickening and hardening of the tissue (lipodermatosclerosis). Edema and pain in the lower legs associated with venous insufficiency usually improve when the legs are raised to a heart level or higher for a period or when compression garments are utilized (Johns Hopkins Medicine, n.d.).
Clinical Pearl and Additional Resources: Scientific literature suggests that mixed venous and arterial disease occurs in up to 25% of all venous insufficiency cases (Marin & Woo, 2017). Arterial blood flow to lower extremities should be evaluated in all venous insufficiency cases (check both lower extremities' pulses, obtain at least a screening ABI, toe pressures, or Doppler studies if necessary). Studies indicate that lymphedema is often a contributing factor to lower extremity edema and wounds and is often overlooked in venous insufficiency cases. This course will not specifically address lymphedema; please see the CEUFast, Inc. course on lymphedema.
Over 40 million individuals in the United States were reported to have diabetes (12% of the population). An additional 115 million people may be classified as having "prediabetes" (blood sugar or hemoglobin A1C levels are elevated but not high enough to be diagnosed with diabetes), which increases their risk of developing type II diabetes, stroke, and heart disease. It is estimated that almost 30% of individuals over 65 have diabetes (American Diabetes Association, n.d.). More recently, it was estimated that 25% of all people with diabetes would develop a diabetic foot ulcer (DFU) in their lifetime. About 85% of all lower-extremity amputations in people with diabetes occur due to DFUs that become infected, and up to 70% of diabetic patients who have an amputation related to a DFU die within five years after the amputation (Mavrogenis et al., 2018).
Diabetes is a group of diseases characterized by high glucose levels in the blood caused by abnormalities in insulin production or insulin action. Abnormally elevated blood sugar levels cause many changes in the human body, particularly in the microvasculature and nerve function. Over time, it is estimated that at least many people with diabetes will develop some degree of nerve damage; this nerve damage can occur in almost every organ of the body. Often, this damage causes few noticeable symptoms, but if a person does develop symptoms, one of the most frequently seen is peripheral neuropathy. Symptoms of diabetic peripheral neuropathy (DPN) may include numbness or tingling in the feet, legs, arms, or hands. It may also cause burning or pain in the extremities. The longer an individual has the disease, and the more inadequate the diabetes control (blood sugars above normal), the more likely nerve damage will occur and cause some symptoms (Sapra & Bhandari, 2023). Impaired sensation in the feet occurs in 30% of people with diabetes who are 40 years old or older. A decreased sensation is the leading cause of foot ulcerations in diabetics, which leads to non-traumatic amputations of the lower extremities. The most common causes of foot ulcerations in people with diabetes are peripheral neuropathy, ischemia, minor trauma, and foot deformities (Mavrogenis et al., 2018).
Prevention activities are paramount for all healthcare providers. The CDC (2011) states, "Comprehensive foot care programs such as those that include risk assessment, foot-care education and preventive therapy, treatment of foot problems, and referral to specialists, can reduce amputation rates by 45% to 85%." Preventive approaches include foot visual inspection (with socks removed, including the plantar aspect of both feet), assessment of lower extremity pulses, and screening for sensory changes of the lower extremities, which should be conducted at least annually but are recommended at every primary care and diabetes care visit.
Clinical Pearl: The standard screening examination for DPN is the Semmes Weinstein 5.07 gauge 10-gram monofilament examination (Dunker et al., 2023). This exam is performed by holding the monofilament against the skin of the foot (for one second) at a perpendicular angle and with only enough pressure to cause a slight bowing of the monofilament. Care must be taken not to apply the monofilament over callused skin, as callus areas do not have the sensation of normal skin. The patient keeps their eyes closed during the exam and tells the examiner when they feel the monofilament touching their skin. Originally, monofilament testing was intended to be done by touching 8-10 points on each foot. However, studies revealed that a 4-touch-point-per-foot process (two toes and the first and third metatarsal heads) had 90% to 93% sensitivity and took less than one minute to complete. Smeija et al. (1999) suggest, "Foot care providers with the time to perform a complete examination may reasonably choose to do so." Any failure to sense the monofilament indicates the patient is at risk of foot ulceration and amputation. Neurological examination for DPN may include vibratory sensation with a 128-hertz tuning fork and cold-warm discrimination assessment. Preventive education and special protective footwear are critical for all diabetics, especially those who exhibit altered sensations in one or more areas of either foot (Mavrogenis et al., 2018).
Image 10: Monofilament Screening
When sensation in the feet changes over time, it may not be perceived by the diabetic, and they may obtain tighter-fitting shoes because their old shoes do not feel snug anymore. They may not be able to sense areas of rubbing or mechanical irritation. If special protective footwear is not initiated for these individuals, they may experience blisters or alterations in skin integrity. Any alteration in skin integrity in a person with diabetes is dangerous, even small cracks in the heel from dry skin. In addition, diabetics with peripheral neuropathy are likely to experience multiple small fractures of the bones of the feet (many times without severe symptoms) and eventually develop a Charcot foot deformity, where the foot significantly changes shape and is at great risk of eventual amputation. Any person with diabetes who develops sudden redness, swelling, warmth, pain, or soreness in the foot should have an X-ray and prompt treatment of any fracture.
To differentiate DFUs from venous or arterial ulcers, clinicians need to ascertain if there are any sensory changes to the foot/feet. Ulcers in people with diabetes tend to develop in areas of trauma or repeated mechanical irritation, cracks in the heels and callus formation, especially on the plantar aspect of the foot, large toe, 2nd and 5th metatarsal heads, bunion areas (hallux valgus of the 1st metatarsal head at the base of the big toe) and over any foot or toe deformity such as hammertoes (contracture of the 2nd, 3rd, 4th, or 5th toes). Because people with diabetes often have comorbid microvascular changes, arterial insufficiency may also occur in conjunction with peripheral neuropathy. Adequate blood flow is necessary for optimal wound healing; therefore, vascular assessment and evaluating tissue perfusion and sensation of the feet are imperative to determine the most significant wound etiology and develop appropriate treatment plans (Mavrogenis et al., 2018). Tissue perfusion in a foot with a DFU can be measured by toe pressure, Doppler ultrasound, or TcPO2 (as mentioned above in the arterial insufficiency section). A toe pressure of < 50 mmHg in the foot with a DFU indicates severe limb ischemia. Similarly, in a foot with warm, pink skin, a capillary refill time of > 5 seconds or delayed discoloration may indicate poor arterial perfusion. Any diabetic patient with a DFU and any symptoms of limb ischemia should be referred immediately to vascular services since limb ischemia in a person with diabetes is limb-threatening and possibly life-threatening (Mavrogenis et al., 2018).
Additional Clinical Resources: The Wound, Ostomy, Continence Nurses’ Society published a nice clinical resource guide to venous, arterial, and neuropathic lower-extremity wounds in 2019. It is available here. See also the free access article by Bowers & Franco.
Chief complaint: Wound on the right lower leg that has not healed for six months.
Possible etiologies and current treatments: He thinks he originally injured the area by accidentally hitting the edge of his dishwasher when it was open. He reports that he cleaned the wound immediately with soap and water, then applied hydrogen peroxide. He reports that he and his wife have been washing it with tap water daily, applying an over-the-counter non-stick pad, and securing it with paper tape. He has not used anything else on the wound. He states it seemed better for the first few weeks but has now been exactly the same for over four months, "maybe with a little redness at the edges."
Past medical history/comorbid conditions and physical limitations: A review of the history and physical assessment of Mr. Smith reveals he has a history of diabetes, hypertension, and high cholesterol. His most recent labs (a basic metabolic panel and complete blood count (CBC) two months ago) were all within normal limits, including his last glycosylated hemoglobin (hemoglobin A1c), which was 6.5% two months ago, indicating adequate glycemic control. The American Diabetes Association recommends that people with diabetes maintain an A1c level of 6.5% to 7% to minimize diabetes complications.
Allergies: Mr. Smith reports no known allergies.
Vaccination history: Mr. Smith's medical record indicates he is up to date on his immunizations, including a tetanus vaccination five years ago.
Social and dietary history: He states he has a high school education, and his wife is his caregiver, but he drives himself to his healthcare visits. He reports that he and his wife have changed the wound dressings daily. He reports having a good appetite and eating three meals per day with a hand-sized portion of protein at each of these meals, plus two small snacks (usually a handful of almonds or 3-4 peanut butter crackers or wheat crackers and cheese).
Medications: He is on standard medication for his hypertension (an angiotensin-converting enzyme [ACE inhibitor]), a statin for his high cholesterol, and an oral diabetes medication (a biguanide). He denies taking any over-the-counter medications recently (such as NSAIDs). He reports taking these medications as ordered for over two years with no recent dosage changes.
General exam and vital signs: General impression is a 68-year-old male who appears his stated age. He is neatly dressed, and his appearance suggests good daily hygiene. His skin is thin and somewhat dry, with a leathery appearance on sun-exposed surfaces. His vital signs today are as follows: Oral temperature is 98.8 degrees Fahrenheit, blood pressure is 128/70, radial pulse is 72 beats per minute, respirations are 18 per minute and appear unlabored. He weighs 175 pounds and is 5'9" (BMI = 25.8," Overweight").
Wound assessment: Mr. Smith has a full-thickness wound on the right lateral lower extremity, just above the ankle, measuring 2.5 cm in length, 2.5 cm in width, and 0.4 cm in depth. The wound bed is 100% pale pink and slightly dry. Drainage is a scant amount of clear yellow fluid with no remarkable odor. The surrounding skin is clear and intact, with slight erythema noted where the tape secured the dressing to the surrounding skin. Furthermore, the wound is noted to have a "punched out" appearance. Sparse hair growth is noted on both lower legs, and the skin's general appearance on the lower extremities is taut and somewhat shiny. There is no noticeable edema. The skin of his feet and toes feels slightly cooler to the touch than the rest of his body. Mr. Smith is also noted to have a hard callus over the plantar aspect of the 2nd metatarsal head on his right foot, but no open wound or drainage was noted in this area.
Pain and sensation: Mr. Smith also demonstrates decreased sensation in the plantar aspect of both feet. A 10-gram Semmes Weinstein monofilament examination (SWME) of at least 3 points (the plantar aspect of the big toe, 3rd metatarsal, and 5th metatarsal) is used in diagnosing DPN. Some texts recommend 4-10 sites for this test on each foot (1st, 3rd, and 5th toes and metatarsal heads, medial and lateral foot, and dorsal surface between 2nd toe and great toe). The SWME has a positive predictive value of 87% to 100% (95% CI of 74% to 100%). Mr. Smith demonstrated decreased sensation in two out of four touchpoints, indicating he is at risk for DFU and amputation and a need for protective footwear. Most DFUs occur on the plantar aspect of the feet, particularly over the metatarsal heads and heels. These are frequently (but not always) preceded by callus formation (Mavrogenis et al., 2018). Mr. Smith reports wearing "loafers" at home most of the time and is wearing sneakers today.
Pulses: Capillary refill of his toes seems to be around three seconds or slightly more sluggish in the toes of the right foot. Both left and right pedal pulses and PT are very weak and difficult to palpate (the left is slightly stronger than the right). An ABI is performed, revealing an ABI on the right of 0.70 and on the left of 0.85. An ABI of less than 0.9 indicates mild arterial insufficiency, an ABI of less than 0.8 indicates moderate arterial insufficiency, and an ABI of less than 0.6 indicates severe arterial insufficiency (ischemia). If ABI results were over 1.2, one would expect a falsely elevated value due to decreased blood vessel elasticity, which may occur in people with diabetes and atherosclerotic changes. In that case, we would have considered TcPO2 tests (requiring expensive equipment) or simple toe pressures as the screening test of choice (toe systolic blood pressure of at least 40 mmHg would indicate adequate arterial blood flow to the lower extremity).
Given the above clinical information, Mr. Smith's open full-thickness wound on his right lower leg just above the ankle is most likely a non-healing ulcer with some arterial insufficiency. However, it is also likely complicated by his diabetes and the type of wound care he has been performing over the last six months (see another CEUFast, Inc. wound course for evidence-based wound dressing selection tips). Besides his diabetes potentially impairing his wound healing, the fact that he has kept the wound bed mostly dry and just covered it with a non-stick pad daily may have impaired wound healing (moist wound beds tend to improve faster than dry wound beds).
Clinical Pearl: Diabetes affects the human body's sensory, motor and autonomic factors, which may impair wound healing.
Sensory factors: include hyperglycemia disrupting myelin sheaths (which protect nerves). This demyelination can slow down nerve conduction and impair sensory perception.
Motor factors: Diabetes is also known to increase atrophy of the foot muscles and may cause contractures of the Achilles tendon and subluxation of metatarsophalangeal joints, resulting in foot deformities and gait abnormalities.
Autonomic factors: Diabetes is associated with loss of some vasomotor control, impaired skin microvascular perfusion, bone flow hyperemia, and arterial-venous shunting, which may lead to anhidrosis, skin fissure formation, fungal skin and toenails, peripheral edema, callus formation, and Charcot formation.
Other factors that may impair wound healing in diabetic foot ulcers may be related to the chronic wound microbiome or bacterial load in the diabetic foot (Weir & Schultz, 2022)
Mr. Smith's plantar callus indicates a diabetic neuropathic etiology and requires immediate preventive attention (offloading shoes) before additional ulcer development in this area. If the open wound were on the plantar aspect of his foot, especially over a callused or insensate area such as a metatarsal head, the etiology would most likely be DPN. If the wound was over a toe in a person with diabetes, it could likely be a mixed etiology (peripheral neuropathy and arterial insufficiency) unless a clear mode of injury could be established in a foot with strong pulses or good toe pressures but sensory impairment.
Recommendations for Mr. Smith could include referral to a wound specialist, podiatrist, or vascular specialist. In the meantime, reinforce that Mr. Smith has been doing very well at his medication and diet compliance, complimenting him and his wife for trying to walk a mile 2-3 times per week. Studies indicate progressive walking may improve peripheral arterial circulation and claudication symptoms (Treat-Jacobson et al., 2019). Key components for any treatment plan for Mr. Smith should include addressing his arterial insufficiency and evaluating it further, addressing wound care principles and wound care education with the patient and his wife, and asking him to record his fasting blood sugars daily for two weeks (people with diabetes may see a rise in their blood sugars as one of the first indicators of infection). Recommendations may also include repeating labs that will check his CBC (looking for anemia and any elevation of white blood cells), zinc and vitamin D levels (deficiencies may impair wound healing), and prealbumin (prealbumin is a serum biomarker of nutritional status) of < 20 may indicate a higher risk of impaired healing or infection (Salvetti et al., 2018).
Chief complaint: Mrs. Watson is a 68-year-old non-smoking female seen in urgent care for worsening edema of both legs and a large open wound on her right leg of six months' duration.
Possible etiologies and current treatments: Mrs. Watson reports she does not know what caused the wound. She denied any injury and reported that it appeared on her right leg one day as a quarter-sized sore that has since grown. Her edema has gotten worse, too. She states she has been wrapping gauze around her legs a few times daily and trying to stay off her feet. She says she sits at home with her legs under a desk, sewing.
Describe past medical history/comorbid conditions and physical limitations: Mrs. Watson is overweight with a BMI of 35 and a history of hypertension and hypothyroidism. Other than hypertension (well-controlled), she has no known history of cardiovascular disease or congestive heart failure (CHF). Mrs. Watson reports she has had "problems with swelling in my legs for a few years." She says the swelling worsens as the day progresses, but improves when she first wakes up or when she keeps her legs elevated for several hours. She reports she has not been wearing her compression stockings, which her primary care provider ordered last year because she could no longer pull them on herself. She denied any recent fever, chills, or severe pain.
Allergies: Allergic to bananas and has a possible latex allergy (gets a rash).
Vaccination history: Current vaccinations are up to date, except there is no record of recent tetanus vaccines within the past ten years.
Social and dietary history: Non-smoker, widow, lives alone with two cats. Reports eating two meals daily (heavy carbohydrates and low in protein) and frequent snacks (more carbohydrates like cookies and chips with occasional fruit).
Medications: Beta-blockers for hypertension and levothyroxine for hypothyroidism. The patient reports rarely missing any doses.
General exam and vital signs: Overweight appearing female who looks slightly older than 68 years. Walking with an unsteady gait and a slightly disheveled appearance, with a musty odor noted.
Vital signs: Temperature is 98.6 degrees Fahrenheit, a radial pulse is 88 beats per minute, blood pressure is 138/84, and respirations are 22 per minute. Height is 5'3 "; weight is 200 lbs.
Wound assessment: The exam reveals a 5 cm in length by 4 cm in width by 0.2 cm deep wound on the anterior-lateral aspect of her right lower leg above the ankle but below the knee in the gaiter area of the leg. The wound bed is 80% red/viable tissue and 20% scattered yellow, loose slough/non-viable tissue (resembles chicken fat). The skin around the wound is macerated (white edges from excessive moisture), and a moderate amount of clear/serous wound drainage is noted to have saturated the gauze wrap and dressing that was removed from the wound, which Mrs. Watson says has only been on the wound for a few hours. In addition, Mrs. Watson has 2+ pitting edema bilaterally, and the skin on her legs appears tight with a brownish discoloration noted (hemosiderin staining) to the skin just above the ankles to about one handbreadth below the knees bilaterally. The skin temperature of her feet and toes is warm but not warmer than the skin of the rest of her body, and no unusual erythema is noted in either lower extremity. She also reports that the wound on her lower right leg has been "weeping an awful lot," so she must change the bandages frequently/several times daily.
Pain and sensation: Mrs. Watson reports her pain level is a dull "aching pain" that worsens as the day progresses (currently about a 2-3 on a scale of 1-10), but she reports it feels better when her legs are elevated.
Pulses: Bilateral pulses of her lower extremities are all 3+ and equal. Capillary refill is <3 seconds in all toes.
Given the above clinical information, Mrs. Watson's wound is likely a venous leg ulcer due to venous insufficiency. The gold standard treatment includes compression therapy, which the patient states has been ordered for her in the past. She may need to be remeasured for the correct size compression stockings (two pairs every six months is typical), and consideration of zippered stockings or a device that may help her apply them herself could be helpful. A wound specialist consult could address these issues. Recommendations to be considered for Mrs. Watson also include (but are not limited to):
Updating her vaccinations (offering a tetanus vaccine since it has been over ten years).
Dietary consult/patient education addressing nutrition and weight.
Reviewing her medical records or evaluating labs for recent CBC, any nutritional deficiencies (e.g., serum zinc, vitamin D, B-12), and current thyroid hormone levels (under-treated hypothyroidism is linked to poor wound healing).
Evaluating her wound care and hygiene practices (does she know she can remove the dressing and get in the shower?).
Patient education (help develop an exercise plan; review venous insufficiency contributing factors such as sitting long periods, dependent feet, lack of calf-pumping movement, and the need for compression (on in the morning and off at night when going to bed).
Appropriate wound dressings under compression that will promote wound healing and help manage periwound maceration (if any treatment is started, she should be re-checked in 2 weeks, and if the wound has not improved, other etiologies could be considered, as well as more in-depth evaluation related to possible infection and compliance with treatment/compression).
Wounds of the lower extremities may have several characteristics of any of the above in combination.
For instance, diabetics may also have venous insufficiency, or diabetic ulcers often have some degree of ischemia/arterial insufficiency.
Here is a picture of a DFU in an uncommon area of the foot due to repetitive trauma from a misfitting new shoe. It is primarily a DFU because the etiology is from repetitive trauma. Still, some mixed etiology is suspected since people with diabetes often have mixed arterial disease as well, and this would impair wound healing. Although this wound does have somewhat of a "punched-out" appearance, the "primary etiology" is not suspected as arterial. The patient's history and other assessment information could help make that diagnosis, such as type 2 diabetes with recent HbA1C of 7.4 and diabetic neuropathy, overall assessment of the wound and bilateral lower extremities, ABI results, toe brachial index, and the wound location matched exactly an area in the shoe that was defective. In addition, drainage from the wound and the wound bed appearance help with diagnosis.
This brief course does not discuss atypical etiologies for non-healing lower extremity wounds. Still, they may include pyoderma gangrenosum, vasculopathy, allergic dermatitis, previous injury with retained foreign body, insect bite, parasitic involvement, or even cancer (to name a few).
Tips to help determine if an atypical etiology may be present include: Wounds with atypical etiologies may not respond to common treatment for the above wounds. They may be more likely in persons with autoimmune diseases or a history of cancer. They may worsen with mechanical or sharp debridement. Example: Pyoderma gangrenosum may be considered in wounds where other etiologies have been ruled out or a more complicated etiology is suspected.
Pyoderma gangrenosum is an ulcerative disorder classified as a neutrophilic dermatosis. It is not an infection and, despite the name, has no connection with gangrene. Pyoderma wounds are often found on the lower extremities and often present with a rapid progression of a very painful cutaneous ulcer with irregular, violaceous (purple to bluish) wound edges, which may have some undermining. The history of the wound may be suggestive of pathergy or cribriform scarring. When these wounds are present on the lower extremity, they are often misdiagnosed as VLUs.
The patient may have a history of autoimmune or inflammatory systemic diseases associated with pyoderma gangrenosum (e.g., inflammatory bowel disease such as ulcerative colitis or Crohn's disease, rheumatoid arthritis, etc.).
Histopathologic findings may suggest sterile dermal neutrophilia, with or without lymphocytic vasculitis and mixed inflammation.
When the patient is treated with topical and/or systemic steroids, Pyoderma wounds tend to improve rapidly (Schmieder & Krishnamurthy, 2023).
Although this course focused on lower extremity wound assessment and diagnosis (and not wound treatment, which is covered in another course), general wound management basics to consider concerning lower extremity wounds include the following (Armstrong & Meyr, 2022; Bryant & Nix, 2023; Sibbald et al., 2021; Tran et al., 2023):
Determine what the patient's concerns and goals are regarding the following:
Pain
Odor management
Exudate management
Mobility
Self-care ability
Healing versus palliative care
Address etiological factors (control comorbid disease and minimize or eliminate causative factors).
Determine if there is an adequate blood supply to the wounded area.
Identify potential impediments to wound healing (systemic and local factors).
Prevent recurrent trauma to the insensate foot.
Offload pressure.
Reduce potential friction and shearing forces.
Protect skin from excessive moisture (e.g., incontinence, sweat).
Provide therapeutic compression to improve venous return when appropriate.
Evaluate and re-evaluate the rate of healing at regular intervals. Wounds that show no improvement in two weeks should be re-evaluated, and possibly additional diagnostic tests should be considered, evaluate for differential diagnoses, or change wound management orders and re-evaluate in another two weeks. Consider the need for a biopsy and/or referral to specialists as appropriate.
Provide systemic support to address potential cofactors and modifiable impairments to wound healing.
Control blood glucose levels.
Provide adequate hydration.
Optimize nutrition.
Reduce edema.
Promote blood flow and adequate oxygenation/perfusion (avoid the cold, control pain, eliminate nicotine/smoking and caffeine).
Reduce medications or treatments that may impair wound healing (when applicable and feasible).
Optimize the local wound environment to promote healing.
Eliminate dead space but avoid overpacking open wounds.
Maintain an appropriate level of moisture.
Cleanse wound and maintain a clean wound bed free of external contaminants.
Remove non-viable tissue (debridement).
Prevent and manage bioburden; remove biofilm.
Control odor.
Eliminate or minimize pain.
Protect wound bed and periwound skin (e.g., from excessive moisture, disruptive dressing materials, cytotoxic wound cleansers, tape trauma, etc.).
Assess and treat wounds for infection/biofilm/inflammation.
In addition, as a reminder, it is good clinical practice to include in your documentation your assessment findings, the treatment plan ordered (and your rationale), what type of debridement was performed (if warranted), and the patient's response to it, your education of the patient and any caregiver, and what follow-up is planned. Assure adequate follow-up frequency for wounds and provide written instructions to the patient/caregiver on when to call (and who) if the wound worsens or does not improve.
This concludes a fundamental review of the three most common etiologies for lower extremity ulcers (diabetic neuropathy, venous, and arterial insufficiency). Other etiological considerations, such as bites/stings, burns, calciphylaxis, malignant wounds, mycoses, lymphedema, lipedema, vasculitis, pyoderma gangrenosum, and other atypical/unusual etiologies, may be discussed in more detail in future wound modules.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
American Diabetes Association. (n.d.). Statistics About Diabetes. American Diabetes Association. Visit Source.
Arputhanathan, H., Hyde, J., Atilola, T., Queen, D., Elliott, J., & Sibbald, R. G. (2022). A patient navigation model to improve complex wound care outcomes. Advances in skin & wound care, 35(9), 499–508. Visit Source.
Armstrong, D. & Meyr, A. (2022). Basic principles of wound management. UpToDate. Visit Source.
Betz, J. (2022). Chapter 3: Wound healing. In McNichol, L., Ratliff, C., & Yates, S. (Eds.), Wound, Ostomy, and Continence Nurses Society Core Curriculum: Wound Management (2nd ed.). (pp. 40-52). Wolters-Kluwer, LWW: Philadelphia.
Bohn, G. & Bryant, R. (2023). Chapter 8: Wound-healing physiology and factors that affect the repair process. In Bryant, R. & Nix, D. (Eds.), Acute and Chronic Wounds: Intraprofessionals from Novice to Expert (6th ed.). (pp. 143-158). Elsevier Limited (UK).
Bonham, P. (2022). Chapter 25: Assessment and management of patients with wounds due to lower extremity arterial disease (LEAD). In McNichol, L., Ratliff, C., & Yates, S. (Eds.), Wound, Ostomy, and Continence Nurses Society Core Curriculum: Wound Management (2nd ed.), 493-531. Wolters-Kluwer, LWW: Philadelphia.
Bonham, P. A., Brunette, G., Crestodina, L., Droste, L. R., González, A., Kelechi, T. J., Ratliff, C. R., & Varnado, M. F. (2022). 2021 Guideline for Management of Patients With Lower-Extremity Wounds Due to Diabetes Mellitus and/or Neuropathic Disease: An Executive Summary. Journal of wound, ostomy, and continence nursing : official publication of The Wound, Ostomy and Continence Nurses Society, 49(3), 267–285. Visit Source.
Bowers, S., & Franco, E. (2020). Chronic wounds: evaluation and management. American family physician, 101(3), 159–166.
Brace, J.A. (2023). Chapter 20: Wound debridement. In Bryant, R. & Nix, D. (Eds.), Acute and chronic wounds: Intraprofessionals from novice to expert (6th ed.). (pp. 430-438). Elsevier Limited (UK).
Bryant, R. & Nix, D. (2023). Acute and chronic wounds: Intraprofessionals from novice to expert (6th ed.). (pp. 143-158). Elsevier Limited (UK).
Centers for Disease Control and Prevention (CDC). (2011). National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States. Atlanta (GA): US Department of Health and Human Services, Centers for Disease Control and Prevention. Visit Source.
Davis, M., & Hom, D. (2023). Current and Future Developments in Wound Healing. Facial plastic surgery: FPS, 39(5), 477–488. Visit Source.
Dunker, Ø., Uglem, M., Bu Kvaløy, M., Løseth, S., Hjelland, I. E., Allen, S. M., Dehli Vigeland, M., Kleggetveit, I. P., Sand, T., & Nilsen, K. B. (2023). Diagnostic accuracy of the 5.07 monofilament test for diabetes polyneuropathy: influence of age, sex, neuropathic pain and neuropathy severity. BMJ open diabetes research & care, 11(6), e003545. Visit Source.
Ermer-Seltun, J.M. & Rolstad, B.S. (2022). Chapter 8: General principles of topical therapy. In McNichol, L., Ratliff, C., & Yates, S. (Eds.), Wound, Ostomy, and Continence Nurses Society Core Curriculum: Wound Management (2nd ed.) (pp. 136-155). Wolters-Kluwer, LWW: Philadelphia.
Hurlow, J. & Kalan, L. (2022). Chapter 19: Wound infection and bioburden: Detection and management. In McNichol, L., Ratliff, C., & Yates, S. (Eds.), Wound, Ostomy, and Continence Nurses Society Core Curriculum: Wound Management (2nd ed.) (pp. 411-429). Wolters-Kluwer, LWW: Philadelphia.
Majno, G. (1975). The healing hand: Man and wound in the ancient world. Cambridge (MA): Harvard University Press.
Marin, J. A., & Woo, K. Y. (2017). Clinical characteristics of mixed arteriovenous leg ulcers: A descriptive study. Journal of wound, ostomy, and continence nursing: Official publication of The Wound, Ostomy and Continence Nurses Society, 44(1), 41–47. Visit Source.
Mavrogenis, A. F., Megaloikonomos, P. D., Antoniadou, T., Igoumenou, V. G., Panagopoulos, G. N., Dimopoulos, L., Moulakakis, K. G., Sfyroeras, G. S., & Lazaris, A. (2018). Current concepts for the evaluation and management of diabetic foot ulcers. EFORT open reviews, 3(9), 513–525. Visit Source.
McNichol, L., Ratliff, C., & Yates, S. (2022). Chapter 23: Differential assessment of lower extremity wounds. In McNichol, L., Ratliff, C., & Yates, S. (Eds.), Wound, Ostomy, and Continence Nurses Society Core Curriculum: Wound Management (2nd ed.) (pp. 446-452). Wolters-Kluwer, LWW: Philadelphia.
Mervis, J. S. (2025). The Impact of Chronic Wound Exudate on the Patient, Clinician and Payer: Addressing the Challenges With Foam Dressings. International wound journal, 22 Suppl 1(Suppl 1), e70369. Visit Source.
Nuutila, K., & Eriksson, E. (2021). Moist wound healing with commonly available dressings. Advances in wound care, 10(12), 685–698. Visit Source.
Oropallo, A. & Quraishi, W. (2023). Chapter 28: Wound pain. In Bryant, R. & Nix, D. (Eds.), Acute and Chronic Wounds: Intraprofessionals from Novice to Expert (6th ed.) (pp. 536-545). Elsevier Limited (UK).
Orsted, H. L., Keast, D. H., Forest-Lalande, L., Kuhnke, J., O’Sullivan-Drombolis, D., Jin, S., Haley, J., & Evans, R. (2017). Foundations of best practice for skin and wound management. Skin: Anatomy, Physiology and Wound Healing. Canadian Association of Wound Care. Visit Source.
Richbourg, L. (2022). Chapter 14: Skin and wound care for the geriatric population. In McNichol, L., Ratliff, C., & Yates, S. (Eds.), Wound, Ostomy, and Continence Nurses Society Core Curriculum: Wound Management (2nd ed.) (pp. 257-277). Wolters-Kluwer, LWW: Philadelphia.
Sharma, S., Mohler, J., Mahajan, S. D., Schwartz, S. A., Bruggemann, L., & Aalinkeel, R. (2023). Microbial Biofilm: A Review on Formation, Infection, Antibiotic Resistance, Control Measures, and Innovative Treatment. Microorganisms, 11(6), 1614. Visit Source.
Salvetti, D. J., Tempel, Z. J., Goldschmidt, E., Colwell, N. A., Angriman, F., Panczykowski, D. M., Agarwal, N., Kanter, A. S., & Okonkwo, D. O. (2018). Low preoperative serum prealbumin levels and the postoperative surgical site infection risk in elective spine surgery: a consecutive series. Journal of neurosurgery. Spine, 29(5), 549–552. Visit Source.
Sapra, A., & Bhandari, P. (2023). Diabetes. In StatPearls. StatPearls Publishing. Visit Source.
Schmieder, S. J., & Krishnamurthy, K. (2023). Pyoderma Gangrenosum. In StatPearls. StatPearls Publishing. Visit Source.
Schorr, E. N., Treat-Jacobson, D., & Lindquist, R. (2017). The relationship between peripheral artery disease symptomatology and ischemia. Nursing research, 66(5), 378–387. Visit Source.
Sibbald, R. G., Elliott, J. A., Persaud-Jaimangal, R., Goodman, L., Armstrong, D. G., Harley, C., Coelho, S., Xi, N., Evans, R., Mayer, D. O., Zhao, X., Heil, J., Kotru, B., Delmore, B., LeBlanc, K., Ayello, E. A., Smart, H., Tariq, G., Alavi, A., & Somayaji, R. (2021). Wound bed preparation 2021. Advances in skin & wound care, 34(4), 183–195. Visit Source.
Tran, D. L., Huang, R. W., Chiu, E. S., Rajhathy, E. M., Gregory, J. H., Ayello, E. A., & Sibbald, R. G. (2023). Debridement: Technical Considerations and Treatment Options for the Interprofessional Team. Advances in skin & wound care, 36(4), 180–187. Visit Source.
Treat-Jacobson, D., McDermott, M. M., Bronas, U. G., Campia, U., Collins, T. C., Criqui, M. H., Gardner, A. W., Hiatt, W. R., Regensteiner, J. G., Rich, K., & American Heart Association Council on Peripheral Vascular Disease; Council on Quality of Care and Outcomes Research; and Council on Cardiovascular and Stroke Nursing. (2019). Optimal Exercise Programs for Patients With Peripheral Artery Disease: A Scientific Statement From the American Heart Association. Circulation, 139(4), e10–e33. Visit Source.
Weir, D. & Schultz, G. (2022). Chapter 11: Assessment and management of wound-related infections. In McNichol, L., Ratliff, C., & Yates, S. (Eds.), Wound, Ostomy, and Continence Nurses Society Core Curriculum: Wound Management (2nd ed.) (pp. 187-209). Wolters-Kluwer, LWW: Philadelphia.
Wound, Ostomy, and Continence Nurses Society. (2019). Venous, arterial, and neuropathic lower-extremity wounds: Clinical resource guide. Wound, Ostomy, and Continence Nurses Society. Visit Source.
Wysocki, A. (2023). Chapter 7: Anatomy and physiology of skin and soft tissue. In Bryant, R. & Nix, D. (Eds.), Acute and Chronic Wounds: Intraprofessionals from Novice to Expert (6th ed.). Elsevier Limited (UK). Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.