This course will be updated or discontinued on or before Tuesday, August 25, 2026
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will know how to identify and respond to Mpox cases.
Objectives
Upon completion of this course, the learner will be able to:
Define Mpox.
Describe the process of Mpox transmission.
Differentiate between Mpox and other differential diagnoses.
Identify complications of Mpox.
Explain recommended treatment for Mpox.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Mpox, previously known as Monkeypox, is an endemic Orthopox virus in West and Central Africa. Mpox is now occurring in other countries, causing major healthcare concerns. Most human Mpox infections are reported from the Congo Basin of the Democratic Republic of Congo (Hughes et al., 2021). Mpox is most commonly found in rural, forested communities with poor sanitation and chronic malnutrition (Beer & Rao, 2019). However, as of March 5th, 2024, since 2022, there have been 32,063 total confirmed Mpox/Orthopoxvirus cases in the United States and a total of 58 deaths (Centers for Disease Control and Prevention [CDC], 2024e). So far, as of August 2024, there have been a total of 1,122 cases reported in the United States (CDC, 2024d).
In November 2022, the World Health Organization (WHO) sent out a news release regarding Mpox. Due to the outbreak expansion over the past year that exposed racist and stigmatizing language, after consultation with several global experts as well as the general public, WHO recommended a new name for “Monkeypox” (World Health Organization [WHO], 2022). “Mpox” was recommended to become the preferred term to replace “Monkeypox” after a period of one year, to allow time for the transitioning of all policies and procedures to reflect the new name as well as for the International Classification of Diseases (ICD) to adopt the new term for medical coding purposes (WHO, 2022).
Mpox cases are being reported sporadically around the world. It is believed to have spread worldwide due to the lack of immunization after the smallpox vaccine was stopped (Grant et al., 2020). Therefore, people who did not receive a smallpox vaccine (those younger than 40-50 years of age) may be susceptible.
Mpox is categorized into 2 genetic clades. These include the genetic clades of West Africa and Central Africa (also called Congo Basin). These clades have epidemiological and clinical differences. The mortality rate of the West African clade, clade 2, is less than 1%, and there is no human-to-human transmission. The Central African clade, clade 1, is more frequent, can have a mortality of up to 11%, and has human-to-human transmission (Singh et al., 2021). Beer and Rao (2019) conducted a systematic review of the research published in English before August 15, 2018. They found an often-quoted 10% mortality rate. This rate came from early 1981-1986 data: 33 deaths out of 338. Data from the Democratic Republic of Congo (DRC) (2001-2013) consistently reported mortality of <5%. Case fatality rate (CFR) from countries with the West African Mpox were mostly 0%. The mortality for the Nigeria outbreak was 2.8%. Six deaths, 4 of whom were immunocompromised, out of 228 suspect cases. The mortality for 47 cases in United States outbreaks was 0%. No deaths have been reported from the April 2018 outbreak in Cameroon or the recent outbreak in the Central African Republic. In reports documenting the cause of death, people in high-risk groups comprised most of the deaths (Beer & Rao, 2019).
As mentioned above, clade 1 occurs regularly in the DRC. However, the current outbreak has become more widespread than any other previous outbreak (CDC, 2024f). As of August 2024, the WHO declared a Public Health Emergency of International Concern (PHEIC) because of the threat that the clade 1 poses to countries around the world (CDC, 2024f). Currently, as of August 2024, there have been no reported cases of clade 1 in the United States (CDC, 2024f).
Because of inconsistencies in healthcare and surveillance systems in rural African settings, Mpox data is incomplete and unreliable (Beer & Rao, 2019). This unreliable data is insufficient for statistical analysis (Beer & Rao, 2019). Due to the clinical overlap and insufficient laboratory availability, varicella-zoster virus (VZV) is often misdiagnosed as Mpox, and the conditions may be co-infected in the same patient (Beer & Rao, 2019; Hughes et al., 2021). There is some suggestion that Mpox is increasing in incidence. Data in more developed countries is more reliable.
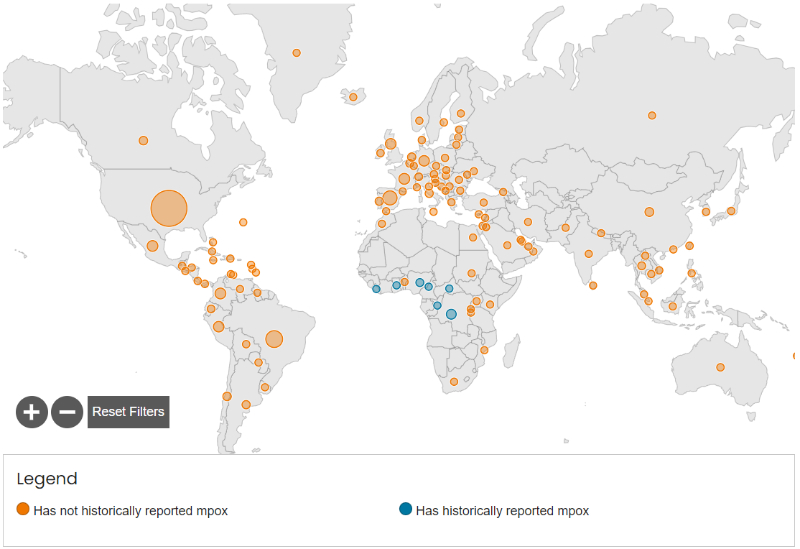
Below is the Mpox Outbreak Global Map with data as of August 6th, 2024, directly from the CDC:
Image 1: Mpox Outbreak Global Map Centers for Disease Control and Prevention (August 6th, 2024)
As included in the legend, the orange circles indicate areas of reported cases of Mpox that historically had not had cases in prior outbreaks. The blue circles indicate areas that had. For more information and specific numbers, feel free to visit here.
Mpox spreads from person to person through direct contact (CDC, 2022a). The transmission mechanisms are respiratory droplets with close and prolonged contact, contact with body fluids, contaminated patient's environment or items, and the rash or scabs of the skin lesion of an infected person. As mentioned above, Mpox can spread from the time symptoms start until the rash has become fully healed with new skin formed over it (CDC, 2022a). As of newer data from February 2023, in some cases, people have been known to spread Mpox to others one to four days BEFORE their symptoms start (CDC, 2022a). Mpox can also be spread through sexual contact. While it is not, by definition, a sexually transmitted infection (STI), it can be more accurately described as a “sexually transmissible” infection, meaning the contact does not have to be exclusively intimate or sexual to be transmitted, as close personal contact can spread the virus (CDC, 2022a). It is important to note that the Mpox virus can be passed to the fetus during pregnancy or to the newborn following birth (World Health Organization [WHO], 2024). Contracting Mpox during pregnancy can lead to the loss of the pregnancy, stillbirth, or death of the infant (WHO. 2024). It can also lead to complications for the mother (WHO, 2024).
Animal-to-human transmission (zoonotic) occurs due to direct contact with the consumption of infected animals or direct contact with the blood, body fluids, and/or lesions of infected animals (The Lancet, 2018). Animals found to transmit Mpox are rodents, rabbits, squirrels, monkeys, porcupines, and gazelles (Singh et al., 2021).
According to the United States case data as of July 25th, 2022, the median age of patients with confirmed Mpox cases is 34 years (CDC, 2023b). The male sex is being the most highly impacted by this outbreak. Of the male patients who provided information on their own sexual activity, 75.1% reported male to male sexual contact (CDC, 2023b). According to the Morbidity and Mortality Weekly Report (MMWR) by the CDC, because the report cases seem to be primarily affecting gay, bisexual, and other men who have sex with men, it is essential that public health programs continue to deliver respectful, harm-reducing, tailored educational and informative messages of strategies of generalized protection that do not create or perpetuate stigma to diverse communities of men who have sex with men (CDC, 2022c). It is important to emphasize that anyone can contract Mpox as it is a public health concern for all.
Mpox is usually a self-limiting disease lasting 2 to 4 weeks (WHO, 2024). The incubation period of Mpox is usually 3 to 17 days (CDC, 2023a). The invasion stage lasts up to 5 days. In this stage, symptoms are fever, intense headache, lymphadenopathy, back pain, myalgia, respiratory symptoms including sore throat, cough, and nasal congestion, and intense asthenia (lack of energy) (CDC, 2022a).
The rash evolves in a set sequence from (WHO, 2024):
Directly from the CDC’s Mpox clinical recognition site, the following collection of pictures include various characteristics of the Mpox rash that are being seen (CDC, 2023a):
Image 2: Mpox Rash Centers for Disease Control and Prevention (August 30, 2023)
For additional photos of the Mpox rash, visit the CDC’s clinical recognition site here.
See below in the following chart for a breakdown of what is being seen with the rash, from enanthem to scabbing (CDC, 2023a):
Table 1: Mpox Rash: From Enanthem to Scab Stages Centers for Disease Control and Prevention (August 30th, 2024)
Stage
Stage Duration
Characteristics
Enanthem
Sometimes, lesions first form on the tongue and in the mouth.
Macules
1-2 days
Macular lesions appear.
Papules
1-2 days
Lesions typically progress from macular (flat) to papular (raised).
Vesicles
1-2 days
Lesions then typically become vesicular (raised and filled with clear fluid).
Pustules
5-7 days
Lesions then typically become pustular (filled with opaque fluid) - sharply raised, usually round, and firm to the touch (deep seated).
Finally, lesions typically develop and depression in the center (umbilication).
The pustules will remain for approximately 5 to 7 days before beginning to crust.
Scabs
7-14 days
By the end of the second week, pustules have crusted and scabbed over.
Scabs will remain for about a week before beginning to fall off.
It is common that areas of lighter or darker skin and/or pitted scars can remain after the rash scabs have healed and fallen off (CDC, 2023a). Once all of the scabs are gone and new skin has covered those spots, the person is no longer contagious (CDC, 2023a).
The number of lesions varies from a few to several thousand (WHO, 2024). The rash is more concentrated on the face and extremities than on the trunk. However, it typically starts in mucosal areas (genital, perianal, oral mucosa). The rash affects the (WHO, 2022):
Face (95% of cases)
Palms of hands and soles of feet (75% of cases)
Oral mucous membranes (70% of cases)
Genitalia (30% of cases)
Conjunctivae (20% of cases)
Additional characteristics to note when identifying Mpox (CDC, 2023a):
The lesions are often being described as painful until the scabs become itchy when they crust over in the healing process.
The rash could be confined to only a few or a single lesion.
They are typically scattered or localized to a body site rather than diffuse all over the body.
The lesions are typically firm or almost rubbery as well as well-circumscribed.
The lesions are often deep-seated with umbilication (a dot on the top of the lesion).
Rectal symptoms are being reported (bloody or purulent stools, pain in the rectum, rectal bleeding).
Lymphadenopathy is a distinctive feature of Mpox compared to other rash-presenting differential diagnoses that may initially appear similar (Grant et al., 2020; WHO, 2024):
Chickenpox
Measles
Smallpox
Bacterial skin infections
Scabies
Syphilis
Medication-associated allergies
VZV skin eruptions usually evolve over 24 hours instead of days, as seen with Mpox, and are seen on the trunk more frequently than Mpox (Singh et al., 2021). Mpox has lesser eruptions than VZV or smallpox. Smallpox is five times more transmissible, has more nausea and vomiting, a less febrile stage before eruptions, more lesions, and a more profound systemic illness (Beer & Rao, 2019).
At this time testing is only recommended if the patient has a rash that is consistent with Mpox (CDC, 2022b).
The polymerase chain reaction (PCR) laboratory test is recommended for accuracy and sensitivity. PCR can be used alone or in combination with sequencing. The recommended specimen type is skin lesion material, including swabs of lesion surface or exudate, roofs from more than one lesion, or lesion crusts. A biopsy is an option, but samples must be stored in a dry, sterile tube with no viral transport media and kept cold. PCR blood tests are usually inconclusive because of the short duration of viremia relative to the timing of specimen collection after symptoms begin and should not be routinely collected from patients (WHO, 2024).
Infection of the cornea with possible loss of vision
Bronchopneumonia occurrence is poorly understood, thought to be a secondary infection, and uncommon (Reynolds et al., 2017).
Hypoalbuminemia and low hematocrit, suggesting malnutrition, were found in patients hospitalized with Mpox during the 2003 outbreak in the United States (Reynolds et al., 2017). This finding may be due to oral lesions and cervical lymphadenopathy. Malnutrition is a common problem that contributes to the severity of Mpox patients in rural Africa (Reynolds et al., 2017).
Mpox lesions on the cornea can lead to conjunctivitis, keratitis (inflammation of the cornea), or loss of vision (CDC, 2022e). This is being termed “ocular Mpox” by the CDC (CDC, 2022e). Although it is fortunately rare, this serious ocular complication requires that healthcare professionals are aware of this sight-threatening condition (CDC, 2022e). Patients who are showing the signs and symptoms of ocular Mpox must be considered for emergency ophthalmologic evaluation and treatment, if necessary (CDC, 2022e). For patients with active Mpox infection, it is essential to decrease the risk of Mpox transfer to the eye (CDC, 2022e). Patients should be advised to practice good hand hygiene and avoid touching their eyes (CDC, 2022e). In the case in which a patient typically wears contact lenses, the CDC recommends that patients refrain from using contact lenses during an active infection (CDC, 2022e).
It is also important to note that children aged eight years of age and younger are at a higher risk for Mpox complications (Zimmerman & Curtis, 2022). Children with Mpox are being reported as having an increased hospitalization rate and having an increased risk for complications including bacterial superinfections, cellulitis, pneumonia, abscesses, and sepsis (Zimmerman & Curtis, 2022).
There are no standard guidelines for the treatment of Mpox at this time (CDC, 2024a). Reynolds et al. (2017) recommend symptomatic support, fever, and pain management, measures to prevent secondary skin infection, adequate hydration and nutrition, protecting vulnerable anatomical locations such as the eyes, and managing complications. The skin and mucosal lesions require care. A serious rash can lead to dehydration, protein loss, and secondary infection. Focal inflammation of the lymphatic system and lung congestion can affect oxygenation and decrease food and fluid ingestion.
The following drugs are currently stockpiled for use from either the Strategic National Stockpile (SNS) or the Study of Tecovirimat for Mpox (STOMP) as options for treatment (CDC, 2024a; CDC, 2024c; WHO, 2024; Zimmerman & Curtis, 2022):
Tecovirimat (TPOXX) is an antiviral approved by the United States Food and Drug Administration (FDA) for the treatment of smallpox in adults and in children as well. It should be considered first for treatment for patients who require more than supportive care. Oral TPOXX is primarily available through STOMP. Clinical trials have found it to be safe with minor side effects. It is available in pill or injection forms. Currently, it is only recommended for those with severe Mpox disease or for those who are at an increased risk of severe disease. High-risk populations for Mpox include children under the age of eight years, children with underlying skin conditions, immunocompromised individuals, pregnant women, healthcare workers with increased risk of exposure, and sex workers of any gender.
Brincidofovir (CMX001 or Tembexa) is an antiviral approved by the FDA for the treatment of human smallpox in adults and children, including neonates. This drug is made available from the SNS to clinicians who obtain an FDA-authorized single-patient emergency use IND. This can be obtained for patients with positive Mpox viral testing and who meet additional criteria set by the FDA.
Smallpox vaccination has been shown to be about 85% effective in preventing Mpox or resulting in a milder illness if it is not prevented (WHO, 2024). The Centers for Disease Control and Prevention (CDC) suggests a smallpox vaccine to be administered within fourteen days of exposure, though preferably within 4 days, for healthcare workers and others exposed to Mpox cases. Vaccinia immune globulin (VIG) has not shown adequacy in treatment or prophylaxis.
Those who are most at risk for Mpox exposure should, ideally, be vaccinated (CDC, 2024b). Vaccinations should also be utilized after exposure to help to prevent contracting Mpox (CDC, 2024b). ACAM2000 and JYNNEOS (Imvamune or Imvanex) are the two vaccines in the United States that can be used to prevent smallpox (CDC, 2024b).
ACAM2000 is a live virus that is inoculated into the skin by pricking the skin surface (CDC, 2024b). After it has been inoculated, a lesion is meant to develop at that site. Because the virus is growing and can spread from that site, individuals who receive this vaccine must take precautions to prevent spread of the vaccine virus until they are considered fully vaccinated in 28 days (CDC, 2024b). ACAM2000 is approved for use and can become available for use against Mpox under an Expanded Access Investigational New Drug (EA-IND) protocol (CDC, 2024b). Up to this point, it has not been used in the current outbreak that started in 2022 (CDC, 2024b). As of August 30th, 2024, the FDA has approved ACAM2000 for the indication of prevention of Mpox disease, specifically in individuals who have been determined to be at high risk for Mpox infection (U.S. Food & Drug Administration [FDA], 2024). There is an adequate supply of ACAM2000 available, but it is important to note that this vaccine option comes with more side effects and contraindications (CDC, 2024b).
JYNNEOS is a live virus that is non-replicating that is licensed to be administered via two subcutaneous injections administered 28 days (four weeks) apart (CDC, 2024b). This vaccine bears no concern for possible spread. Individuals who receive this vaccination are not considered vaccinated until 2 weeks after the second dose of the vaccine (CDC, 2024b). JYNNEOS is approved and recommended first for the prevention of Mpox by the CDC and the Advisory Committee on Immunization Practices (ACIP) (CDC, 2024b). This has been the main vaccine utilized in the United States during this current outbreak starting in 2022 (CDC, 2024b). There is currently enough supply of JYNNEOS available for use as of April 2024 (CDC, 2024b). While there have been two different options for route of administration, because there is plenty of JYNNEOS available now, the subcutaneous route is preferred (CDC, 2024b). The administration of more than 2 doses of JYNNEOS as a booster is only recommended, at this time, for people who work with Mpox/orthopoxviruses in research or diagnostic laboratories (CDC, 2024b). This booster for those with occupational exposure would be recommended at 2-10 years, depending on the type of occupation (CDC, 2024b).
At this time, the CDC does not recommend or endorse the use of routine immunization against Mpox for the general public (CDC, 2024g). It is also not recommended for healthcare professionals unless other risk factors are present (CDC, 2024g). The specific recommendations for those who should receive JYNNEOS vaccination that have been provided by ACIP include (CDC, 2024g):
Individuals who have a risk of occupational exposure to orthopoxviruses
Individuals 18 years and older who at risk for Mpox during the current outbreak
Individuals 18 years and older who have the following risk factors:
Bisexual, gay, or other men who have sex with men, transgender, or nonbinary people who have, in the last six months, either had a new diagnosis of one or more sexually transmitted diseases, more than one sexual partner, or engaged in sexual activity at a commercial venue or in a geographic area where Mpox transmission is occurring
Individuals who have sexual partners with the risk listed above
Children/adolescents under the age of 18 with the same risks listed above
The WHO recommends contact and droplet precautions for Mpox. The CDC's (2007) most recent recommendations for Mpox are contact and airborne precautions. To serve as a reminder (CDC, 2007):
Contact Precautions are used for patients with known or suspected infections or colonized with epidemiologically important microorganisms that can be transmitted by direct or indirect contact. The patient should be in a private room.
Standard Precautions should be used, and a gown and gloves should be worn if there is likely to be contact with the patient or environmental surfaces.
Airborne Precautions are implemented for diseases transmitted by microorganisms carried by airborne droplet nuclei. Possibly infectious patients should be separated from others and asked to wear a surgical mask before airborne precautions can be provided. A surgical N95 respirator is recommended for Airborne Precautions. The N95 is a single-use, disposable item that must be fit-tested to be effective. Airborne Precautions also require the use of an airborne infection isolation room (AIIR) that has specially engineered airflow and ventilation systems. The door to the room must be kept closed, and the negative air pressure should be monitored. When the patient in airborne precautions has to be moved or transported, they should wear a surgical mask from when they leave the isolation room until they return.
Regarding environmental infection control in inpatient hospital settings, the following recommendations have been made by the CDC (CDC, 2022d):
Soiled patient laundry should be removed from patient rooms while avoiding contact with any lesion material left on them
Soiled laundry should be promptly contained in a laundry bag and never be shaken (so as to not disperse infectious material)
Cleaning activities such as dry dusting, sweeping, or vacuuming should be avoided and wet cleaning methods used instead (so as not to disperse infectious material in the air)
No portable fans should be allowed in patient rooms
Anyone who has been diagnosed with Mpox or suspects that they might have it should avoid any close contact with other people. Once the rash sores scab over completely and fall off, the infected person is considered to be no longer contagious (CDC, 2023a). Due to the fact that many cases have included sores in the genital and rectal areas among men who have sex with men, abstinence from sex when Mpox is suspected is encouraged.
A 35-year-old female presents with a five-day history of fever, intense headache, lymphadenopathy, and lack of energy. She has clear fluid-filled vesicles on her face, palms, and soles. Vital signs are within normal limits except for a pulse of 110. She reports that her significant other has been sick for about two weeks and has sores on his face. She does not know if she had chicken pox as a child and has not started any new medications. She has been taking Tylenol. She reports not eating for days and that she has also not been drinking very much. She is pale, and her skin turgor is poor. Her physical examination is otherwise normal.
The patient is given a surgical mask and put in an ER room with the door closed. A CBC, metabolic profile, urinalysis, and swab of her lesions are sent for PCR. The patient is hospitalized on contact and airborne precautions for hydration and symptom management.
The patient's symptoms are significantly better the next day. Her PCR was positive for Mpox. These results are reported to the Health Department, which has initiated contact tracing. She is discharged with symptom management instructions and contact management education to be followed until her lesions heal.
Hopefully, the ER staff is conscious of the potential for Mpox and notices the lymphadenopathy. Given the differential diagnoses and the sanitation and nutrition status of the average American, Mpox may not be considered. Contact isolation and blood and urine tests would have been done with open lesions. Swabbing for a PCR would not be a normal test. In the worst case scenario, she is treated for her symptoms and discharged.
Mpox has been raising concern worldwide. Symptom management is the best treatment at this point. Smallpox vaccination is recommended for exposure to Mpox and for prevention for those at high risk. Healthcare professionals need to be aware of the potential for Mpox and how to identify it from differential diagnoses.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Beer, E. & Rao, V. (2019). A systematic review of the epidemiology of human monkeypox outbreaks and implications for outbreak strategy. PLOS Neglected Tropical Diseases, 13(10), e0007791. Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024a). Treatment information for healthcare professionals. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024b). Monkeypox and smallpox vaccine guidance. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024c). Patient’s guide to mpox treatment with tecovirimat (TPOXX). Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024d). Ongoing clade II mpox global outbreak. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024e). 2022 U.S. map & case count. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024f). Clade 1 mpox outbreak originating in central Africa. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2024g). Vaccination. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2023a). Monkeypox clinical recognition. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2023b). Technical report 3: Multi-national mpox outbreak, United States, 2022. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2022a). Frequently asked questions. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2022b). Monkeypox testing basics. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2022c). Morbidity and mortality weekly report (MMWR). Strategies adopted by gay, bisexual, and other men who have sex with men to prevent monkeypox virus transmission—United States, August 2022. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2022d). Infection prevention and control of monkeypox in healthcare settings. Centers for Disease Control and Prevention (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2022e). Morbidity and mortality weekly report (MMWR): Ocular monkeypox—United States, July-September 2022. Centers for Disease Control and Prevention. (CDC). Visit Source.
Centers for Disease Control and Prevention. (CDC). (2007). Guideline for isolation precautions: Preventing transmission of infectious agents in healthcare settings. Centers for Disease Control and Prevention (CDC). Visit Source.
Grant, R., Nguygen, L., & Breban, R. (2020). Modeling human-to-human transmission of monkeypox. Bulletin of the World Health Organization, 98(9), 638-640. Visit Source.
Hughes, C., Liu, L., Davidson, W., Radford, K., Wilkins, K., Monroe, B., Metcalfe, M., Likafi, T., Lushima, R., Kabamba, J., Nguete, B., Malekani, J., Pukuta, E., Karhemere, S., Muyembe Tamfum, J., Okitolonda Wemakoy, E., Reynolds, M., Schmid, D., & McCollum, A. (2021). A tale of two viruses: Monkeypox and varicella zoster virus coinfections in the Democratic Republic of Congo. The American Journal of Tropical Medicine and Hygiene, 104(2), 604-611. Visit Source.
The Lancet. (2018). Monkeypox contacts: A puzzling problem. The Lancet, 392(10152), 986. Visit Source.
Reynolds, M., McCollum, A., Nguete, B., Shongo Lushima, R., & Petersen, B. (2017). Improving the care and treatment of monkeypox patients in low-resource settings: Applying evidence from contemporary biomedical and smallpox biodefense research. Viruses, 9(12), 380. Visit Source.
Singh, N., Sharma, S., Ghai, G., & Singh, A. (2021). A systematic review on epidemiology of human monkeypox virus. Annals of the Romanian Society for Cell Biology, 25(7), 602-610. Visit Source.
U.S. Food and Drug Administration. (FDA). (2024). FDA roundup: August 30, 2024. U.S. Food and Drug Administration (FDA). Visit Source.
World Health Organization. (WHO). (2024). Monkeypox. World Health Organization (WHO). Visit Source.
World Health Organization. (WHO). (2022). WHO recommends new name for monkeypox disease. World Health Organization (WHO). Visit Source.
Zimmerman, P., & Curtis, N. (2022). Monkeypox—What pediatricians need to know. The Pediatric Infectious Disease Journal, 41(12): 1020-1031. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.