This course will be updated or discontinued on or before Monday, October 11, 2027
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
CEUFast, Inc. is an AOTA Provider of professional development, Course approval ID#14810. This distant learning-independent format is offered at 0.1 CEUs Intermediate, Categories: OT Service Delivery, Foundational Knowledge
AOTA does not endorse specific course content, products, or clinical procedures. AOTA provider number 9757.
CEUFast, Inc. (BOC AP#: P10067) is approved by the Board of Certification, Inc. to provide education to Athletic Trainers (ATs).
CEUFast, Inc. is recognized by the New York State Education Department's State Board for Physical Therapy as an approved provider of physical therapy and physical therapist assistant continuing education.
FPTA Approval: CE26-1334013. Accreditation of this course does not necessarily imply the FPTA supports the views of the presenter or the sponsors.
Outcomes
≥ 92% of participants will know the signs and symptoms of postural orthostatic tachycardia syndrome (POTS), how it is diagnosed, and the treatment options available to patients.
Objectives
After completing this continuing education course, the participant will be able to meet the following objectives:
Recognize at least two hallmark signs and symptoms experienced by a person with postural orthostatic tachycardia syndrome (POTS).
Evaluate the differences in compensation between a healthy person and someone with POTS.
Outline the clinical diagnostic process of POTS.
Formulate a non-pharmacological treatment plan for a patient with POTS utilizing exercise, dietary, and behavioral modification strategies.
Elaborate on pharmacological treatments for POTS.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
Imagine feeling lightheaded and dizzy, having heart palpitations, and nearly fainting almost every time you stand up. Luckily, this time you did not actually pass out. You cannot afford to get another concussion or take time off work- AGAIN. Well, there goes the day, as you will likely feel wiped out or in a fog the rest of the day. Just another bad day. While we have all experienced this occasionally, most of us do not think twice about standing up. Yet, this can be a daily occurrence for a person with Postural Orthostatic Tachycardia Syndrome, commonly known as POTS.
POTS is a form of dysautonomia, or a disorder of the autonomic nervous system, characterized by lightheadedness and a fast heartbeat when standing. It is part of a group of disorders that involve orthostatic intolerance (National Institute of Neurological Disorders and Stroke [NINDS], n.d.).
Unfortunately, POTS is still not widely known for several reasons, including its relatively recent distinction as a syndrome, the complexity of symptoms, and the lack of widespread awareness. There may be early references to similar symptomology in medical literature as early as the Civil War period (Boris et al., 2024). However, the term POTS was first utilized to describe a patient "with postural tachycardia without postural hypotension" by Rosen and Cryer (1982) in an article published in the American Journal of Medicine. Despite this, POTS did not receive its own diagnostic code until October 2022 (Tupponce, 2025). Additionally, the symptoms of POTS can be vague, diverse, and affect multiple body systems, making it difficult to diagnose at times or frequently misdiagnosed (George & Winters, 2023; Vernino et al., 2021). Lastly, many healthcare providers are not familiar with POTS, so people can often experience symptoms for years before being diagnosed (Lewis, 2024). It is gaining more recognition, partly because of patient advocacy groups, possible connections to Long COVID, and increased awareness on social media and in the public eye about the syndrome. This was evident in the 2024 Paris Olympics, when U.S. Swimmer Katie Ledecky reported that she suffers from the condition (Tupponce, 2025).
The classic characteristic of POTS is tachycardia when standing (NINDS, n.d; Raj et al., 2022; Zao & Tran, 2023). Within ten minutes of standing, a person's heart rate might increase by more than 30 beats per minute or exceed 120 beats per minute. This racing heartbeat will typically improve when the person lies down again. Common symptoms of POTS may include the following (NINDS, n.d.):
Although the prevalence of POTS has not been adequately investigated, data are based largely on clinical experiences. It is estimated that approximately 0.2%-1% of the U.S. population is affected, suggesting that 1-3 million persons live with POTS (Vernino et al., 2021). The worldwide prevalence of POTS has not been well-established (Zhao & Tran, 2023).
Anyone can be affected by POTS; however, it is more common in pubescent girls and premenopausal women between the ages of 15 and 50 years (NINDS, n.d.; Raj et al., 2022), with the majority presenting between 15 and 25 (Zhao & Tran, 2023). A higher prevalence of POTS occurs in the U.S compared to other countries and in people who are White and non-Hispanic in race and ethnicity (Shaw et al., 2019). The onset of POTS will often begin after a stressor such as pregnancy, major surgery, puberty, physical trauma (such as a concussion), or viral illness (Vernino et al., 2021; Zhao & Tran, 2023). A family history of POTS or other related conditions also increases risk (Shaw et al., 2019).
The initial presentation of POTS seems to have two clinical patterns (Vernino et al., 2021):
Acute onset following a viral infection (20-50% of patients)
Slowly progressing symptoms over a longer period of time
A number of conditions have been shown to be closely associated with POTS, with the three most common comorbidities being migraine headaches, irritable bowel syndrome (IBS), and Ehler-Danlos Syndrome (EDS), specifically the hypermobility type of EDS (hEDS) (Chopra, 2025; NINDS, n.d., Raj et al., 2022).
Migraine: It is reported that about 40% of POTS patients also experience migraine. According to Riggins (n.d.), this may be due to common pathophysiologic mechanisms involving sympathetic nervous system dysregulation, hemodynamics, and central sensitization.
IBS: Gastrointestinal symptoms are common in patients with POTS, resulting in some people who may simultaneously meet the diagnostic criteria of IBS. While the pathophysiology of POTS and gastrointestinal dysfunction has not been studied, gastrointestinal symptoms are controlled and regulated by the autonomic nervous system, creating speculation that dysautonomia may disrupt the gastrointestinal system (Vernino et al., 2021).
hEDS: EDS is an inherited connective tissue disorder that is characterized by joint hypermobility and pain. Because EDS is a collagen disorder, it may contribute to the development of POTS. While often found together, the connection between the two is not fully understood. According to Chopra (2025), "studies indicate that up to 80% of individuals with hEDS also experience POTS, and about 31% of POTS patients have hEDS."
A 2019 study involving 4835 participants living with POTS showed the following prevalence of various comorbidities (Shaw et al., 2019):
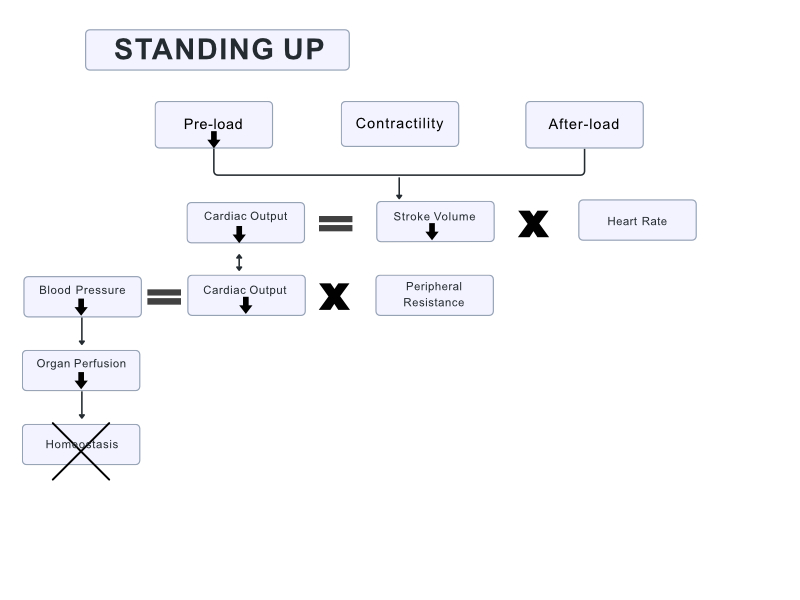
In a typical healthy person, the autonomic nervous system uses many systems to achieve adequate cardiac output, organ perfusion, and hemodynamic stability. This is a combination of sympathetic and parasympathetic controls within the autonomic nervous system.
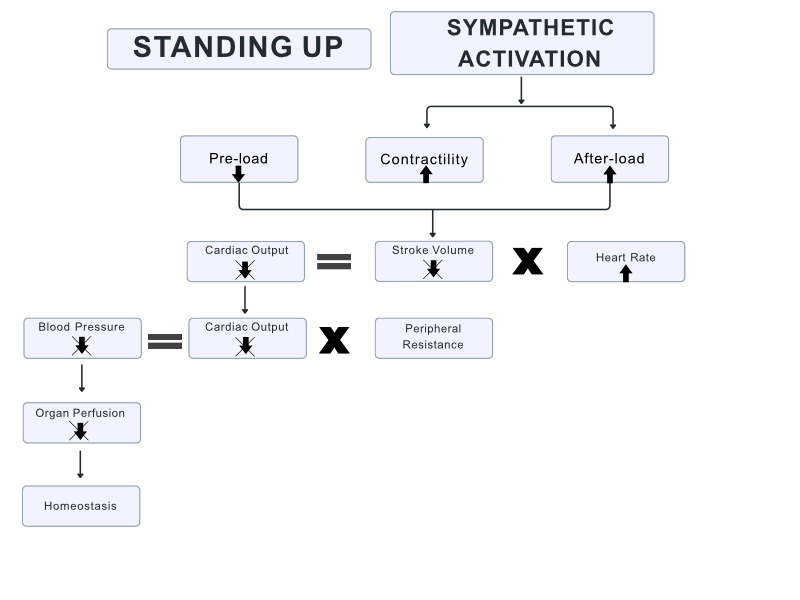
When a healthy person stands up, the force of gravity causes approximately 500-1000 milliliters (ml) of blood to shift from the chest to the lower extremities (George & Winters, 2023). Approximately 25% of this vascular volume moves into the interstitial space, or the space between the cells and the blood vessels. Left uncompensated, this shift in blood would cause hemodynamic instability. However, almost immediately, the autonomic baroreceptors sense this change and compensate by increasing the sympathetic activity, leading to a temporary increase in heart rate, increased cardiac contractility, and increased systemic vascular resistance, among other things (George & Winters, 2023). These changes occur within seconds to stabilize the blood pressure until the body is able to restore cardiac output and regain orthostatic homeostasis.
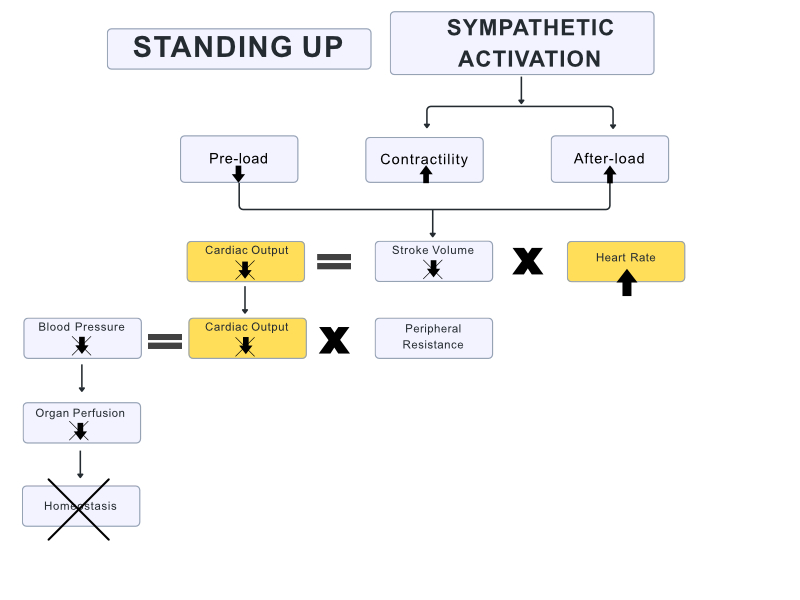
When a person with POTS stands up, they experience the same gravitational shift in blood and decrease in cardiac output; however, the normal autonomic compensation is not enough to restore hemodynamic stability, leading to a variety of symptoms commonly associated with POTS (George & Winters, 2023).
Physiology of POTS
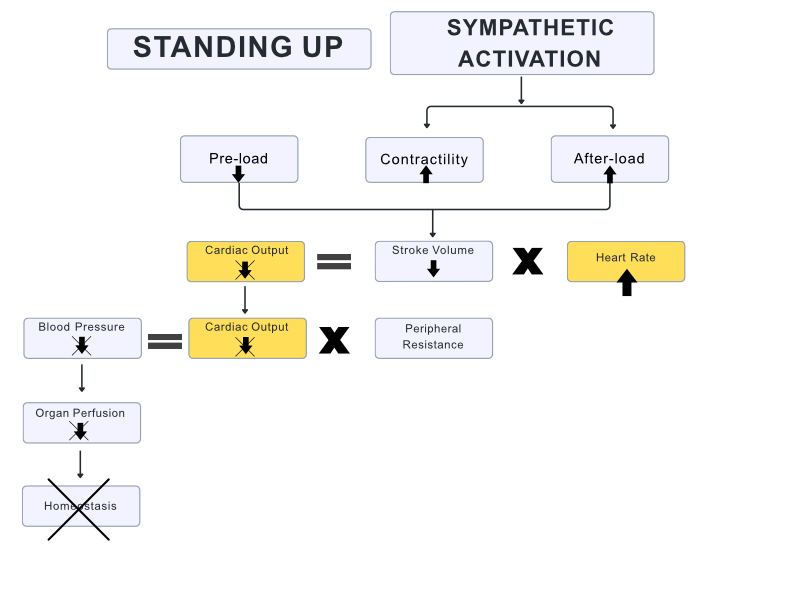
Similar to a patient with orthostatic hypotension, the person with POTS is unable to maintain adequate blood pressure in standing. However, as opposed to orthostatic hypotension, in which there is a drop in blood pressure when moving in an upright posture, part of the diagnostic criteria for POTS is not having a decrease in blood pressure upon standing (George & Winters, 2023). The autonomic compensation in a person with POTS is enough to avoid a dramatic drop in blood pressure, instead creating exaggerated tachycardia. Instead of being a temporary compensation like it should be, this compensation remains constant in a patient with POTS, or continues to increase as long as the patient is standing (George & Winters, 2023). Additionally, studies have shown a decrease in cerebral blood flow (CBF) by 29% in patients with POTS during tilt table testing (van Campen et al., 2020). This cerebral hypoperfusion can manifest as dizziness, presyncope, and headaches (van Campen et al., 2020).
Compensation of POTS with Standing
While most patients have an unknown or multifactorial cause of POTS, some studies have shown a significant decrease in central venous pressure (CVP) by at least 50%, or up to 1-2 millimeters of mercury (mmHg) when standing (George & Winters, 2023). Although there are some correlations in a person with POTS with a pathological disease of CVP, the underlying cause of this change is unknown, which is why POTS is considered a syndrome and not a disease (George & Winters, 2023).
There are many proposed etiologies, leading to the characterization of subtypes of POTS (Zhao & Tran, 2023).
Neuropathic: Characterized by lower limb sympathetic denervation leading to decreased venoconstriction and venous pooling. This requires an excessive cardiovascular response to maintain adequate mean arterial pressure. In studies, POTS patients exhibited peripheral sudomotor denervation, correlating with a lack of sweating (distal anhidrosis) and cyanosis in the hands and feet (acrocyanosis).
Hyperadrenergic: Characterized by elevated standing plasma norepinephrine levels > 600 picograms per milliliter (pg/ml). Predominant symptoms include increased sympathetic tone, including tremors, palpitations, hypertension, anxiety, and tachycardia. It is estimated that 30-60% of patients with POTS fall into this subtype.
Hypovolemic: Up to 70% of patients with POTS have decreased plasma, red blood cells, and total blood volume. This may be due to low renin and aldosterone levels, which are responsible for maintaining plasma volume. Additionally, secondary hypovolemia may present in patients with co-existing gastrointestinal problems such as nausea, vomiting, and diarrhea, leading to excessive volume loss and poor intake.
Autoimmune: A significant overlap between patients with POTS and other systemic autoimmune disorders leads to a hypothesis of autoimmune etiology.
Deconditioning: Physical and cardiovascular deconditioning is often noted in patients with POTS, although it is undetermined if this is a cause or effect of POTS. A decrease in cardiac size and mass has been observed in patients with POTS, with a 16% decrease in left ventricular mass and a 20% decrease in plasma volume. Chronic fatigue and reduced tolerance to physical activity result in an "unfavorable feedback cycle that exacerbates already prominent existing symptoms" (Zhao & Tran, 2023).
Diagnosis of POTS can be challenging because the symptoms often present similarly to other conditions, leading to a delay in diagnosis, misdiagnosis, or the need to see specialists like cardiologists or neurologists (NINDS, n.d.). A thorough review of a person's medical history and symptoms is an essential starting point in the diagnostic process. While it is not uncommon to occasionally get lightheaded or dizzy when standing from lying down or sitting, for a person with POTS, this is a regular, chronic occurrence.
A physician will typically measure the person's heart rate and blood pressure, and determine how these measurements change in response to changes in position, such as standing up quickly (NINDS, n.d.), formally known as an active stand test. During this test, the patient will lie supine for ten minutes, and the baseline heart rate and blood pressure will be measured. The person then stands, and the provider immediately measures their heart rate and blood pressure, repeating the measurements at one minute, three minutes, and five minutes (Zhao & Tran, 2023).
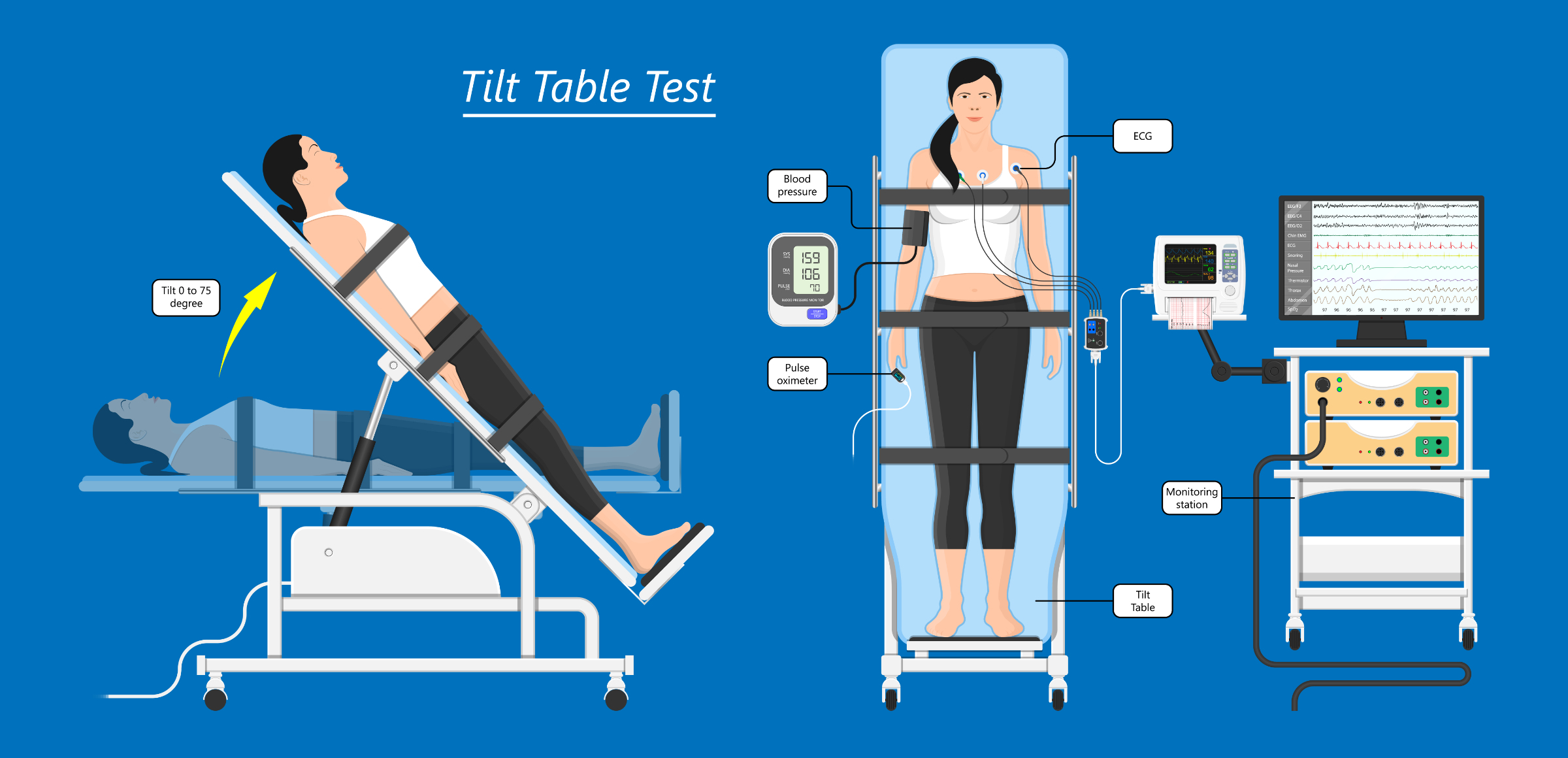
A tilt table test is another common test utilized in the diagnosis, also known as a head-up-tilt test (HUTT). During this test, the person is strapped to a table while being monitored for vital signs. The table will tilt to different positions while measurements are recorded to show how different positions affect the heart rate, heart rhythm, and blood pressure (Cleveland Clinic, 2023). As the person is tilted into a standing position (with the head always remaining up), the provider will monitor for any symptoms, such as lightheadedness, dizziness, palpitations, nausea, or feelings of syncope (Cleveland Clinic, 2023). A significant increase in heart rate, without a significant drop in blood pressure, strongly suggests POTS.
Laboratory studies should include a complete blood count, electrolytes, thyroid function test, and electrocardiogram in addition to a physical examination. Based on the person's clinical presentation, other laboratory tests may be required (Vernino et al., 2021).
Occasionally, abnormal sudomotor tests, such as the quantitative sudomotor axon reflex test (QSART) or abnormal intraepidermal nerve fiber density on skin biopsy, are required for patients with a more neuropathic phenotype of POTS (Vernino et al., 2021).
Tilt Table Test
(*Please click on the image above to enlarge.)
Diagnostic Criteria
For a diagnosis of POTS, all of the following criteria must be met:
Sustained heart rate increase of ≥ 30 beats per minute within ten minutes of upright posture. This is altered to ≥ 40 beats per minute in patients aged 12-19 years.
Absence of significant orthostatic hypotension (blood pressure decrease of > 20/10 mmHg).
Very frequent symptoms of orthostatic intolerance that are worse while upright, with significant and quick improvement after returning to a supine position.
Symptom duration ≥ three months
No other condition that could explain sinus tachycardia
(Raj et al., 2022; Shaw et al., 2019)
According to Raj et al. (2022), "While orthostatic tachycardia must occur in the absence of classical hypotension, transient initial orthostatic hypotension does not preclude a diagnosis of POTS." It is physiologically normal to have orthostatic tachycardia variations from day to day and at different times of day; in fact, a higher level of orthostatic tachycardia occurs in the morning than later in the day. Therefore, if a patient does not meet the diagnostic criteria, but clinical suspicion is high, it is advisable to reassess at a later date, preferably in the morning (Raj et al., 2022).
Patients with POTS are frequently misdiagnosed as having an anxiety disorder, with 77% of survey respondents being told that they have a psychological disorder (Shaw et al., 2019). This is likely because symptoms such as palpitations, dizziness, and lightheadedness can resemble anxiety-related conditions.
Because POTS is a syndrome, not a disease, the diagnostic criterion for POTS involves ruling out other known pathologies in addition to specific heart rate criteria (George & Winters, 2023).
Non-pharmacologic interventions are considered first-line treatment for a person with POTS, with patient education being a foundation of management. Patient education is aimed at strategies that aid in reducing the excessive venous pooling when moving into upright postures in order to decrease the symptoms experienced by a person with POTS. Management of expectations is also a crucial part of patient education. It is important that the patient understands that POTS is often non-specific and chronic. Focusing on daily functional improvement is key.
Strategies include the use of exercise, dietary changes, and the use of compression garments.
Despite the pathophysiological cause of POTS, cardiovascular deconditioning appears to be a common finding in people with POTS. This is evidenced by cardiac atrophy and hypovolemia (Fu & Levine, 2018). Because of this deconditioning, exercise is an essential component of the management of POTS. It is recommended that all patients begin slowly on a gradual physical exercise routine (Zhao & Tran, 2023). Due to the potential for dizziness, lightheadedness, or syncope, it is optimal to have supervised exercise sessions. Using horizontal exercise is a critical strategy early in the course of treatment. This allows the person to exercise while avoiding upright postures that elicit the POTS symptoms (Fu & Levine, 2018). This can be accomplished through:
Swimming
Rowing
Recumbent stationary bike
As the person increases their physical fitness, the duration, intensity, and frequency of exercise should be progressively increased. The person may only be able to tolerate starting with 1-2 exercise sessions per week, building to 5-6 days per week. Gradually, upright exercise can be added as tolerated (Fu & Levine, 2018).
Resistance training and muscle strengthening are recommended to increase muscle tone, especially in the lower extremities and core musculature (Fu & Levine, 2018). Increased resting muscle tone will increase peripheral resistance to fluid moving into the interstitial spaces and will aid in venous return. Because many POTS patients may also have hEDS, it is very important to protect the joints that are susceptible to hypermobility. Braces and protection are highly recommended to protect joints such as elbows, wrists, thumbs, and knees. Physical therapy is recommended to avoid worsening or aggravating joint damage, joint instability, and pain (Fu & Levine, 2018).
Dietary changes are a crucial component of managing POTS, aimed at stabilizing blood pressure, increasing blood volume, and regulating symptoms. Many patients with POTS have decreased plasma and blood volume, contributing to decreased stroke volume and reflexive tachycardia during orthostasis (Fu & Levine, 2018). Increased fluid and salt intake are means by which a person with POTS can increase plasma volume and orthostatic tolerance (Fu & Levine, 2018). It is recommended that patients with POTS with normal cardiac and renal-adrenal function gradually increase their daily salt intake up to ten grams (g) per day. Doing this through increasing sodium intake via food is advisable over salt tablets, as tablets can cause nausea, vomiting, and dehydration due to osmotic loading into the stomach, resulting in further reduction of plasma and blood volume (Fu & Levine, 2018). Water intake is recommended up to three liters per day (12.5 cups); however, consuming water and salt together throughout the day is recommended over water alone. "Water alone is not effective in long-term volume expansion", according to Fu & Levine (2018).
Suggestions for salty snacks:
Pickles
Olives
Tomato juice
Cheese
Cured meats
Pretzels or chips (it can be beneficial to keep a small snack bag of pretzels with you for those times you feel like you need a quick salt intake)
Salty Snacks
Other dietary considerations include (University of Central Florida Health, n.d.):
Whole grains: Do not forget your grains like quinoa, brown rice, and oats! Whole grains break down slowly and sustain energy over a longer period of time without blood sugar spikes.
Fiber-rich foods: Eat your oats and apples! Soluble fiber helps promote nutrient absorption and soften stool. Insoluble fiber prevents constipation and promotes regular bowel movements. Remember that 30% of people with POTS also report IBS symptoms.
Electrolyte-rich foods: Increase foods like bananas, leafy greens, and nuts! Electrolytes such as sodium, potassium, and magnesium play key roles in nerve function, muscle contraction, and fluid balance. Electrolyte balance is important for a person with POTS and can significantly decrease symptoms.
Consider gluten-free options: Some people with POTS may also have undiagnosed gluten intolerance (sometimes the symptoms overlap). Eating a gluten-free diet may help reduce inflammation and alleviate gastrointestinal symptoms. A small study indicates that a gluten-free diet may be effective in non-celiac people with POTS who were not celiac patients (Zha et al., 2022).
Physical Countermeasures are actions that increase orthostatic tolerance and may be effective in alleviating acute symptoms, as well as preventing orthostatic intolerance, syncope, or near-syncope (Fu & Levine, 2018).
Physical Countermeasure Maneuvers (adapted from Fu & Levine, 2018)
Activity
Description
Action
Squeezing a rubber ball
Static or rhythmic contraction to increase arterial pressure and prevent orthostatic intolerance or syncope
Sympathetic activation, vagal withdrawal, or both via exercise pressor reflex
Leg crossing and muscle tightening
Crossing one foot in front of the other, tightening the thighs and gluteal muscles
Restores venous return and prevents further blood pooling in the lower body
Compression garments are elastic clothing that have a compression gradient designed to apply a mechanical pressure on the surface of the body zones (Xiong & Tao, 2018). Also known as nonpneumatic antishock garments, they apply approximately 20-40 mmHg of compression (Bourne et al., 2021) and come in a variety of sizes (calf, full leg). They can be custom-fitted for the patient with a prescription or readily purchased over the counter. Lower body compression garments have been shown to reduce symptoms and reduce heart rate in patients with POTS (Bourne et al., 2021). While partial lower body compression (i.e., compression socks) did demonstrate effectiveness, there were greater benefits with more compression (full leg compression stockings or leggings) (Bourne et al., 2021). If a person is unable to tolerate the use of lower extremity compression, there is evidence that abdominal compression (like an abdominal binder) can still provide some symptom reduction (Miller & Bourne, 2020).
Sleep with the head of the bed elevated. Sleeping with the head of the bed elevated, with the entire body at a slight angle, can increase circulating plasma and central blood volume through the activation of the renin-angiotensin-aldosterone system (Fu & Levine, 2018).
Eat smaller meals. Blood is redirected to assist with digestion after eating a large meal, which can exacerbate symptoms for a patient with POTS. Smaller meals will limit this blood diversion (Dysautonomia International, 2019).
Monitor reactions to caffeine. Caffeine can be helpful to some patients with POTS, and exacerbate symptoms in others (Dysautonomia International, 2019).
Avoid Alcohol: Alcohol can worsen POTS symptoms due to its dehydration effect and possible hypotension from dilation of veins (Dysautonomia International, 2019).
Remain flexible with scheduling activities: Mornings can be an especially symptomatic time for many people with POTS. Schedule activities during a time of day that seems to be the best for the person with POTS. Remain flexible, as symptoms can flare without much warning (Dysautonomia International, 2019).
POTS Rescue Kit
Since symptoms can be unpredictable and can change rapidly and without warning, having your emergency supplies handy and together can be very helpful. Here are a few things to keep in your kit.
Salty snacks!
Water bottle or electrolyte drink (or a packet of electrolytes to add to your water)
Handheld fan
Emergency medications (if you are on any prescribed medications)
List of medications currently prescribed
Emergency contact in case fainting and/or injury do occur. It may also be helpful to have a brief explanation of POTS in case someone finds you unconscious. Many emergency medical providers and emergency physicians are not well-versed in POTS, so understanding that this is a known issue and diagnosis can be helpful.
Pharmacologic therapy is not considered first-line treatment for POTS and is not proven to be more effective than non-pharmacologic strategies (Zhao & Tran, 2023). Although there is currently no drug approved by the U.S. Food and Drug Administration (FDA), there are several used off-label for the treatment of POTS. A recent systematic review of studies of oral medication for the management of POTS was just published in the journal Frontiers in Neurology by Pierson et al. (2025). In this review, they determined that the most researched medications evaluated were cardioselective beta-blockers, midodrine, ivabradine, non-cardioselective beta-blockers, and fludrocortisone (Pierson et al., 2025). The findings of this review indicate that the medications with the most evidence supporting their use are midodrine, which has shown a 78% successful improvement in symptoms; ivabradine (75%); and beta-blockers (64%). Below are actions, dosing recommendations, side effects, and precautions for the medications with the most evidence supporting their use as indicated in the study mentioned above. Please note that this chart is not exhaustive, and there are other medications used to try to treat POTs, including medications that treat specific symptoms, and not the underlying causes of POTs.
Table: Medications commonly used to treat POTS
Medication
Action
Dosing Information
Side effects
Precautions
Midodrine
Midodrine is a vasoconstrictor and works by increasing the tone of the peripheral blood vessels. This reduces the likelihood of blood pooling, improves blood return, and increases vascular tone
2.5-15 milligrams (mg) orally 3x daily
Headache, scalp and skin tingling, supine hypertension
Ivabradine
Beta-blocker that modulates the intrinsic pacemaker rate of the sinus node
2.5-7.5 mg orally 2x daily
Headaches, palpitations, hypertension, and visual disturbances
Propranolol
Beta-blockers used to decrease the heart rate as a means to decrease upright tachycardia
10-20 mg orally up to 4x daily
Hypotension, bradycardia
Can cause bronchoconstriction in patients with asthma
(Miller & Raj, 2018)
Several lines of evidence suggest an autoimmune mechanism, at least in some people with POTS. Case reports and retrospective case series have suggested anecdotal evidence of the efficacy of intravenous immunoglobulin (IVIG) in the treatment of POTS (Vernino et al., 2021). Two randomized trials are currently in progress evaluating IVIG for POTS (Pierson et al., 2025). Evidence does not support the use of fludrocortisone or pyridostigmine as treatments for POTS (Pierson et al., 2025).
Generally, medications that exacerbate symptoms such as tachycardia (amphetamines, selective serotonin and/or norepinephrine reuptake inhibitors, droxidopa) or that worsen orthostatic intolerance (diuretics, calcium channel blockers, nitrates, opiates, tricyclic antidepressants) should be avoided (Zhao & Tran, 2023).
Long-term data are limited, but overall, the prognosis for POTS is generally favorable (Zhao & Tran, 2023). Over 50% of patients do not meet the criteria for POTS within 5 years, most within the first 1-2 years, as characterized by minimal functional impairment (Zhao & Tran, 2023). Younger patients generally experience more favorable outcomes, and there have been no deaths directly attributed to POTS (Zhao & Tran, 2023).
While not usually fatal, complications of POTS can arise if the syndrome remains undiagnosed or is poorly managed. These complications can range from physical injuries to significant mental health impacts.
Physical Injuries: (Boris et al., 2024):
Injuries from fainting: Given that POTS can cause fainting or near-fainting, trauma such as concussions, fractures, cuts, and bruises can occur.
Dehydration: People with POTS may experience nausea and vomiting. This could lead to dehydration or electrolyte imbalances, possibly affecting cardiac or muscular function.
Decreased exercise tolerance: Excessive fatigue and orthostatic intolerance may severely limit the physical activity in a person with POTS. This could even result in them not being able to participate in sports in which they were previously involved, and affect their overall quality of life.
Mental Health Complications (Raj et al., 2018):
Anxiety and depression: The chronic and sometimes debilitating symptoms of POTS can impact mental health, lead to anxiety and depression, and sometimes suicidal thoughts.
Cognitive dysfunction: Brain fog resulting from POTS can lead to difficulty concentrating, memory problems, and impact decision-making.
Sleep disturbances: Many people with POTS experience sleep issues, including difficulty falling asleep, difficulty staying asleep, or getting restful sleep. This can exacerbate fatigue already associated with POTS.
POTS is a long-term condition that impacts multiple body systems by disrupting normal autonomic nervous system function. It is typically identified by a sharp increase in heart rate and other symptoms triggered by standing upright. The condition most often emerges in females during adolescence and can persist throughout their reproductive years. POTS can severely limit daily functioning, making it difficult for individuals to attend school, maintain employment, or enjoy a fulfilling quality of life. Because the biological mechanisms behind POTS are not yet fully understood, treatment options remain limited. Expanding research into both the causes and therapies of the condition is essential for developing more effective care and improving the lives of those living with it. "Treatment for POTS can improve symptoms and function and can be initiated in primary care" (Raj et al., 2022).
Samantha, a 20-year-old collegiate track runner, had no significant past medical history aside from mild seasonal allergies. She reported being in excellent health, with no prior cardiac or neurologic conditions.
During a routine training run, Samantha suddenly experienced dizziness, palpitations, shortness of breath, and an episode of near-syncope upon transitioning from a walking warm-up to running. The nearby athletic trainer witnessed Samantha's near-fainting episode and immediately went over to provide care. Samantha reported her heart "racing out of control" and significant fatigue despite low exertion. She reported that she has not been ill and has never experienced this type of occurrence before.
Samantha was escorted into the athletic training room, where an initial evaluation was completed. Her vital signs showed:
Resting heart rate supine: 78 beats per minute
Blood pressure supine: 110/70 mmHg
Heart rate after standing two minutes: 128 beats per minute
Heart rate after standing 10 minutes: 142 beats per minute
Blood pressure remained stable at 110/72 mmHg
Oxygen saturation: 98%
Neurological exam was negative
Samantha was referred to the team physician (a family practice, sports medicine specialist), where an electrocardiogram (ECG) ruled out arrhythmia. Basic lab work, thyroid function, and electrolytes were within normal limits. An echocardiogram revealed no structural heart disease. Based on her history, absence of structural heart disease, and marked increase in heart rate upon standing without significant orthostatic hypotension, the team physician ordered a tilt-table test, which showed a marked increase in heart rate in the upright position. Samantha was subsequently diagnosed with POTS. The team physician prescribed Samantha 2.5 mg of midodrine orally to be taken 2-3 times a day.
Samantha worked closely with the athletic trainer on treatment, which began with lifestyle modifications and a structured exercise progression.
Increased daily fluid intake (2–3 liters).
Increased dietary salt (8–10 g/day as tolerated).
Use of compression stockings during training and daily activities.
Gradual reconditioning exercises starting with recumbent cycling and rowing.
Slow and gradual lower extremity strengthening exercises to improve muscle tone, resist venous pooling, and improve venous blood return.
Over three months, Samantha noted improvement in her exercise tolerance and a reduction in presyncope episodes. With careful monitoring from her medical team and athletic trainers, she transitioned from recumbent exercises back to light jogging. She was counseled on pacing strategies, hydration, and symptom recognition to participate in athletics safely. Samantha learned always to carry her rescue kit so she always had a salty snack and electrolytes handy if she started to notice any symptoms developing.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
Boris, J. R., Shadiack, E. C., McCormick, E. M., MacMullen, L., George‐Sankoh, I., & Falk, M. J. (2024). Long‐term POTS Outcomes Survey: Diagnosis, therapy, and clinical outcomes. Journal of the American Heart Association, 13(14). Visit Source.
Bourne, K. M., Sheldon, R. S., Hall, J., Lloyd, M., Kogut, K., Sheikh, N., Jorge, J., Ng, J., Exner, D. V., Tyberg, J. V., & Raj, S. R. (2021). Compression garment reduces orthostatic tachycardia and symptoms in patients with postural orthostatic tachycardia syndrome. Journal of the American College of Cardiology, 77(3), 285–296. Visit Source.
Chopra, P. (2025). Ehlers-Danlos Syndrome and POTS. The Center for Complex Conditions. Visit Source.
Fu, Q., & Levine, B. D. (2018). Exercise and non-pharmacological treatment of POTS. Autonomic Neuroscience, 215, 20–27. Visit Source.
George, A., & Winters, B. (2023). Postural Orthostatic Tachycardia Syndrome (POTS): A frequently missed diagnosis. The Journal for Nurse Practitioners, 19(2), 104439. Visit Source.
Lewis, D. K. L. (2024). POTS: Diagnosing and treating this dizzying syndrome. Harvard Health. Visit Source.
Miller, A. J., & Bourne, K. M. (2020). Abdominal compression as a treatment for postural tachycardia syndrome. Journal of the American Heart Association, 9(14), e017610. Visit Source.
Miller, A. J., & Raj, S. R. (2018). Pharmacotherapy for postural tachycardia syndrome. Autonomic Neuroscience Basic & Clinical, 215, 28–36. Visit Source.
National Institute of Neurological Disorders and Stroke (NINDS). (n.d.). Postural Tachycardia Syndrome (POTS). National Institute of Neurological Disorders and Stroke. Visit Source.
Pierson, B. C., Apilado, K., Franzos, M. A., Allard, R., Mancuso, J. D., Tribble, D., Saunders, D., & Koehlmoos, T. P. (2025). Oral medications for the treatment of postural orthostatic tachycardia syndrome: A systematic review of studies before and during the COVID-19 pandemic. Frontiers in Neurology, 15, 1515486. Visit Source.
Raj, S. R., Fedorowski, A., & Sheldon, R. S. (2022). Diagnosis and management of postural orthostatic tachycardia syndrome. Canadian Medical Association Journal, 194(10), E378–E385. Visit Source.
Raj, V., Opie, M., & Arnold, A. C. (2018). Cognitive and psychological issues in postural tachycardia syndrome. Autonomic Neuroscience, 215, 46–55. Visit Source.
Riggins, N. (n.d.). Research Summary: Postural orthostatic tachycardia syndrome (POTS) and migraine: A narrative review. American Headache Society. Visit Source.
Rosen, S. G., & Cryer, P. E. (1982). Postural tachycardia syndrome. The American Journal of Medicine, 72(5), 847–850. Visit Source.
Shaw, B. H., Stiles, L. E., Bourne, K., Green, E. A., Shibao, C. A., Okamoto, L. E., Garland, E. M., Gamboa, A., Diedrich, A., Raj, V., Sheldon, R. S., Biaggioni, I., Robertson, D., & Raj, S. R. (2019). The face of postural tachycardia syndrome – insights from a large cross‐sectional online community‐based survey. Journal of Internal Medicine, 286(4), 438–448. Visit Source.
Tupponce, J. (2025). What is Postural Orthostatic Tachycardia Syndrome or POTS? VCU Health. Visit Source.
University of Central Florida Health. (n.d.). The best POTS diet: Choosing which foods to eat and avoid. University of Central Florida. Visit Source.
Van Campen, C. M., Verheugt, F. W., Rowe, P. C., & Visser, F. C. (2020). Cerebral blood flow is reduced in ME/CFS during head-up tilt testing even in the absence of hypotension or tachycardia: A quantitative, controlled study using Doppler echography. Clinical Neurophysiology Practice, 5, 50–58. Visit Source.
Vernino, S., Bourne, K. M., Stiles, L. E., Grubb, B. P., Fedorowski, A., Stewart, J. M., Arnold, A. C., Pace, L. A., Axelsson, J., Boris, J. R., Moak, J. P., Goodman, B. P., Chémali, K. R., Chung, T. H., Goldstein, D. S., Diedrich, A., Miglis, M. G., Cortez, M. M., Miller, A. J., Freeman, R., … Raj, S. R. (2021). Postural orthostatic tachycardia syndrome (POTS): State of the science and clinical care from a 2019 National Institutes of Health Expert Consensus Meeting - Part 1. Autonomic Neuroscience, 235, 102828. Visit Source.
Xiong, Y., & Tao, X. (2018). Compression garments for medical therapy and sports. Polymers, 10(6), 663. Visit Source.
Zha, K., Brook, J., McLaughlin, A., & Blitshteyn, S. (2022). Gluten-free diet in postural orthostatic tachycardia syndrome (POTS). Chronic Illness, 19(2), 409–417. Visit Source.
Zhao, S., & Tran, V. H. (2023). Postural Orthostatic Tachycardia Syndrome. In StatPearls. StatPearls Publishing. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.