This course will be updated or discontinued on or before Tuesday, August 3, 2027
Nationally Accredited
CEUFast, Inc. is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation. ANCC Provider number #P0274.
Outcomes
≥ 92% of participants will know what a maternal fetal triage tool is and how to use them.
Objectives
After completing this continuing education course, the participant will be able to:
Define maternal fetal triage.
Describe the existing maternal fetal triage index tools that are available.
Explain the rationale behind the need for maternal fetal triage.
Determine how to use a maternal fetal triage assessment tool.
Justify the use of maternal fetal triage assessment tools to improve patient outcomes.
CEUFast Inc. and the course planning team for this educational activity do not have any relevant financial relationship(s) to disclose with ineligible companies whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
Last Updated:
$39 Unlimited Access for 1 Year (Includes all state required Nursing CEs)
No Tests Required (Accepted by most states & professions)
Nursing Assistants from California, only. You must read the material on this page before you can take the test. The California Department of Public Health, Training Program Review Unit has determined that is the only way to prove that you actually spent the time to read the course. Less
The Association of Women's Health, Obstetric, and Neonatal Nurses (AWHONN) defines obstetric (OB) triage as "the brief, thorough, and systematic maternal and fetal assessment performed when a pregnant woman presents to care to determine priority for full evaluation”(Mayberger et al., 2022).
A maternal fetal triage assessment tool is a tool that can be used for nurses to determine the medical and nursing needs of the pregnant woman who arrives at a triage unit or labor and delivery unit. Not all hospitals have maternal fetal triage units, so this triage may occur in the labor and delivery unit.
Obstetric triage has been regarded as a multidisciplinary specialty within labor and delivery (Quaile, 2018). It has been compared to an emergency department as it often features an unpredictable census, various chief complaints, and unexpected challenges (Quaile, 2018). It is important for nurses and providers to quickly assess a patient’s status to determine how urgently they will need to be treated.
Prior to the year 2007, a maternal fetal triage assessment tool did not exist. Since then, various tools have been created to better streamline assessment and intervention for the obstetric population including The Florida Hospital OB Triage Acuity Tool, the Gothenburg Obstetrical Triage System (GOTS), and Association of Women's Health, Obstetric, and Neonatal Nurses (AWHONN)’s Maternal Fetal Triage Index (MFTI). The newest, evidence-based tool created by the Association of Women's Health, Obstetric, and Neonatal Nurses (AWHONN) was developed in 2015 (Quaile, 2018). It was more recently revised in 2022.
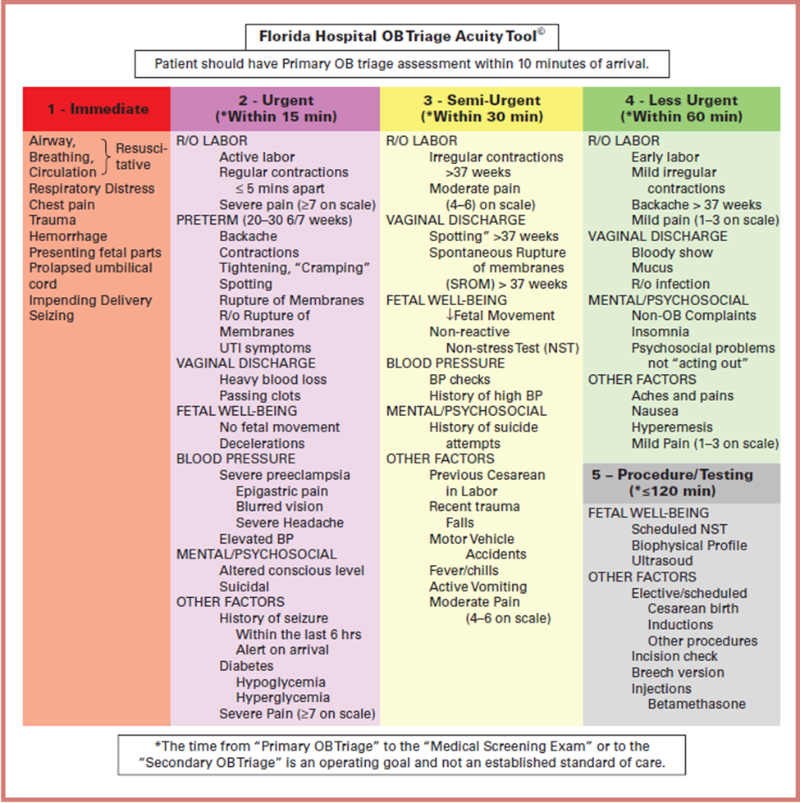
The Florida Hospital OB Triage Acuity Tool was developed in 2008. This is a 5-tier system that was created to determine how quickly obstetric patients need to get a medical exam (Paisley et al., 2011). The main goal, accompanying the development of this tool, was that obstetric patients are seen by a triage nurse and then assigned an appropriate acuity level, based on their presentation, within ten minutes of arrival to the unit (Paisley et al., 2011). This tool does not appear to have been validated at this point (Lindroos et al., 2021).
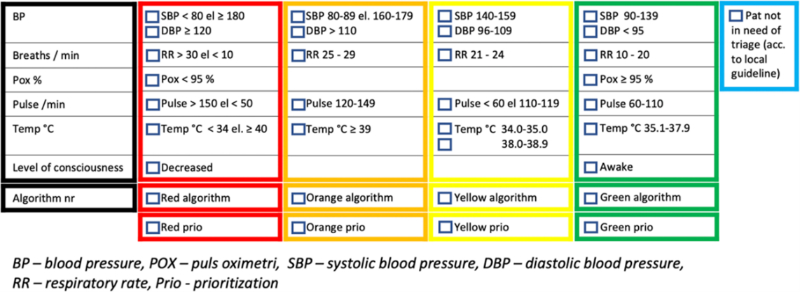
In Sweden, there is a newer obstetric triage that has been created, called the Gothenburg Obstetrical Triage System (GOTS).
Image 2: The Gothenburg Obstetric Triage System: Vital Signs
(Lindroos et al., 2021)
The GOTS acuity level assessment was developed to reflect both vital signs and to include an algorithm for 14 chief complaints (Lindroos et al., 2021). The tool’s reference ranges for vital signs were specifically adapted to the physiological changes in pregnancy (Lindroos et al., 2021). The included algorithms feature information on both obstetric and non-obstetric causes of symptoms, diagnosis, and treatment (Lindroos et al., 2021). Algorithm topics include (Lindroos et al., 2021):
Reduced fetal movements
Trauma
Suspected hypertensive disorder
Postpartum hemorrhage
Chest pain/breathing problems
Hyperemesis
Suspected mastitis
Neurological problems
Vaginal bleeding
Suspected rupture of the membranes
Contractions
Suspected thromboembolism
Signs of prenatal or postpartum infection
Abdominal/back pain
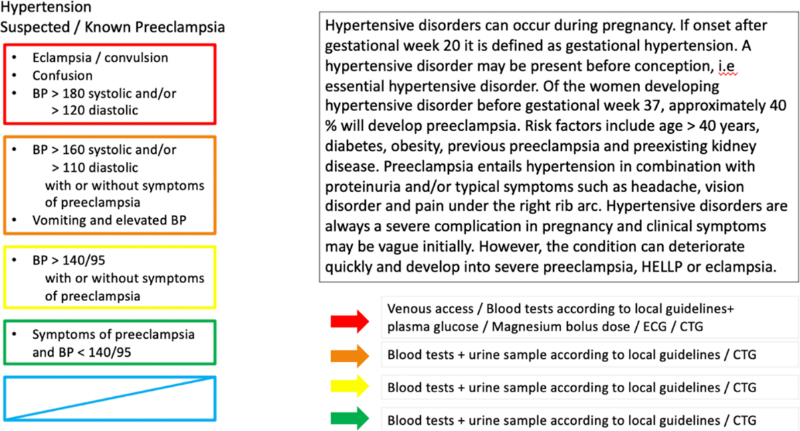
The following image is an example of the “suspected hypertensive disorder” chief complaint algorithm provided in the GOTS tool (Lindroos et al., 2021).
Image 3: The Gothenburg Obstetric Triage System: Chief Complaint Algorithms
(Lindroos et al., 2021)
The GOTS has been shown to improve the management of obstetric patients in Sweden (Lindroos et al., 2021). While there are a few different options available, not all hospitals have adopted a specific tool for triaging patients.
Women frequently come to labor and delivery units for triage just as a non-pregnant woman would go to the Emergency Department, where triage levels are used. The American College of Obstetricians and Gynecologists (ACOG) released a committee opinion in 2016 that supports the use of maternal fetal triage guidelines (American College of Obstetricians and Gynecologists [ACOG], 2016). ACOG believes that each hospital should utilize a maternal fetal triage tool because triage guidelines could improve the quality and efficiency of women's care when going to labor and delivery(ACOG, 2016).
Obstetric triage patients can increase the labor and delivery unit volume by 20-50%. As many as 33% of all women who present to labor and delivery go home without delivering their baby(Kodama et al., 2021). These increased volumes can impact patient care and outcomes. Not every patient can be seen by a provider immediately. Nurses need a way to evaluate the pregnant woman and prioritize the level of care that is needed and the speed at which care must be given(ACOG, 2016).
According to the federal Emergency Medical Treatment and Labor Act (EMTALA), all pregnant women who present to a hospital must receive an initial medical screening exam to determine if a medical emergency exists, regardless of the patient's ability to pay or where the woman usually received care (Centers for Medicare & Medicaid Services [CMS], 2023). Women who are not determined to have an emergency may be transferred, if appropriate. For women in labor, they may be transferred if the patient requests transfer, if the medical benefits outweigh possible risks to the patient and unborn child, and if the accepting hospital has space and personnel to care for the patient and agree to take the transfer(CMS, 2023).
Various tools are diverse and use slightly different criteria. The tool will have categories into which the patient should be classified (ACOG, 2016). These categories will also determine when the woman should be treated.
Several obstetric triage acuity tools have been created based on the Emergency Severity Index (ESI). Most consist of a 5-category system that classifies patients based on their acuity (ACOG, 2016). Few of these tools have more than one study supporting them, and some have not yet been validated (Mayberger et al., 2022).
The most recent tool developed by AWHONN, the Maternal Fetal Triage Index (MFTI), also has 5 categories (Association of Women's Health, Obstetric, and Neonatal Nurses [AWHONN], 2022; ACOG, 2016). It was published in 2015 and has had its most recent update in 2022. It is the very first acuity tool that was developed by a professional obstetrics society specifically intended to be used across the United States (Ruhl et al., 2015; AWHONN, 2022).
The nurse who sees the patient first (or triages them) would use this tool to determine which category the patient belongs in. Not every pregnant individual requires treatment immediately.The MFTI tool accounts for the patient’s vital signs, pain, signs of labor, and other scenarios such as leaking of fluid, HIV+ status, and presentation of fetus, along with other factors to help the nurse decide next steps(Kodama et al., 2021; AWHONN, 2022).
According to AWHONN’s tool (AWHONN, 2022; ACOG, 2016; Ruhl et al., 2015):
A woman who comes to the unit via stretcher and has a seizure would be placed into the first category or stat.
A woman with decreased fetal movement or a recent trauma would be placed in the second category, or urgent.
A woman ≥ 34 weeks in active labor would be placed in the third category, or prompt.
A woman ≥ 37 weeks in early labor would be placed in the fourth category, or non-urgent.
A woman scheduled for a non-stress test with no complaints would be placed in the fifth category or scheduled.
Unfortunately, due to copyright restrictions, AWHONN’s Maternal Fetal Triage Index tool visually cannot be displayed here. To see the most up-to-date version of the AWHONN MFTI, please visit the following link and view the videos and images provided directly by AWHONN.
While the AWHONN algorithm cannot be displayed visually, we will now review some of the included components. Let’s break down AWHONN’s MFTI tool to help us better understand its criteria for assigning triage level.
The following maternal vital signs would be considered priority 1, requiring “Stat” assistance (AWHONN, 2022; ACOG, 2016):
Heart rate <40 or >130 bpm
Apnea
Oxygen saturation <93%
Systolic blood pressure <60 or ≥160 mmHg
Diastolic blood pressure that is palpable or ≥110 mmHg
Fetal heart rate <110 bpm for >60 seconds
No fetal heart rate detected by doppler (unless known fetal demise)
In the event that immediate lifesaving intervention is required, the patient should be treated as a priority 1. Such life-threatening situations can include (AWHONN, 2022; ACOG, 2016):
Maternal cardiac compromise
Signs of placental abruption
Maternal seizures
Maternal hemorrhaging
Signs of uterine rupture
Maternal severe respiratory distress
Acute change in mental status
Unresponsiveness
Prolapsed cord
Active bearing-down
Fetal body visible on the perineum, indicating imminent birth
As described more specifically above, if the mother or fetus demonstrate these emergency vital signs, require immediate lifesaving intervention like in the situations listed, OR if birth is imminent, the woman should be made a priority level 1 (AWHONN, 2022; ACOG, 2016).
The following maternal vital signs would be considered priority 2, requiring urgent assistance (AWHONN, 2022; ACOG, 2016):
Heart rate <50 or >120 bpm
Oxygen saturation <95%
Temperature ≥101.0°F (38.3°C)
Respiratory rate <12 or >26 bpm
Systolic blood pressure <80 or ≥140 mmHg
Diastolic blood pressure <40 or ≥90 mmHg (repeated)
Fetal heart rate >160 bpm for >60 seconds
Fetal heart rate decelerations
In the event that more urgent attention but not immediate lifesaving intervention is required, the patient should be treated as a priority 2. Such situations requiring more prompt involvement can include (AWHONN, 2022; ACOG, 2016):
Mother is in severe pain, though not related to contractions, rating it >7 (on a 0-10 pain scale)
Recent trauma (assault to abdomen, fall, intimate partner violence, motor vehicle accident)
Complaints of decreased fetal movement
Difficulty breathing
Altered mental status
Active vaginal bleeding
Suicidal or homicidal behavior
Presence of unstable, high-risk medical conditions
<34 weeks gestation with complaints of uterine contractions
<34 weeks gestation with complaints of leaking of fluid, spontaneous rupture of the membranes, or spotting
≥34 weeks gestation with regular contractions or spontaneous rupture of the membranes in addition to being HIV+, a planned C-section (for maternal or fetal medical reasons), breech fetal presentation, multiple gestation, or placenta previa
Higher level of care needs that will require transfer of care to another hospital
To summarize, if a woman or fetus is exhibiting these abnormal vital signs OR in any of these situations, the woman should be made a priority level 2 (AWHONN, 2022; ACOG, 2016).
The following maternal vital signs would be considered priority 3, requiring less urgent or prompt assistance (AWHONN, 2022; ACOG, 2016):
Temperature ≥100.4°F (38.0°C)
Systolic blood pressure ≥140 mmHg (asymptomatic)
Diastolic blood pressure ≥90 mmHg (asymptomatic)
In the event that more prompt attention but not immediate lifesaving nor urgent intervention is required, the patient should be treated as a priority 3. Such situations requiring more prompt involvement can include (AWHONN, 2022; ACOG, 2016):
Mother is not coping with labor
Signs of active labor ≥34 weeks gestation
Complaints of early labor signs
Complaints of spontaneous rupture of the membranes/leaking fluid 34-36 6/7 weeks gestation
Multiple gestation at ≥34 weeks gestation having irregular contractions
≥34 weeks gestation with regular contractions and current Herpes Simplex Virus lesion
≥34 weeks gestation with planned, repeat C-section, having regular contractions
To review, if a woman or fetus is exhibiting these abnormal vital signs or in any of these clinical situations, the woman should be made a priority level 3 (AWHONN, 2022; ACOG, 2016).
In the event that more prompt attention but not immediate lifesaving, urgent, or even prompt intervention is required, the patient should be treated as a priority 4. Such situations that are non-urgent situations can include (AWHONN, 2022; ACOG, 2016):
≥37 weeks gestation showing early labor signs and/or leaking/spontaneous rupture of the membranes
Vaginal discharge
Constipation
Ligament pain
Nausea
Anxiety
Common complaints of pregnancy
If a woman is showing any of these signs and symptoms only, the woman should be made a priority level 4 (AWHONN, 2022; ACOG, 2016).
In the case in which a woman comes in, without complaint, for a scheduled procedure or is requesting a service such as a refill of her medication prescription, the woman should be made a priority 5(AWHONN, 2022; ACOG, 2016).
While AWHONN’s MFTI is thorough, it is not all-inclusive of all possible patient situations, conditions, and chief complaints (AWHONN, 2022; ACOG, 2016). It is also important to note that the included vital signs discussed above are suggested values. Variables like altitude should further guide vital sign parameters based on your own geographic region (AWHONN, 2022; ACOG, 2016).
The categories are intended to guide the nurses and providers as to when the patient should receive treatment. Each case needs to be evaluated using critical thinking, but the tool provides basic criteria to help guide the nurse and provider. A woman brought in after a motor vehicle accident with abdominal trauma should take precedence over a woman who is 37 weeks gestation and comes in because her water broke (ACOG, 2016). While the MFTI is designed and intended to guide clinical decision-making, it should not replace clinical judgment and expertise (AWHONN, 2022; ACOG, 2016).
According to AWHONN, each hospital should choose a maternal fetal triage assessment tool to guide the care of the woman who arrives at labor and delivery for triage (AGOG, 2016).
Two pregnant women arrive in a busy labor and delivery unit. Both of these pregnant women require triage. All nurses already had been assigned patient assignments when these two women arrived. Both women go into evaluation rooms.
One woman is 35 weeks pregnant and leaking fluid. She has a repeat cesarean section scheduled in 4 weeks.
The second patient is 38 weeks pregnant and complaining of leaking fluid. She is contracting every 4 to 5 minutes.
Which patient needs to be seen by the provider first?
Using a maternal fetal triage tool, the RN will first determine which patient needs to receive medical treatment. The woman who is 35 weeks and leaking fluid, with a planned repeat c-section scheduled should be evaluated first.
With a triage tool, the RN will see that the 35-week patient who has a scheduled repeat c-section and is leaking fluid should be evaluated first. The reason for the first c-section is not known and there is the possibility that this patient will need a c-section urgently. The infant is also pre-term and additional personnel could be needed. The second patient could be in early labor and can wait to be seen.
An RN with experience may already know that a 35-week patient with a previous c-section is at higher risk of a complication, but a new nurse may think that the 35-week woman is too early to deliver and choose to see the early labor patient first. Using a maternal fetal triage index tool will also enable the nurse to determine that this patient needs care urgently.
A labor and delivery unit can operate like an Emergency Department, where the next patient is usually unknown. One woman or five women may walk in the door at any time. Nursing units are not often staffed for walk-in patients. Triage patients are usually not included in staffing ratios, even though they require nursing time. The number of providers and resources may also be limited depending on the size and area of the hospital. At any time, a woman or her fetus may be in a life-or-death situation. Having a maternal fetal triage tool in place to guide the care and timeliness may improve the outcome for the mother, fetus, or both.
Women in labor and delivery units should not receive care in the order of arrival. They must be cared for in order of priority (ACOG, 2016). A process to evaluate maternal and fetal status in a triage setting is important to ensure the best outcomes for the woman and her baby.
Select one of the following methods to complete this course.
Take TestPass an exam testing your knowledge of the course material.
CEUFast, Inc. is committed to furthering diversity, equity, and inclusion (DEI). While reflecting on this course content, CEUFast, Inc. would like you to consider your individual perspective and question your own biases. Remember, implicit bias is a form of bias that impacts our practice as healthcare professionals. Implicit bias occurs when we have automatic prejudices, judgments, and/or a general attitude towards a person or a group of people based on associated stereotypes we have formed over time. These automatic thoughts occur without our conscious knowledge and without our intentional desire to discriminate. The concern with implicit bias is that this can impact our actions and decisions with our workplace leadership, colleagues, and even our patients. While it is our universal goal to treat everyone equally, our implicit biases can influence our interactions, assessments, communication, prioritization, and decision-making concerning patients, which can ultimately adversely impact health outcomes. It is important to keep this in mind in order to intentionally work to self-identify our own risk areas where our implicit biases might influence our behaviors. Together, we can cease perpetuating stereotypes and remind each other to remain mindful to help avoid reacting according to biases that are contrary to our conscious beliefs and values.
American College of Obstetricians and Gynecologists. (ACOG). (2016). Committee opinion no. 667 Summary: Hospital-based triage of obstetric patients. Obstetrics & Gynecology, 128(1), 228. Visit Source.
Association of Women’s Health, Obstetric, and Neonatal Nurses. (AWHONN). (2022). Maternal fetal triage index (MFTI). AWHONN.org. Visit Source.
Centers for Medicare & Medicaid Services. (CMS). (2023). Emergency Medical Treatment & Labor Act (EMTALA). CMS.gov. Visit Source.
Kodama, S., Mokhtari, N. B., Iqbal, S. N., & Kawakita, T. (2021). Evaluation of the maternal-fetal triage index in a tertiary care labor and delivery unit. American Journal of Obstetrics Gynecology Maternal-Fetal Medicine, 3(4), 100351. Visit Source.
Lindroos, L., Korsoski, R., Öhman, M.O. Elden, H., Karlsson, O., & Sengpiel, V. (2021). Improving assessment of acute obstetric patients – introducing a Swedish obstetric triage system. BMC Health Services Research, 21, 1207. Visit Source.
Mayberger, J., Cera, J., Rowland, S., Struwe, L., & Barnason, S. (2022). Implementation of the maternal fetal triage index to improve obstetric triage. Nursing for Women’s Health, 26(4), 269–277. Visit Source.
Paisley, K.S., Wallace, R., & DuRant, P.G. (2011). The development of an obstetric triage acuity tool. The American Journal of Maternal/Child Nursing, 36(5), 290-296. Visit Source.
Quaile, H. (2018). Implementing an obstetrics-specific triage acuity tool to increase nurses' knowledge and improve timeliness of care. Nursing for Women’s Health, 22(4), 293-301. Visit Source.
Ruhl, C., Scheich, B., Onokpise, B., & Bingham, D. (2015). Content validity testing of the maternal fetal triage index. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 44(6), 701–709. Visit Source.
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
Listen Anywhere
Listen from your pocket or in your car, Apple CarPlay and Android Auto compatible.
Subscribe for Access
Sync Between Devices
Start on your desktop, pickup on your mobile. Never lose your place.
Reinforce Your Learning
Switch between reading and listening to your course or read while you listen!
Enhance Your Experience
Interactive course outline, robust play controls, multiple voices and different playback speed options.
×
Away for now!
We're sorry! All our support agents are unavailable to chat at the moment.
Need Immediate Assistance? Please visit our FAQ section which provides answers to many common inquiries.
Get in Touch Directly via Email If your query is urgent or you'd prefer to reach us directly, we invite you to submit a support ticket through our Contact Us page. Our dedicated support team will review your inquiry and get back to you as soon as possible.
Support Hours Our chat support is typically available Monday to Friday, 9:00 AM - 6:00 PM EST. For support outside of these hours, please use our email contact
Are you sure?
You should NOT select "Remember me for 30 days" if you are on a public or shared computer.