Long-term medication use is a part of management for many chronically ill children, and while it may help manage symptoms, it is not without its own problems and risks. Many children require daily medications to manage symptoms and complications, but there are risks of side effects, tolerance, dependence, and interactions between drugs. Polypharmacy increases the risk of all of those and makes adherence to treatment plans more complicated as there are more medications and dosing schedules to keep track of (Halli-Tierney et al., 2019).
Among the risks of long-term medication use is immunosuppression, which can occur with corticosteroids, chemotherapy, or immunomodulators. Children may take these types of medications for autoimmune diseases, malignancy, or organ transplants. Reduced immune function and impaired wound healing put these children at increased risk of infections, more serious illnesses, and even common respiratory viruses. This makes attending school, sports, and social events risky, as exposure to other children greatly increases the risk of contact with infectious pathogens. However, missing out on these activities negatively impacts quality of life as well (Spinner & Denfield, 2022).
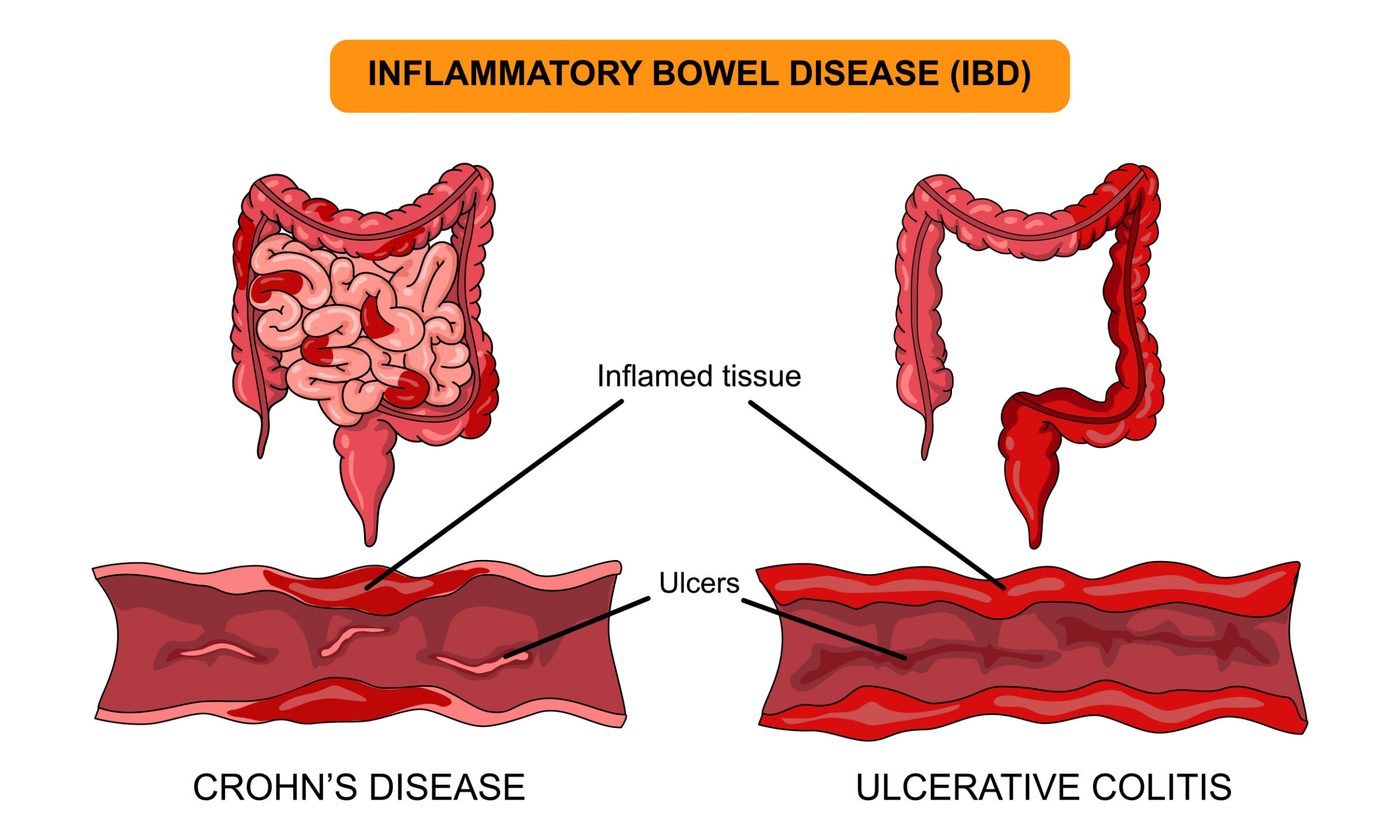
Endocrine disruption can result as well, such as Cushing’s syndrome with long-term corticosteroid use. Conditions like asthma, lupus, or inflammatory bowel disease frequently include corticosteroids in their treatment. Symptoms such as weight gain, hypertension, osteoporosis, glucose intolerance, and moon facies can occur with long-term steroid use. Not only is this syndrome hard on the body systems, but the physical changes that occur can also impact children’s self-esteem, body image, and predispose them to bullying or social stigma (Dani et al., 2023).
Long-term use of certain antiepileptic medications can lead to a deficiency of vitamin D and cause bone demineralization, which can impair growth and increase the risk of fractures (Siniscalchi et al., 2020).
Children requiring frequent injections, such as those with type 1 diabetes, are at an increased risk for lipoatrophy. Daily insulin injections can damage and cause loss of fat tissue, particularly if injection sites are not being rotated enough. Young children may be hesitant or scared to try new injection locations and stick to ones they feel comfortable with, but this can lead to fat breakdown, indentations, and visible changes in the skin. Irregular fat tissue also makes insulin absorption in those areas more unpredictable, negatively impacting glucose control (Kordonouri et al., 2020).
There are also mental health considerations for long-term medication use. Children may become frustrated with frequent medication administration, dietary restrictions, or side effects. Teens may feel a lack of control over their own treatment or may feel increased social stigma and wish to be like their peers. Many specialty medications are expensive and may not be fully covered by insurance, or may require arduous paperwork or insurance appeals, adding to the logistical and financial strain on caregivers who manage the medications (Consolini, 2022).
There is also a safety issue of having multiple medications in the house, some of which may be controlled substances. This poses a risk for siblings or pets and may also be a risk for children who have comorbid depression or thoughts of suicide. In general, prescription medications should be kept in a safe location accessible only to adults.