What was once a minor focus problem has rapidly become a widespread public health concern, demanding urgent attention. Projections show that 50 percent of the world's population will experience nearsightedness by 2050. This issue threatens individual visual clarity and the long-term eye health of future generations.
For children, increased time on close-up activities, digital screens, and intensive schooling, combined with reduced outdoor time drives the rising prevalence of myopia. In contrast, myopia progression usually slows and stabilizes in adulthood compared to childhood and adolescence. Some adults, particularly those with high or pathological myopia, certain underlying health conditions, or demanding near work, can still experience gradual worsening.
Myopia is far more than a simple focus problem. This article examines how it physically changes the eye, explores its genetic, environmental, and medical causes, and addresses its symptoms, complications, and prevention, emphasizing why early recognition at every stage of life is essential for protecting long-term eye health.
What Is Myopia?
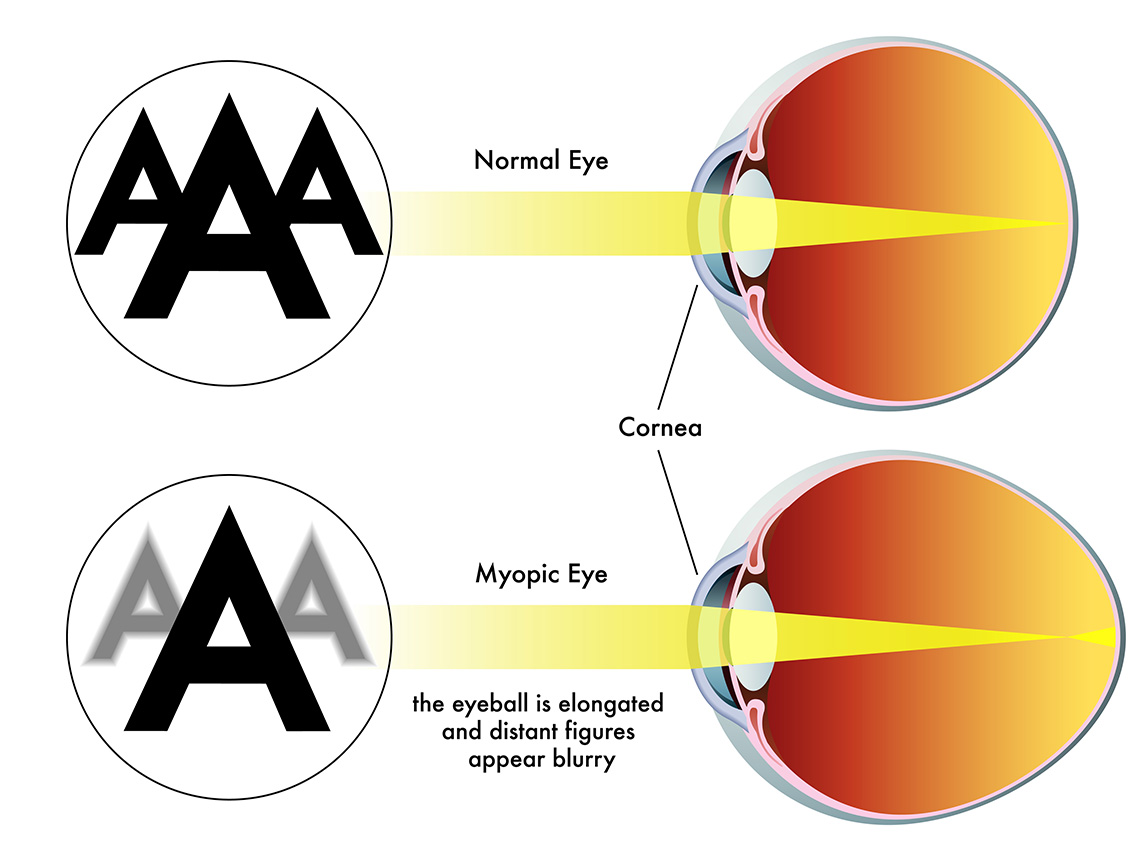
In a healthy eye, the cornea and lens bend incoming light rays to focus precisely on the retina, producing clear vision. In myopia, there is an elongation of the eyeball or an overly curved cornea that forces light to focus in front of the retina instead of on the retina. This leads to blurred distance vision, while near objects remain clear. Clinicians classify this as a refractive error of the eye.
The story of why myopia develops and progresses so differently across individuals begins with the most fundamental influence of all: our genetic inheritance.
Causes of Myopia
Research indicates a significant genetic component, with multiple genes contributing to an individual's risk. Children with one or especially two myopic parents are much more likely to develop myopia themselves. Some genes affect eye growth (axial length), others influence scleral structure (shape and rigidity), and others are involved in retinal signaling pathways that regulate development.
Gene and Environment Interaction
While genetics establishes an individual's susceptibility to myopia, the environment often determines whether and how strongly that risk is expressed. Over recent decades, lifestyle changes, particularly in children and adolescents, have created conditions that accelerate myopia onset and progression.
Identifying the key environmental influences, including reduced outdoor time, intensive near work and educational demands, and features of modern urban living, is essential for empowering individuals, families, and healthcare providers to make choices that can delay, reduce, or help prevent the worsening of myopia.
Environmental Factors That Influence Myopia
Reduced Outdoor Time
Spending time outdoors plays a protective role against the development and progression of myopia. Exposure to natural light stimulates dopamine release in the retina, which helps regulate axial eye growth and reduces elongation linked to myopia. Research suggests that adding roughly an extra hour of outdoor time per day can significantly lower the risk of myopia onset. The shift toward predominantly indoor lifestyles in modern childhood is therefore considered one of the most important and modifiable contributors to the global rise in myopia.
Near Work
Near work refers to visually demanding tasks performed at close range, such as reading, writing, drawing, and using digital devices like smartphones, tablets, and computers. This predisposes a person to having a higher likelihood of both developing myopia and experiencing faster progression, especially when working distances are shorter than about 20 to 30 centimeters. The widespread use of digital technology has greatly increased the hours children spend on near work during key years of eye development.
Educational Demands
Educational pressures intensify this effect. Intensive study schedules, long homework hours, and highly competitive school environments increase near-work demands and reduce outdoor time. Children in academically demanding settings and systems that emphasize extended reading, writing, and screen-based learning may see higher rates of myopia.
Urban Living
Urban living often combines several myopia-promoting factors into one setting. Children in cities are more likely to spend time indoors, have limited access to safe outdoor spaces, live in smaller homes with shorter viewing distances, and experience greater academic pressure. These conditions together are associated with higher myopia prevalence compared with rural environments.
Studies comparing urban and rural students consistently show higher myopia rates in urban groups. Children living in apartments, which are common in densely populated areas, appear particularly vulnerable, reflecting how the built environment and lifestyle patterns can shape eye growth and visual outcomes from an early age.
Medical Causes of Myopic Shifts
While genetic predisposition and environmental pressures account for the majority of myopia cases, not all myopic changes reflect typical developmental onset or progression. A range of systemic and ocular conditions can induce true or temporary shifts toward nearsightedness, sometimes mimicking progressive myopia and leading to mismanagement if left unrecognized. Accurate diagnosis is therefore critical. Distinguishing a medical cause from routine myopia progression determines whether a patient needs a stronger prescription or a targeted clinical intervention.
The following scenarios illustrate how diverse these medical causes can be.
Systemic Conditions
Systemic conditions are whole-body illnesses or medication effects that indirectly alter how the eye focuses light, producing a myopic shift without any permanent change in eye structure.
1. Diabetes and Fluctuating Blood Sugar
"My distance vision was fine last month. Now it alternates between blurry and clear." - A middle-aged patient with diabetes might say something similar to this.
When a diabetic patient reports fluctuating distance vision, the clinician should consider blood sugar levels before attributing the change to myopia progression. Uncontrolled or fluctuating blood sugar disrupts the fluid balance within the lens, altering its ability to bend light properly. This creates a temporary shift toward nearsightedness that fluctuates alongside glucose levels rather than reflecting any permanent change in eye shape.
Reviewing the patient's glucose records alongside the timeline of visual changes often confirms the link. This type of myopic shift is reversible with better blood sugar control. Prescribing stronger glasses without investigating the underlying cause risks giving an inaccurate correction, underscoring the important connection between overall health and vision.
2. Medication-Induced Myopia with Secondary Angle Closure
"My distance vision got blurry over two days, and my eyes feel achy. The only thing that has changed is a new migraine medication." - An example of something a patient in their 30s would present with urgently.
This presentation is a genuine eye emergency. Sudden nearsightedness in both eyes, occurring soon after taking medications like topiramate, certain antibiotics, or diuretics, signals a potential drug-induced fluid reaction behind the lens.
The medication causes fluid to build up behind the lens, pushing it forward. This increases the eye's focusing power, shallows the space at the front of the eye, and blocks the eye's natural drainage system, causing pressure inside the eye to rise dangerously. If untreated, this can lead to a serious form of glaucoma.
Examination confirms a sudden shift toward nearsightedness, raised eye pressure, and a shallow front chamber. Management is time-critical: the medication must be stopped immediately, eye pressure treated, and the eye closely monitored. A thorough medication history is essential in any patient presenting with a sudden visual change.
Ocular Conditions
Ocular conditions are problems originating within the eye itself, whether structural, developmental, or functional, that alter how light is focused and perceived.
3. Index Myopia from Nuclear Cataracts
"Funny thing, I can read better without my glasses now, but my night driving is terrible." - An older adult with longstanding farsightedness might say something similar to this.
This surprising improvement in near vision is a well-recognized sign of a developing cataract. As the central part of the lens gradually hardens and becomes denser with age, a process known as nuclear sclerosis, it increases the lens's focusing power, shifting the eye toward nearsightedness.
In someone who has been farsighted for most of their life, this shift may temporarily reduce or cancel out their prescription, making reading easier without glasses. However, overall image quality deteriorates, and night vision worsens due to light scatter within the clouded lens.
Microscopic eye examination confirms the cataract, and the appropriate treatment is cataract surgery, not a prescription change. Recognizing this pattern prevents the mistaken belief that vision is spontaneously improving when the lens is in fact worsening.
4. Form-Deprivation Myopia: When the Eye Is Denied Clear Images
"One eye turns in at times, and she does not see well out of it." - Example of something parents might say describing their child.
Form-deprivation myopia develops when something blocks clear images from reaching the eye during the critical window of early visual development. In this case, a drooping upper eyelid, a condition known as ptosis, partially covers the pupil, preventing the eye from receiving the sharp visual input it needs to grow normally.
Without this clear visual stimulation, the eye loses its normal growth regulation and begins to elongate abnormally, resulting in significant nearsightedness in the affected eye. Examination confirms the diagnosis. Management must be prompt and thorough. It should include surgery for the eyelid obstruction and address the resulting nearsightedness and the risk of amblyopia (lazy eye) if the blockage persists during early development. Early recognition is essential, as the window for successful vision recovery narrows quickly with age.
5. Pseudo-Myopia: When a Muscle Spasm Mimics Progression
"My nearsightedness suddenly got way worse after cramming for exams. I just got new glasses last year." - A college student might say something similar to this example.
A sudden worsening of nearsightedness in a young person after prolonged intense study is an important clinical signal. A careful clinician considers whether a functional rather than structural cause may be responsible, rather than proceeding directly to a prescription update.
Standard vision testing initially suggests an increase in myopia. However, when dilating eye drops are used to fully relax the eye's internal focusing muscle, in a test known as cycloplegic refraction, the apparent increase in nearsightedness disappears. Pseudo-myopia occurs when the eye's focusing muscle becomes overworked from close work, a condition called accommodative spasm. This causes the muscle to remain contracted, artificially increasing nearsightedness.
This is a reversible condition. Prescribing stronger glasses would reinforce the problem rather than solve it. Management focuses on regular breaks from close work, good visual habits, and occasionally short-term use of relaxing eye drops.
Symptoms and Complications of Myopia
Myopia does not always announce itself dramatically. In many cases, particularly in children, the early signs are subtle and easily mistaken for inattention, tiredness, or learning difficulties. Recognizing symptoms early and understanding the complications that can arise when myopia goes unmanaged or progresses significantly are both essential steps toward protecting vision across the lifespan.
Common Symptoms of Myopia
The most recognizable symptom of myopia is blurred vision when looking at distant objects, such as a whiteboard at school, road signs, or faces across a room, while near vision typically remains clear. Alongside this, individuals may experience the following symptoms.
Squinting is one of the earliest and most telling signs, particularly in children. Narrowing the eyes temporarily improves focus by reducing the amount of unfocused light entering the eye. A child who consistently squints at screens, boards, or during outdoor activities should be assessed promptly.
Eye strain and headaches frequently accompany uncorrected myopia. When the eye works harder to compensate for blurred distance vision, the surrounding muscles fatigue, producing a dull ache around or behind the eyes and tension headaches, especially after prolonged visual tasks.
Difficulty seeing at night is particularly common in moderate to high myopia. Reduced contrast sensitivity and increased light scatter make nighttime driving, walking, or navigating poorly lit environments more challenging.
Rubbing the eyes and excessive blinking are frequently observed in younger children who cannot yet articulate visual difficulty but instinctively respond to visual discomfort.
How Symptoms Present Differently Across the Lifespan
In children, myopia often goes unrecognized because children adapt quickly and may not realize their vision is abnormal. Common behavioral indicators include sitting too close to the television, holding books very near the face, losing interest in activities that require distance vision, such as sports, and performing poorly at school due to difficulty reading the board.
In adults, symptoms are more likely to be self-reported and typically prompt an eye test. Adults may notice increasing difficulty driving, watching television, or recognizing people at a distance. Uncorrected or undercorrected myopia in working adults also contributes to reduced productivity and persistent visual fatigue.
Complications of Myopia
While low to moderate myopia is manageable with corrective lenses, high myopia, generally defined as a prescription of negative six diopters or more, significantly increases the risk of serious, sight-threatening complications. The structural stress placed on the eye at this level of severity makes the retina, macula, optic nerve, and lens increasingly vulnerable over time. The following complications represent the most clinically significant risks.
Retinal Detachment
Retinal detachment is one of the most serious complications of high myopia. The structural vulnerability of a highly myopic eye increases the likelihood of tears or holes forming in the retina, through which fluid can seep and lift it away from its underlying tissue. This is a medical emergency. Symptoms include a sudden increase in floaters, flashes of light, or a curtain-like shadow spreading across the visual field. Without prompt surgical intervention, permanent vision loss can result.
Myopic Macular Degeneration
The macula is the small central region of the retina responsible for sharp, detailed vision used for reading and recognizing faces. In high myopia, progressive tissue stress in this area can lead to myopic maculopathy, ranging from mild thinning to severe atrophy or abnormal blood vessel growth beneath the retina. This condition is a leading cause of irreversible vision loss in people with high myopia and can significantly affect quality of life.
Glaucoma
People with myopia, particularly high myopia, carry a significantly elevated risk of developing glaucoma, a condition in which progressive optic nerve damage gradually reduces the visual field. It often develops silently with no pain or obvious symptoms until significant vision loss has occurred, making regular monitoring essential in myopic individuals.
Cataracts
Although cataracts are commonly associated with aging, people with high myopia tend to develop them earlier and more rapidly than the general population. The structural stress within a highly myopic eye accelerates the clouding process, potentially requiring surgical intervention at a younger age than expected.
Myopia Severity and Complication Risk
Research confirms that even low and moderate myopia carries some degree of risk, reinforcing the value of early intervention to slow progression before it reaches more dangerous levels. Every diopter of myopia that can be prevented or slowed represents a meaningful reduction in long-term risk.
When to Seek Help
Certain symptoms warrant prompt clinical attention regardless of whether a myopia diagnosis has already been made:
- A sudden increase in floaters or flashes of light.
- A shadow, curtain, or dark area appearing in the visual field.
- Sudden blurring or distortion of central vision.
- Any rapid or unexplained change in vision.
These may signal a retinal event or other acute complication requiring urgent evaluation. Knowing the full picture of what myopia looks like and what it can lead to raises the most important question of all: what can be done to prevent it, slow it, and catch it before it causes lasting harm?
Prevention and Early Recognition
Knowing the risk factors for myopia creates a genuine opportunity for action. Prevention in the context of myopia does not always mean eliminating the condition entirely, as genetic susceptibility cannot be changed. It means reducing the likelihood of onset where possible, slowing progression once myopia develops, and intervening clinically before the condition reaches levels associated with serious complications. These goals are achievable, but they depend on awareness, consistent habits, and timely professional assessment.
Prevention
Lifestyle Modification
The environmental factors discussed earlier, particularly time spent outdoors, near work habits, and the demands of modern education, are also the most accessible targets for prevention. Current evidence supports a minimum of one to two hours of outdoor time daily for children as a meaningful protective measure against myopia onset. This recommendation has gained enough clinical weight that the National Academies of Sciences, Engineering, and Medicine has formally endorsed it as part of a broader public health approach to myopia.
Reducing prolonged close-up tasks, taking regular breaks during reading or device use, and maintaining working distances greater than 30 centimeters are practical steps that families, schools, and employers can implement without clinical intervention. These are not simply good habits but evidence-informed strategies grounded in an understanding of how the eye responds to its environment.
Clinical Myopia Control
For children in whom myopia has already developed, a growing range of clinically proven treatments can significantly slow its progression. This is a distinct and important step beyond simply prescribing corrective lenses. The goal of myopia control is not only to improve current vision but to reduce the total amount of myopia a child accumulates, thereby lowering their long-term risk of the complications outlined earlier.
Low-dose atropine eye drops are among the most widely studied myopia control options. Administered nightly in very small concentrations, typically 0.01 to 0.05 percent, they work by relaxing the internal mechanisms that drive eye elongation. Research indicates they can reduce myopia progression by approximately one diopter per year, with a favorable safety profile at low doses.
Orthokeratology, commonly called Ortho-K, involves wearing specially designed rigid contact lenses overnight. These lenses gently reshape the front surface of the eye during sleep, temporarily correcting vision through the day without glasses or contact lenses. Beyond vision correction, they have a demonstrated effect in slowing the rate at which myopia worsens in children.
Myopia control spectacle lenses and soft contact lenses are specially designed optical lenses that correct distance vision while simultaneously sending signals to the eye that reduce the stimulus for further elongation. These offer a practical and accessible option for children who are not suitable candidates for Ortho-K or atropine therapy, and their use is becoming increasingly mainstream as evidence for their effectiveness grows.
The most appropriate myopia control strategy depends on a child's age, degree of myopia, rate of progression, and individual circumstances. An eye care professional is best placed to guide these decisions, and early referral is key to maximizing the benefit of available interventions.
Early Recognition
Myopia that goes undetected during childhood does not simply affect vision. It affects learning, development, confidence, and safety. A child who cannot see the classroom board clearly may be misidentified as inattentive or struggling academically when the real barrier is uncorrected vision. Beyond the immediate functional impact, undetected myopia that is left to progress unchecked accumulates into higher levels of myopia that carry significantly greater complication risks later in life. Detecting myopia early creates the opportunity to manage it actively rather than simply correct it passively.
Regular Comprehensive Eye Examinations
Vision screening at school or during a general health check, while valuable as a first step, is not a substitute for a full eye examination. School screenings are designed to identify children who need further assessment, not to provide a comprehensive picture of eye health. A comprehensive eye examination by an optometrist or ophthalmologist assesses not only visual acuity but also the health of the eye, the degree of any refractive error, and signs of early progression or associated risk.
Children should have their first formal eye examination before starting school and at regular intervals throughout childhood, with frequency guided by individual risk. Those with a family history of myopia warrant closer monitoring given their elevated baseline risk.
The Role of Parents, Schools, and Healthcare Providers
Early recognition is a shared responsibility. Parents are often the first to notice behavioral signs of visual difficulty, such as squinting, sitting too close to screens, losing interest in distance activities, or complaints of headaches after schoolwork. These observations are clinically significant and should prompt a professional eye assessment rather than a wait-and-see approach.
Teachers and school staff are equally well-positioned to notice children who consistently struggle to read the board, copy work inaccurately, or avoid activities requiring distance vision. Integrating vision awareness into school health programs strengthens the likelihood of early identification.
For healthcare providers, including nurses, every clinical encounter with a child is an opportunity to ask about vision. Asking a few brief screening questions during routine consultations, noting any parental concerns, and referring appropriately costs little time but can make a meaningful difference to a child's visual future.
Conclusion
Myopia is no longer just a minor focusing issue but a lifelong eye condition that can increase the risk of retinal disease, glaucoma, and earlier cataract if it progresses unchecked. Because both genes and environment shape how it develops, many of its risks can be reduced through early detection, healthier visual habits, and targeted myopia control treatments in childhood. Viewing myopia as a condition to be actively managed rather than passively corrected allows clinicians, families, and patients to protect not only clear sight today but also long-term eye health into adulthood.
About the Author
Glenel Loring is a dedicated nurse transitioning into freelance health writing. With 20 years of bedside nursing experience, Glenel deeply understands healthcare. She is now looking to apply her medical expertise to craft engaging, informative content for diverse audiences. Glenel's writing highlights her ability to make complex health topics accessible and relatable. Her interest in herbal supplements as alternative health solutions showcases her dedication to lifelong learning. As a mother of two and avid gardener, Glenel brings a personal touch to her work. With her strong nursing background and emerging writing skills, Glenel seeks opportunities to help brands and publications educate and empower readers to take control of their well-being.
Glenel is an independent contributor to CEUfast's Nursing Blog Program. Please note that the views, thoughts, and opinions expressed in this blog post are solely those of the independent contributor and do not necessarily represent those of CEUfast. This blog post is not medical advice. Always consult with your personal healthcare provider for any health-related questions or concerns.
If you want to learn more about CEUfast's Nursing Blog Program or would like to submit a blog post for consideration, please visit https://ceufast.com/blog/submissions.